Introduction
The most common type of kidney cancer is renal cell
carcinoma (RCC), constituting ~85% of malignant renal tumors and
3–6% of all adult malignancies (1).
RCC is a heterogeneous malignancy, the most common histological
subtypes being clear-cell (60–75%), papillary (10–15%), chromophobe
(5%), and collecting duct carcinoma, each of which are associated
with specific histopathological and genetic characteristics. In the
2004 World Health Organization renal tumor classification, the
Xp11.2 translocation RCC with TFE3 gene fusion is described as a
distinct entity (2). Furthermore,
Xp11.2 translocation RCCs have been reported as being more
aggressive and having a poorer prognosis compared with other
subtypes of RCC (3). In addition,
Xp11.2 translocation RCCs are generally considered a pediatric
cancer, accounting for 20–40% of pediatric RCCs and only 1–1.6% of
adult RCCs (4,5). In addition, adult Xp11.2 translocation
RCC has a poorer prognosis compared with its pediatric counterpart
(6). This type of RCC is generally
characterized by a range of translocations on chromosome Xp11.2
leading to a gene fusion between TFE3 and at least 6 possible
partners (7). The diagnosis of
Xp11.2 translocation RCC is based on fluorescent in situ
hybridization (FISH) rather than histological characteristics and
imaging examination (8). The
