Introduction
Brain metastases (BM) are particularly frequent in
lung cancer cases (40–50%), and their presence considerably worsens
the prognosis of the patients (1).
It has been estimated that 25% of patients with non-small-cell lung
cancer (NSCLC) also suffer from BM (2). Patients with BM often experience severe
neurological symptoms and a poor quality of life (QoL). The overall
survival (OS) of patients with BM from NSCLC is <3–6 months
without treatment (3), and the
1-year survival rate is <20% (4).
Whole-brain radiotherapy (WBRT) may prolong survival, it is the
standard of care for patients with BM, and it is crucial for the
control of distant microscopic metastases (5). However, approximately half of patients
with BM experience intracranial progression within a few months of
RT (6). Chemotherapy has also
exhibited limited efficacy in the treatment of BM due to the
presence of the blood-brain barrier (7). The efficacy of tyrosine kinase
inhibitors (TKIs), such as erlotinib or gefitinib, in central
nervous system metastasis is modest, due to the limited
cerebrospinal fluid penetration (8,9);
therefore, TKIs are generally used only for lung adenocarcinoma
with epidermal growth factor receptor mutations (9). Temozolomide (TMZ) is able to cross the
blood-brain barrier and has exhibited efficacy against a number of
cancers with BM, including NSCLC (10). The efficacy of TMZ in patients with
metastatic lung cancer has been previously demonstrated (11,12). In
addition to TMZ, certain alkylating agents, such as cisplatin, may
exert an effect on BM by crossing the blood-brain barrier (5). TMZ with cisplatin has been confirmed to
be an active and well-tolerated combination in patients with BM
(13). The present study was
designed to assess the efficacy and the associated QoL of WBRT
combined with TMZ in patients with BM from NSCLC.
Patients and methods
Patients
Between January 2013 and July 2015, 77 cases of lung
cancer patients with BM were selected and divided into two groups
(details shown in Table I). The
patients were required to meet the following criteria: i)
First-time patients with pathologically diagnosed NSCLC and with no
other prior tumors, and with a Karnofsky performance status (KPS)
score ≥70; ii) BM confirmed by magnetic resonance imaging (MRI)
with at least 3 evaluations of cranial lesions and no previously
administered cranial RT; iii) 18< age <75 years; iv) no other
serious medical conditions, an expected survival >3 months and
adequate renal, hepatic and hematological function. All the
patients provided written informed consent, and the study protocol
was approved by the Ethics Committee of the Qianfoshan Hospital
Affiliated to Shandong University (Jinan, China).
 | Table I.General patient characteristics. |
Table I.
General patient characteristics.
| Characteristics | Group 1 | Group 2 |
|---|
| N | 40 | 37 |
| Sex |
|
|
| Male | 26 | 23 |
|
Female | 14 | 14 |
| Median age,
years | 57 | 61 |
| KPS score |
|
|
| ≤80 | 15 | 10 |
|
>80 | 25 | 27 |
| Histological
type |
|
|
| Squamous
cell carcinoma | 16 | 12 |
|
Adenocarcinoma | 24 | 25 |
| Extracranial
disease |
|
|
|
Absent | 22 | 17 |
|
Present | 18 | 20 |
Treatment
The first group of patients were administered WBRT
(total dose of 30 Gy/10 fractions, 3 Gy/day on days 1–5 weekly) and
TMZ (75 mg/m2 p.o. q.d., until the end of WBRT). The
second group of patients were administered WBRT, at the same dose
as the first group, with placebo (p.o. q.d. until the end of WBRT).
Platinum-based chemotherapy was allowed in the two groups following
WBRT, under the guidance of the doctors. The first group was
administered TMZ 75 mg/m2 p.o. q.d. on days 1–5 combined
with chemotherapy, and the second group was administered
chemotherapy and placebo simultaneously. Mannitol and dexamethasone
were given at the dose required in order to reduce the RT-related
side effects. Treatment was continued until unacceptable toxicity
occurred (such as grade 4 myelosuppression that did not improve
after 1 week, or coma).
