Introduction
Skeletal injury is one of the most prevalent
problems observed clinically, which impairs the daily activities of
the patients (1). Bone repair is
regulated by a highly coordinated series of molecular, cellular and
tissue events; and the recruitment, proliferation and accumulation
of stem cells at the site of injury are the essential aspects of
the repair process (2). Immature
stem cells differentiate into dynamic osteoblasts in order to
restore bone tissues (3). Bone
injury healing also critically depends on the growth of blood
vessels, not only for nutrient supply, but also for the influx of
osteoblasts (4,5). Previous evidence has indicated that
physiological bone remodeling occurs in close proximity to blood
vessels, and these vessels carry perivascular stem cells, which
then differentiate into osteoblasts (5).
The marrow stroma is a complex tissue, which
contains cells that are required for the lineage commitment of
hematopoietic and non-hematopoietic cells and can differentiate
into various types of mesenchymal and non-mesenchymal cell
(6). Bone marrow mononuclear cells
(BMMCs) include several types of marrow stem cells, including
hematopoietic stem cells, mesenchymal stem cells, endothelial
progenitor cells and other precursor stem cells (7). Following trauma, these cells secrete
cell growth factors, which promote tissue differentiation of the
transplanted BMMCs, leading to repair of the injured organs and
restoration of organ function (8–10).
In preclinical and clinical trials, bone marrow-derived stem cells
have been successfully applied for bone and cartilage regeneration
following osteoporotic fracture and arthritis (11,12).
Although studies have suggested that homing of
native stem cells to injured tissue and their subsequent
involvement in the regenerative process is a natural healing
response (13–15), the mechanism underlying the
function of these stem cells in bone repair remains to be
elucidated. In the present study, a rat model of midpalatal
incision and expansion was constructed and used to investigate the
mechanism underlying the movement of transplanted BMMCs into the
circulation and how they become stationed at the injury site for
bone repair. The results may provide further understanding of bone
injury healing by stem cells.
Materials and methods
Animals and grouping
A total of 15 male, 8-week-old Sprague-Dawley rats
(Vital River Laboratory Animal Technology Co., Ltd., Beijing,
China), with a mean weight of 208.36±7.32 g, were used in the
present study. The rats were housed in an International Standards
Organization (ISO) class 7 room with 50% relative humidity. The
rats underwent a reversed 12:12 h light/dark cycle and were
maintained at 22–25°C in an atmosphere containing 5%
CO2. They were given 5 g feedstuff and 11 ml per 100 g
body weight of water daily. All groups of animals were housed
together with a different marker. All rats were treated according
to the ethical regulations defined by the Ethics Committee of
Capital Medical University (Beijing, China).
The rats were divided into five groups, with three
rats in each group, as follows: Control group (Inc), in which the
midpalatal suture was sectioned without expansion or BMMC
transplantation; expansion group (Exp), in which the rats underwent
midpalatal expansion for 2 weeks with incision, but no BMMC
transplantation; expansion and transplantation group (EaT), in
which the rats underwent midpalatal expansion for 2 weeks with
incision and BMMC transplantation; expansion and relapse group
(ExR), in which the rats underwent midpalatal expansion for 2 weeks
with incision, but no BMMC transplantation, followed by removal of
the expansion appliance (0.45 mm stainless steel AJ Wilcock
Australian Wire; AJ Wilcock PTY., Ltd., Whittlesea, Australia) and
observation of palatal changes during relapse;
expansion/transplantation/relapse group (EtR), in which the rats
underwent midpalatal expansion for 2 weeks with incision and BMMC
transplantation, prior to removal of the expansion appliance and
sacrifice of the rats 2 weeks later in order to observe palatal
changes during relapse. The rats were sacrificed by cervical
dislocation. None of the groups of rats experienced a significant
loss of body weight during the fed period. At the beginning of
rapid suture expansion, food intake was disturbed, however, the
body weight of the rats recovered afterwards. Samples of midpalatal
tissues were obtained from these rats in each group, which were
used for further histological and immunohistochemical analyses.
Expansion of the midpalatal suture
The rats were subjected to midpalatal expansion, as
described in a previous study (16). The distal ends of the expansion
appliances were placed into the inter-proximate space between the
second and third molars, and the appliances were activated through
the ends of the compression helices to exert an initial expansion
force of 150 g. A 1.5 cm anteroposterior mid-sagittal incision was
made following appliance placement. The expansion appliances were
activated once every other day (150 g each time) in order to obtain
the effects of midpalatal expansion. The duration of midpalatal
expansion was two weeks.