majority of patients with Xp11.2 translocation RCC present at a
more advanced stage compared with conventional RCC (9). Surgical resection is considered as the
most effective method for the treatment of Xp11.2 translocation
RCC.
We herein report a rare case involving an elderly
patient with Xp11.2 translocation RCC with TFE3 gene fusion, and
review the relevant literature.
Case report
A 70-year-old man was diagnosed with a solid mass in
the right kidney during a routine health examination and consulted
a doctor at the Department of Urology, Peking University Shenzhen
Hospital (Shenzhen, China) on June 9, 2015. The patient was healthy
prior to the discovery of the tumor, and he had no surgical
history, no family history of cancer, and no history of smoking or
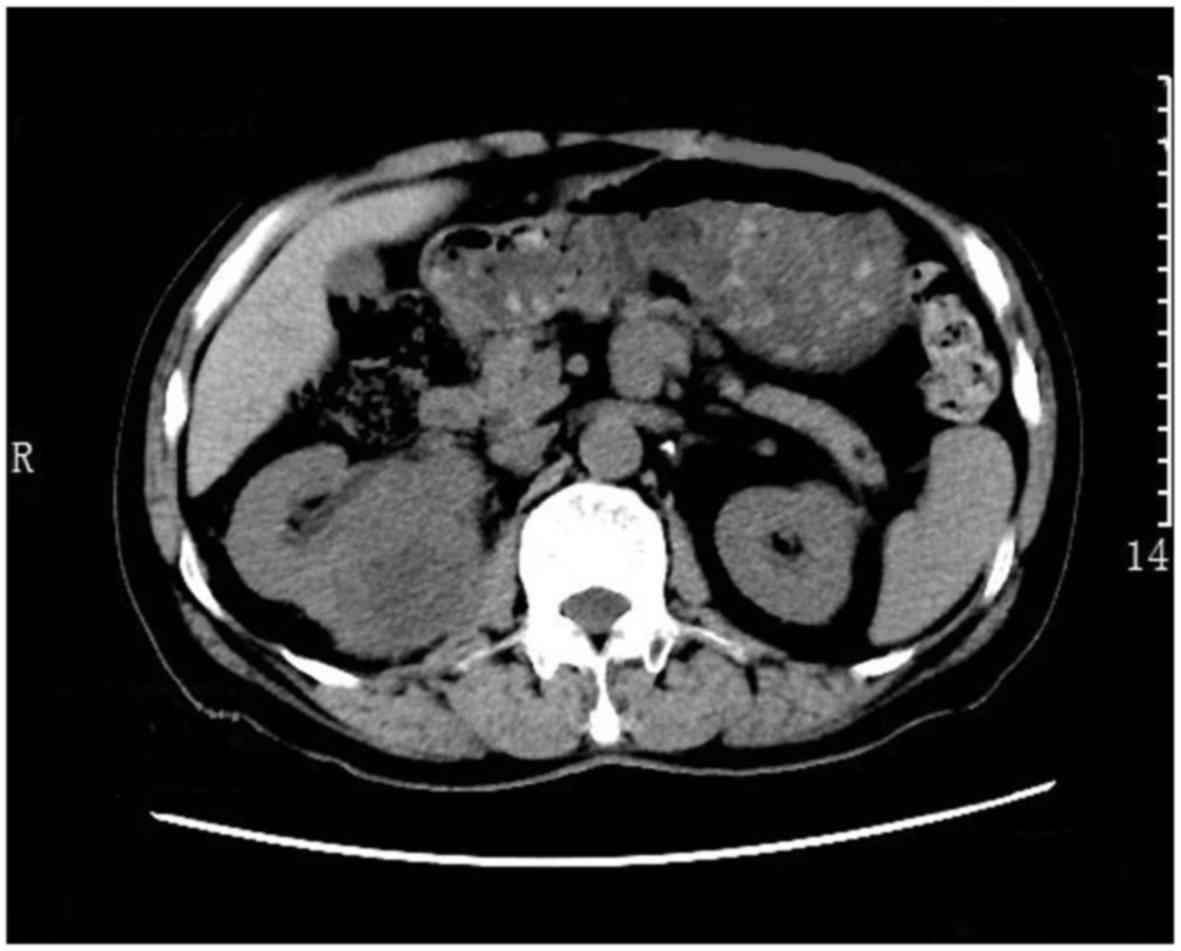
drinking. The routine blood tests were normal. A computed
tomography scan revealed a solid mass in the right kidney, sized
6.1×5.6×8.2 cm (Fig. 1).
As there were no contraindications to surgery, the
patient underwent radical right nephrectomy on June 15, 2015. The
surgery was successful, and the size of excised kidney was
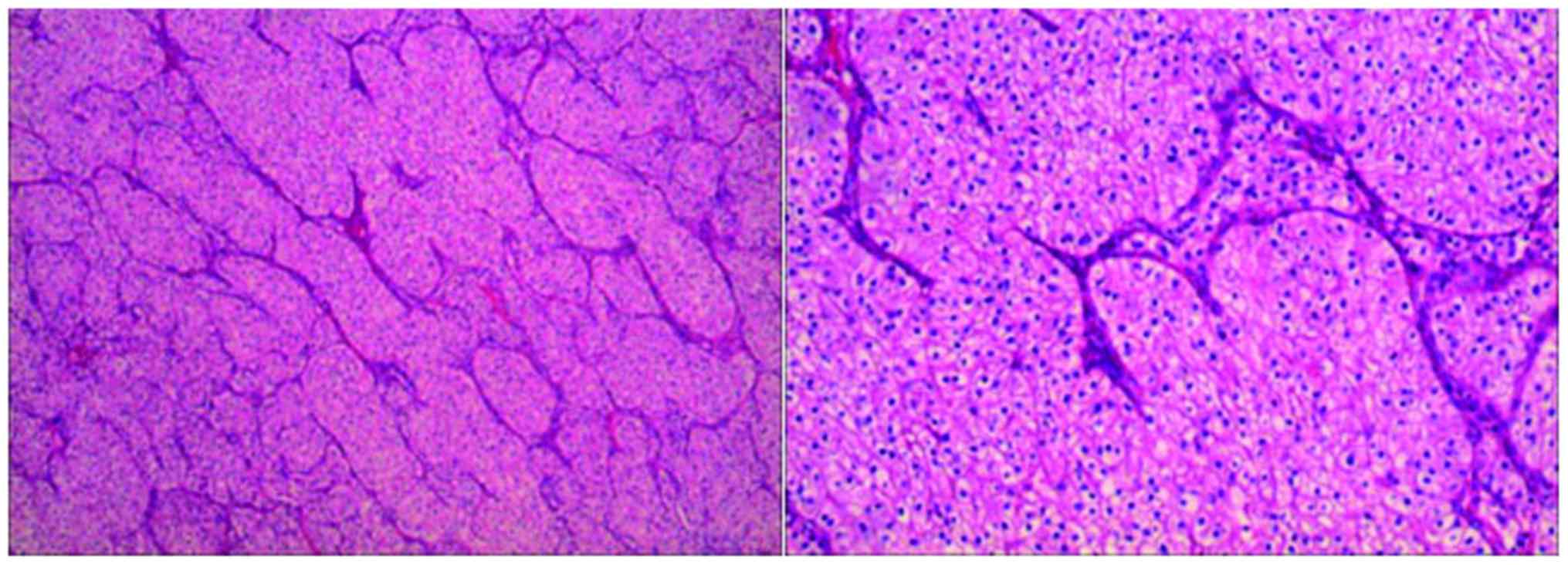
8×13.5×6.5 cm. On pathological examination, a proportion of the
tumor cells were arranged in nests and had a clear cytoplasm,
whereas the remaining cells were arranged in a papillary pattern
and had eosinophilic cytoplasm (Fig.
