Introduction
Lung cancer is the malignant neoplasm with the
highest incidence and is the primary cause of cancer-related
mortality worldwide; with >1,800,000 novel cases and ~1,600,000
fatalities estimated in 2012 (1).
Incidence rates in the general population are closely associated
with the incidence of tobacco smoking, as the majority of lung
cancer cases are linked to this single risk factor (2). As a consequence of the multiple
campaigns adopted in previous decades against smoking in the
majority of Western countries, a decrease in the incidence of lung
cancer was registered in males from ~78 novel cases per 100,000
inhabitants per year between 1992–1998 to ~67/100,000 between
2005–2010 (3). However, incidence
rates continuously increase in developing countries and in females,
due to progressively increasing rates of smoking (3). The world standardised incidence rates
of lung cancer were augmented by 22% among females and decreased by
3% among males in the period between 1985 and 2002 (4). Considering the current smoking
trends, it is calculated that by 2030, lung cancer may affect
females and males equally (5).
Despite recent developments in the diagnosis,
clinical management and medical and surgical therapy of lung
cancer, mortality rates remain high. The 5-year relative survival
rate for lung cancer for the period between 1995 and 2001 was
15.7%, reflecting a steady but slow improvement from 12.5% in the
period between 1974 and 1976. More recent studies have estimated a
5 year survival rate of ~16% in the USA (6,7).
Several factors determine such high rates of mortality in patients
with lung cancer. The most important are: i) Insufficient campaigns
against smoking, pollution and other risk factors for lung cancer;
ii) lack of effective screening strategies; iii) subclinical
evolution of early stage disease; iv) delays in the diagnosis and
clinical assessment of patients with suspicious signs and symptoms;
v) insufficient comprehension of the pathophysiological mechanisms
of the disease; and, as a consequence, vi) lack of effective
treatment strategies, particularly for patients with advanced-stage
disease.
Although the pathophysiology of lung cancer remains
to be elucidated, a great quantity of research has been performed,
particularly in the last two decades, and certain findings were
translated into clinical practice. One of the most relevant
insights was the determination of the role of the deregulation of
the epidermal growth factor receptor (EGFR) for patients with
non-small cell lung cancer (NSCLC). It was identified that EGFR was
often overexpressed and aberrantly activated in NSCLC, and several
activating mutations within the kinase domain of the EGFR
gene were detected in lung adenocarcinomas (8). As a consequence, these tumours were
highly sensitive to the EGFR-tyrosine kinase inhibitors (TKIs).
TKIs were subsequently adopted into clinical practice, offering an
additional therapeutic option in patients with lung
adenocarcinomas. However, the increased frequency of resistance to
TKIs reduced the initial enthusiasm associated with the use of this
therapeutic agent (8).
Nevertheless, the identification of EGFR mutations in
patients with lung cancer remains of great importance for their
clinical management and prognosis.
Assessment of the EGFR mutational status has
therefore become a crucial step in the molecular classification of
patients, with regards to treatment strategy. Different techniques
are currently in use for the detection of TKI-sensitizing mutations
in the EGFR gene at the somatic level (9). Although several approaches have been
demonstrated to be more sensitive in detecting such EGFR
gene variants [predominantly, those based on quantitative
polymerase chain reaction (PCR) strategies], the most frequently
used method is Sanger sequencing (10). Despite its well-recognised low
sensitivity, this technique is considered the gold standard for
mutational analysis (11,12). The quality of the specimen
available for analysis represents a variable, which profoundly
affects EGFR mutational classification. It is postulated
that genomic DNA obtained from a quality-assessed tissue sample may
markedly increase the sensitivity of the assessment, particularly
when the Sanger sequencing approach is used. In addition, this
factor is important in patients that do not require surgery,
considering the intrinsic technical difficulties of lung biopsy
methods and considering the possibility for complications that may
be severe in certain instances.
The aim of the present study was to investigate the
impact of the quality of the tissue sample, expressed as a
percentage of neoplastic cells in the specimen, as well as the type
of analysed lesions, represented by primary or secondary tumours
and biopsy (transcutaneous or endoscopic) or surgical specimens, on
a sequencing-based mutation analysis of the kinase domain of the
EGFR gene in patients with lung adenocarcinomas.
