Introduction
Oral cancer is the sixth most common cancer type
worldwide (1). Of note, one third
of the total global oral cancer cases are from India (2), and >90% of all oral cancer cases
are oral squamous cell carcinomas (OSCCs) (3,4).
OSCCs result from the progression of oral submucous fibrosis
(OSMF), a pre-cancerous condition. In recent years, an increase in
the occurrence of OSMF has been observed in South and Southeast
Asia, particularly India. Comparatively, fewer cases have been
reported in Europe and North America (5,6).
OSMF cases are most commonly noted in younger generations owing to
the intake of smokeless tobacco products (4,7,8).
Smokeless tobacco is a tobacco product that is consumed in any
manner or form other than smoking (8). Smokeless tobacco is promoted as an
alternative to smoking and most consumers use it daily (4). However, various carcinogens, such as
nicotine, tobacco-specific N-nitrosamines, arsenic, beryllium,
chromium, nitrite, nitrate, cadmium, nickel and polynuclear
hydrocarbon benzo[a]pyrene, are present in smokeless tobacco
(4,8). These carcinogens cause dysplastic
changes in the oral mucosa and lead to various pathologic lesions,
including smokeless tobacco keratosis, verrucous carcinoma,
leucoplakia, erythroplakia, leukoedema, parakeratosis and OSCC
(4,7). Gutkha is the most popular smokeless
tobacco sold in multi-coloured attractive pouches and is available
only in India. Gutkha is a mixture of sun-dried, roasted and finely
chopped tobacco, areca nut, slaked lime, catechu, spices,
sweeteners and essences. This mixture is held in the mouth, chewed,
or sucked with the generated saliva and is either spit out or
swallowed (4,7,9).
Epidemiological studies have indicated that chewing gutkha is one
of the most significant risk factors for OSMF (6,10-12)
accounting for >3,50,000 oral cancer cases worldwide (7).
Previous studies have demonstrated that the
malignant transformation rate of OSMF is 7-13% (13,14).
In patients with OSMF, dysplastic changes occur in the epithelium,
thereby disrupting the basement membrane and invading the
connective tissue. Thus, the oral epithelium becomes atrophied and
hence more vulnerable to carcinogens (4). Simultaneous exposure to the
ingredients of betel quid (betel leaf, areca nut and slaked lime)
and tobacco has been shown to markedly increase the incidence of
oral cancer in patients with OSMF (15). OSMF generally turns into oral
cancer (OSCC) 3-16 years following the initial diagnosis (12). The most potent risk factors for the
development of OSCC are alcohol and tobacco usage (4). These factors are not only associated
with the development of OSCC, but also with the course of the
disease, and their consumption is associated with a poor prognosis
(16). As OSCC usually follows
pre-malignant lesions and conditions that are easily detectable,
therapeutic intervention at this stage is a critical factor in
preventing the further development and progression of the
disease.
Trace elements are essential for the activity of
numerous enzymes, and therefore, variations in the serum levels of
these biochemical markers may be linked to the pathogenesis of
various cancers, including oral cancer (17). Therefore, the role of trace
elements has been extensively studied in recent years in various
types of cancer, such as breast (18-20),
gastric (21,22), lung (23-25),
oral (17,26-29)
and pancreatic cancers (30), as
well as in liver cirrhosis (30).
A number of studies have concluded that trace elements can be used
for the early prediction or diagnosis of cancer (17,18,23,26-29).
The study by Choi et al (31) demonstrated that the levels of trace
elements were significantly higher in patients with stage IV breast
cancer than in those with non-stage IV breast cancer, suggesting
the possibility of using trace elements for the early detection of
cancer. Gutkha is known to contain several trace elements,
including copper (Cu), zinc (Zn), selenium (Se) and molybdenum
(Mo). Therefore, it may contribute to alterations in the serum and
salivary levels of trace elements (32). Cu levels have been shown to be
increased in the serum of patients with cancer, as Cu enables
angiogenesis, growth and metastasis (33). The serum Cu level has been reported
to be a possible tumour marker due to its association with the
stage of Hodgkin's disease (34).
Zn can induce the apoptosis of cancer cells and inhibit their
proliferation. The high supplementation of Zn has been observed to
be effective in reducing oxidative stress and improving immune
responses in patients with cancer (35,36).
Furthermore, the Cu and Zn ratio (Cu:Zn) has been documented to
predict tumour progression in patients with osteosarcoma and
non-small cell lung cancer (37,38).
Fisher et al (37)
demonstrated that the ratio of Cu:Zn in serum was higher in
patients with metastatic osteosarcoma than those with primary
osteosarcoma. Moreover, in their study, Oyama et al
(38) observed that the Cu:Zn
ratio exhibited prognostic significance similar to tumour markers,
such as carcinoembryonic antigen. Se functions as a chemopreventive
agent due to its antioxidant effects (35,36).
Mo is regarded as an essential trace element in human nutrition, as
it functions as a cofactor for enzymes such as xanthine oxidase,
aldehyde oxidase and sulfite oxidase in mammals. Biochemical
alterations in the levels of these trace elements in the serum of
patients with precancerous conditions and oral cancer can aid not
only in early diagnosis and treatment, but also in prognosis as the
disease progresses (39).
As gutkha intake is one of the factors responsible
for OSMF and it also contains several trace elements that can
influence the levels of trace elements in the body of the consumer,
the present study aimed to estimate the levels of serum and
salivary trace elements in patients with OSMF and OSCC. In the
present study, the levels of selected trace elements, namely, Cu,
Zn, Se and Mo, were measured in patients with OSCC and OSMF, and
compared with those of a control group to determine the changes in
trace element levels.