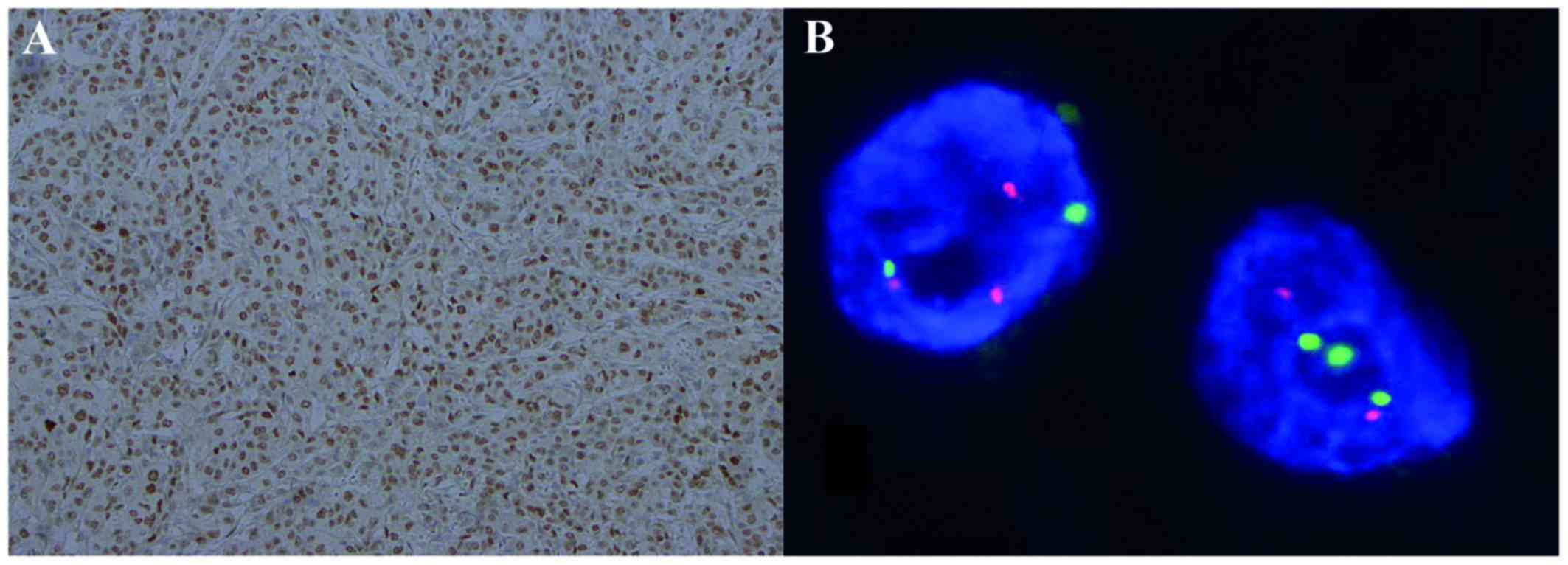
2). The immunohistochmical (IHC) examination revealed that CD10
and CK8/18 were negative and TFE3 was positive (Fig. 3A). FISH analysis revealed positive
TFE3 translocation in the tumor cells (Fig. 3B).
After the surgery, the patient was treated with
intravenous fluid therapy and pain relief medication. The patient
had an uneventful postoperative recovery and was discharged from
the hospital after 2 weeks. However, he succumbed to cancer
recurrence 1 year later.
Discussion
Xp11.2 translocation RCC with TFE3 gene fusion is a
rare tumor, and adult Xp11.2 translocation RCC has a poorer
prognosis compared with its pediatric counterpart. The aim of the
present study was to report a rare case involving an elderly
patient with Xp11.2 translocation RCC with TFE3 gene fusion of the
right kidney and review the relevant literature to help elucidate
the characteristics of this rare type of cancer.
Xp11.2 RCC with TFE3 gene fusion has at least 5
fusion partners, including ASPL-TFE3, PSF-TFE3, CLTC-TFE3,
PRCC-TFE3 and Nono-TFE3, with the chromosomal rearrangements
t(X;17)(p11.2;q25), t(X;1)(p11.2;p34), t(X;17)(p11.2;q23),
t(X;1)(p11.2;q21) and inv(X)(p11.2;q12), respectively (10,11).