Materials and methods
Samples
A total of 515 patients with
histologically-confirmed diagnosis of NSCLC and regular follow-up
in Sardinia, Italy were recruited in the present study. They were
consecutively collected between September 2010 and May 2013,
regardless of age at diagnosis and disease characteristics. All
patients were of Sardinian origin as determined by the place of
birth of the patient’s parents. Clinical and pathological features
for the assessment of the disease stage at diagnosis, as well as of
the onset age and anatomical location of the neoplasia, were
confirmed using medical records and pathology reports.
Formalin-fixed paraffin embedded (FFPE) tissue samples from NSCLC
patients were obtained from the archives of the pathology
institutions involved in the present study [University of Sassari,
Sassari, Italy; Oncologic Hospital of Cagliari, Cagliari, Italy and
the Local Health Units of Olbia (Olbia, Italy) and Nuoro (Nuoro,
Italy)]. Tissue samples were evaluated for the content of
neoplastic cells using light microscopy. Paraffinized sections from
each patient were stained with Harris hematoxylin and aqueous eosin
1% (Leica Biosystems Richmond, Inc., Richmond, IL, USA) and
examined under an Olympus BX51 optical microscope (Olympus, Center
Valley, PA, USA); minimal tumoral cellularity (proportion and
number of tumor cells) was established in all samples.
All patients were informed of the aims of the study
and prior to collection of the tissue sample, gave written informed
consent. The present study was reviewed and approved by the ethical
review board of the Local Health Agency of Sassari.
Mutation analysis
All tumour tissues were collected and processed at
the laboratory of the Institute of Biomolecular Chemistry (Sassari,
Italy). Genomic DNA was isolated from tissue sections using a
standard protocol and DNA quality was assessed for each specimen.
Paraffin was removed from FFPE samples by treatment with Bio-Clear
(Bio-optica, Milan, Italy) and DNA was purified using the QIAamp
DNA FFPE Tissue kit (Qiagen Inc., Valencia, CA, USA).
The coding sequence and splice junctions of exons 19
and 21 (for all cases), as well as exon 18 for a large fraction of
the patients (incompleteness was due to the low quantity of
available tumour tissue samples) in the EGFR gene were
screened for mutations by direct automated sequencing. Briefly, PCR
was performed on 25–50 ng of isolated genomic DNA in a 9700 Thermal
cycler (Life Technologies, Carlsbad, CA, USA) using 0.5 μM
of each specific primer, 1.5 μM MgCl2, 0.2
μM dNTPs, and 1U AmpliTaq Polymerase (GE Healthcare Life
Sciences, Piscataway, NJ, USA). PCR assays were performed by 30
cycles of denaturation at 94°C, primer annealing at 56–64°C
(depending on primers), and polymerase extension at 72°C. All ll
PCR-amplified products were directly sequenced using an automated
fluorescence-based cycle sequencer (ABI PRISM 3100; Life
Technologies), as previously described (13). Primer sequences for PCR-based
assays were designed and optimised in the aforementioned laboratory
and they are available upon request.
Statistical analysis
A descriptive analysis for qualitative and
quantitative variables was conducted using proportions and the mean
± standard deviation (SD), respectively. An inferential analysis
was performed for the clinical and demographic variables in terms
of proportion of neoplastic cells in the specimen. P≤0.05 was
considered to indicate a statistically significant difference. Data
were analysed using the statistical software STATA 12®
(StataCorp LP, College Station, TX, USA).
Results
Among the 515 cases examined, 357 (69.3%) were male
and 158 (30.7%) were female. The mean age was 64.9 years (SD:10.1).
A total of 382 patients (84.5%) were active tobacco smokers or had
a history of smoking, while the remaining 133 patients (15.5%) had
never smoked. A total of 452 specimens (87.8%) were obtained from
primary lung lesions, whereas 63 (12.2%) were obtained from
metastatic lesions. The anatomical distribution of metastatic
lesions was as follows: Lymph nodes, 19 (30.2%); liver, 15 (23.8%);
bone, 12 (19.1%); central nervous system, 7 (11.1%); pleura, 4
(6.3%); skin, 2 (3.2%); and other tissues, 4 (6.3%). A total of 429
tissue samples (83.3%) were obtained from biopsy (transcutaneous or
endoscopic), while 86 samples (16.7%) were obtained from surgical
specimens.
