Introduction
Diabetes mellitus and colorectal adenocarcinoma
(CRC) are common diseases worldwide (1,2). There
is considerable evidence that people with type 2 diabetes mellitus
(DM2) have an increased risk of developing several cancer types,
among them CRC. Meta-analysis results indicate that diabetic
patients have a 1.3-fold risk of developing CRC as well as a
1.3-fold risk of dying from it if compared to the general
population and to cancer patients without diabetes, respectively
(3,4).
Chronic hyperinsulinemia may increase the risk of
cancer because of the mitogenic and antiapoptotic effect of
insulin. Glucose-lowering therapies have been implicated in
modulating cancer risk in DM2 patients with controversial results
(4). Diabetes medications such as
insulin or secretagogues, which increase circulating insulin
levels, have been reported to increase cancer risk (5). Conversely, insulin sensitizers such as
metformin, the drug of choice in the DM2 treatment, seem to reduce
cancer risk by decreasing hyperinsulinemia (5). Metformin as well as acetylsalicylic
acid (ASA, aspirin), a drug prescribed for cardioprotection of
patients with or without DM2, also inhibit the mTOR signalling
pathway, which is commonly mutated and constitutively active in
many adenocarcinomas (6). Moreover,
a synergistic or additive inhibitory effect of metformin with ASA
on lung and prostate cancer cell survival due to depletion of de
novo lipogenesis was found by O'Brien at al (7).
This population-based study was aimed at
investigating prevalence of DM2 among CRC patients and survival for
CRC in patients with and without DM2.
Patients and methods
The present study was approved by the Ethics
Committee of the University of Trieste (Report number 37,
10/02/2012) and was conducted in accordance with the Declaration of
Helsinki protocols. Furthermore, clinical data were available only
for patients who signed an informed consent for research use of
their data.
All permanent residents of the northeastern Italian
province of Trieste (2013 population, 232,000) histologically
diagnosed with a first primary invasive adenocarcinoma of the colon
(excluding appendix) or of the rectum between January 1, 2004 and
December 31, 2007 were ascertained through the regional health
information system. Cases discovered at autopsy were excluded from
the analyses.
Medical records, pathology reports and the regional
health information system were examined for information on patients
(date of birth, sex, date of last follow-up or death, underlying
and contributing causes of death); on CRC (date and basis of
diagnosis, primary site, histological type, stage according to the
7th TNM classification (8), type and
place of treatments, local recurrence); on DM2 diagnosed according
to the criteria of the American Diabetes Association (9) and on any other chronic disease (type,
date and basis of diagnosis, treatments). All diabetic patients had
been diagnosed with the disease at least one year before CRC
detection, but we were not able to precisely quantify the duration
of DM2 or of treatment with antidiabetic drugs and ASA in the
majority of patients because their medical records were
incomplete.
Patients were followed-up from the date of CRC
diagnosis to death or December 31, 2013, whichever was the
earliest. None was lost to follow-up. Underlying and contributing
causes of death classified according to the International
Statistical Classification of Diseases, 10th revision (10) were known for all deceased
individuals.
Proportions were compared through Fisher exact test
(11). One-way analysis of variance
followed by Scheffé test (11) were
used to examine the significance of the differences between the
mean values of plasma parameters for the four groups in which
participants were allocated according to presence or absence of DM2
treated with metformin, and presence or absence of daily ASA
therapy.
Two parametric regression survival-time models, i.e.
Gompertz and log-logistic models (12), and Cox proportional-hazards
regression model (12) were used to
analyse possible factors affecting mortality from CRC. The test
proposed by Grambsch and Therneau (13) was used to evaluate the assumption
that hazard ratios in Cox analysis were proportional over time.
CRC-specific survival probabilities were computed by
the actuarial method (14) for each
group of patients defined by CRC stage, DM2 status, and metformin
and ASA use, and were compared with the logrank test (12). Relative survival probability
(14) of each group of patients was
calculated using the procedure described by Ederer et al
(15). Data on the number of
survivors in the province of Trieste between 2004 and 2015 by sex
and 5-year age groups were provided by the National Institute for
Statistics (16). Cornfield's
formulas (17) were applied to
estimate the limits of the 95% CI of the ratio of two relative
survivals. Chi-square test for heterogeneity (17) was used to compare relative survival
of different patient groups.
For each group of patients, Cox survival curves
adjusted for sex and age at CRC diagnosis were compared with the
likelihood ratio test (12).
Statistical analyses were performed using Stata/SE
12 (StataCorp, College Station, TX, USA).
Results
Between 2004 and 2007 in the province of Trieste a
first primary invasive CRC was diagnosed histologically in 690
individuals, 175 of whom were identified as having DM2. At the time
of CRC diagnosis, 156 DM2 patients had been under treatment with
metformin (105 with metformin only and 51 in association with
sulphonylureas, meglitinides or incretin mimetics), 6 with insulin,
4 with meglitinides, 3 with sulphonylureas and 6 with diet
alone.
The present study enrolled the 515 CRC patients
without DM2 (282 males and 233 females) and the 156 with DM2
treated with metformin (102 males and 54 females). The proportion
of males and females in these two groups differed significantly
(P=0.02).
At the time of CRC diagnosis, 71 (14%) patients
without DM2 and 39 (25%) with DM2 were taking ASA daily. The
proportion of patients taking ASA differed significantly between
diabetics and non-diabetics (P=0.002).
The 39 patients (27 males and 12 females) with DM2
and treated with metformin and ASA (Group 1), and the 71 patients
(44 males and the 27 females) without DM2 and treated with ASA
(Group 2) showed a median age at CRC diagnosis of 77 years (Group
1: 25th-75th percentile=71–83; Group 2: 25th-75th
percentile=69–82). The median age at diagnosis among the 117
patients (75 males and the 42 females) with DM2 treated with
metformin but not with ASA (Group 3) was 73 years (25th-75th
percentile=67–78), and it was 71 (25th-75th percentile=63–78) in
the 444 patients (238 males and 206 females) without DM2 and not
taking ASA (Group 4). The non-parametric test for trend (18) showed that age at CRC diagnosis tended
to decrease significantly across the four patient groups
(P<0.0001).