Patients and methods
Study location and case selection
Ethical clearance was obtained from the Ethics
Committee at MNR Dental College and Hospital (Hyderabad, India;
Protocol ID: D139803007) before pursuing the study. The present
study was performed at the MNR Dental College and Hospital
(Department of Oral and Maxillofacial Pathology), the Centre for
Cellular and Molecular Biology (CCMB) and the Indian Institute of
Chemical Technology (IICT) in Hyderabad, India. Participant
selection and sample collection were carried out at the MNR Dental
College and Hospital, while samples were processed at CCMB and
sample analysis was conducted at IICT.
A total of 80 participants were recruited after
explaining the study protocol to them and obtaining their written
informed consent. Patients were selected after obtaining their
health history and performing clinical and histological
examinations to confirm OSMF and OSCC. The study included a total
of 48 males and 32 females with an age range of 20-65 years. The
patients were categorized into four groups with 20 patients in each
(Table I). Group A included
individuals with a history of gutkha intake without OSMF. Group B
comprised individuals with a history of gutkha intake with OSMF.
Group C consisted of individuals with OSCC, and group D included
healthy controls. Patient selection was performed based on
pre-defined inclusion and exclusion criteria. As per the inclusion
criteria, the following patients were selected: i) Patients with
OSCC of the oral cavity only (buccal mucosa, tongue, floor of the
mouth, palate, gingiva, labial mucosa and retromolar area); and ii)
patients who had a positive history of gutkha chewing for >1
year. The following patients were excluded from the study: i)
Patients with a history of consumption of tobacco in any other form
such as cigars, bidi, or mawa; ii) patients who had previously
received treatment for OSMF or OSCC; iii) patients with a history
of any systemic diseases or carcinoma elsewhere in the body; iv)
those with OSMF, but had stopped chewing gutkha; and v) those with
congenital deficiency in trace elements and deficiency-related
diseases.
 | Table IDistribution of the study
participants in the different groups. |
Table I
Distribution of the study
participants in the different groups.
| | Group A (n=20) | Group B (n=20) | Group C (n=20) | Group D (n=20) |
|---|
| Age group
(years) | M | F | M | F | M | F | M | F |
|---|
| 21-30 | 3 | 1 | 7 | 2 | 2 | 0 | 2 | 3 |
| 31-40 | 8 | 1 | 3 | 1 | 5 | 2 | 6 | 2 |
| 41-50 | 3 | 3 | 0 | 4 | 1 | 3 | 1 | 2 |
| 51-60 | 0 | 1 | 1 | 2 | 2 | 1 | 2 | 2 |
| 61-70 | 0 | 0 | 0 | 0 | 2 | 2 | 0 | 0 |
| Total | 14 | 6 | 11 | 9 | 12 | 8 | 11 | 9 |
Sample collection and storage
Samples were collected from January, 2015 to
October, 2015. Under aseptic conditions, 3 ml blood were collected
and allowed to clot at room temperature for 1 h. Subsequently, the
serum was separated via centrifugation at 1,912 x g and 4˚C for 10
min and collected in a sterile vacutainer.
Prior to the collection of saliva, patients were not
allowed to eat or drink for 2 h. Unstimulated whole saliva (2 ml)
was collected using the spit method in a sterile container. The
samples were centrifuged at 1,912 x g and 4˚C for 5 min to remove
large debris and reduce viscosity. Supernatants were transferred to
fresh containers. All samples were labelled and stored at -20˚C
until analysis.
Sample processing
The procedure was adapted from the study by Li et
al (40). Briefly, a 500 µl
aliquot of serum or saliva was transferred into a 1.5-ml
polypropylene microcentrifuge tube. To this sample, 350 µl
concentrated nitric acid (#LP NACL40-2.5L, ANPROS Pty Ltd.) and 300
µl hydrogen peroxide (#00182, Loba Chemie Pvt. Ltd.) were added.
The tubes were then centrifuged for 10 min at 4,112 x g and 4˚C,
and samples were placed in a hot water bath at 90˚C for 90 min. In
the case that particulates were observed in the samples, they were
placed back in the hot water bath for an additional 60 min. The
digested serum samples were diluted (1:20) in Milli-Q water. Saliva
samples were diluted (1:20) in nitric acid. Following this, the
samples were centrifuged for 5 min at 4.112 x g and 4˚C.
Sample analysis
The protocol for sample analysis was modified from
the studies by Kara (41) and
Momen et al (42). Briefly,
the samples were analysed using inductively coupled plasma-optical
emission spectrometry (ICP-OES; #725ES, Varian Australia Pty Ltd.).
The operating conditions for the instrument are presented in
Table II. Cu, Zn, Se and Mo were
monitored at wavelengths of 324.75, 213.85, 196.09 and 202.03 nm,
respectively.
| Table IIInductively coupled plasma-optical
emission spectrometry operating conditions. |
Table II
Inductively coupled plasma-optical
emission spectrometry operating conditions.
| Parameters | Conditions |
|---|
| RF power | 1.3 kW |
| Viewing height
above the load coil | 10 mm |
| Nebulizer
pressure | 250.0 kPa |
| Coolant gas flow
rate | 12 l/min |
| Auxiliary gas flow
rate | 0.5 l/min |
| Nebulizer gas flow
rate | 0.30 l/min |
| Sample uptake
rate | 0.8 ml/min |
| Sample uptake
delay | 30 sec |
| Instrument
stabilization delay | 15 sec |
| Pump rate | 20 rpm |
| Rinse time | 20 sec |
| Replicates | Three times |
| Replicate read
time | 7 sec |
Statistical analysis
The mean concentrations of the trace elements were
determined. ANOVA with Tukey's honestly significant difference
(HSD) post hoc test were performed using IBM SPSS Statistics
(version 22.0; IBM Corp.). A P-value ≤0.05 was considered to
indicate a statistically significant difference.
