Introduction
Myxedema crisis is a decompensated form of
hypothyroidism associated with high mortality rates. The condition
is more common among females and the elderly. A notable proportion
of patients (39-51%) are diagnosed with hypothyroidism at their
presentation as myxedema crisis (1,2). Central
hypothyroidism accounts for 5-17% of patients presenting with
myxedema crisis (2,3). Sheehan's syndrome is a rare condition
characterized by panhypopituitarism due to post-partum pituitary
necrosis. Sheehan's syndrome presenting as a myxedema crisis is
extremely rare.
The present study describes the case of a patient
with Sheehan's syndrome with a first-time presentation as myxedema
crisis. Furthermore, the patient developed acute parkinsonism
during the recovery phase of the myxedema crisis, resulting in a
prolongation of the altered sensorium. Acute parkinsonism leading
to prolongation of the altered sensorium in a patient of myxedema
crisis has not been reported previously, at least to the best of
our knowledge.
Case report
A 31-year-old female patient presented with multiple
episodes of vomiting for 1 week and hypoactive delirium for 3 days.
The patient was evaluated at a local medical facility for the same
and was found to have hyponatremia. She was managed for
hyponatremia with 3% saline, but was referred to the Tertiary Care
Centre at Dr Rajendra Prasad Government Medical College Kangra at
Tanda (Kangra, India) due to the persistence of altered sensorium.
Upon evaluation, she was found to have a history of fever 1 week
prior. She had no history of headaches, abnormal body movements, or
weakness in any body part. Her previous history was significant,
with secondary amenorrhea and the failure of lactation following
the delivery of a child 11 years prior. The child was delivered at
home and there was no history of post-partum haemorrhage. At the
time of admission, the patient was drowsy with a Glasgow coma scale
of 11/15, had bradycardia (pulse rate-, 50 beats/min) and
hypotension (blood pressure, 84/50 mmHg). Her oral temperature was
91.5˚F (33.1˚C) and she had pallor. Upon a neurological
examination, the pupils were found to be bilaterally equal and
reacting to light. There was no facial asymmetry. Neck rigidity and
Kernig's sign were absent. There was a delayed relaxation of deep
tendon reflexes. Bilateral plantar reflexes were flexor. A
cardiovascular examination revealed bradycardia, although other
systemic examinations were within normal limits.
An analysis revealed that her haemoglobin level was
106 gm/l (normal range, 120-150 gm/l), the total leucocyte count
was 4.1x109/l (normal range, 4-10) and her platelet
count was 90,000/mm³ (range, 1.5-4.5 lakh); the differential counts
were: Polymorphs, 88%; lymphocytes, 10%; eosinophils, 1%;
monocytes, 1%; erythrocyte sedimentation rate, 40 mm/1st hour;
random blood glucose, 4.662 mmol/l; urea, 7.14 mmol/l (normal
range, 4.64-16.06 mmol/l); creatinine, 33.5 µmol/l (normal range,
35.36-106.08 µmol/l); serum sodium, 120 mmol/l (normal range,
135-155 mmol/l); serum potassium, 4 mmol/l (normal range, 3.5-5.5
mmol/l); aspartate aminotransferase, 56 IU (normal range, 5-34 IU);
alanine aminotransferase, 53 IU (normal range, 6-40 IU); and
alkaline phosphatase, 73 IU (normal range, 15-112 IU). Scrub and
dengue serology were negative. HBsAg, hepatitis C virus and HIV
serology were non-reactive. The results of a urine examination,
chest X-ray and ultrasound abdomen were all within normal limits.
Her arterial blood gas analysis, cerebrospinal fluid examination
and electroencephalogram were within normal limits. Given her
history of altered sensorium, the delayed relaxation of deep tendon
reflexes, bradycardia and hyponatremia, myxedema crisis was
suspected and her myxedema score was calculated. Her myxedema score
was 75, suggesting myxedema crisis. Thyroid function tests revealed
that T3 was <0.616 nmol/l (normal range, 1.08-3.14 nmol/l), T4
was 39.12 nmol/l (normal range, 64.35-141.57 nmol/l) and thyroid
stimulating hormone (TSH) was 1.14 mIU/l (normal range, 0.550-4.780
mIU/l), suggestive of secondary hypothyroidism as opposed to sick
euthyroid syndrome. Since there was a history of lactation failure,
secondary amenorrhea and the delayed relaxation of deep tendon
reflexes, the possibility of secondary hypothyroidism was kept.