Sidhar et al were the first to describe this rare cancer
(12), and the World Health
Organization recognized it as a distinct entity in 2004 (2). The different gene fusions may be
associated with different clinical and morphological
characteristics (13). As these
translocations are located on the X chromosome, it would appear
reasonable to expect gender differences in this rare cancer;
however, there is a insufficient evidence to support this
hypothesis.
Xp11.2 translocation RCC exhibits different
morphological characteristics similar to clear-cell RCC and
papillary renal cancer (14). The
typical morphology includes nested or papillary architecture, with
cells with voluminous, clear or eosinophilic cytoplasm.
The most common diagnostic method of Xp11.2
translocation RCC with TFE3 gene fusion is IHC assay using an
antibody for the C-terminal portion of TFE3 (15), as this cancer involves TFE3 protein
overexpression. However, recent studies have reported that IHC for
TFE3 is associated with a high rate of false-positive results
(16). Thus, the genetic
identification of this rare cancer using FISH is an important
diagnostic method (7).
Xp11.2 translocation RCC mostly affects children,
accounting for 20–40% of pediatric RCCs and only 1–1.6% of RCCs in
adults (4,5). However, as the overall incidence of RCC
has increased, the Xp11.2 translocation RCC in adults has become
more common. It has been reported that Xp11.2 translocation RCC in
adult patients may be associated with advanced stage at diagnosis
and an aggressive clinical course, with a poor prognosis (17). Srigley et al reported the
adult patients have a mean survival of up to 2 years, whereas the
mean survival in pediatric patients is 6.3 years (7). Furthermore, it has been reported that
~15% of the adult patients with Xp11.2 translocation RCC had a
history of chemotherapy; thus, the occurrence of this cancer may be
correlated with chemotherapy (7).
The treatment for Xp11.2 RCC varies; however, there
has been no established effective treatment to date. The most
common treatment of Xp11.2 RCC is similar to that for conventional
RCC. For localized Xp11.2 RCC with positive regional lymph nodes,
surgery is the optimal treatment (18). If the tumor is sized <7 cm,
nephron-sparing surgery is considered as a treatment option
(19). Immunotherapy may be
beneficial for patients who have hematogenous metastases, including
multikinase inhibitors, interleukin-2 and interferon-α. Recent
studies suggested that mammalian target of rapamycin inhibitors may
be effective for Xp11.2 translocation RCC (12,20).
Moreover, targeted agents, such as sunitinib, sorafenib and
everolimus, have also been applied (21).
Acknowledgements
The present study was supported by the National
Natural Science Foundation of China (grant no. 81101922), the
Science and Technology Development Fund Project of Shenzhen (grant
nos. JCYJ20150403091443329 and JCYJ20170307111334308), the fund of
‘San-ming’ Project of Medicine in Shenzhen, and the fund of
Guangdong Key Medical Project.
References
|
1
|
Verhoest G, Veillard D, Guillé F, De La
Taille A, Salomon L, Abbou CC, Valéri A, Lechevallier E, Descotes
JL, Lang H, et al: Relationship between age at diagnosis and
clinicopathologic features of renal cell carcinoma. Eur Urol.
51:1298–1304. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Bruder E, Passera O, Harms D, Leuschner I,
Ladanyi M, Argani P, Eble JN, Struckmann K, Schraml P and Moch H:
Morphologic and molecular characterization of renal cell carcinoma
in children and young adults. Am J Surg Pathol. 28:1117–1132. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Qiu Rao, Bing Guan and Zhou XJ: Xp11.2
translocation renal cell carcinomas have a poorer prognosis than
non-Xp11.2 translocation carcinomas in children and young adults: A
meta-analysis. Int J Surg Pathol. 18:458–464. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kmetec A and Jeruc J: Xp 11.2
translocation renal carcinoma in young adults; recently classified
distinct subtype. Radiol Oncol. 48:197–202. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Komai Y, Fujiwara M, Fujii Y, Mukai H,
Yonese J, Kawakami S, Yamamoto S, Migita T, Ishikawa Y, Kurata M,
et al: Adult Xp11 translocation renal cell carcinoma diagnosed by
cytogenetics and immunohistochemistory. Clin Cancer Res.