Results
Trace element levels in the serum
The levels of each trace element are presented in
Table III. The results indicated
an increase in the Cu levels in all the test groups when compared
with the control group (Fig. 1A).
Moreover, the Cu levels demonstrated a statistically significant
increase in patients with OSCC (group C) when compared with the
control group. Furthermore, there was a significant difference
between patients with gutkha intake without OSMF (Group A) and
those with OSCC (Group C). In addition, there was a decrease in Zn
levels in all the test groups when compared with the control group
(Fig. 1A). The Zn levels exhibited
a statistically significant decrease in patients with gutkha intake
without OSMF (group A) and patients with OSCC (group C) when
compared with the control group. The mean Se levels exhibited a
statistically significant decrease in all the test groups when
compared with the control group (Fig.
1B). Furthermore, the mean Mo levels exhibited a statistically
significant decrease in all the test groups when compared with the
control group (Fig. 1B).
 | Figure 1Trace element levels in serum and
saliva. (A) In serum, a significant increase in the Cu level was
observed in group C. In groups A and C, the Zn level was
significantly reduced. In saliva, a significant increase in the Cu
level was observed in groups B and C. In group A, the Zn level was
significantly increased. (B) In serum, all the test groups
exhibited a significant reduction in Se and Mo compared with the
control group. In saliva, none of the test groups exhibited
significant differences in Se and Mo compared with the control
group. *P≤0.05, and ***P≤0.001. Group A,
gutkha intake without OSMF; group B, gutkha intake with OSMF; group
C, with oral squamous cell carcinoma; group D, healthy controls.
OSMF, oral submucous fibrosis; Zn, zinc; Cu, copper; Se, selenium;
Mo, molybdenum. |
| Table IIIComparison of trace elements (Cu, Zn,
Se and Mo) between the groups in the present study. |
Table III
Comparison of trace elements (Cu, Zn,
Se and Mo) between the groups in the present study.
| | Group A | Group B | Group C | Group D | |
|---|
| Element | Mean | SD | Mean | SD | Mean | SD | Mean | SD | P-value | Post hoc test
comparison |
|---|
| Cu (µg/ml) | | | | | | | | | | |
|
Serum | 0.98 | 0.44 | 1.07 | 0.53 | 1.57 | 0.73 | 0.66 | 0.45 | <0.001 | C>D |
|
Saliva | 0.02 | 0.02 | 0.06 | 0.04 | 0.09 | 0.09 | 0.02 | 0.02 | <0.001 | C>D |
| Zn (µg/ml) | | | | | | | | | | |
|
Serum | 1.09 | 1.21 | 1.46 | 1.00 | 0.68 | 0.32 | 1.98 | 1.13 | 0.001 | D>A, C |
|
Saliva | 0.45 | 0.70 | 0.12 | 0.05 | 0.24 | 0.34 | 0.08 | 0.09 | <0.05 | A>D |
| Se (µg/ml) | | | | | | | | | | |
|
Serum | 0.01 | 0.01 | 0.01 | 0.01 | 0.05 | 0.04 | 0.07 | 0.03 | <0.001 | D>A, B, C |
|
Saliva | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | >0.05 | - |
| Mo (µg/ml) | | | | | | | | | | |
|
Serum | 0.01 | 0.01 | 0.02 | 0.02 | 0.03 | 0.03 | 0.06 | 0.03 | <0.001 | D>A, B, C |
|
Saliva | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.02 | 0.02 | >0.05 | - |
Trace element levels in saliva
The level of each trace element is shown in Table III. The results revealed a
significant increase in the mean Cu levels in patients with OSMF
(group B) and OSCC (group C) when compared with the control group
(group D). Moreover, patients with gutkha intake without OSMF
(group A) and OSCC (group C) exhibited a significant difference in
Cu levels (Fig. 1A). There was an
increase in the Zn levels in all the test groups when compared with
the control group (group D). A statistically significant increase
was observed in Zn levels patients with gutkha intake without OSMF
(group A) compared with the control (Fig. 1A). The findings revealed that there
was no significant difference in Se and Mo levels in any of the
groups (Fig. 1B).
Role of age in trace element levels in
serum and saliva
All age groups exhibited higher levels of trace
elements in the serum than in the saliva. However, there were no
significant differences in the levels of trace elements based on
age (Fig. 2). The only exception
was the Se level in serum, where there was a significant difference
between the age groups of 41-50 years and 51-60 years.