Of the 671 adenocarcinomas 654 were not otherwise
specified, 8 mucinous, 6 in adenomatous polyp and 3 in
tubulovillous adenoma. No adenocarcinomas in adenomatous polyps
and/or in tubulovillous adenoma were found in the patients
belonging to the previously described Groups 1 and 2, and no
mucinous ones were diagnosed in Group 4 patients. However, the
distribution of the histological types among the four groups of
patients did not differ statistically.
A total of 221 adenocarcinomas (33%) were within the
left-sided colon: 133 in the sigmoid colon, 70 in the descending
colon and 18 in the splenic flexure. There were 218 (32%)
right-sided lesions: 133 in the ascending colon, 46 in the caecum
and 39 in the hepatic flexure. One hundred and forty-one lesions
(21%) arose in the rectum, 52 (8%) in the rectosigmoid junction and
39 (6%) in the transverse colon.
Distribution of patients by group, colorectal
subsite, and TNM stage and substage for CRC is shown in Table I. No statistically significant
differences were found among the four groups.
 | Table I.Number of colorectal adenocarcinoma
patients by TNM stages and substages, colorectal subsites, DM2
status, and metformin and ASA use. |
Table I.
Number of colorectal adenocarcinoma
patients by TNM stages and substages, colorectal subsites, DM2
status, and metformin and ASA use.
|
|
|
|
|
|
| Stage II | Stage III | Stage IV |
|---|
|
|
|
|
|
|
|
|
|
|
|---|
| Patient group | DM2 | Metformin | ASA |
Subsitea | Stage I | A | B | C | Total | A | B | C | Total | A | B | Total |
|---|
| 1 (n=39) | Yes | Yes | Yes | Proximal | 2 | 2 | 0 | 1 | 3 | 1 | 8 | 0 | 9 | 1 | 0 | 1 |
|
|
|
|
| Distal | 6 | 9 | 0 | 0 | 9 | 1 | 7 | 1 | 9 | 0 | 0 | 0 |
| 2 (n=71) | No | No | Yes | Proximal | 10 | 12 | 1 | 0 | 13 | 2 | 6 | 0 | 8 | 3 | 0 | 3 |
|
|
|
|
| Distal | 10 | 7 | 1 | 1 | 9 | 1 | 13 | 1 | 15 | 3 | 0 | 3 |
| 3 (n=117) | Yes | Yes | No | Proximal | 8 | 12 | 4 | 1 | 17 | 2 | 18 | 4 | 24 | 5 | 0 | 5 |
|
|
|
|
| Distal | 20 | 13 | 2 | 3 | 18 | 2 | 16 | 1 | 19 | 5 | 1 | 6 |
| 4 (n=444) | No | No | No | Proximal | 34 | 38 | 11 | 9 | 58 | 7 | 45 | 13 | 65 | 11 | 4 | 15 |
|
|
|
|
| Distal | 84 | 66 | 8 | 8 | 82 | 8 | 69 | 8 | 85 | 15 | 6 | 21 |
| All patients
(n=671) |
|
|
| Proximal | 54 | 64 | 16 | 11 | 91 | 12 | 77 | 17 | 106 | 20 | 4 | 24 |
|
|
|
|
| Distal | 120 | 95 | 11 | 12 | 118 | 12 | 105 | 11 | 128 | 23 | 7 | 30 |
All patients had been treated in the three hospitals
of the province of Trieste according to up-to-date therapy
protocols. All stage I, II and III cancers had undergone
potentially curative treatments.
Local CRC recurrence was experienced by 62 patients
(9%) (Table II): 5, 6, 8 and 11%
among patients belonging to respectively Groups 1, 2, 3 and 4. The
proportion of local recurrences did not differed statistically
across the four patient groups.
| Table II.Number of patients with local
recurrence of colorectal cancer by TNM stages, DM2, and metformin
and ASA use. |
Table II.
Number of patients with local
recurrence of colorectal cancer by TNM stages, DM2, and metformin
and ASA use.
| Patient group | DM2 | Metformin | ASA | Number of
patients | Stage I | Stage II | Stage III | Stage IV |
|---|
|
1 | Yes | Yes | Yes | Total |
8 | 12 | 18 | 1 |
|
|
|
|
| With local
recurrence |
1 |
1 |
0 | 0 |
|
|
|
|
| % | 13 |
8 |
0 | 0 |
|
2 | No | No | Yes | Total | 20 | 22 | 23 | 6 |
|
|
|
|
| With local
recurrence |
2 |
0 |
2 | 0 |
|
|
|
|
| % | 10 |
0 |
9 | 0 |
|
3 | Yes | Yes | No | Total | 28 | 35 | 43 | 11 |
|
|
|
|
| With local
recurrence |
3 |
1 |
5 | 0 |
|
|
|
|
| % | 11 |
3 | 12 | 0 |
|
4 | No | No | No | Total | 118 | 140 | 150 | 36 |
|
|
|
|
| With local
recurrence |
7 | 18 | 20 | 2 |
|
|
|
|
| % |
6 | 13 | 13 | 6 |
| All patients |
|
|
| Total | 174 | 209 | 234 | 54 |
|
|
|
|
| With local
recurrence | 13 | 20 | 27 | 2 |
|
|
|
|
| % |
7 | 10 | 12 | 4 |
Table III shows the
mean values of four admission plasma parameters. Patients belonging
to Group 3 showed a mean value of glucose and triglycerides
significatively higher than those belonging to the other three
groups and than those belonging to Groups 2 and 4, respectively.
Total cholesterol and HDL cholesterol were higher in Group 2 with a
statistically significant difference between Groups 2 and 3 for HDL
cholesterol.
| Table III.Mean values of admission plasma
parameters of the 671 study participants by patient groups. |
Table III.