Response evaluation
Blood tests were performed once weekly, and a brain
MRI was performed within 1 month of RT completion to evaluate the
treatment efficacy. Following RT, all patients were evaluated every
2 months if they experienced no headaches or other symptoms. The
evaluation included assessment of complications, physical
examination and MRI scan of brain. The primary endpoints included
objective response (OR), which was evaluated within 1 week after
the end of WBRT. Response to treatment in the brain was assessed
according to the World Health Organization/Eastern Cooperative
Oncology Group criteria, and defined as CR (complete remission), PR
(partial remission), SD (stable disease) and PD (progressive
disease). OR was defined as a measure of treatment efficacy (CR +
PR). The secondary endpoints were overall survival (OS) and QoL. OS
was defined as the time from RT initiation to death or the date of
the last follow-up. QoL was measured using the Functional
Assessment of Cancer Therapy-Brain (FACT-BR, version 4) before and
after WBRT. Adverse reactions were evaluated according to the
National Cancer Institute Common Terminology Criteria for Adverse
Events, version 3.0 (14).
Statistical analysis
Data were analyzed using SPSS 22.0 software (IBM
Corp., Armonk, NY, USA). General information on patients, such as
OR and toxicity, were described and compared using the Chi-squared
test. OS was calculated with the Kaplan-Meier method and the
differences were compared using the log-rank test. The difference
in QoL between the two groups prior to and following WBRT was
compared by the independent samples t-test, and comparison of the
QoL difference within each group before and after WBRT was
performed using the paired samples t-test. P<0.05 were
considered to indicate a statistically significant difference.
Results
Patients
All the patients completed the treatment