BMMC culture and transplantation
Bone marrow aspirate is considered to be the most
accessible and enriched source of mesenchymal stem cells due to the
efficient isolation of multi-potential cells from this tissue
(17). Mouse BMMCs were harvested
and cultured using a previously described method with modifications
(18). Briefly, a 2-month-old male
BALB/C mouse (Vital River Laboratory Animal Technology Co., Ltd.)
was chosen as the donor of BMMCs. The mouse was housed in an ISO
class 7 room with 50% relative humidity. The mouse underwent a
reversed 12:12 h light/dark cycle and was maintained at 22–25°C in
an atmosphere containing 5% CO2, and was given 4 g
feedstuff and 5 ml per 100 g body weight of water daily. BMMCs were
obtained by flushing the femur of the mouse with Dulbecco's
modified Eagle's medium (DMEM)/F12 (Invitrogen; Thermo Fisher
Scientific, Inc., Waltham, MA, USA), and centrifuged at 400 × g for
10 min to remove adipose tissue. The cell pellet was suspended in 5
ml chilled Hanks' balanced salt solution and layered over 8 ml
Percoll solution (1.073 g/ml) (both GE Healthcare Life Sciences,
Chalfont, UK). Following centrifugation at 800 × g for 30 min, the
mononuclear cell layer was removed from the interface, suspended in
DMEM/F12 supplemented with 20% fetal bovine serum, 50 mg/ml
ascorbic acid, and 100 mg/ml penicillin-streptomycin (Gibco; Thermo
Fisher Scientific, Inc.), and incubated at 37°C in a humidified
atmosphere containing 5% CO2. The cells reached 80%
confluence in 8–10 days, and were then suspended using
trypsin-ethylenediaminetetraacetic acid, prior to passage for
expansion. The cells from passage four were numerous and of
suitable shape, and were used for subsequent cell
transplantation.
To identify and track BMMCs following midpalatal
transplantation, the cells were labeled with bromodeoxyuridine
(BrdU; Sigma-Aldrich, St. Louis, MO, USA). The expanded and labeled
BMMCs (1×106 cells/ml; 0.5 ml) suspended in sterile
medium were intra-orally injected into the left masseter area
opposite the first molar in the EaT and EtR groups 2 days following
the second activation, and the expansion appliances were maintained
in place for two weeks. Physiological saline solution (5 mg/kg;
0.9% sodium chloride) was injected, in the same manner, in the rats
of the Exp and ExR groups.
Observation of histological changes in
morphology
Once the rats had been sacrificed, the mandible and
facial skin were removed. The maxillary tissue was fixed in 10%
formalin solution [New England Biolabs (Beijing) Ltd., Beijing,
China] for 48 h, and was then demineralized in 10% EDTA (pH 7.2;
Sinopharm Chemical Reagent Co., Ltd., Beijing, China) for 6–8 weeks
until the bone tissue had softened. Subsequently, samples of the
midpalatal bone between the first and third molars of the rats were
isolated and embedded with paraffin [New England Biolabs (Beijing)
Ltd.]. Sections (5 µm) were mounted on poly-L-lysine-coated
glass slides [New England Biolabs (Beijing) Ltd.]. Prior to
staining, the sections were incubated at 60°C for 1 h, treated with
xylene [New England Biolabs (Beijing) Ltd.], and rehydrated through
a series of ethanol solutions. Hematoxylin and eosin [H&E; New
England Biolabs (Beijing) Ltd.] staining was performed to observe
histological changes in morphology of the midpalatal bone and the
surrounding tissues under an optical microscope (Olympus CX22;
Olympus Corporation, Tokyo, Japan).
Tracking and evaluation of the
differential potential of transplanted BMMCs in the masseter and
midpalatal bone
The transplanted BMMCs labeled with BrdU were
identified and tracked using immunofluorescence staining with mouse
monoclonal anti-BrdU primary antibody (1:100; cat. no. B8434;
Sigma-Aldrich). The paraffin sections were treated with xylene and
a series of ethanol solutions. Subsequently, antigen retrieval was
conducted using 0.1% trypsin at 37°C for 5 min, and the sections
were incubated with 3% H2O2 for 15 min. The
sections were then incubated with the antibody in a humid chamber
at 4°C for 24 h, prior to incubation with fluorescein isothionate
(FITC) or tetramethyl-rhodamine-isothiocyanate (TRITC)-conjugated
rabbit anti-mouse IgG secondary antibodies (1:100; cat. no.