Mean values of admission plasma
parameters of the 671 study participants by patient groups.
|
|
|
|
| Mean value of
admission plasma parameter (mg/dl) |
|---|
|
|
|
|
|
|
|---|
| Patient group | DM2 | Metformin | ASA |
Glucosea
SD |
Triglyceridesb SD | Total cholesterol
SD | HDL
cholesterolc SD |
|---|
| 1 (n=39) | Yes | Yes | Yes | 97 | 135 | 185 | 46 |
|
|
|
|
| 22 | 62 | 46 | 16 |
| 2 (n=71) | No | No | Yes | 93 | 106 | 188 | 53 |
|
|
|
|
| 12 | 34 | 46 | 18 |
| 3 (n=117) | Yes | Yes | No | 107 | 140 | 185 | 46 |
|
|
|
|
| 22 | 84 | 52 | 15 |
| 4 (n=444) | No | No | No | 94 | 113 | 187 | 50 |
|
|
|
|
| 13 | 54 | 60 | 16 |
Of the 515 CRC patients without DM2, 339 (66%)
suffered from 494 chronic diseses other than CRC: 1 chronic disease
in 217 patients, 2 in 99, 3 in 15, 4 in 6 and 5 in 2 patients. The
two most frequent categories of comorbidities were cardiovascular
diseases (287 patients, 56%) and invasive malignant tumours (103
patients, 20%). The most frequent malignancy was prostate cancer
among males (32 patients) and breast cancer among females (13
patients).
Other than CRC and DM2 229 chronic diseases were
detected in 142 out of 156 diabetic patients (91%): 1 chronic
disease in 79 patients, 2 in 43, 3 in 16, and 4 in 4 patients.
Cardiovascular disases (135 patients, 87%) and invasive cancers (38
patients, 24%) were the two most frequent disease categories.
Prostate cancer (8 patients) and breast cancer (5 patients) were
the most frequent malignancies among males and females,
respectively.
Table IV shows the
distribution of chronic diseases other than CRC and DM2 among the
four patient groups. Diabetic patients belonging to Groups 1 and 3
had a significantly higher proportion of cardiovascular diseases
and genitourinary system diseases, namely chronic kidney disease,
than nondiabetic patients (87 vs. 56%, P<0.0001 and 13 vs. 4%,
P<0.0001, respectively). Moreover, a significantly higher
proportion of respiratory system diseases was found among patients
belonging to Group 1 compared with those belonging to Groups 3
(P=0.007) and 4 (P=0.002).
| Table IV.Chronic diseases other than
colorectal cancer and DM2 diagnosed in the 671 study participants
by patient groups. |
Table IV.
Chronic diseases other than
colorectal cancer and DM2 diagnosed in the 671 study participants
by patient groups.
|
|
| Patient
groupa |
|---|
|
|
|
|
|---|
| Disease category
(ICD-10 codes)b |
| 1 (n=39) | 2 (n=71) | 3 (n=117) | 4 (n=444) |
|---|
| Invasive malignant
neoplasms (C00-C17, C18.1, C21-C96) | Number | 9 | 19 | 29 | 84 |
|
| % | 23 | 27 | 25 | 19 |
| Diseases of the
blood and disorders involving the immune mechanism (D50-D89) | Number | 1 | 1 | 1 | 6 |
|
| % | 3 | 1 | 1 | 1 |
| Endocrine,
nutritional and metabolic diseases (E00-E10, E15-E90) | Number | 2 | 3 | 7 | 12 |
|
| % | 5 | 4 | 6 | 3 |
| Mental and
behavioural disorders (F00-F99) | Number | 0 | 3 | 3 | 7 |
|
| % | 0 | 4 | 3 | 2 |
| Diseases of the
nervous system (G00-99) | Number | 0 | 0 | 2 | 6 |
|
| % | 0 | 0 | 2 | 1 |
| Diseases of the
circulatory system (I00-I99)c | Number | 32 | 37 | 103 | 250 |
|
| % | 82 | 52 | 88 | 56 |
| Diseases of the
respiratory system (J00-J99)d | Number | 8 | 5 | 6 | 23 |
|
| % | 21 | 7 | 5 | 5 |
| Diseases of the
digestive system (K00-K99) | Number | 0 | 2 | 4 | 12 |
|
| % | 0 | 3 | 3 | 3 |
| Diseases of the
musculoskeletal system and connective tissue (M00-M99) | Number | 0 | 1 | 1 | 3 |
|
| % | 0 | 1 | 1 | 1 |
| Diseases of the
genitourinary system (N00-N99)e | Number | 7 | 7 | 14 | 13 |
|
| % | 18 | 10 | 12 | 3 |
Cox proportional-hazards regression analysis
(Table V) showed that factors
resulted in a higher hazard and therefore a shorter survival time
controlling for the other factors were CRC stage [hazard ratio
(HR)=1.98, 95% CI=1.67–2.34, P<0.0001], admission plasma HDL
cholesterol lower than 40 mg/dl (HR=1.41, 95% CI=1.02–1.95,
P=0.04), patient group (HR=1.21, 95% CI=1.03–1.44, P=0.02) and age
at CRC diagnosis (HR=1.04, 95% CI=1.02–1.05, P<0.0001). However,
after testing the proportional hazard assumption, i.e. the null
hypothesis of a zero slope in the regression, the assumption held
for a model with covariates CRC stage and patient group
(χ2=0.79, degrees of freedom=2, P=0.7). Gompertz and
log-logistic analyses produced results similar to those reported in
Table V.
| Table V.Cox proportional-hazards regression
analysis of possible factors affecting mortality from CRC among the
671 study participants. |
Table V.
Cox proportional-hazards regression
analysis of possible factors affecting mortality from CRC among the
671 study participants.