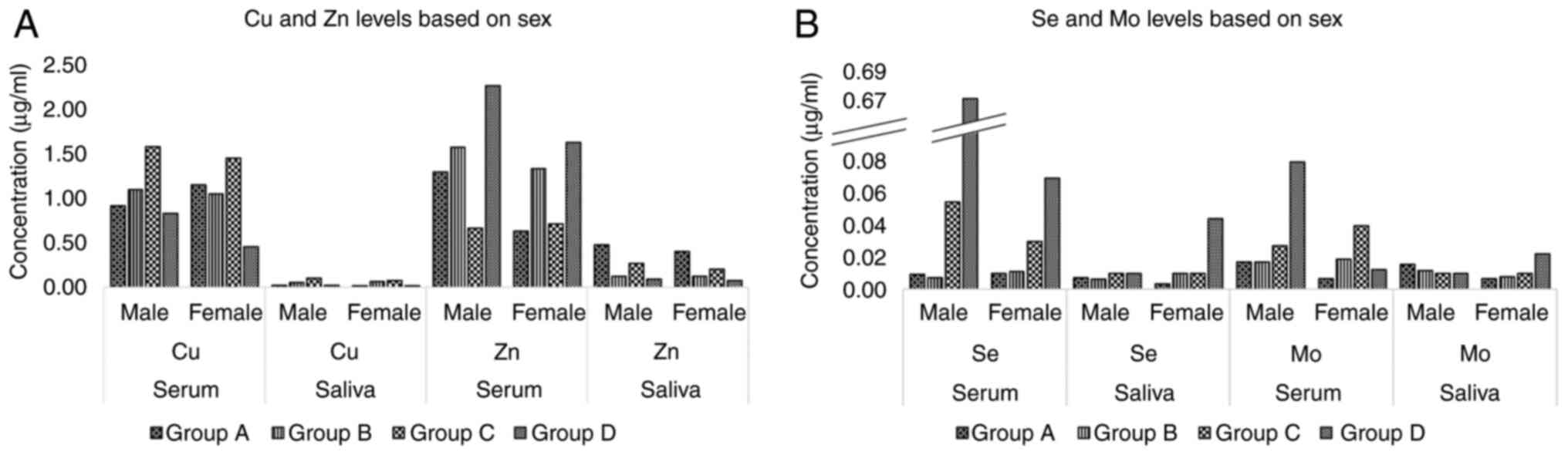
Role of sex in trace element levels in
the serum and saliva
There were no significant differences in the levels
of trace elements based on sex within their respective groups
(Fig. 3).
Discussion
The present study focussed on the levels of trace
elements, namely, Cu, Zn, Se and Mo in serum and saliva samples.
These elements exhibit various physiological functions and have
been linked to the development of OSMF, a pre-malignant oral
condition, and OSCC, a malignant oral condition. In the present
study, as shown in Table I, the
mean age of the individuals was 37.55 years in group A, 35.70 years
in group B, 47.10 years in group C and 38.60 years in group D. A
male predominance was noted, with 14 (70%) in group A, 11 (55%) in
group B, 12 (60%) in group C and 11 (55%) in group D. A similar
male prevalence was also reported in the studies by Kumar et
al (43) and Tyagi et
al (29).
Cu is essential for cell growth and functions as a
co-factor for a number of enzymes. Necrosis and oxidative stress in
cancer cells lead to an increase in the serum Cu level (18). Accordingly, in the present study,
an increase in the serum Cu level was observed in all patients with
gutkha intake with or without OSMF and with OSCC compared with the
control group. These findings indicate an alteration in the serum
Cu level as the disease progressed. This alteration increased with
gutkha intake and was followed by the development of OSMF and its
malignant transformation into OSCC. The significant difference
observed in Cu levels between the patients with gutkha intake
without OSMF (group A) and OSCC (group C) suggested the key role of
Cu in OSCC. The increase in the serum Cu level with gutkha intake
may be attributed to the high Cu content in areca nut (mean 302
nmol/g) (44), a major etiological
factor in the pathogenesis of OSMF. A further increase in the Cu
level in pre-malignant and malignant conditions suggests its
possible role as a tumour marker (34). As Cu is involved in angiogenesis,
growth and metastasis in cancer (33), its increase in OSMF and OSCC
signifies its supportive role in disease progression.
The serum Zn level was decreased with gutkha intake
and the development of OSMF and OSCC. This decrease may be
attributed to the utilization of Zn for protection against cancer
(35,36) by acting as an antioxidant, aiding
in the formation of glutathione peroxidase, and activating the DNA
repair enzymes (18). Tannin and
arecoline present in areca nut reduce the degradation and increase
the production of collagen, respectively, thereby inducing OSMF
(6). However, Zn decreases the
activity of lysyl oxidase and inhibits the cross-linking of
collagen peptides. Zn also serves as an active centre for the
collagen degradation enzymes, collagenase and matrix
metalloproteinase. and thus promotes collagen degradation via the
action of these enzymes (45). Zn
deficiency further contributes to cancer initiation via the
activation of NF-κB and the consequent induction of tumorigenic
signalling (46). Overall, the
Cu/Zn ratio was found to be increased in patients with OSCC,
indicating the malignant condition.
The significant reduction in serum Se and Mo levels
with gutkha intake and OSMF and OSCC development suggests that the
levels of these trace elements were altered even prior to the
development of OSMF. The decrease in the level of Se is one of the
key serum characteristics in patients with advanced-stage head and
neck cancer. Various epidemiological studies have established that
Se offers protection against cancer. The loss of appetite and the
accompanying malnutrition and metabolic malnutrition caused by
tumour cells are other possible factors for the reduction in the
serum levels of Se (47).
Similarly, Mo has been shown to play a protective role against
gastric cancer in patients in China (48). Mo supplementation has also been
shown to decrease the incidence of N-nitrososarcosine ethyl
ester-induced cancer of the oesophagus and stomach in rats
(49).