YB-22908 and YB33709ES60, respectively; Shanghai Yubo Biotech Co.,
Ltd., Shanghai, China) at 37°C for 1 h. The cell nuclei were
visualized in the masseter and palatal tissues samples using
4′,6-diamidino-2-phenylindole (DAPI; Molecular Probes, Thermo
Fisher Scientific, Inc.). Fluorescence imaging was captured using a
laser scanning confocal microscope (LSM710; Carl Zeiss AG,
Oberkochen, Germany) or fluorescence microscope (Olympus BX61;
Olympus Corporation) with an excitation wavelengths of 490 nm for
FITC and 550 nm for TRITC. If the fluorescent signal areas (green)
were consistent with the cell nuclei (blue) in the tissue samples
stained with DAPI, the cells were determined to be BrdU-positive
BMMCs.
M-cadherin is a member of the
Ca2+-dependent cell-cell adhesion molecule family, and
its expression is confined to muscle satellite cells (19). Elivision™ Plus kit (cat. no.
KIT-9901) and Ultrasensitive™ S-P kit (cat. no. KIT-9709) (Fuzhou
Maixin Biotechnology Co., Ltd., Fuzhou, China) were used to detect
the expression of BrdU and M-cadherin (polyclonal rabbit anti-rat
antibody; 1:100; cat. no. sc-10734; Santa Cruz Biotechnology, Inc.,
Dallas, TX, USA) in the masseter, in order to examine the
distribution and myogenic orientation of the transplanted BMMCs.
The blue/black BrdU-positive sections were visualized with
5-bromo-4-chloro-3-indolyl-phosphate (BCIP)/nitro-blue-tetrazolium,
whereas the red/brown M-cadherin-positive sections were visualized
with 3-amino-9-ethylcarbozole (AEC). The sections were
counter-stained with hematoxylin prior to being mounted.
The expression of osteocalcin by osteoblasts
indicates the commencement of active bone formation (20). Double immunohistochemical staining
for osteocalcin (polyclonal rabbit anti-rat antibody; 1:100; cat.
no. BA0121-2; Wuhan Boster Biological Technology, Ltd., Wuhan,
China) and BrdU were performed to investigate the osteogenic
differentiation of the transplanted BMMCs in the palatal bone. The
blue/black BrdU-positive sections were visualized with
BCIP/nitro-blue-tetrazolium, whereas the red/brown
osteocalcin-positive sections were visualized with AEC.
Results
Changes of morphology following
midpalatal expansion and BMMC transplantation in rats
H&E staining was performed to observe the
morphological changes of the midpalatal bone in the groups of rats.
A palatal shelf structure with an incision in the middle of the
suture is shown in Fig. 1A. The
midpalatal suture was centrally located, and the hyaline cartilage
was separated. The chondrocytes on either side of the suture
gradually matured and migrated laterally towards the
bone-marrow-like cavities and the compact bone of the maxilla. The
bony plates were enveloped by two layers of soft tissue, mucosa at
the nasal and oral sides. In the submucosa tissue on the oral side,
the palatine vessels and nerves formed large bundles, which were
located in bilateral concavities in the bone. A single layer of
osteoblasts lined the oral and nasal surface of the bone. There
were a small number of endogenous spindle cells migrating from the
submucosa tissue into the midpalatal suture.