15:1170–1176. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Argani P and Ladanyi M: Translocation
carcinomas of the kidney. Clin Lab Med. 25:363–378. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Klatte T, Streubel B, Wrba F, Remzi M,
Krammer B, de Martino M, Waldert M, Marberger M, Susani M and
Haitel A: Renal cell carcinoma associated with transcription factor
E3 expression and Xp11.2 translocation: Incidence, characteristics,
and prognosis. Am J Clin Pathol. 137:761–768. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Srigley JR, Delahunt B, Eble JN, Egevad L,
Epstein JI, Grignon D, Hes O, Moch H, Montironi R, Tickoo SK, et
al: The international society of urological pathology (ISUP)
vancouver classification of renal neoplasia. Am J Surg Pathol.
37:1469–1489. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Sukov WR, Hodge JC, Lohse CM, Leibovich
BC, Thompson RH, Pearce KE, Wiktor AE and Cheville JC: TFE3
rearrangements in adult renal cell carcinoma: Clinical and
pathologic features with outcome in a large series of consecutively
treated patients. Am J Surg Pathol. 36:663–670. 2012.PubMed/NCBI
|
|
10
|
Wang W, Ding J, Li Y, Wang C, Zhou L, Zhu
H and Peng W: Magnetic resonance imaging and computed tomography
characteristics of renal cell carcinoma associated with Xp11.2
translocation/TFE3 gene fusion. PLoS One. 9:e999902014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Liu K, Xie P, Peng W and Zhou Z: Renal
carcinomas associated with Xp11.2 translocations/TFE3 gene fusions:
Findings on MRI and computed tomography imaging. J Magn Reson
Imaging. 40:440–447. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ellati RT, Abukhiran I, Alqasem K, Jasser
J, Khzouz J, Bisharat T, Al-Saidi I and Al-Daghmin A:
Clinicopathologic features of translocation renal cell carcinoma.
Clin Genitourin Cancer. 15:112–116. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Rao Q, Williamson SR, Zhang S, Eble JN,
Grignon DJ, Wang M, Zhou XJ, Huang W, Tan PH, Maclennan GT and
Cheng L: TFE3 break-apart FISH has a higher sensitivity for Xp11.2
ranslocation-associated renal cell carcinoma compared with TFE3 or
cathepsin K immunohistochemical staining alone: Expanding the
morphologic spectrum. Am J Surg Pathol. 37:804–815. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Rao Q, Chen JY, Wang JD, Ma HH, Zhou HB,
Lu ZF and Zhou XJ: Renal cell carcinoma in children and young
adults: Clinicopathological, immunohistochemical, and VHL gene
analysis of 46 cases with follow-up. Int J Surg Pathol. 19:170–179.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Dey B, Badhe B, Govindarajan KK and Ramesh
RA: Xp11.2 translocation renal cell carcinoma diagnosed by
immunohistochemistry and cytogenetics. J Lab Physicians. 8:123–125.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Green WM, Yonescu R, Morsberger L, Morris
K, Netto GJ, Epstein JI, Illei PB, Allaf M, Ladanyi M, Griffin CA
and Argani P: Utilization of a TFE3 break-apart FISH assay in a
renal tumor consultation service. Am J Surg Pathol. 37:1150–1163.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Xu L, Yang R, Gan W, Chen X, Qiu X, Fu K,
Huang J, Zhu G and Guo H: Xp11.2 translocation renal cell
carcinomas in young adults. BMC Urol. 15:572015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ahluwalia P, Nair B and Kumar G: Renal
cell carcinoma associated with Xp11.2 translocation/TFE3 gene
fusion: A rare case report with review of the literature. Case Rep
Urol. 2013:8105902013.PubMed/NCBI
|
|
19
|
Song HC, Sun N, Zhang WP, He L, Fu L and
Huang C: Biological characteristics of pediatric renal cell
arcinoma associated with Xp11.2 translocations/TFE3 gene fusions. J
Pediatr Surg. 49:539–542. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Kakoki K, Miyata Y, Mochizuki Y, Iwata T,
Obatake M, Abe K, Nagayasu T and Sakai H: Long-term treatment with
sequential molecular targeted therapy for Xp11.2 translocation
renal cell carcinoma: A case report and review of the literature.
Clin Genitourin Cancer. 15:e503–e506. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Sudour-Bonnange H, Leroy X, Chauvet MP,
Classe M, Robin PM and Leblond P: Cutaneous metastases during an
aggressive course of Xp11.2 translocation renal cell carcinoma in a
teenager. Pediatr Blood Cancer. 61:1698–1700. 2014. View Article : Google Scholar : PubMed/NCBI
|