Alterations in the levels of all four trace elements
in the serum of patients with gutkha intake without OSMF suggest
their use as tumour markers for the early detection of OSMF and
OSCC development.
In the present study, in saliva, the Cu level was
found to be increased only in patients with OSMF and OSCC,
indicating that the alteration was not seen due to gutkha intake,
but due to disease progression. In contrast to the increased serum
Zn level in all groups, the Zn level in the saliva was higher in
all the test groups, but did not differ significantly from that of
the control. Similar results were also been reported by Al-Rawi and
Talabani (50) and Ayinampudi and
Narsimhan (51). Al-Rawi and
Talabani noted a significant increase in Zn levels in the
pre-operative saliva of patients with oral cancer when compared
with the control group (50).
Similarly, Ayinampudi and Narsimhan (51) found that the Zn level was higher in
the saliva, thereby reducing the Cu:Zn ratio in the saliva of
patients with pre-malignant and malignant lesions of the oral
cavity. However, some conflicting results have been documented for
Zn levels in the saliva, with the level being decreased in patients
with OSMF and OSCC (52-54).
Herein, no significant differences were found in the
levels of Se and Mo in saliva, and their levels were identical to
those of the control. On the contrary, in serum, both the Se and Mo
levels were significantly reduced in all the groups.
Furthermore, age and sex analysis revealed that
changes in trace element levels were consistent, irrespective of
the age and sex of the participants. Therefore, trace elements can
be used for the early detection of pre-malignant and malignant
conditions across different age groups and sexes.
Standard reference values for serum levels of Cu,
Zn, Se and Mo in a healthy individual are 0.6-3.6, 0.6-1.5, 60-150
and 0.0-3.6 ng/ml, respectively (55-57).
However, these levels can vary from one individual to the other
based on their overall health condition and dietary intake.
Reference levels for salivary Cu, Zn, Se and Mo are less clearly
defined and are information on these is limited in the literature.
From existing studies, approximate values for Cu, Zn and Se have
been inferred to be 0.01-0.75 µg/ml (58,59),
0.05-2.36 µg/ml (59,60) and 0.03 ng/ml (59), respectively. When these trace
elements deviate from their normal levels, several health issues
can arise. In the present study, considering all the test groups,
the serum Cu level was increased by 48%, whereas the Zn, Se and Mo
levels were decreased by 26, 29 and 50%, respectively. By contrast,
the Cu and Zn levels in saliva were increased by 200 and 50%,
respectively; Se levels did not exhibit any notable no changes,
whereas the Mo levels were decreased by 50%. These alterations
suggest that deviations of 20-30% from the normal levels may
contribute to disease progression.
Overall, trace element levels were higher in serum
than those in saliva. The possible reason for this may be the rapid
absorption of trace elements into the bloodstream within 15 min of
ingesting gutkha (32). Given that
the serum level represents the current level of trace elements in
the body, it is considered to be more reliable than the salivary
level. Moreover, saliva samples tend to exhibit more variability
than serum samples due to local oral conditions, such as
mechanical, olfactory or psychological factors, as well as the
autonomic nervous system (61). In
contrast to saliva, the high levels of trace elements in serum
facilitate their easy and early detection. This early detection can
prevent potential health risks from increased or decreased levels
of trace elements. Hence, the clinical implications of detecting
trace elements in serum are crucial, offering a proactive approach
for the early detection and prediction of pre-malignant and
malignant conditions in patients.
The limitations of the present study arise from its
small group of participants. Furthermore, the dietary intake of the
patients was not recorded, which may have influenced the trace
element levels in serum and saliva. Hence, the role of dietary
factors in influencing the levels of these trace elements is not
yet known. Moreover, the high Cu content (mean, 302 nmol/g) of
areca nuts compared with other commonly consumed nuts (22-173
nmol/g) (62) may have
significantly altered the Cu levels of the consumers and may thus
have introduced differences in comparison with those who did not
consume the nut.
Moreover, in the present study, ICP-OES was used for
detecting trace elements, capable of identifying them within the
range of parts per million to parts per billion. Employing ICP-mass
spectrometry (ICP-MS), which is more sensitive and highly accurate
compared with ICP-OES, would have resulted in precise results. This
is due to the fact that ICP-MS uses isotopic variations and can
distinguish between isotopes of elements based on their
mass-to-charge range (https://veeprho.com/difference-between-icp-oes-and-icp-ms/;
https://lab-training.com/which-is-a-better-choice-icp-oes-or-icp-ms/;
https://www.drawellanalytical.com/icp-oes-vs-icp-ms%ef%bc%9a7-key-differences-analysis/).
Consequently, ICP-MS is capable of detecting trace element levels
in the part per trillion range. Hence, a more comprehensive
investigation, involving a larger and more randomized sample,
controlled dietary intake, and the use of ICP-MS, is required to
draw more robust conclusions.
In conclusion, the present study highlights the
alterations in serum and salivary levels of trace elements in
pre-malignant and malignant lesions, indicating disease
progression. As the saliva composition often varies, monitoring
serum trace element levels as diagnostic and prognostic markers may
aid in early detection and efficacious therapeutic management.