The total number of EGFR mutations found was
59 (11.5%). TKI-sensitizing mutations in EGFR exons 18, 19,
and 21 accounted for 1 (1.7%), 30 (51%) and 28 (47.3%) cases,
respectively. The types of EGFR mutations observed are
listed in Table I. The
age-distribution of these mutations included 4
EGFR-mutations (23.5%) among the 17 patients aged <45
years. Among the other age classes, EGFR mutations were
identified in 7/37 (18.9%) and 12/98 (12.2%) of the cases aged
between 45 and 50 years and between 51 and 60 years, respectively.
Approximately 10% of EGFR-mutation cases were found in patients
>60 years old. The global number of EGFR mutations was
significantly higher in females than in males [35/158 (22.2%) vs.
24/357 (6.7%)], due to a consistently higher incidence of EGFR exon
19 mutation in females. According to the smoking status, EGFR
mutations were found to be significantly more common in patients
that had never smoked (52.9%) as compared with patients that had
smoked or continue to smoke (5.5%). Finally, the distribution of
the mutations among primary and metastatic tissues demonstrated no
statistically significant differences in the proportions of EGFR
mutations detected in primary lung adenocarcinomas (51/452
mutations, 11.3%) and those found in metastatic samples (8/63
mutations, 12.7%). Table II
summarises the distribution of EGFR mutations according to patient
characteristics.
 | Table ISequence variations in epidermal
growth factor receptor gene among the 59 mutated cases found. |
Table I
Sequence variations in epidermal
growth factor receptor gene among the 59 mutated cases found.
| No. of positive cases
(%) | EGFR exon | DNA change | Amino acid
change | Effect | Designation |
|---|
| 1 (1.7) | 18 | c.2154 G>C | p.Gly719Ala | Missense | G719A |
| 22 (37.2) | 19 | c.2235-2249
del15 | p.del746_750 | In-frame
deletion | delELREA |
| 1 (1.7) | 19 | c.2237_2255
del18>TT |
p.del746_S752>V | In-frame deletion
complex | delELREATS>V |
| 1 (1.7) | 19 | c.2235_2249
del15 | p.del745_750 | In-frame
deletion | delKELREA |
| 1 (1.7) | 19 | c.2239_2251 del13;
2253_2254insA | p.del747_750 | In-frame deletion
complex | delLREA |
| 1 (1.7) | 19 | c.2239_2248 del10;
2248_2249ins | p.del747_749 | In-frame deletion
complex | delLRE |
| 1 (1.7) | 19 | c.2239_2253
del15 | p.del747_751 | In-frame
deletion | delLREAT |
| 2 (3.4) | 19 | c.2252C>G;
2253_2277 del24 | p.T751S;
del752_759 | In-frame deletion
complex | delSPKANKEI |
| 1 (1.7) | 19 | c.2239_2240
TT>CC | p.Leu747Pro | Missense | L747P |
| 1 (1.7) | 21 | c.2572 C>A | p.Leu858Met | Missense | L858M |
| 1 (1.7) | 21 | c.2582 T>A | p.Leu861Gln | Missense | L861Q |
| 26 (44.1) | 21 | c.2573 T>G | p.Leu858Arg | Missense | L858R |
| Table IIDistribution of epidermal growth
factor receptor mutations according to patient characteristics. |
Table II
Distribution of epidermal growth
factor receptor mutations according to patient characteristics.