Samples for the pituitary hormonal profile were sent and management
for the myxedema crisis was initiated. The patient was managed with
oral levothyroxine 500 µg stat followed by 100 µg once daily
through a Ryle's tube, hydrocortisone infusion, intravenous fluids,
injectable antibiotics and rewarming. Her pituitary hormonal
profile was suggestive of panhypopituitarism [prolactin, 76.08
pmol/l (normal range, 145.21-1,161.73 pmol/l); adrenocorticotropic
hormone, 1.30 pmol/l (normal range, 1.58-13.92 pmol/l); cortisol,
108.98 nmol/l (normal range, 120.18-626.75 nmol/l); luteinising
hormone, 5.4 IU/l (normal range, 1.9-12.5 IU/l); follicle
stimulating hormone, 3.11 IU/l (normal range, 3.85-8.78 IU/l); and
estradiol, 36.71 pmol/l (normal range, 71.58-528.62 pmol/l)]. The
hormonal profile of the patient is presented in Table I. The patient exhibited an
improvement in bradycardia, hypotension and hyponatremia over the
ensuing 4 days; however, there was no improvement in the altered
sensorium. She was awake, but not able to speak or move her limbs.
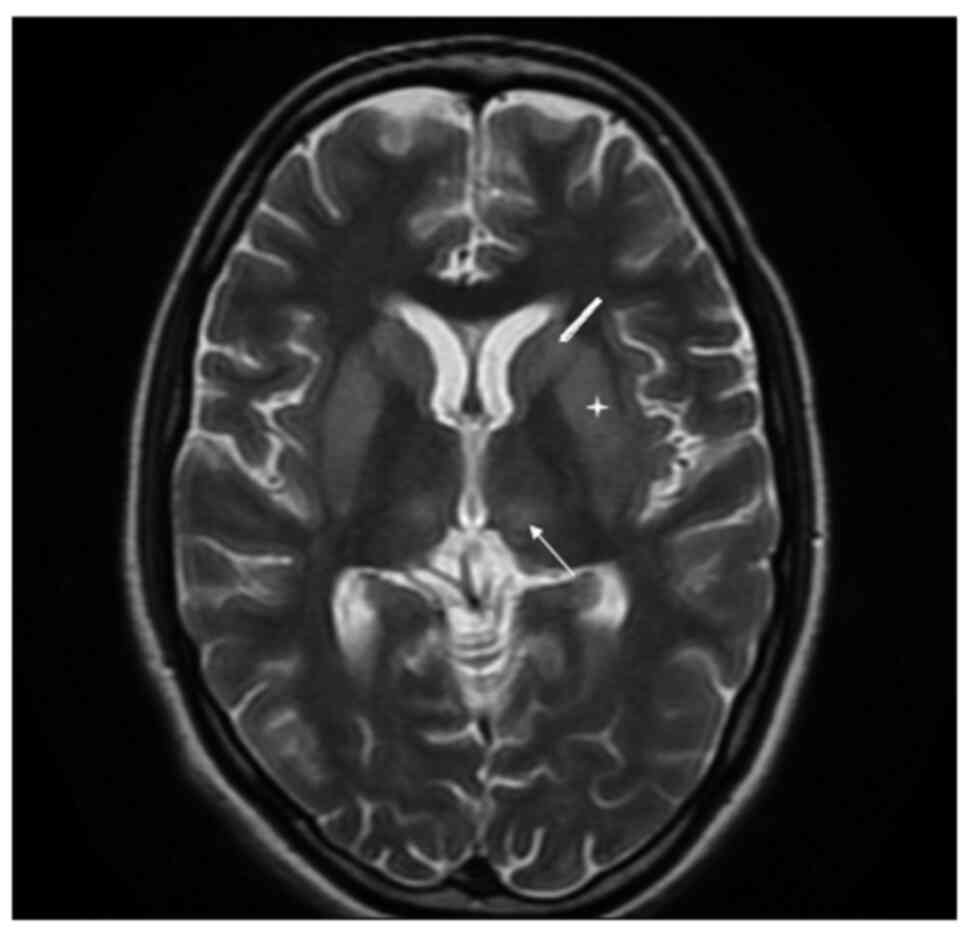
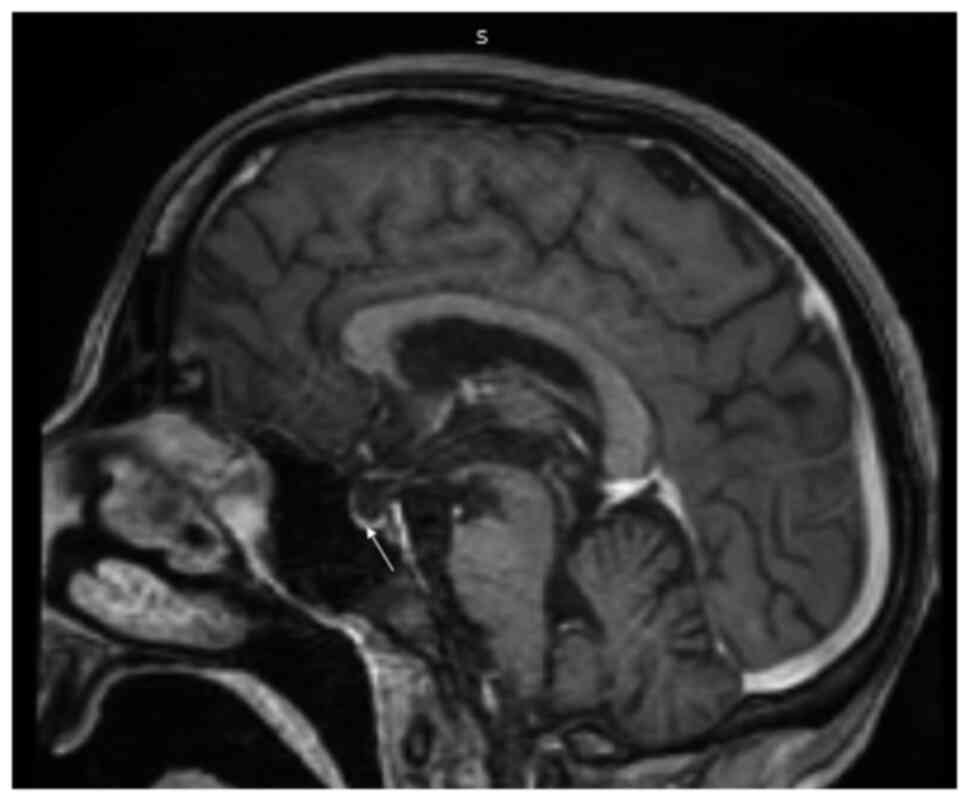
A repeat neurological examination was performed, which revealed
cogwheel rigidity and paraparesis. The possibility of acute
parkinsonism was kept. Magnetic resonance imaging of the sella and
brain was suggestive of an empty sella and extrapontine
myelinolysis (Figs. 1 and 2), substantiating the diagnosis of
Sheehan's syndrome with acute parkinsonism. The patient was
commenced on levodopa/carbidopa following which there was a partial
improvement in symptoms. She was discharged on oral hydrocortisone,