successfully. The patient characteristics are listed in Table I. The sample included a total of 49
male and 28 female patients, with a median age of 57 years and a
median KPS score of 80 for the first group, and a median age of 61
years and a median KPS score of 80 for the second group. The sex
ratios of male to female patients were 1.86 and 1.64, respectively,
in the two groups.
Treatment and efficacy
As shown in Table
II, all the patients were followed up after the completion of
RT. The first group was superior to the second group in terms of OR
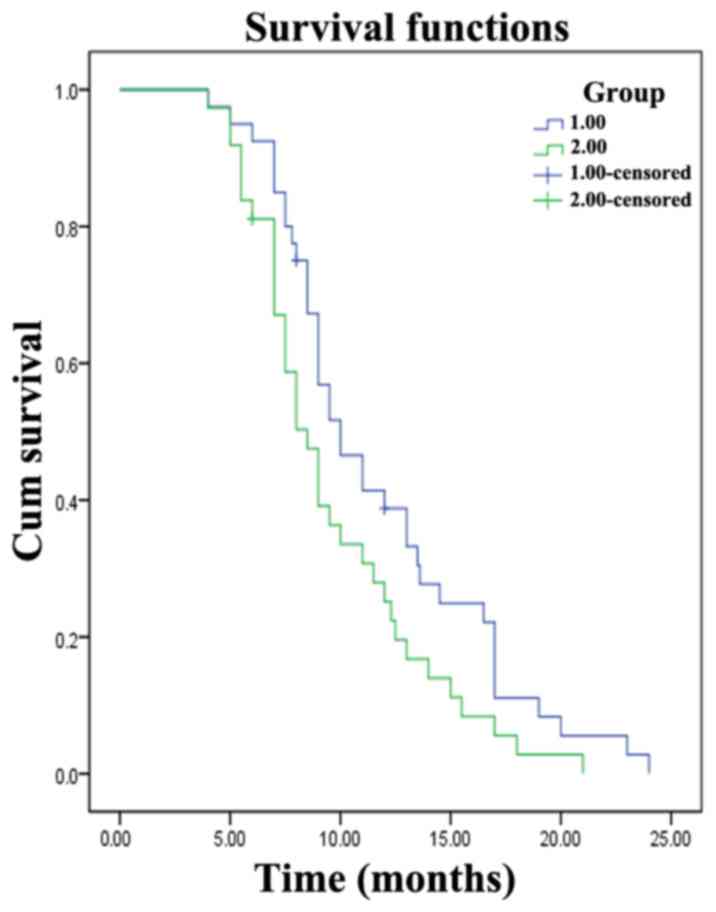
(P<0.05). A total of 3 patients were lost to follow-up at 6, 8
and 12 months after RT. The median OS was 10 months [95% confidence
interval (CI): 8.0–12.0 months] for the first group and 8.5 months
(95% CI: 7.3–9.8 months) for the second group. The first group
exhibited an advantage in terms of OS when compared with the second
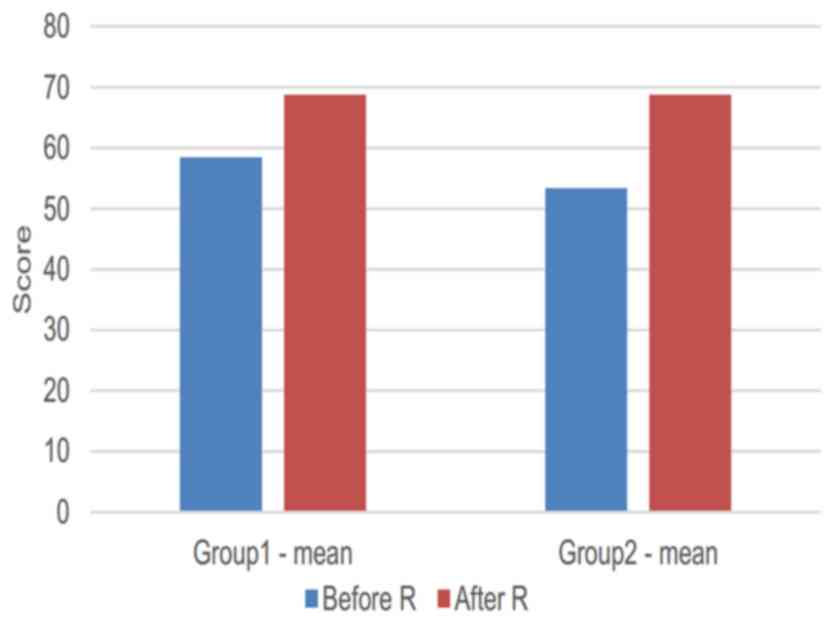
group (P<0.05; Fig. 1). There was
no significant difference between the two groups before and after
RT (Table IV). However, QoL after
RT was higher compared with that prior to RT in both groups (group
1, P<0.001; group 2, P<0.001; Fig.
2).
| Table II.Response of brain metastases after
irradiation. |
Table II.
Response of brain metastases after
irradiation.
| Group | CR | PR | SD | PD | χ2 | P-value | OR | χ2 | P-value |
|---|
| 1 | 8 | 19 | 8 | 5 | 5.43 | 0.14 | 27 | 4.59 | 0.03 |
| 2 | 3 | 13 | 11 | 10 |
|
| 16 |
| Table IV.FACT-BR score before and after
radiotherapy. |
Table IV.
FACT-BR score before and after
radiotherapy.
|
| Before RT | After RT |
|---|
|
|
|
|
|---|
| Group | BR score | t | P-value | BR score | t | P-value |
|---|
| 1 | 58.50 (9.56) | 0.55 | 0.59 | 68.78 (7.74) | 0.51 | 0.61 |
| 2 | 57.32 (9.33) |
|
| 67.73 (10.11) |
|
|
Safety
The toxicities observed are summarized in Table III. There was no significant
difference in the side effects between the two groups.