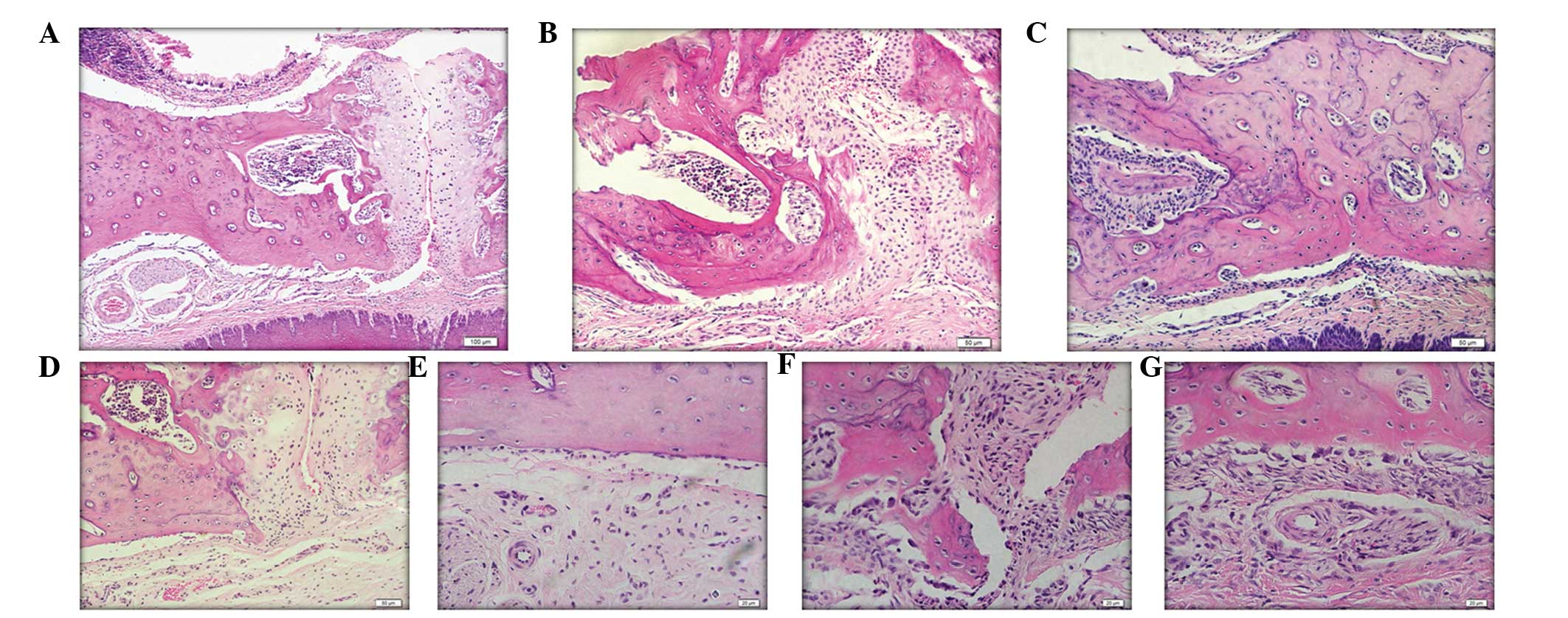 | Figure 1Microphotographs of the midpalatal
bone and surrounding tissues following midpalatal expansion with or
without BMMC transplantation in Sprague-Dawley rats. All images are
oriented nasal side up and oral side down. (A) A central incision
shown in the suture of the midpalatal bone in the Inc group. Arrows
indicate bone-marrow-like cavity. Scale bar=100 µm. (B)
Central incision after 4 weeks, compared with the ExR group. Arrows
indicate two layers of soft tissue and the mucosa at the nasal
side. Scale bar=50 µm. (C) BMMC transplantation accelerated
midpalatal bone formation, exhibiting calcified compact bone in the
EtR group. At 2 weeks following expansion in the Exp groups, the
mesenchymal stem-like cells migrated from the soft tissue into the
central area of the suture. Arrows indicate the mucosa at the oral
side scale bar=50 µm. In the (D) Exp group, the pattern of
the chondrocyte array is evident. Arrows indicate a single layer of
osteoblasts lining the oral and nasal surface of the bone. Scale
bar=50 µm. (E) A number of osteoblasts were present at the
boundary of the midpalatal bone, and collagenic fibers were
observed surrounding the neurovascular bundle in the Exp group.
Arrows indicate a small number of endogenous spindle cells
migrating from the submucosal tissue to the midpalatal suture.
Scale bar=20 µm. (F) In the EaT group, the majority of the
chondrocytes had disappeared and were replaced by fibrous-like
tissues, which contained numerous mesenchymal cells migrating from
the submucosal tissue. Scale bar=20 µm. (G) Submucosal layer
was thicker and a large number of mesenchymal cells entered the
surrounding compact palatal bone, transforming it into trabecular
bone. Scale bar=20 µm. BMMC, bone marrow mononuclear cells;
Inc group, control group; Exp, expansion group; EaT, expansion and
transplantation group; ExR, expansion and relapse group; EtR,
expansion/transplantation/relapse group. |
Following 2 weeks of expansion and relapse in the
ExR group (Fig. 1B), the
midpalatal suture was almost bridged by a large number of
mononuclear cells. The chondrocytes remained evident and were
involved in endochondral-type bone formation. By contrast, 4 weeks
following BMMC transplantation in the EtR group (Fig. 1C), the suture and surrounding
tissues had already constituted newly formed bone, with a calcified
compact structure and several small vessels. In the Exp group, 2
weeks following expansion (Fig.