Acknowledgements
The authors would like to thank Mr. Palavardhan
Peddapalegani, biostatistician at Malla Reddy Medical College for
Women (Hyderabad, India) for performing the comprehensive
statistical analysis in the present study.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analysed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
VK was involved in the conceptualization of the
study, as well as in data analysis and interpretation, and in the
writing of the original draft. NK was involved in data analysis and
interpretation, in the writing of the final draft of the manuscript
and in the critical revision of the manuscript. KKRE was involved
in the conceptualization of the study, as well as in study
supervision, data analysis and interpretation, and in the critical
revision of the manuscript. SG was involved in data analysis and
interpretation, and in the writing of the original draft and the
final draft of the manuscript. HS was involved in the
conceptualization of the study, as well as in data analysis and
interpretation, and in the critical revision of the manuscript. SR
was involved in study supervision, as well as in data analysis and
interpretation, and in the critical revision of the manuscript. VK,
KKRE, and SG confirm the authenticity of all the raw data. All
authors have read and approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of MNR Dental College (Protocol ID: D139803007). All
participants written informed consent prior to obtaining their
data.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Tranby EP, Heaton LJ, Tomar SL, Kelly AL,
Fager GL, Backley M and Frantsve-Hawley J: Oral cancer prevalence,
mortality, and costs in medicaid and commercial insurance claims
data. Cancer Epidemiol Biomarkers Prev. 31:1849–1857.
2022.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Borse V, Konwar AN and Buragohain P: Oral
cancer diagnosis and perspectives in India. Sens Int.
1(100046)2020.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Johnson NW, Jayasekara P and Amarasinghe
AAHK: Squamous cell carcinoma and precursor lesions of the oral
cavity: Epidemiology and aetiology: Oral cancer
epidemiology/aetiology. Periodontology 2000. 57:19–37.
2011.PubMed/NCBI View Article : Google Scholar
|
|
4
|
McKinney R and Olmo H: Pathologic
Manifestations of Smokeless Tobacco. In: StatPearls. StatPearls
Publishing, Treasure Island, FL, 2023.
|
|
5
|
Sachdev PK, Freeland-Graves J, Beretvas SN
and Sanjeevi N: Zinc, Copper, and Iron in Oral Submucous Fibrosis:
A Meta-Analysis. Int J Dent. 2018(3472087)2018.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Passi D, Bhanot P, Kacker D, Chahal D,
Atri M and Panwar Y: Oral submucous fibrosis: Newer proposed
classification with critical updates in pathogenesis and management
strategies. Natl J Maxillofac Surg. 8:89–94. 2017.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Miļuna S, Melderis R, Sperga M, Skadiņš I,
Kroiča J and Rostoka D: Histopathological findings of oral mucosa
in smokeless tobacco users: Case report. TODENTJ.
16(e187421062212232)2022.
|
|
8
|
Sharma AD, Garg S, Singh MM, Deshmukh C,
Mishra A, Singh V and Sharma R: Pattern of smokeless tobacco
initiation and use among school going adolescents in Delhi, India:
A mixed method study. Asian Pac J Cancer Prev. 24:3187–3193.
2023.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Sankhla B, Kachhwaha K, Hussain SY, Saxena
S, Krishana-Sireesha S and Bhargava A: Genotoxic and carcinogenic
effect of Gutkha: A fast-growing smokeless tobacco. Addict Health.
10:52–63. 2018.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Javed F, Chotai M, Mehmood A and Almas K:
Oral mucosal disorders associated with habitual gutka usage: A
review. Oral Surg Oral Med Oral Pathol Oral Radiol Endod.
109:857–864. 2010.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Murti PR, Gupta PC, Bhonsle RB, Daftary
DK, Mehta FS and Pindborg JJ: Effect on the incidence of oral
submucous fibrosis of intervention in the areca nut chewing habit.
J Oral Pathol Med. 19:99–100. 1990.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Shih YH, Wang TH, Shieh TM and Tseng YH:
Oral Submucous fibrosis: A review on etiopathogenesis, diagnosis,
and therapy. Int J Mol Sci. 20(2940)2019.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Tilakaratne WM, Klinikowski MF, Saku T,
Peters TJ and Warnakulasuriya S: Oral submucous fibrosis: Review on
aetiology and pathogenesis. Oral Oncol. 42:561–568. 2006.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Murti PR, Bhonsle RB, Pindborg JJ, Daftary
DK, Gupta PC and Mehta FS: Malignant transformation rate in oral
submucous fibrosis over a 17-year period. Commun Dent Oral
Epidemiol. 13:340–341. 1985.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Tilakaratne WM, Ekanayaka RP and
Warnakulasuriya S: Oral submucous fibrosis: A historical
perspective and a review on etiology and pathogenesis. Oral Surg
Oral Med Oral Pathol Oral Radiol. 122:178–191. 2016.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Khalili J: Oral cancer: Risk factors,
prevention and diagnostic. Exp Oncol. 30:259–264. 2008.PubMed/NCBI
|
|
17
|
Bhattacharya PT, Misra SR and Hussain M:
Nutritional aspects of essential trace elements in oral health and
disease: An extensive review. Scientifica (Cairo).
2016(5464373)2016.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Laya A, Wangso H and Camargo JM: Trace
elements homeostasis in biological samples as new candidate
biomarkers for early diagnosis and prognostic of female breast
cancer and therapeutic response: Systematic review: Biomarkers for
early diagnosis of breast cancer. Arch Breast Cancer. 10:26–37.
2022.
|
|
19
|
Takahashi E, Imai K, Fukuyama M, Terata K,
Nanjo H, Ishiyama K, Hiroshima Y, Yatsuyanagi M, Kudo C, Morishita
A, et al: Changes in serum trace element concentrations before and
after surgery in resectable breast cancer. Anticancer Res.