Hematological toxicity and vomiting in the first group were more
severe compared with those in the second group, but the difference
was not statistically significant. Only a few patients in both
groups developed grade 3 or 4 toxicities.
| Table III.Treatment-related hematological and
non-hematological toxicity. |
Table III.
Treatment-related hematological and
non-hematological toxicity.
|
| Group 1 | Group 2 |
|
|
|---|
|
|
|
|
|
|
|---|
| Toxicity | Grade I–II | Grade III–IV | Grade I–II | Grade III–IV | χ2 | P-value |
|---|
| Neutropenia | 19 | 10 | 9 | 5 | 0.01 | 0.94 |
| Thrombocytopenia | 12 | 6 | 5 | 1 | 0.60 | 0.63 |
| Anemia | 8 | 3 | 5 | 2 | 0.00 | 1.00 |
| Vomiting | 15 | 9 | 10 | 2 | 1.64 | 0.27 |
| Headache | 10 | 6 | 12 | 3 | 1.15 | 0.43 |
| Vertigo | 13 | 5 | 11 | 6 | 0.23 | 0.73 |
Discussion
Lung cancer is the type of cancer that most commonly
metastasizes to the brain. The median survival of patients with BM
from lung cancer is <3 months (3). There are several treatment options for
BM, such as WBRT, stereotactic body radiation therapy (SBRT),
surgery and chemotherapy. The efficacy of SBRT and surgery is
limited, as they may be applied to single small metastatic lesions,
but BM generally manifest as multiple lesions. WBRT has been shown
to increase the median survival in a number of trials, and it is
considered as the standard treatment for BM (15,16). The
use of conventional chemotherapeutic drugs is limited, as it is
difficult for these drugs to cross the blood-brain barrier. TMZ,
which can penetrate through the blood-brain barrier, has
demonstrated efficacy in BM, and may increase the effectiveness of
WBRT (17). A meta-analysis
including four trials demonstrated that the combination of TMZ and
WBRT was superior to RT alone in terms of PR and SD. The
combination group also exhibited a mild improvement compared with
RT alone in terms of OS. However, the combination group also
exhibited a significantly higher incidence of gastrointestinal and
grade >3 hematological toxicities compared with the RT alone
group (17). Another meta-analysis
also demonstrated that concomitant administration of TMZ and RT
significantly increased the OR in patients with BM compared with RT
alone, but failed to demonstrate a survival advantage (18). A phase 2 trial demonstrated that the
OR for TMZ combined with RT was significantly higher compared with
that observed with RT alone (P=0.017). The median OS of the
combination group was higher compared with the median OS of the RT
alone group (8.6 vs. 7.0 months, respectively) (19). In another trial, the addition of TMZ
to RT conferred an advantage in terms of PFS and OR (P<0.05),
but there was no significant improvement in OS compared with RT
alone. There was little difference in QoL between the two groups
(20). A trial reported that the OR
rate of concomitant WBRT with TMZ was 45%. The median time to
progression (TTP) was 9 months and the median OS was 13 months. The
analysis of QoL in the trial revealed a high level of satisfaction
among patients (21). Addition of
TMZ to RT increased OR in patients with BM from NSCLC, as
determined in a meta-analysis, but the differences in PFS and OS
were not statistically significant (22). The efficacy and safety of TMZ were
confirmed in these trials. However, other trials failed to
demonstrate any significant improvements in OR or OS with the
addition of TMZ to WBRT. A phase 3 trial reported that the
combination of TMZ or erlotinib with RT did not improve OS in NSCLC
patients with BM. The trial also demonstrated that the OS of
erlotinib compared with that of TMZ in combination with RT did not
differ significantly (23). Another
phase 2 study reported no differences in TTP and OS between the TMZ
+ RT and the RT alone groups (24),
and a phase 3 trial reported that adding TMZ or erlotinib to RT
conferred no OS benefit to patients with BM from NSCLC (8). In addition, the benefit of adding TMZ
to WBRT has not been confirmed (11). Therefore, the administration of TMZ
concomitantly with RT in patients with BM currently remains
controversial.