1D), endogenous spindle mesenchymal cells had migrated along
the disconnected surface at the midline of the midpalatal suture.
The chondrocytes were located laterally as mesenchymal cells,
migrating into the incision ends and bridging one third of the
incision. Following mechanical stimulation, the trabecular bone
lining cells developed ultrastructural features of differentiated
osteoblasts, and exhibited a cuboidal shape and rounded nuclei
(Fig. 1E). By contrast, the
majority of the chondrocytes in the EaT group disappeared and were
replaced by fibrous-like tissues, which contained numerous
mesenchymal cells migrating from the submucosal tissue (Fig. 1F). The submucosal layer became
thicker, and numerous mesenchymal cells entered the surrounding
compact palatal bone, which was transformed into trabecular bone
(Fig. 1G).
Tracking and observation of the
expression of M-cadherin of transplanted BMMCs in the masseter
During the 4 week experimental period, the BMMCs
injected into the masseter were observed at several anatomical
locations, traced by BrdU-positive staining. A number of positive
spindle cells were located on the collagen fibers surrounding the
blood vessels between the muscle fibers in the EaT group (Fig. 2A and B). During the experiment, a
number of transplanted BMMCs penetrated into the blood vessels and
exhibited rounded morphology in the EtR group (Fig. 2C). Co-expression of BrdU and
M-cadherin was observed, which appeared in the sublaminar position,
usually occupied by satellite cells (Fig. 2D, EaT group; Fig. 2E, EtR group). However, no
BrdU-positive cells were observed in the Exp group (Fig. 2F). The observations demonstrated
that the connective tissue fibers provided anchors for the
transplanted BMMCs to migrate between muscle fibers. These
observations suggested that the transplanted BMMCs injected into
the masseter were able to migrate into the blood circulation and
possessed systemic characteristics.
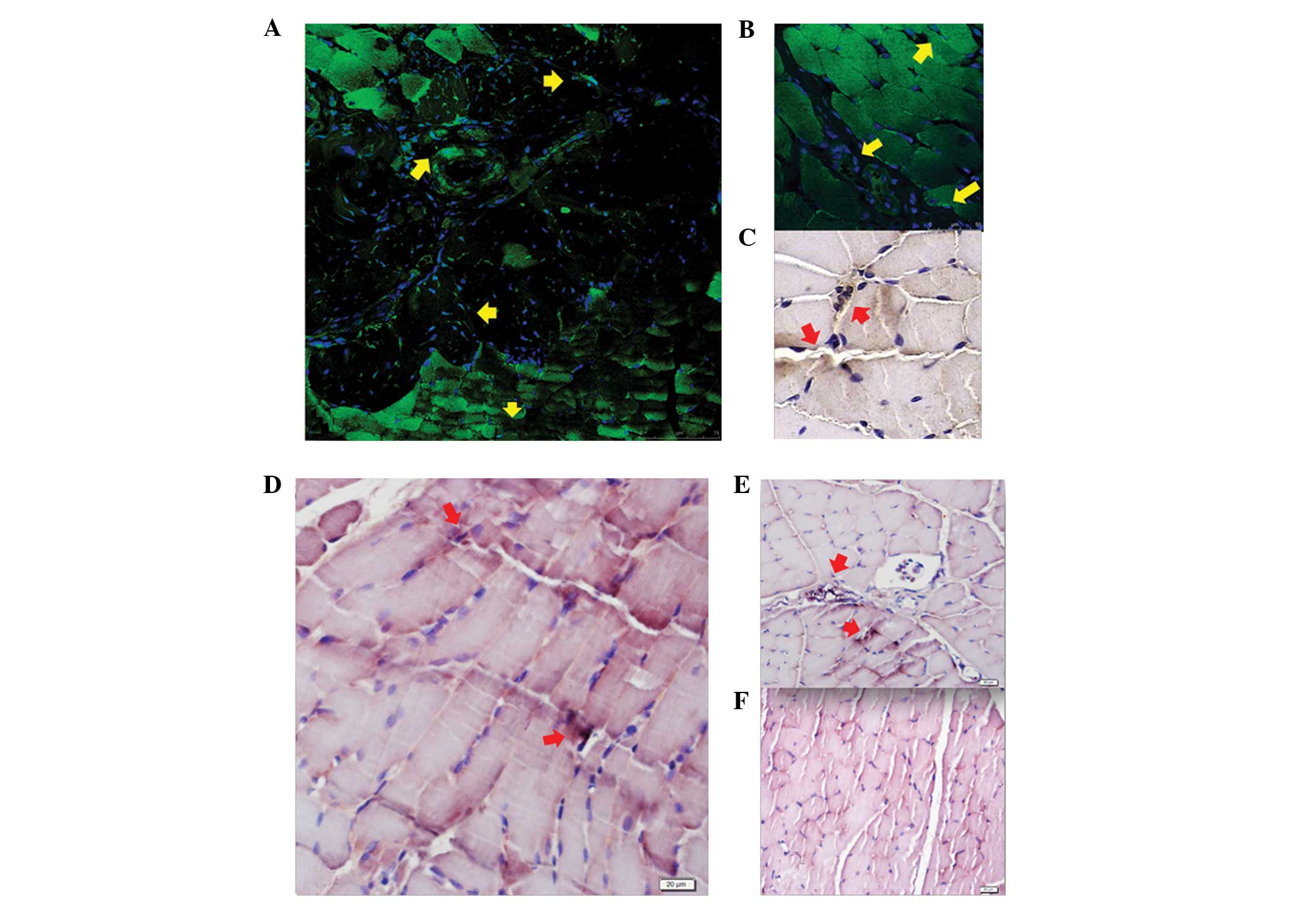 | Figure 2Microphotographs of
immunohistochemical staining for BrdU-positive cells in the
masseter area in Sprague-Dawley rats following expansion, with or