| Characteristic | No. of
patients | No. of EGFR
mutated cases (%) |
|---|
| Total analysed | 515 | 59 (11.5) |
| Males/females | 357/158 | 24/35
(6.7/22.2) |
| Age (years) |
| <45 | 17 | 4
(23.5) |
| 45–50 | 37 | 7
(18.9) |
| 51–60 | 98 | 12 (12.2) |
| >60 | 363 | 36 (9.9) |
| Smoking status |
| Smoker | 174 | 6
(3.4) |
| Former smoker | 209 | 15 (7.2) |
| Never smoked | 70 | 37 (52.9) |
| Unknown | 62 | 1
(1.6) |
| Tumour status |
| Primary
tumour | 452 | 51 (11.3) |
| Metastasis |
| Sample type | 63 | 8
(12.7) |
| Biopsy | 429 | 49 (11.4) |
| Surgical | 86 | 10 (11.6) |
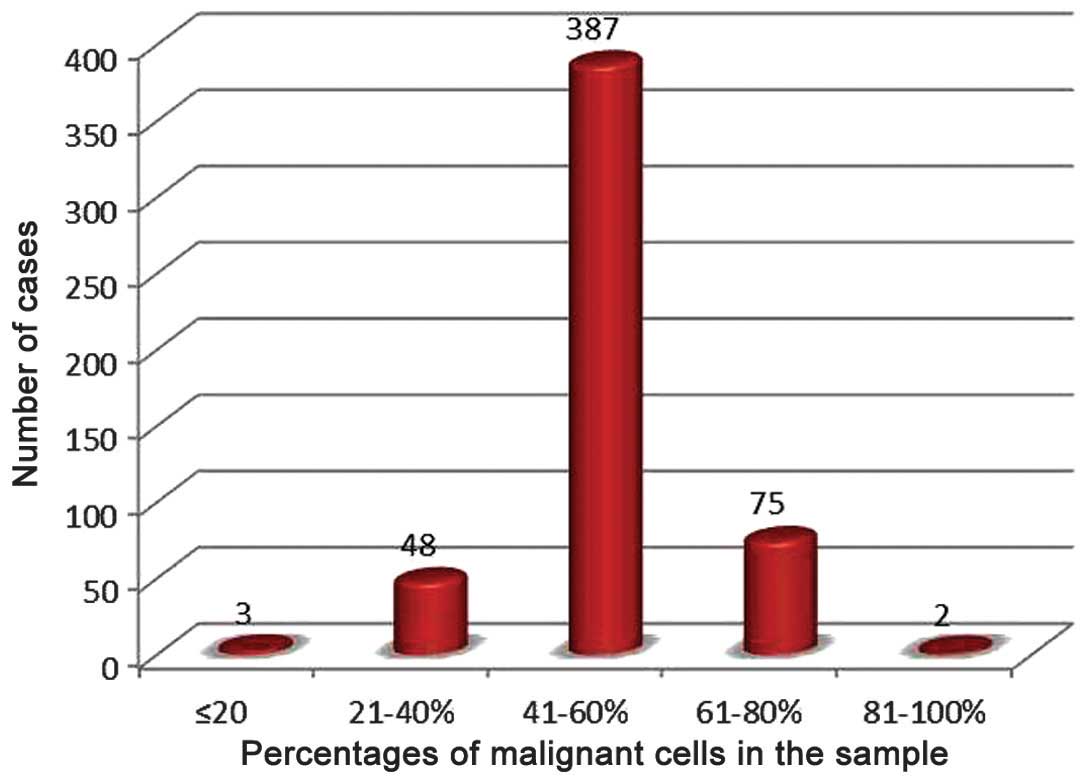
The mean (SD, range) percentage of neoplastic cells
in the samples employed for mutational analysis was 52.5% (9.8,
20–90). The distribution of the percentages of neoplastic cells in
the specimens is shown in Fig. 1.
In >75% of the cases examined, the percentage of malignant cells
in the tissue sample was between 41 and 60%, while in <1% of the
cases the percentage was <20% or >90%. A statistically
significant difference in the number of mutations detected was
found between samples with ≥50% of neoplastic cells (450 cases-57
mutations; 12.7%) and those with <50% of neoplastic cells (65
cases-2 mutations; 3.1%). Furthermore, a statistically significant
difference in the proportion of malignant cells was found between
samples obtained by biopsy and those obtained by surgery. The mean
percentage of neoplastic cells was 50.3% (range 20–90) in biopsy
specimens and 63.1% (range 40–90) in surgical samples. However, no
statistical difference was inferred in EGFR mutation rates
between tissue samples obtained by biopsy (49/429; 11.4%) or
surgery (10/86; 11.6%; Table
II).
Discussion
EGFR mutations were found in 11.5% of
Sardinian patients with lung adenocarcinoma. This percentage is
similar to that reported in the literature for other Caucasian
populations (14). Additionally,
in the present study EGFR mutations were found to be
significantly more frequent in females and patients that had never
smoked than in males and former or active smokers. This finding has
been extensively reported in numerous previous studies from
different geographical areas (15–18).
The proportions of exon 18, 19 and 21 mutations were
similar to those reported in the literature for other Caucasian
populations (15). These mutations
were frequent, other than in females and never-smokers, amongst
patients aged ≤60 years at diagnosis (15.1% compared with 9.9% in
patients aged >60 years at diagnosis). No statistical
differences in the distribution of EGFR mutations were found
in patients aged ≤50 years (14.1%) as compared with those aged ≥50
years (10.5%).