In the present study, we reported an OR rate of
67.5% in the first group, while the OR rate was 43.2% in the second
group. WBRT plus TMZ is a well-tolerated treatment with high
response rates. In addition to its antitumor effect, TMZ may also
increase the sensitivity of tumor cells to RT. The improvement in
OS following the addition of TMZ to the treatment regimen may be
due to the improved local control of BM. The Graded Prognostic
Assessment (GPA) score may be used to evaluate the prognosis of
lung cancer. An attempt was made to evaluate the effect of the GPA
score on treatment efficacy and patient survival in the two groups,
but there was no statistically significant difference. The reason
may be that the sample size was limited. In addition, the lack of
randomization is also a limitation of the present study, and the
results including the value of GPA score require future
confirmation by large-sample clinical trials in the future. Based
on the results of this trial, TMZ is recommended for concomitant
use with WBRT in patients with BM from lung cancer. PFS
prolongation in patients with intracranial metastatic tumors is key
to improving OS. Previous trials confirmed that TKIs combined with
WBRT can prolong the OS when compared with WBRT alone, while other
trials reported little benefit in terms of OS (25,26). The
reason for this inconsistency may be associated with the fact that
the concentration of TKIs in the cerebrospinal fluid is markedly
lower compared with their concentration in the serum. A
large-sample trial is required to confirm the effect of TKIs on BM.
The OS of patients with BM is shortened by treatment limitations,
and the QoL of the patients is also becoming increasingly
important. The QoL of patients with BM may be evaluated by FACT-BR,
which has exhibited good reliability and validity (27). The QoL was not compromised in the TMZ
combination group compared with the RT alone group in our trial,
which is consistent with previous reports (28). The QoL of patients following RT was
higher compared with that prior to RT, which may be due to the
reduction of the tumor volume and relief of the peripheral nerve
compression symptoms (28).
Furthermore, psychological support and nursing interventions may
improve QoL (29). The incidence of
BM exhibits an increasing trend due to the increased incidence of
cancer, but the OS of patients with BM was not significantly
prolonged. Treatment of BM represents a major challenge, and there
is an urgent need for novel drugs that are able to penetrate the
blood-brain barrier.
Acknowledgements
Not applicable.
Funding
This study was supported by the National Natural
Science Foundation of China (grant no. 81672974).
Availability of data and materials
The analysed data sets generated during the study
are available from the corresponding author on reasonable
request.
Authors' contributions
JZ designed this trial and was responsible for the
final decision to submit for publication and had the full data of
the paper. YL gathered data and wrote the report. ZL and NL helped
to gather data. YT performed the literature search. All the authors
have read and approved the final version of this manuscript.
Ethics approval and consent to
participate
All procedures performed in studies involving human
participants were in accordance with the ethical standards of the
institutional and/or national research committee and with the 1964
Helsinki Declaration and its later amendments or comparable ethical
standards. The study protocol was approved by the Ethics Committee
of the Qianfoshan Hospital Affiliated to Shandong University, and
all the patients provided written informed consent.
Consent for publication
All the patients provided written informed
consent.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Seoane J and De Mattos-Arruda L: Brain
metastasis: New opportunities to tackle therapeutic resistance. Mol
Oncol. 8:1120–1131. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Berger LA, Riesenberg H, Bokemeyer C and
Atanackovic D: CNS metastases in non-small-cell lung cancer:
Current role of EGFR-TKI therapy and future perspectives. Lung
Cancer. 80:242–248. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Sperduto PW, Kased N, Roberge D, Xu Z,
Shanley R, Luo X, Sneed PK, Chao ST, Weil RJ, Suh J, et al: Summary
report on the graded prognostic assessment: An accurate and facile
diagnosis-specific tool to estimate survival for patients with
brain metastases. J Clin Oncol. 30:419–425. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Tabouret E, Chinot O, Metellus P, Tallet
A, Viens P and Gonçalves A: Recent trends in epidemiology of brain
metastases: An overview. Anticancer Res. 32:4655–4662.