without BMMC transplantation. (A and B) In the EaT group, the
transplanted BMMCs predominantly appeared as spindle cells located
in the peri-vessel sites and on the walls of the vessels. Arrows
indicate BrdU-positive areas. Scale bar=75 and 50 µm,
respectively. (C) In the EtR group, the cells were also seen
penetrating into the vessels and exhibited a rounded morphology.
Arrows indicate blue/black BrdU-positive staining. Scale bar=50
µm. In the (D) EaT and (E) EtR groups, co-expression of BrdU
and M-cadherin BMMCs was observed in the sub-laminar position,
usually occupied by satellite cells. Arrows indicate blue/black
BrdU-positive staining and red M-cadherin-positive staining. Scale
bar=20 µm. (F) No BrdU-positive cells were observed in the
Exp group. Scale bar=20 µm. BMMC, bone marrow mononuclear
cells; BrdU, bromodeoxyuridine; Inc group, control group; Exp,
expansion group; EaT, expansion and transplantation group; ExR,
expansion and relapse group; EtR, expansion/transplantation/relapse
group. |
Tracking BMMCs in the midpalatal
bone
Heterologous BMMC transplantation via masseter
injection resulted in a large quantity of spindle cells migrating
into the midpalatal bone injured by incision and expansion
(Fig. 3). These cells included,
not only transplanted BMMCs, but also endogenous mesenchymal-like
cells. In the EaT group, BrdU-positive cells were located in the
fibrous-like tissue at the midline of the suture (Fig. 3A), whereas they resided in the
blood vessel walls (Fig. 3B) in
the EtR group. In addition, mesenchymal-like cells in the ExR group
were involved in midpalatal bone remodeling (Fig. 3C). The junction between the soft
and hard tissue manifested the importance of the differentiation of
mesenchymal-like cells into osteoblasts. In the EaT group,
BrdU-positive cells were also located in the bone-marrow-like
tissues (Fig. 3D). The results
clearly showed that the transplanted BMMCs, which appeared in the
oral mucosa, enveloped the midpalatal bone in the EaT group
(Fig. 3E), and these
differentiated into osteoblasts at the boundary of the
neuromuscular bundle and in the newly forming bone during
midpalatal bone regeneration (Fig.