With regards to the origin of the tissue specimen
used for mutational analysis, no statistically significant
differences were identified in the percentages of EGFR
mutations detected between samples obtained from primary tumours
and those obtained from distant metastatic lesions, developed
either through a lymphatic or hematogenous diffusion. In addition,
no significant difference was observed in EGFR mutation
frequencies between tissue samples obtained by biopsy and those
obtained by surgery. The two findings elucidate a practical aspect
for the clinical management of patients with lung cancer, as they
demonstrate a clear indication that EGFR mutational analysis
may be performed in small tissue samples obtained by biopsy methods
on either primary or secondary tumour lesions, thus, avoiding the
invasiveness of surgical approaches.
Several studies have investigated the effectiveness
of mutation analysis performed on biopsies or fine needle
aspiration samples (14,19–21).
These studies, along with technological improvements in laboratory
methods, confirmed the effectiveness of EGFR mutational analysis in
small tumour samples. This finding was also confirmed in the
present study. Malapelle et al (22) in a previous study compared EGFR
mutation analysis in 318 histology samples with that performed on
364 cytology specimens; the authors registered 8.5% and 8.8% of
total EGFR mutations in the histological and cytological samples,
respectively.
To the best of our knowledge, the impact of the
quantity of neoplastic cells on mutation analysis has not been
previously investigated thoroughly, and only empirical and sporadic
data are available. Recommendations of several scientific societies
on the minimum quantity of neoplastic cells required in the
specimen for an adequate mutational analysis are generally based on
such data. The Italian guidelines produced recently by a
collaboration of three different scientific societies
(AIOM-SIAPEC-IAP) recommend that when standard mutational analysis
procedures are used (direct sequencing) the sample should be
composed of at least 50% neoplastic cells (23).
As has been previously mentioned, in the present
data, the majority of the samples examined comprised >50%
neoplastic cells. It was identified that specimens with >50%
neoplastic cells correlated positively with a higher number of
EGFR mutations detected. This finding confirms that what is
important is not whether specimens are taken during biopsy or
surgery or whether they are taken from primary or metastatic
tumours, but the quality of its cell composition. This appears to
be the main aspect, which pathologists should focus on when
evaluating or preparing specimens for mutation analysis.
Additionally, standardised and reproducible methods must be
outlined for a precise evaluation of the percentage of malignant
cells in neoplastic specimens, in order to avoid confusion due to
the different methods and criteria currently in use.
Acknowledgments
The present study was partially supported by the
Italian Ministry of Health ‘Progetto Ricerca Finalizzata’ and the
Sardinian Regional Government ‘Regione Autonoma della
Sardegna’.
References
|
1
|
Ferlay J, Shin HR, Bray F, Forman D,
Mathers C and Parkin DM: GLOBOCAN 2012 v1.2, Cancer Incidence and
Mortality Worldwide: IARC CancerBase No. 10 (Internet).
International Agency for Research on Cancer; Lyon, France: 2012,
http://globocan.iarc.fr.
Accessed February 12, 2013.
|
|
2
|
Alberg AJ, Brock MV, Ford JG, Samet JM and
Spivack SD: Epidemiology of lung cancer: Diagnosis and management
of lung cancer, 3rd ed: American college of chest physicians
evidence-based clinical practice guidelines. Chest. 143(Suppl 5):
e1S–e29S. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Paliogiannis P, Attene F and Cossu A: Lung
cancer epidemiology in North Sardinia, Italy. Multidiscip Respir
Med. 8:452013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Parkin DM, Bray F, Ferlay J and Pisani P:
Global cancer statistics, 2002. CA Cancer J Clin. 55:74–108. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Jemal A, Siegel R, Xu J and Ward E: Cancer
statistics, 2010. CA Cancer J Clin. 60:277–300. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Alberg AJ, Ford JG and Samet JM: American
college of chest physicians. Epidemiology of lung cancer: ACCP
evidence-based clinical practice guidelines (2nd edition). Chest.
132(Suppl 3): 29S–55S. 2007. View Article : Google Scholar
|
|
7
|
Lewis DR, Chen HS, Feurer EJ, et al: SEER
Cancer statistics review, 1975–2008. Bethesda, MD national cancer
institute; 2010, http://seer.cancer.gov/csr/1975_2010/.