levothyroxine, ethinyl estradiol and progesterone, and
physiotherapy was recommended. At the 6th month of follow-up, the
patient was communicating well, the paraparesis had improved and
she could perform all household activities.
 | Table IHormonal profile of the patient in the
present case report. |
Table I
Hormonal profile of the patient in the
present case report.
| Parameter | Patient value | Reference range |
|---|
| T3 | <40 ng/dl | 70-204 ng/dl |
| T4 | 3.04 µg/dl | 5-11 µg/dl |
| TSH | 1.14 µIU/ml | 0.550-4.780
µIU/ml |
| Prolactin | 1.75 ng/dl | 3.34-26.72 ng/ml |
| ACTH | 5.9 pg/ml | 7.2-63.3 pg/ml |
| Cortisol | 3.95 µg/dl | 4.3-22.4 µg/dl |
| LH | 5.4 mIU/ml | 1.9-12.5 mIU/ml |
| FSH | 3.11 mIU/ml | 3.85-8.78 mIU/ml |
| Estradiol | 10 pg/ml | 19.5-144 pg/ml |
Discussion
Sheehan's syndrome is characterised by the
development of hypopituitarism due to post-partum pituitary
necrosis. Severe post-partum haemorrhage leads to an impairment in
the blood supply of the physiologically enlarged pituitary gland
during pregnancy, culminating in pituitary necrosis. Owing to the
improvement in obstetrical care, Sheehan's syndrome is currently
rare in developed countries, but is still frequently encountered in
developing nations. In addition, it is more frequently encountered
with home deliveries as compared to institutional deliveries
(4). Although post-partum
haemorrhage is the most critical factor determining the development
of Sheehan's syndrome, other factors, such as genetic
susceptibility and autoimmunity also play a role. Growth hormone
deficiency is the most common deficiency observed in different
studies (5-8).