3F).
 | Figure 3Immunofluorescent staining for BrdU
in the midpalatal suture area in Sprague-Dawley rats following
expansion with or without BMMC transplantation. (A) In the EaT
group, as indicated by the arrows, the transplanted BMMCs were
present in the suture area. Scale bar=50 µm. (B) In the EtR
group, the transplanted BMMCs appeared on the vessel walls in the
midpalatal bone, as indicated by the arrows. Scale bar=25
µm. (C) Mesenchymal-like cells were also present in the ExR
group, and were involved in midpalatal bone remolding. Scale bar=50
µm. (D) In the EaT group, as indicated by the arrows, the
transplanted BMMCs were present in the bone marrow-like tissues.
Scale bar=20 µm. (E) Connective tissues surrounding the
midpalatal bone provided a micro-platform for the stem cells in the
EaT group. Scale bar=20 µm. (F) In the EtR group, as
indicated by the arrows, the transplanted BMMCs indicated by the
blue-black BrdU-positive areas were differentiated into the
pericytes of the neuromuscular bundles, and subsequently into
osteoblasts, finally migrating into the midpalatal bone. Scale
bar=50 µm. BrdU, bromodeoxyuridine;BMMC, bone marrow
mononuclear cells; EaT, expansion and transplantation group; ExR,
expansion and relapse group; EtR, expansion/transplantation/relapse
group. |
Expression of osteocalcin in BMMCs
transplanted through the masseter into the midpalatal bone
During midpalatal expansion in the BMMC
transplantation (EaT) group, fibrous-like tissue channels formed
from the submucosal tissues at the nasal side in the midpalatal
bone. These channels contained a small number of clones of
transplanted BMMCs, which appeared as blue/black BrdU-positive
sections, and also contained a large number of spindle cells that
originated from the host soft tissues. Several spindle cells
expressing osteocalcin were indicated by a red/brown signal in
these progenitor migrating channels (Fig. 4A). Similar transplanted cells were
observed in the submucosal tissue at the oral sides, which
exhibited a darkened color indicating expression of osteocalcin,
and a small number of transplanted BMMCs were located in the vessel
walls in the EaT group (Fig. 4B,
arrows). After 4 weeks, a few transplanted BMMCs were located in
the midpalatal bone in the EtR group, which exhibited a light
red/brown color, indicating lower expression levels of osteocalcin
(Fig. 4C). In this group, a small
number of BMMCs continued to co-express BrdU and osteocalcin, and
were present at the junction of the mucosa and the midpalatal bone,
as well as the vessels in the midpalatal bone (Fig. 4D). Although mesenchyma-like cells,
migrating from the submucosa at the nasal side, were also observed,
no cell channels were observed in the Exp group (Fig. 4E). Chondroblasts were located along
the mesial incision of the midpalatal bone, and a row of cubic
oseoblasts were arrayed orderly at the boundary between the
neuromuscular bundle and midpalatal bone in the Exp group (Fig. 4F). A similar observation was