Accessed October 20, 2013.
|
|
8
|
Yamamoto H, Toyooka S and Mitsudomi T:
Impact of EGFR mutation analysis in non-small cell lung cancer.
Lung Cancer. 63:315–321. 2009. View Article : Google Scholar
|
|
9
|
Thunnissen E, Kerr KM, Herth FJ, et al:
The challenge of NSCLC diagnosis and predictive analysis on small
samples. Practical approach of a working group. Lung Cancer.
76:1–18. 2012. View Article : Google Scholar
|
|
10
|
Ellison G, Zhu G, Moulis A, Dearden S,
Speake G and McCormack R: EGFR mutation testing in lung cancer: a
review of available methods and their use for analysis of tumour
tissue and cytology samples. J Clin Pathol. 66:79–89. 2013.
View Article : Google Scholar :
|
|
11
|
Tsiatis AC, Norris-Kirby A, Rich RG, Hafez
MJ, Gocke CD, Eshleman JR and Murphy KM: Comparison of Sanger
sequencing, pyrosequencing, and melting curve analysis for the
detection of KRAS mutations: diagnostic and clinical implications.
J Mol Diagn. 12:425–432. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Anderson S, Bloom KJ, Vallera DU, et al:
Multisite analytic performance studies of a real-time polymerase
chain reaction assay for the detection of BRAF V600E mutations in
formalin-fixed paraffin-embedded tissue specimens of malignant
melanoma. Arch Pathol Lab Med. 136:1385–1391. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Palomba G, Colombino M, Contu A, et al:
Prevalence of KRAS, BRAF and PIK3CA somatic mutations in patients
with colorectal carcinoma may vary in the same population: clues
from Sardinia. J Transl Med. 10:1782012. View Article : Google Scholar
|
|
14
|
Nana-Sinkam SP and Powell CA: Molecular
biology of lung cancer: Diagnosis and management of lung cancer,
3rd ed: American college of chest physicians evidence-based
clinical practice guidelines. Chest. 143:e30S–e9S. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Pao W, Miller V, Zakowski M, et al: EGF
receptor gene mutations are common in lung cancers from ‘never
smokers’ and are associated with sensitivity of tumors to gefitinib
and erlotinib. Proc Natl Acad Sci USA. 101:13306–13311. 2004.
View Article : Google Scholar
|
|
16
|
Shigematsu H, Lin L, Takahashi T, et al:
Clinical and biological features associated with epidermal growth
factor receptor gene mutations in lung cancers. J Natl Cancer Inst.
97:339–346. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Fukuoka M, Yano S, Giaccone G, et al:
Multi-institutional randomized phase II trial of gefitinib for
previously treated patients with advanced non-small-cell lung
cancer (The IDEAL 1 Trial) [corrected]. J Clin Oncol. 21:2237–2246.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Miller VA, Kris MG, Shah N, et al:
Bronchioloalveolar pathologic subtype and smoking history predict
sensitivity to gefitinib in advanced non-small-cell lung cancer. J
Clin Oncol. 22:1103–1109. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Hantson I, Dooms C, Verbeken E, et al:
Performance of standard procedures in detection of EGFR mutations
in daily practice in advanced NSCLC patients selected according to
the ESMO guideline: a large Caucasian cohort study. Transl Respir
Med. 2:92014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Vigliar E, Malapelle U, Bellevicine C, et
al: Outsourcing cytological samples to a referral laboratory for
EGFR testing in non-small cell lung cancer: does theory meet
practice? Cytopathology. Nov 7–2014.Epub ahead of print. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Lozano MD, Labiano T, Echeveste J, et al:
Assessment of EGFR and KRAS mutation status from FNAs and
core-needle biopsies of nonsmall cell lung cancer. Cancer
Cytopathol. Dec 19–2014.Epub ahead of print. View Article : Google Scholar
|
|
22
|
Malapelle U, Bellevicine C, De Luca C, et
al: EGFR mutations detected on cytology samples by a centralized
laboratory reliably predict response to gefitinib in non-small cell
lung carcinoma patients. Cancer Cytopathol. 121:552–560. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Marchetti A, Normanno N; AIOM-SIAPEC-IAP;
et al: Recommendations for mutational analysis of EGFR in lung
carcinoma. Pathologica. 102:119–126. 2010.In English, Italian.
PubMed/NCBI
|