However, data regarding prolactin and TSH deficiencies are
variable. Although previous studies have reported prolactin
deficiency to be more frequent, a study in India observed TSH
deficiency to be more common (9).
Chronic Sheehan's syndrome typically has non-specific features such
as easy fatigability, lassitude, giddiness, etc., and thus often
remains undiagnosed for years. The first-time presentation of
Sheehan's syndrome in the emergency room as a myxedema crisis is
rare. In a previous study with a cohort of 23 patients of myxedema
crisis, 3 patients had Sheehan's syndrome as the aetiology of
hypothyroidism (1).
Myxedema crisis is an under-recognised differential
of patients visiting the emergency department with an altered
sensorium. The most critical part of the management of a myxedema
crisis is the timely suspicion of diagnosis and early initiation of
treatment (2). Hyponatremia is a
common metabolic abnormality in the emergency room and can itself
present as an altered sensorium. Hence, the suspicion of myxedema
crisis in the setting of hyponatremia, particularly when the
patient has not previously been diagnosed with hypothyroidism,
becomes difficult. The absence of features of frank hypothyroidism
in secondary hypothyroidism due to TSH-independent secretion of
levothyroxine, further adds to the difficulty (10). Moreover, the thyroid profile in
secondary hypothyroidism is similar to sick euthyroid syndrome,
which can be seen in critically ill patients of any aetiology. The
history of lactation failure and secondary amenorrhea in the
patient described herein was the key to the suspicion of secondary
hypothyroidism. The presence of a multitude of features like
hyponatremia, hypotension, bradycardia, hypothermia, etc. in a
patient of altered sensorium indicates towards the diagnosis of
myxedema crisis in such a setting. The use of myxedema score >60
aids in the confirmation of diagnosis (11).
Extrapontine myelinolysis (EPM) as a cause of
persistent altered sensorium during the recovery phase of myxedema
crisis has not been reported previously, at least to the best of
our knowledge. Persistent altered sensorium in a patient with
myxedema crisis can be due to electrolyte abnormalities,
cerebrovascular accident, septic encephalopathy, myxedema psychosis
and slow recovery in the elderly. Extrapontine myelinolysis occurs
due to a rapid osmotic shift and usually develops 7-14 days
following an acute insult (12).
Alcoholism, malnutrition, cirrhosis and severe burns are
well-recognized predisposing factors for the development of EPM
(13). However, hypocortisolism as a
predisposing factor for EPM has only recently been recognized
(14). Although the rapid correction
of hyponatremia of any aetiology can lead to EPM, chances increase
in the setting of undiagnosed hypocortisolism. Rapid steroid
replacement in the setting of hypocortisolism along with the
correction of hyponatremia by 3% saline can add to damage due to a
steep rise in sodium levels. The patient in the present study had a
history of secondary amenorrhea and lactation failure; however,
Sheehan's syndrome was not suspected at her initial medical
contact. Thus, the case in the present study also reiterates the
importance of a basic history and clinical examination, while
treating an electrolyte imbalance. In general, demyelination is
associated with a poor prognosis with the persistence of morbidity
following treatment. However, EPM associated with hypocortisolism
has been shown to have a more favourable outcome, as observed in
the patient described herein (15).
In conclusion, the present study describes a case
with the first-time presentation of Sheehan's syndrome as a
myxedema crisis. Sheehan's syndrome remains prevalent in developing
countries and should be suspected in females with a history of
lactation failure and secondary amenorrhea especially with home
delivery. The present case report reiterates the importance of
basic history and clinical examination, while treating an
electrolyte imbalance and exercising caution during correction. The
timely suspicion of myxedema crisis in patients presenting with an
altered sensorium in the emergency room remains the most crucial
part of managing the condition. Furthermore, the case described
herein highlights the importance of being vigilant during the
recovery phase of a myxedema crisis, and considering alternative
causes if altered sensorium persists.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
Data sharing is not applicable to this article, as
no datasets were generated or analyzed during the current
study.