| Factors | Hazard ratio | 95% CI | P-value |
|---|
| CRC stage | 1.98 | 1.67–2.34 | <0.0001 |
| Stage
II | 1.24 | 0.79–1.94 | 0.4 |
| Stage
III | 2.70 | 1.81–4.04 | <0.0001 |
| Stage
IV | 6.94 | 4.14–11.63 | <0.0001 |
| Number of
comorbidities | 1.94 | 0.58–6.51 | 0.3 |
| Local recurrence of
CRC (0=no, 1=yes) | 1.49 | 0.99–2.23 | 0.06 |
| Sex (1=male,
2=female) | 1.22 | 0.91–1.63 | 0.2 |
| Patient
groupa | 1.21 | 1.03–1.44 | 0.02 |
| Group
2 | 3.12 | 1.22–8.00 | 0.02 |
| Group
3 | 3.83 | 1.58–9.29 | 0.003 |
| Group
4 | 3.37 | 1.44–7.89 | 0.005 |
| CRC
subsiteb (1=proximal,
2=distal) | 1.05 | 0.79–1.39 | 0.8 |
| Age at CRC
diagnosis (years) | 1.04 | 1.02–1.05 | <0.0001 |
| CRC-directed
therapyc | 1.03 | 0.88–1.21 | 0.7 |
| Admission plasma
glucose (mg/dl) | 1.01 | 0.99–1.02 | 0.1 |
|
≥100 | 1.00 | 0.72–1.39 | 1.0 |
| Admission plasma
total cholesterol (mg/dl) | 1.00 | 0.99–1.00 | 0.6 |
|
200–239 | 0.76 | 0.51–1.12 | 0.2 |
|
≥240 | 0.79 | 0.49–1.26 | 0.3 |
| Admission plasma
triglycerides (mg/dl) | 1.00 | 0.99–1.00 | 0.7 |
|
150–199 | 1.07 | 0.64–1.79 | 0.8 |
|
≥200 | 0.80 | 0.43–1.51 | 0.5 |
| Admission plasma
HDL cholesterol (mg/dl) | 0.98 | 0.97–0.99 | 0.005 |
|
<40 | 1.41 | 1.02–1.95 | 0.04 |
| Comorbidity (0=no,
1=yes) | 0.96 | 0.50–1.85 | 0.9 |
| Diseases of the
genitourinary system (0=no, 1=yes) | 0.96 | 0.30–3.05 | 0.9 |
| Endocrine,
nutritional and metabolic disease other than type 2 diabetes
mellitus (0=no, 1=yes) | 0.67 | 0.21–2.12 | 0.5 |
| Invasive malignant
neoplasms other than CRC (0=no, 1=yes) | 0.61 | 0.18–2.02 | 0.4 |
| Diseases of the
digestive system (0=no, 1=yes) | 0.60 | 0.16–2.23 | 0.4 |
| Diseases of the
circulatory system (0=no, 1=yes) | 0.57 | 0.17–1.98 | 0.4 |
| Diseases of the
blood and disorders involving the immune mechanism (0=no,
1=yes) | 0.47 | 0.11–2.06 | 0.3 |
| Diseases of the
respiratory system (0=no, 1=yes) | 0.44 | 0.13–1.51 | 0.2 |
| Diseases of the
nervous system (0=no, 1=yes) | 0.43 | 0.09–2.05 | 0.3 |
| Mental and
behavioural disorders (0=no, 1=yes) | 0.43 | 0.08–2.25 | 0.3 |
| Diseases of the
musculoskeletal system and connective tissue (0=no, 1=yes) | 0.24 | 0.02–2.52 | 0.2 |
Five-year CRC-specific and relative survival
probabilities stratified by TNM stages and patient groups are shown
in Table VI. Cancer-specific
survival for stage III CRC was significantly higher in the 18
diabetic patients treated with metformin and ASA (Group 1) than in
the 43 diabetic patients treated with metformin but not ASA (Group
3) (P=0.008), and in the 150 nondiabetic patients not taking ASA
(Group 4) (P=0.03). Patients belonging to Group 1 with stage III
CRC showed a five-year relative survival 3.5-fold higher (95%
CI=1.4–8.3, P=0.003) than those belonging to Group 3. On the other
hand, the ratio of relative survivals between Group 2 and Group 4
patients with stage III CRC was 1.0 (95% CI=0.5–1.9, P=0.8). To a
lesser extent, five-year cancer-specific and relative survivals for
stage II CRC were better in DM2 patients on metformin and aspirin
therapy compared with Groups 2, 3 and 4. However, survival was
similar across the four Groups for stages I and IV. No
statistically significant differences in five-year CRC-specific and
relative survival probabilities between males and females belonging
to the same Groups were found across the four TNM stages.
| Table VI.Number of CRC patients, number of
deaths due to CRC and to any cause, actuarial 5-year CRC-specific
and relative survival probabilities, by TNM stages, type 2 diabetes