42:5323–5334. 2022.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Singh Kainth H, Khandelwal D, Singh R,
Singh G and Puri S: Role of trace elements in breast cancer and
their characterization using X-Ray fluorescence techniques. In:
Trace Elements and Their Effects on Human Health and Diseases.
Joseph D (ed). IntechOpen, London, 2021.
|
|
21
|
Abbas AM, Kredy HM and Hasan MS: Selected
trace elements and heavy metals in the serum of postoperative
gastric cancer patients and their relationship to CEA. J Commun
Dis. 53:220–226. 2021.
|
|
22
|
Afzal A, Qayyum MA and Shah MH:
Comparative assessment of trace elements in the blood of gastric
cancer patients and healthy subjects. Biointerface Res Appl Chem.
11:10824–10843. 2020.
|
|
23
|
Tan C, Chen H and Xia C: Early prediction
of lung cancer based on the combination of trace element analysis
in urine and an Adaboost algorithm. J Pharm Biomed Anal.
49:746–752. 2009.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Araz O and Araz A: Are Trace Element
concentrations in lung cancer tissue associated with metastasis?
Eurasian J Med. 53:227–230. 2021.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Saikawa H, Nagashima H, Cho K, Chiba R,
Sera K, Shigeeda W, Tomoyasu M, Deguchi H, Takahashi F, Saito H, et
al: Relationship between trace element in tumor and prognosis in
lung cancer patients. Medicina (Kaunas). 57(209)2021.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Hande A, Bansod AV, Agrawal AG, Gadbail A
and Reche AM: Estimation of serum copper and zinc in patients of
oral submucous fibrosis in rural population. World J Dent.
11:478–481. 2021.
|
|
27
|
Swain N and Ray JG: Altered trace element
level and antioxidant activity in whole blood of oral Leukoplakia
and cancer patients in comparison with healthy controls. Int J Oral
Maxillofacial Pathol. 2:2–6. 2011.
|
|
28
|
Shetty SR, Babu S, Kumari S, Shetty P,
Hegde S and Karikal A: Role of serum trace elements in oral
precancer and oral cancer-a biochemical study. J Cancer Res Ther.
11:1–3. 2013.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Tyagi B, Bhargava D, Sharma R,
Chandarvarkar V and Sundersan P: Estimation of serum copper levels
in oral submucous fibrosis patients: A quantitative study. Act Scie
Dental Sci. 5:99–104. 2021.
|
|
30
|
Karapinar HS, Türkdoğan MK and Kiliçel F:
Serum trace element levels of liver cirrhosis and pancreatic cancer
patients. Arch Community Med Public Health. 8:055–061. 2022.
|
|
31
|
Choi R, Kim MJ, Sohn I, Kim S, Kim I, Ryu
JM, Choi HJ, Kim JM, Lee SK, Yu J, et al: Serum trace elements and
their associations with breast cancer Subgroups in Korean breast
cancer patients. Nutrients. 11(37)2018.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Kode MA and Karjodkar FR: Estimation of
the serum and the salivary trace elements in OSMF patients. J Clin
Diagn Res. 7:1215–1218. 2013.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Denoyer D, Masaldan S, La Fontaine S and
Cater MA: Targeting copper in cancer therapy: ‘Copper That
Cancer.’. Metallomics. 7:1459–1476. 2015.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Thorling EB and Thorling K: The clinical
usefulness of serum copper determinations in Hodgkin's disease. A
retrospective study of 241 patients from 1963-1973. Cancer.
38:225–231. 1976.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Bargellini A, Piccinini L, De Palma M,
Giacobazzi P, Scaltriti S, Mariano M, Roncaglia R and Borella P:
Trace elements, anxiety and immune parameters in patients affected
by cancer. J Trace Elem Med Biol. 17 (Suppl 1):S3–S9.
2003.PubMed/NCBI
|
|
36
|
Federico A, Iodice P and Federico P, Del
Rio A, Mellone M, Catalano G and Federico P: Effects of selenium
and zinc supplementation on nutritional status in patients with
cancer of digestive tract. Eur J Clin Nutr. 55:293–297.
2001.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Fisher GL, Byers VS, Shifrine M and Levin
AS: Copper and zinc levels in serum from human patients with
sarcomas. Cancer. 37:356–363. 1976.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Oyama T, Kawamoto T, Matsuno K, Osaki T,
Matsumoto A, Isse T, Nakata S, Ozaki S, Sugaya M, Yasuda M, et al:
A case-case study comparing the usefulness of serum trace elements
(Cu, Zn and Se) and tumor markers (CEA, SCC and SLX) in non-small
cell lung cancer patients. Anticancer Res. 23:605–612.
2003.PubMed/NCBI
|
|
39
|
Khanna S: Immunological and biochemical
markers in oral carcinogenesis: The public health perspective. Int
J Environ Res Public Health. 5:418–422. 2008.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Li G, Brockman JD, Lin SW, Schell LA and
Robertson JD: Measurement of the Trace Elements Cu, Zn, Fe, and Mg
and the Ultratrace Elements Cd, Co, Mn, and Pb in Limited Quantity
Human Plasma and Serum Samples by Inductively Coupled Plasma-Mass
Spectrometry. Am J Analy Chem. 3:646–650. 2012.
|
|
41
|
Kara D: Evaluation of trace metal
concentrations in some herbs and herbal teas by principal component
analysis. Food Chem. 114:347–354. 2009.
|
|
42
|
Momen AA, Ali DMH and Khalid MA:
Assessment of digestion procedure for determination of trace
elements by ICP-OES. Open Science Repository Chemistry.