Authors' contributions
RG wrote the initial draft of the manuscript and
contributed to patient management. SC edited and finalised the
draft of the manuscript and contributed to patient management. VS
helped in editing the manuscript and contributed to patient
management. NSC helped in editing the manuscript and contributed to
the radiology-related patient management. NC helped in editing the
manuscript and contributed to patient management. DK helped in
editing the manuscript and contributed to patient management. All
authors have read and approved final version of the manuscript. RG
and SC confirm the authenticity of all the raw data.
Ethics approval and consent to
participate
Written informed consent for participation was
obtained from the patient.
Patient consent for publication
Written informed consent for publication was
obtained from the patient for the publication of the present case
report and any related images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Dutta P, Bhansali A, Masoodi SR, Bhadada
S, Sharma N and Rajput R: Predictors of outcome in myxoedema coma:
A study from a tertiary care centre. Crit Care.
12(R1)2008.PubMed/NCBI View
Article : Google Scholar
|
|
2
|
Chaudhary S, Das L, Sharma N, Sachdeva N,
Bhansali A and Dutta P: Utility of myxedema score as a predictor of
mortality in myxedema coma. J Endocrinol Invest. 46:59–65.
2023.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Wartofsky L: Myxedema coma. Endocrinol
Metab Clin North Am. 35:687–698, vii-viii. 2006.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Zargar AH, Singh B, Laway BA, Masoodi SR,
Wani AI and Bashir MI: Epidemiologic aspects of postpartum
pituitary hypofunction (Sheehan's syndrome). Fertil Steril.
84:523–528. 2005.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Diri H, Tanriverdi F, Karaca Z, Senol S,
Unluhizarci K, Durak AC, Atmaca H and Kelestimur F: Extensive
investigation of 114 patients with Sheehan's syndrome: A continuing
disorder. Eur J Endocrinol. 171:311–318. 2014.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Gokalp D, Alpagat G, Tuzcu A, Bahceci M,
Tuzcu S, Yakut F and Yildirim A: Four decades without diagnosis:
Sheehan's syndrome, a retrospective analysis. Gynecol Endocrinol.
32:904–907. 2016.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Kelestimur F, Jonsson P, Molvalilar S,
Gomez JM, Auernhammer CJ, Colak R, Koltowska-Häggström M and Goth
MI: Sheehan's syndrome: baseline characteristics and effect of 2
years of growth hormone replacement therapy in 91 patients in
KIMS-Pfizer international metabolic database. Eur J Endocrinol.
152:581–587. 2005.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Lim CH, Han JH, Jin J, Yu JE, Chung JO,
Cho DH, Chung DJ and Chung MY: Electrolyte imbalance in patients
with Sheehan's syndrome. Endocrinol Metab (Seoul). 30:502–508.
2015.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Laway B, Misgar R, Mir S and Wani A:
Clinical, hormonal and radiological features of partial Sheehan's
syndrome: An Indian experience. Arch Endocrinol Metab. 60:125–129.
2016.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Brent GA and Weetman AP: Hypothyroidism
and thyroiditis. In: Williams Textbook of Endocrinology. Melmed S,
Koenig R, Rosen C, Auchus R and Goldfine A (eds). 14th edition.
Elsevier, Philadelphia, PA, p423, 2020.
|
|
11
|
Popoveniuc G, Chandra T, Sud A, Sharma M,
Blackman MR, Burman KD, Mete M, Desale S and Wartofsky L: A
diagnostic scoring system for myxedema coma. Endocr Pract.
20:808–817. 2014.PubMed/NCBI View Article : Google Scholar
|
|
12
|
John TM, Jacob CN, Xavier J, Kondanath S,
Ittycheria CC and Jayaprakash R: A case of acute onset
parkinsonism. Qatar Med J. 2013:29–32. 2013.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Singh TD, Fugate JE and Rabinstein AA:
Central pontine and extrapontine myelinolysis: A systematic review.
Eur J Neurol. 21:1443–1450. 2014.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Imam YZ, Saqqur M, Alhail H and Deleu D:
Extrapontine myelinolysis-induced parkinsonism in a patient with
adrenal crisis. Case Rep Neurol Med. 2012(327058)2012.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Perikal PJ, Jagannatha AT, Khanapure KS,
Furtado SV, Joshi KC and Hegde AS: Extrapontine myelinolysis and
reversible parkinsonism after hyponatremia correction in a case of
pituitary adenoma: Hypopituitarism as a predisposition for osmotic
demyelination. World Neurosurg. 118:304–310. 2018.PubMed/NCBI View Article : Google Scholar
|