mellitus status, and metformin and acetylsalicylic acid use. |
Table VI.
Number of CRC patients, number of
deaths due to CRC and to any cause, actuarial 5-year CRC-specific
and relative survival probabilities, by TNM stages, type 2 diabetes
mellitus status, and metformin and acetylsalicylic acid use.
|
|
|
|
| Stage I | Stage II | Stage III | Stage IV |
|---|
|
|
|
|
|
|
|
|
|
|---|
|
|
|
|
|
| No. of deaths | Survival, 5-year
(%) |
| No. of deaths | Survival, 5-year
(%) |
| No. of deaths | Survival, 5-year
(%) |
| No. of deaths | Survival, 5-year
(%) |
|---|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|---|
| Patient group | DM2 | Metformin | ASA | n | CRC | All causes | Specific (95%
CI) | Relative (95%
CI) | n | CRC | All causes | Specific (95%
CI) | Relative (95%
CI) | n | CRC | All causes |
Specifica (95% CI) |
Relativeb (95% CI) | n | CRC | All causes | Specific (95%
CI) | Relative (95%
CI) |
|---|
| 1 (n=39) | Yes | Yes | Yes | 8 | 1 | 5 | 80 | 73 | 12 | 1 | 5 | 91 | 109 | 18 | 3 | 6 | 83 | 101 | 1 | 1 | 1 | 0 | 0 |
|
|
|
|
|
|
|
| (20–97) | (22–123) |
|
|
| (52–99) | (74–145) |
|
|
| (56–94) | (76–126) |
|
|
| (−) | (−) |
| 2 (n=71) | No | No | Yes | 20 | 3 | 7 | 90 | 106 | 22 | 6 | 11 | 69 | 76 | 23 | 10 | 15 | 57 | 55 | 6 | 4 | 6 | 20 | 23 |
|
|
|
|
|
|
|
| (66–97) | (79–133) |
|
|
| (43–85) | (47–104) |
|
|
| (33–75) | (31–78) |
|
|
| (1–59) | (0–64) |
| 3 (n=117) | Yes | Yes | No | 28 | 7 | 15 | 76 | 75 | 35 | 9 | 19 | 73 | 62 | 43 | 20 | 36 | 44 | 29 | 11 | 7 | 9 | 29 | 25 |
|
|
|
|
|
|
|
| (54–88) | (53–97) |
|
|
| (54–85) | (43–81) |
|
|
| (26–60) | (13–45) |
|
|
| (6–58) | (0–56) |
| 4 (n=444) | No | No | No | 118 | 23 | 40 | 81 | 89 | 140 | 32 | 53 | 80 | 85 | 150 | 65 | 92 | 55 | 55 | 36 | 21 | 34 | 25 | 13 |
|
|
|
|
|
|
|
| (76–90) | (79–99) |
|
|
| (72–86) | (75–94) |
|
|
| (47–63) | (45–65) |
|
|
| (10–44) | (1–26) |
| All patients |
|
|
| 174 | 34 | 67 | 82 | 88 | 209 | 48 | 88 | 78 | 82 | 234 | 98 | 149 | 56 | 54 | 54 | 33 | 50 | 25 | 16 |
| (n=671) |
|
|
|
|
|
| (75–87) | (79–96) |
|
|
| (72–83) | (74–90) |
|
|
| (49–63) | (47–62) |
|
|
| (12–39) | (5–27) |
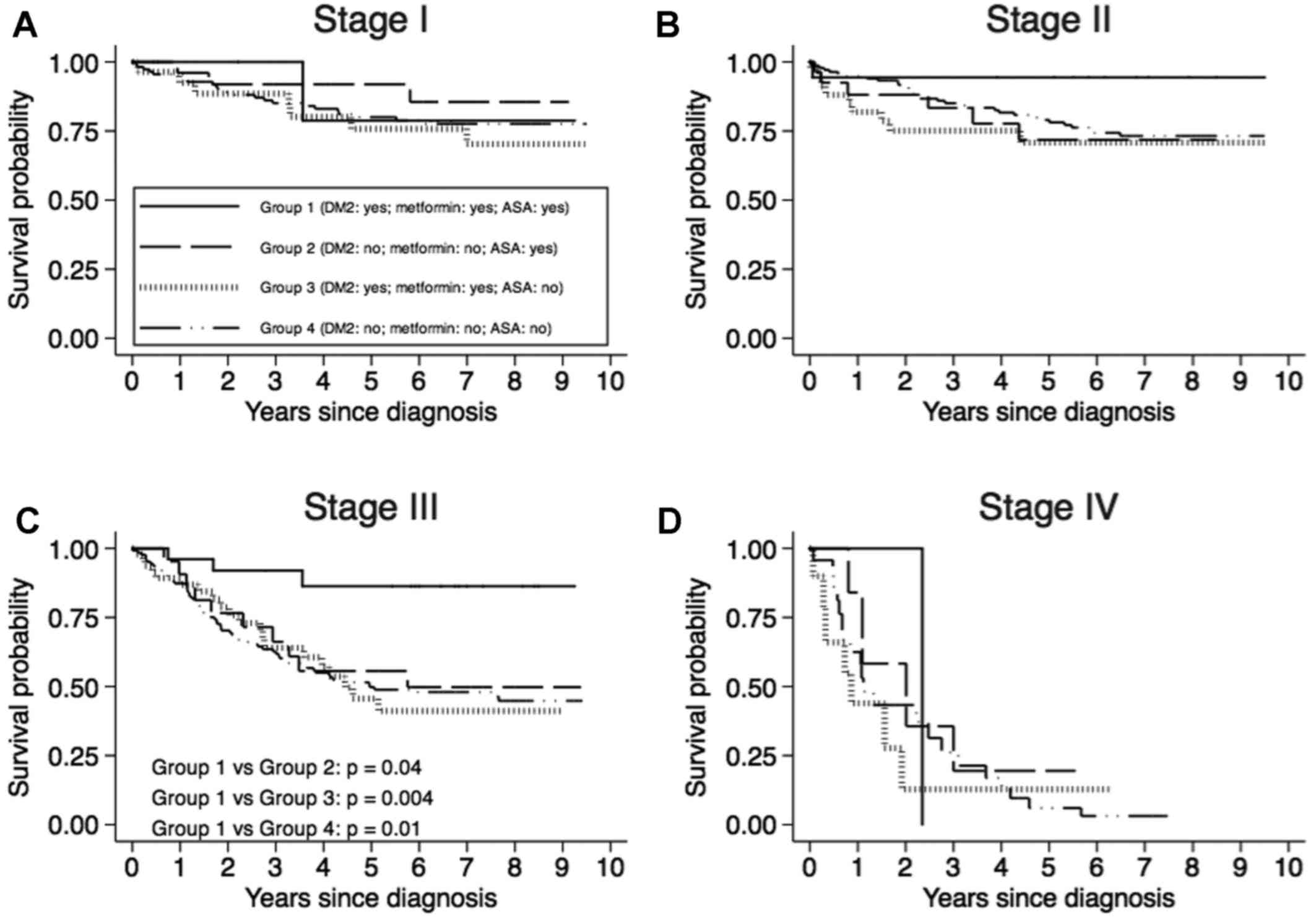
For each TNM stage and for each patient group,
CRC-specific survival curves adjusted for sex and age at diagnosis
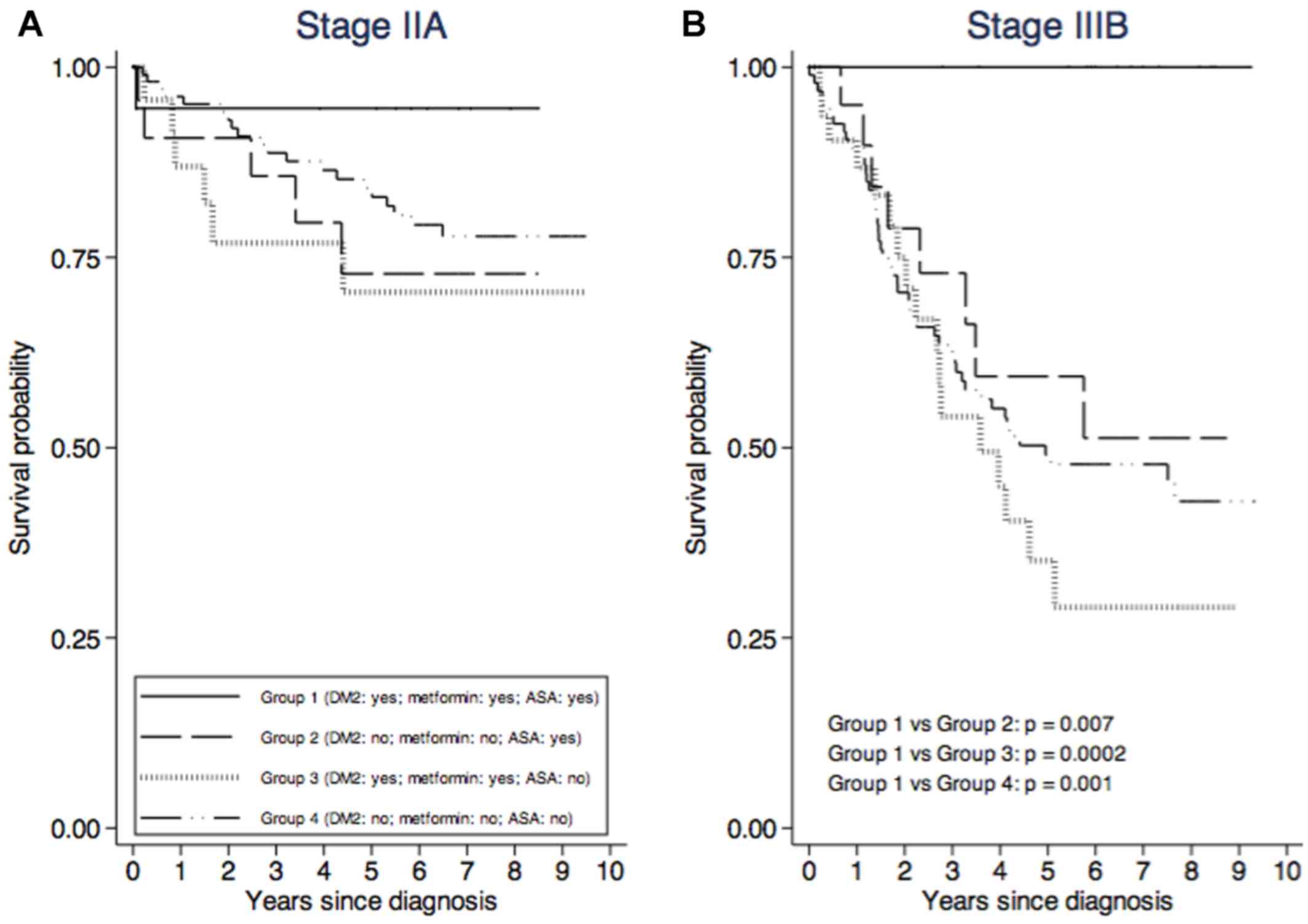
are shown in Fig. 1. It was possible
to draw survival curves for TNM substages IIA and IIIB only
(Fig. 2) because of the small number
of patients classified in the other substages (Table I). Survival for stage III CRC was
significantly higher among patients belonging to Group 1 than among
those belonging to Group 2 (P=0.04), Group 3 (P=0.004) and Group 4
(P=0.01). The same was true for stage IIIB (Fig. 2). A not statistically significant
higher survival for stages II (Fig.
1) and IIA (Fig. 2) was shown by
Group 1 patients compared with those of the other three groups.
Discussion
We carried out an observational study on colorectal
cancer patients diagnosed between 2004 and 2007 in the Italian
province of Trieste. Information on the duration of DM2 and on
treatment with antidiabetic drugs and ASA, and on body mass index
(BMI) was limited (for BMI it was available only in 10% of
patients). This missing information is, admittedly, a weak point in
our study since those data would have improved it. Nonetheless, in
the limited number of cases where body mass index was available, a
similar distribution of this index was observed between diabetic