2012.PubMed/NCBI
|
|
5
|
Baykara M, Kurt G, Buyukberber S, Demirci
U, Ceviker N, Algin E, Coskun U, Aykol S, Emmez H, Ozet A, et al:
Management of brain metastases from non-small cell lung cancer. J
Cancer Res Ther. 10:915–921. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Scoccianti S and Ricardi U: Treatment of
brain metastases: Review of phase III randomized controlled trials.
Radiother Oncol. 102:168–179. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Walbert T and Gilbert MR: The role of
chemotherapy in the treatment of patients with brain metastases
from solid tumors. Int J Clin Oncol. 14:299–306. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Sperduto PW, Wang M, Robins HI, Schell MC,
Werner-Wasik M, Komaki R, Souhami L, Buyyounouski MK, Khuntia D,
Demas W, et al: A phase 3 trial of whole brain radiation therapy
and stereotactic radiosurgery alone versus WBRT and SRS with
temozolomide or erlotinib for non-small cell lung cancer and 1 to 3
brain metastases: Radiation Therapy Oncology Group 0320. Int J
Radiat Oncol Biol Phys. 85:1312–1318. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Chun SG, Choe KS, Iyengar P, Yordy JS and
Timmerman RD: Isolated central nervous system progression on
Crizotinib: An Achilles heel of non-small cell lung cancer with
EML4-ALK translocation? Cancer Biol Ther. 13:1376–1383. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Tatar Z, Thivat E, Planchat E, Gimbergues
P, Gadea E, Abrial C and Durando X: Temozolomide and unusual
indications: Review of literature. Cancer Treat Rev. 39:125–135.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Chua D, Krzakowski M, Chouaid C, Pallotta
MG, Martinez JI, Gottfried M, Curran W and Throuvalas N:
Whole-brain radiation therapy plus concomitant temozolomide for the
treatment of brain metastases from non-small-cell lung cancer: A
randomized, open-label phase II study. Clin Lung Cancer.
11:176–181. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Gamboa-Vignolle C, Ferrari-Carballo T,
Arrieta Ó and Mohar A: Whole-brain irradiation with concomitant
daily fixed-dose temozolomide for brain metastases treatment: A
randomised phase II trial. Radiother Oncol. 102:187–191. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Christodoulou C, Bafaloukos D, Linardou H,
Aravantinos G, Bamias A, Carina M, Klouvas G and Skarlos D:
Hellenic Cooperative Oncology Group: Temozolomide (TMZ) combined
with cisplatin (CDDP) in patients with brain metastases from solid
tumors: A Hellenic Cooperative Oncology Group (HeCOG) Phase II
study. J Neurooncol. 71:61–65. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Trotti A, Colevas AD, Setser A, Rusch V,
Jaques D, Budach V, Langer C, Murphy B, Cumberlin R and Coleman CN:
CTCAE v3.0: Development of a comprehensive grading system for the
adverse effects of cancer treatment. Semin Radiat Oncol.
13:176–181. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Ferrarese F, Baggio V, Zorat PL and Fiore
D: Treatment and prophylaxis for brain metastases from non-small
cell lung cancer: whole brain radiation treatment versus
stereotactic radiosurgery. Ann Oncol Suppl. 2:ii71–ii72. 2006.
View Article : Google Scholar
|
|
16
|
Larson D and Sahgal A, Larson D and Sahgal
A: Adjuvant whole brain radiotherapy: strong emotions decide but
rationale studies are needed: in regard to Brown et al. (Int
J Radiat Oncol Biol Phys 2008;70:1305-1309). In reply to Drs.