(e70081933)2013.
|
|
43
|
Kumar LB, Mathew P, Madhavan N, Siddique
S, Kshetrimayum N and Iyer K: Evaluation of mast cells and burning
sensation in various stages of Oral Submucous Fibrosis. J Oral Biol
Craniofac Res. 10:430–434. 2020.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Trivedy CR, Warnakulasuriya KA, Peters TJ,
Senkus R, Hazarey VK and Johnson NW: Raised tissue copper levels in
oral submucous fibrosis. J Oral Pathol Med. 29:241–248.
2000.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Desai V, Gaurav I, Kumar MV, Sharma R and
Bathi R: Molecular analysis of trace elements in oral submucous
fibrosis and future perspectives. Univ Res J Dent. 4(26)2014.
|
|
46
|
Hosthor SS, Mahesh P, Priya SA, Sharada P,
Jyotsna M and Chitra S: Quantitative analysis of serum levels of
trace elements in patients with oral submucous fibrosis and oral
squamous cell carcinoma: A randomized cross-sectional study. J Oral
Maxillofac Pathol. 18:46–51. 2014.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Virtamo J, Valkeila E, Alfthan G, Punsar
S, Huttunen JK and Karvonen MJ: Serum selenium and risk of cancer.
A prospective follow-up of nine years. Cancer. 60:145–148.
1987.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Cao GH, Yan SM, Yuan ZK, Wu L and Liu YF:
A study of the relationship between trace element Mo and gastric
cancer. World J Gastroenterol. 4:55–56. 1998.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Luo XM, Wei HJ and Yang SP: Inhibitory
effects of molybdenum on esophageal and forestomach carcinogenesis
in rats. J Natl Cancer Inst. 71:75–80. 1983.PubMed/NCBI
|
|
50
|
Al-Rawi NH and Talabani NGA: Quantitative
analysis of trace elements in saliva of oral cancer patients from
Iraq. J Coll Dentistry. 17:32–35. 2005.
|
|
51
|
Ayinampudi BK and Narsimhan M: Salivary
copper and zinc levels in oral pre-malignant and malignant lesions.
J Oral Maxillofac Pathol. 16:178–182. 2012.PubMed/NCBI View Article : Google Scholar
|
|
52
|
Kanjani V, Rani A and Kanjani D: Salivary
evaluation of trace elements in oral submucous fibrosis-an atom
absorption spectroscopic study. J Med Sci Clin Res. 7:43–47.
2019.
|
|
53
|
Shetty SR, Babu S, Kumari S, Shetty P,
Hegde S and Karikal A: Status of trace elements in saliva of oral
precancer and oral cancer patients. J Can Res Ther. 11:146–149.
2015.PubMed/NCBI View Article : Google Scholar
|
|
54
|
Okade A, Hallikeri K and Trivedi D:
Salivary estimation of copper, iron, zinc and manganese in oral
submucous fibrosis patients: A case-control study. Clin Cancer
Investig J. 4:302–306. 2015.
|
|
55
|
Khanna S, Udas AC, Kumar GK, Suvarna S and
Karjodkar FR: Trace elements (copper, zinc, selenium and
molybdenum) as markers in oral sub mucous fibrosis and oral
squamous cell carcinoma. J Trace Elem Med Biol. 27:307–311.
2013.PubMed/NCBI View Article : Google Scholar
|
|
56
|
Lossow K, Schwarz M and Kipp AP: Are trace
element concentrations suitable biomarkers for the diagnosis of
cancer? Redox Biol. 42(101900)2021.PubMed/NCBI View Article : Google Scholar
|
|
57
|
Liu X, Zhang Y, Piao J, Mao D, Li Y, Li W,
Yang L and Yang X: Reference values of 14 serum trace elements for
pregnant Chinese Women: A cross-sectional study in the China
Nutrition and Health Survey 2010-2012. Nutrients.
9(309)2017.PubMed/NCBI View Article : Google Scholar
|
|
58
|
Rice EW and Goldstein NP: Copper content
of saliva of normal subjects and treated Wilson's disease patients.
Metabolism. 15:1050–1053. 1966.PubMed/NCBI View Article : Google Scholar
|
|
59
|
Baima G, Iaderosa G, Corana M, Romano F,
Citterio F, Giacomino A, Berta GN and Aimetti M: Macro and trace
elements signature of periodontitis in saliva: A systematic review
with quality assessment of ionomics studies. J Periodontal Res.
57:30–40. 2022.PubMed/NCBI View Article : Google Scholar
|
|
60
|
Mathur A, Wallenius K and Abdulla M:
Relation between zinc content in saliva and blood in healthy human
adults. Scand J Clin Lab Invest. 37:469–472. 1977.PubMed/NCBI
|
|
61
|
Sánchez J, Fuentes N, Ibañez-López FJ,
López-García I and Gutiérrez AM: A multi-herd study shows that
saliva is more than a reflection of serum biomarkers in pigs.
Animal. 15(100413)2021.PubMed/NCBI View Article : Google Scholar
|
|
62
|
Trivedy C, Baldwin D, Warnakulasuriya S,
Johnson N and Peters T: Copper content in Areca catechu (betel nut)
products and oral submucous fibrosis. Lancet.
349(1447)1997.PubMed/NCBI View Article : Google Scholar
|