and nondiabetic patients (P=0.3) (data not shown) in agreement with
Rosato et al (19). Our group
of diabetic patients was homogeneous because only patients treated
with metformin were enrolled in the study, given that the aim of
the study was not to compare the efficacy of metformin with other
treatments for DM2.
No statistically significant difference in the
proportion of diabetic and nondiabetic patients was found across
the four TNM stages for CRC in agreement with Siddiqui et al
(20) who reported no differences in
stage at presentation in patients with a well-controlled DM2 and
nondiabetic controls.
A positive association between DM2 and proximal
colon cancer had already been observed, albeit not homogenously, in
several studies (19,21,22), but
in our study we were not able to confirm this in our study. The
distribution of colon subsites was comparable in CRC patients with
and without DM2. A possible explanation could be the selection
criterion of DM2 patients because only those treated with metformin
were included.
Increased plasma triglycerides and reduced HDL
cholesterol are the main quantitative lipid abnormalities in
diabetic dyslipidemia (23).
Diabetic patients who take metformin are patients with more severe
diabetes who need pharmacological therapy. In patients with
insulin-resistant diabetes treated with metformin, there is the
so-called atherogenic dyslipidemia, characterized by fasting
hypertriglyceridemia, which is usually associated with low levels
of HDL cholesterol and high levels of small and dense LDL particles
(24). In our study, the values of
total and HDL cholesterol was higher in patients without DM2 taking
ASA, while glucose and triglycerides were higher in DM2 patients
not on ASA treatment. This is a possible consequence of ASA intake,
which lowers plasma triglycerides (25) and suppresses the abnormal lipid
metabolism (26). Higher levels of
HDL cholesterol in nondiabetic patients taking ASA can also be
related to the fact that diabetic patients have significantly lower
levels of HDL than nondiabetic patients (27).
In the present study cardiovascular diseases,
malignancies other than CRC and chronic kidney diseases are the
most frequent comorbidities in DM2 patients in agreement with other
studies (28,29). Diabetes mellitus is, indeed, a major
risk factor for cardiovascular diseases, whose prevalence is twice
as high in males and even four times more frequent in females
(30).
Among the variables affecting survival, CRC stage
and plasma HDL cholesterol lower than 40 mg/dl had a negative
effect on survival. Higher stage at diagnosis is, of course,
related to a worse prognosis. As regards HDL cholesterol, our data
are indirectly supported by Notanicola and colleagues, who reported
that the presence of metastases in CRC patients was associated to
higher levels of LDL cholesterol over HDL cholesterol ratio,
irrespective of sex and BMI (31).
Additionally, the relationship between Serum Amyloid A and HDL
particles can explain the inverse relationship between HDL
cholesterol levels and cancer (32).
Daily ASA intake has been shown to reduce incidence
and mortality from CRC (33,34). In the present study, the protective
effect of ASA in both diabetic and nondiabetic patients is
suggested by the older median age at CRC diagnosis of patients
taking ASA. However, in agreement with the results of Din et
al (33), no influence of ASA
alone on cancer-specific and relative survival was observed.