Larson and Sahgal. Int J Radiat Oncol Biol Phys. 75:316–317.
2009.
|
|
17
|
Liu R, Wang X, Ma B, Yang K, Zhang Q and
Tian J: Concomitant or adjuvant temozolomide with whole-brain
irradiation for brain metastases: A meta-analysis. Anticancer
Drugs. 21:120–128. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Zhao Q, Qin Q, Sun J, Han D, Wang Z, Teng
J and Li B: Brain radiotherapy plus concurrent temolomide versus
radiotherapy alone for patients with brain metastases: A
meta-analysis. PLoS One. 11:e01504192016. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Antonadou D, Paraskevaidis M, Sarris G,
Coliarakis N, Economou I, Karageorgis P and Throuvalas N: Phase II
randomized trial of temozolomide and concurrent radiotherapy in
patients with brain metastases. J Clin Oncol. 20:3644–3650. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Xia Deng, Zhen Zheng, Baochai Lin, et al:
The efficacy and roles of combining temozolomide with whole brain
radiotherapy in protection neurocognitive function and improvement
quality of life of non-small-cell lung cancer patients with brain
metastases. BMC cancer. 17:422017. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Addeo R, Caraglia M, Faiola V, Capasso E,
Vincenzi B, Montella L, Guarrasi R, Caserta L and Del Prete S:
Concomitant treatment of brain metastasis with whole brain
radiotherapy [WBRT] and temozolomide [TMZ] is active and improves
quality of life. BMC Cancer. 7:182007. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ma W, Li N, An Y, Zhou C, Bo C and Zhang
G: Effects of Temozolomide and Radiotherapy on Brain Metastatic
Tumor: A Systematic Review and Meta-Analysis. World Neurosurg.
92:197–205. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Qin H, Pan F, Li J, Zhang X, Liang H and
Ruan Z: Whole brain radiotherapy plus concurrent chemotherapy in
non-small cell lung cancer patients with brain metastases: A
meta-analysis. PLoS One. 9:e1114752014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Hassler MR, Pfeifer W, Knocke-Abulesz TH,
Geissler K, Altorjai G, Dieckmann K and Marosi C: Temozolomide
added to whole brain radiotherapy in patients with multiple brain
metastases of non-small-cell lung cancer: A multicentric Austrian
phase II study. Wien Klin Wochenschr. 125:481–486. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Zheng MH, Sun HT, Xu JG, Yang G, Huo LM,
Zhang P, Tian JH and Yang KH: Combining Whole-Brain Radiotherapy
with Gefitinib/Erlotinib for Brain Metastases from Non-Small-Cell
Lung Cancer: A Meta-Analysis. BioMed Res Int. 2016:58073462016.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Broniscer A, Panetta JC, O'Shaughnessy M,
Fraga C, Bai F, Krasin MJ, Gajjar A and Stewart CF: Plasma and
cerebrospinal fluid pharmacokinetics of erlotinib and its active
metabolite OSI-420. Clin Cancer Res. 13:1511–1515. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Chow R, Lao N, Popovic M, Chow E, Cella D,
Beaumont J, Lam H, Pulenzas N, Bedard G, Wong E, et al: Comparison
of the EORTC QLQ-BN20 and the FACT-Br quality of life
questionnaires for patients with primary brain cancers: A
literature review. Support Care Cancer. 22:2593–2598. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Pulenzas N, Ray S, Zhang L, McDonald R,
Cella D, Rowbottom L, Sahgal A, Soliman H, Tsao M, Danjoux C, et
al: The Brain Symptom and Impact Questionnaire in brain metastases
patients: A prospective long-term follow-up study. CNS Oncol.
5:31–40. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Pan CJ, Liu HC, Liang SY, Liu CY, Wu WW
and Cheng SF: Resilience and coping strategies influencing the
quality of life in patients with brain tumor. Clin Nurs Res Jun.
1:10547738177145622017.
|