Diabetic patients treated with metformin showed a
lower incidence of CRC (35–37) and mortality from CRC (38–40). In
the present study, diabetic patients taking ASA and metformin have
both higher five-year cancer-specific and relative survival for
stage II and III CRC compared with diabetic patients not taking ASA
and to nondiabetic patients with or without ASA intake. These
results differ from those obtained by Mei et al (38), Du et al (39) and Ramjeesingh et al (40) who showed the protective effect of
metformin on CRC patient mortality. On the other hand, Zanders and
colleagues (41) did not find any
survival improvement in CRC patients taking metformin or ASA.
Our results indirectly support the hypothesis of a
possible interaction between ASA and metformin in anticancer
activity, even though those drugs are not labelled for cancer
therapy. O'Brien et al (7)
showed that salicylate and metformin reduce synergistically or
additively the clonogenic survival of prostate and lung cancer
cells by inhibiting de novo lipogenesis. Furthermore, the
combination of metformin and 5-ASA, which displays a mechanism
similar to ASA in inhibiting COX-2 enzyme, has recently been shown
to increase cell death in CRC cell lines (42). Nonetheless, we cannot exclude the
possibility that metformin alone or in combination with ASA could
enhance the chemotherapeutical activity of 5-fluorouracil (5-FU),
since the major benefit of metformin and ASA was observed in stage
III CRC patients, who underwent adjuvant 5-FU chemotherapy. A
synergistic effect of metformin in combination with 5-FU on CRC
stem cell proliferation has already been hypothesized (43).
The findings reported are promising but, like all
descriptive epidemiological studies, our study was exploratory and
aimed at generating hypotheses. Therefore, randomized controlled
trials investigating the combined effect of metformin and ASA on
CRC patient survival are needed to confirm or refute our
findings.
Acknowledgements
We wish to thank Dr C.J. Garwood for his language
editing work on the manuscript.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Binefa G, Rodríguez-Moranta F, Teule A and
Medina-Hayas M: Colorectal cancer: From prevention to personalized
medicine. World J Gastroenterol. 20:6786–6808. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Guariguata L, Whiting DR, Hambleton I,
Beagley J, Linnenkamp U and Shaw JE: Global estimates of diabetes
prevalence for 2013 and projections for 2035. Diabetes Res Clin
Pract. 103:137–149. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Renehan AG, Yeh HC, Johnson JA, Wild SH,
Gale EA and Møller H; Diabetes and cancer research consortium, :
Diabetes and cancer (2): Evaluating the impact of diabetes on
mortality in patients with cancer. Diabetologia. 55:1619–1632.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Johnson JA, Carstensen B, Witte D, Bowker
SL, Lipscombe L and Renehan AG; Diabetes and cancer research
consortium, : Diabetes and cancer: Evaluating the temporal
relationship between type 2 diabetes and cancer incidence.
Diabetologia. 55:1607–1618. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Park HK: Metformin and cancer in type 2
diabetes. Diabetes Metab J. 37:113–116. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Din FV, Valanciute A, Houde VP, Zibrova D,
Green KA, Sakamoto K, Alessi DR and Dunlop MG: Aspirin inhibits
mTOR signaling, activates AMP-activated protein kinase, and induces
autophagy in colorectal cancer cells. Gastroenterology.
142:1504–1515 e3. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
O'Brien AJ, Villani LA, Broadfield LA,
Houde VP, Galic S, Blandino G, Kemp BE, Tsakiridis T, Muti P and
Steinberg GR: Salicylate activates AMPK and synergizes with
metformin to reduce the survival of prostate and lung cancer cells
ex vivo through inhibition of de novo lipogenesis. Biochem J.
469:177–187. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Edge S, Byrd DR, Compton CC, Fritz AG,
Greene FL and Trotti A: AJCC Cancer Staging Manual.
Springer-Verlag; New York: 2010
|
|
9
|
American Diabetes Association, . Diagnosis
and classification of diabetes mellitus. Diabetes Care. 37 Suppl
1:S81–S90. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Word Health Organization, . ICD-10
International statistical classification of diseases and related
health problems. World Health Organization; Geneva: 2011
|
|
11
|
Armitage P and Berry G: Statistical
methods in medical research. 2nd. Oxford, Boston, Blackwell
Scientific, Chicago, III, Distributors, USA: Year Book Medical
Publishers, England; 1987
|
|
12
|
Kalbfleisch JD and Prentice RL: The
statistical analysis of failure time data. John Wiley; New York:
1980
|
|
13
|
Grambsch PM and Therneau TM: Proportional
hazards tests and diagnostics based on weighted residuals.
Biometrika. 81:515–526. 1994. View Article : Google Scholar
|
|
14
|
Estève J, Benhamou E and Raymond L:
Statistical methods in cancer research. Volume IV. Descriptive
epidemiology. IARC Sci Publ. 1994:3021994.
|
|
15
|
Ederer F, Axtell LM and Cutler SJ: The
relative survival rate: A statistical methodology. Natl Cancer Inst
Monogr. 6:101–121. 1961.PubMed/NCBI
|
|
16
|
Patruno V, Venturi M and Roberto S:
Demografia in cifre-Tavole di Mortalità. Available from ISTAT.
http://www.demo.istat.it/tvm2016
|
|
17
|
Breslow NE and Day NE: Statistical methods
in cancer research. Volume II-The design and analysis of cohort
studies. IARC Sci Publ. 1–406. 1987.
|
|
18
|
Cuzick J: A Wilcoxon-type test for trend.
Stat Med. 4:87–90. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Rosato V, Tavani A, Gracia-Lavedan E,
Guinó E, Castaño-Vinyals G, Villanueva CM, Kogevinas M, Polesel J,
Serraino D, Pisa FE, et al: Type 2 diabetes, antidiabetic
medications and colorectal cancer risk: Two case-control studies
from italy and spain. Front Oncol. 6:2102016. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Siddiqui AA, Spechler SJ, Huerta S, Dredar
S, Little BB and Cryer B: Elevated HbA1c is an independent
predictor of aggressive clinical behavior in patients with
colorectal cancer: A case-control study. Dig Dis Sci. 53:2486–2494.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Campbell PT: The role of diabetes and
diabetes treatments in colorectal cancer mortality, incidence and
survival. Curr Nutr Rep. 2:37–47. 2013. View Article : Google Scholar
|
|
22
|
Peeters PJ, Bazelier MT, Leufkens HG, de
Vries F and De Bruin ML: The risk of colorectal cancer in patients
with type 2 diabetes: Associations with treatment stage and
obesity. Diabetes Care. 38:495–502. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Vergès B: Pathophysiology of diabetic
dyslipidaemia: Where are we? Diabetologia. 58:886–899. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Sirtori CR, Calabresi L, Pisciotta L,
Cattin L, Pauciullo P, Montagnani M, Manzato E, Bittolo Bon G and
Fellin R: Effect of statins on LDL particle size in patients with
familial combined hyperlipidemia: A comparison between atorvastatin
and pravastatin. Nutr Metab Cardiovasc Dis. 15:47–55. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
van Diepen JA, Vroegrijk IO, Berbée JF,
Shoelson SE, Romijn JA, Havekes LM, Rensen PC and Voshol PJ:
Aspirin reduces hypertriglyceridemia by lowering VLDL-triglyceride
production in mice fed a high-fat diet. Am J Physiol Endocrinol
Metab. 301:E1099–E1107. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Yang G, Wang Y, Feng J, Liu Y, Wang T,
Zhao M, Ye L and Zhang X: Aspirin suppresses the abnormal lipid
metabolism in liver cancer cells via disrupting an NFκB-ACSL1
signaling. Biochem Biophys Res Commun. 486:827–832. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Eliasson B, Gudbjörnsdottir S, Zethelius
B, Eeg-Olofsson K and Cederholm J; National diabetes register
(NDR), : LDL-cholesterol versus non-HDL-to-HDL-cholesterol ratio
and risk for coronary heart disease in type 2 diabetes. Eur J Prev
Cardiol. 21:1420–1428. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Middleton RJ, Foley RN, Hegarty J, Cheung
CM, McElduff P, Gibson JM, Kalra PA, O'Donoghue DJ and New JP: The
unrecognized prevalence of chronic kidney disease in diabetes.
Nephrol Dial Transplant. 21:88–92. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Dörhöfer L, Lammert A, Krane V, Gorski M,
Banas B, Wanner C, Krämer BK, Heid IM and Böger CA; DIACORE Study
Group, : Study design of DIACORE (DIAbetes COhoRtE) a cohort study
of patients with diabetes mellitus type 2. BMC Med Genet.
14:252013. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Casanova F, Adingupu DD, Adams F, Gooding
KM, Looker HC, Aizawa K, Dove F, Elyas S, Belch JJF, Gates PE, et
al: The impact of cardiovascular co-morbidities and duration of
diabetes on the association between microvascular function and
glycaemic control. Cardiovasc Diabetol. 16:1142017. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Notarnicola M, Altomare DF, Correale M,
Ruggieri E, D'Attoma B, Mastrosimini A, Guerra V and Caruso MG:
Serum lipid profile in colorectal cancer patients with and without
synchronous distant metastases. Oncology. 68:371–374. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Gomaraschi M, Ossoli A, Favari E, Adorni
MP, Sinagra G, Cattin L, Veglia F, Bernini F, Franceschini G and
Calabresi L: Inflammation impairs eNOS activation by HDL in
patients with acute coronary syndrome. Cardiovasc Res. 100:36–43.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Din FV, Theodoratou E, Farrington SM,
Tenesa A, Barnetson RA, Cetnarskyj R, Stark L, Porteous ME,
Campbell H and Dunlop MG: Effect of aspirin and NSAIDs on risk and
survival from colorectal cancer. Gut. 59:1670–1679. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Sehdev A and O'Neil BH: The role of
aspirin, vitamin D, Exercise, diet, statins and metformin in the
prevention and treatment of colorectal cancer. Curr Treat Options
Oncol. 16:432015. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Zhang ZJ, Zheng ZJ, Kan H, Song Y, Cui W,
Zhao G and Kip KE: Reduced risk of colorectal cancer with metformin
therapy in patients with type 2 diabetes: A meta-analysis. Diabetes
Care. 34:2323–2328. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Liu F, Yan L, Wang Z, Lu Y, Chu Y, Li X,
Liu Y, Rui D, Nie S and Xiang H: Metformin therapy and risk of
colorectal adenomas and colorectal cancer in type 2 diabetes
mellitus patients: A systematic review and meta-analysis.
Oncotarget. 8:16017–16026. 2017.PubMed/NCBI
|
|
37
|
Nie Z, Zhu H and Gu M: Reduced colorectal
cancer incidence in type 2 diabetic patients treated with
metformin: A meta-analysis. Pharm Biol. 54:2636–2642. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Mei ZB, Zhang ZJ, Liu CY, Liu Y, Cui A,
Liang ZL, Wang GH and Cui L: Survival benefits of metformin for
colorectal cancer patients with diabetes: A systematic review and
meta-analysis. PLoS One. 9:e918182014. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Du L, Wang M, Kang Y, Li B, Guo M, Cheng Z
and Bi C: Prognostic role of metformin intake in diabetic patients
with colorectal cancer: An updated qualitative evidence of cohort
studies. Oncotarget. 8:26448–26459. 2017.PubMed/NCBI
|
|
40
|
Ramjeesingh R, Orr C, Bricks CS, Hopman WM
and Hammad N: A retrospective study on the role of diabetes and
metformin in colorectal cancer disease survival. Curr Oncol.
23:e116–e122. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Zanders MM, van Herk-Sukel MP, Vissers PA,
Herings RM, Haak HR and van de Poll-Franse LV: Are metformin,
statin and aspirin use still associated with overall mortality
among colorectal cancer patients with diabetes if adjusted for one
another? Br J Cancer. 113:403–410. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Saber MM, Galal MA, Ain-Shoka AA and
Shouman SA: Combination of metformin and 5-aminosalicylic acid
cooperates to decrease proliferation and induce apoptosis in
colorectal cancer cell lines. BMC Cancer. 16:1262016. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Zhang Y, Guan M, Zheng Z, Zhang Q, Gao F
and Xue Y: Effects of metformin on CD133+ colorectal cancer cells
in diabetic patients. PLoS One. 8:e812642013. View Article : Google Scholar : PubMed/NCBI
|