observed in the BMMC transplantation group.
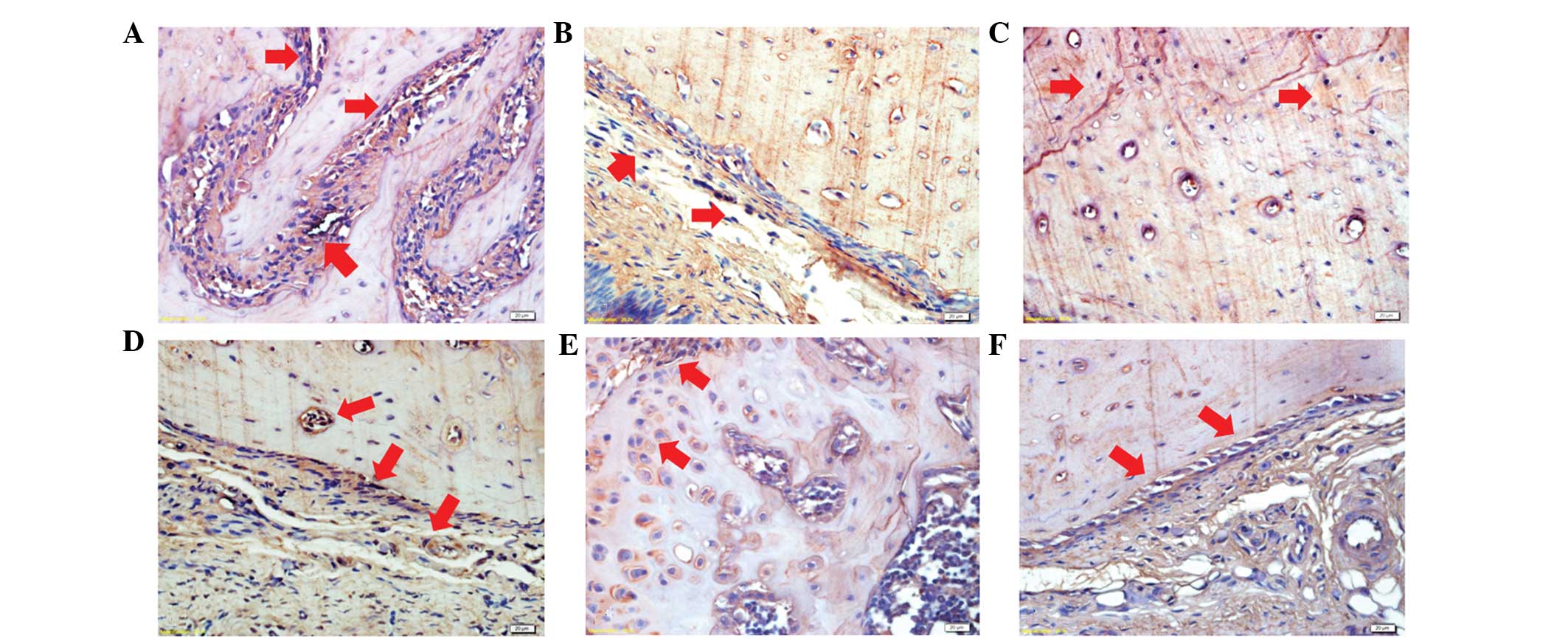 | Figure 4Co-expression of BrdU and osteocalcin
in transplanted BMMC in the midpalatal bone and surrounding tissues
in Sprague-Dawley rats following midpalatal expansion. (A)
Transplanted BMMCs expressing osteocalcin are indicated by
blue/black and red/brown color in the progenitor migrating channel,
inn the submucosal tissue at the oral side, and on the (B) blood
vessel walls (arrows) in the EaT group. (C) A small number of
BrdU-positive BMMCs were located in the midpalatal bone in the EtR
group, exhibiting a red-brown color. (D) Transplanted BMMCs
expressing osteocalcin were observed at the junction of the mucosa
and the midpalatal bone, demonstrating their transition from
mesenchymal stem-like cells to osteoblasts. The blood vessel walls
also contained BrdU and osteocalcin co-expressing transplanted
BMMCs in the EtR group. (E) In the Exp group, no cell channels were
observed, however, (F) a row of cubic oseoblasts arrayed orderly at
the boundary were observed between the neuromuscular bundle and the
midpalatal bone. Scale bar=20 µm. BrdU, bromodeoxy-uridine;
BMMC, bone marrow mononuclear cells; Exp, expansion group; EaT,
expansion and transplantation group; ExR, expansion and relapse
group; EtR, expansion/transplantation/relapse group. |
Discussion
Healing from injury requires the activation and
proliferation of stem cells for tissue repair (21). In the present study, a rat model
exhibiting midpalatal incision and expansion was used to observe
the trajectory of BMMCs following BMMC transplantation via masseter
injection. The BMMCs injected into the masseter were observed, not
only in the masseter, but also in the blood vessels and oral
mucosa, and enveloped the midpalatal bone. A number of the BMMCs
differentiated into osteoblasts at the boundary of the
neuromuscular bundle, and were located in the newly formed bone
during midpalatal bone regeneration.
Rapid midpalatal expansion is a common treatment
solution for patients with a narrow maxillary dental arch (22). The results of previous studies have
revealed the mechanism of midpalatal bone remodeling induced by
mechanical expansion. Hall et al (23) reported that the re-establishment of
a suture with the palatine bone margins was covered by newly formed
cartilage in the oral side of a mice model. It has also been
suggested that mesenchymal cells located on the inner side of the
cartilaginous tissue proliferate and differentiate into osteoblasts
when the suture is expanded (20,24).
The midpalatal expansion model used in the present study differed
from the above-mentioned studies, as a surgical incision was made
in the suture to simulate the repair mechanism of distraction
osteogenesis.
Several studies have demonstrated that stem cell
transplantation has a marked effect on promoting callus formation
and in shortening the consolidation period (25,26).
The results of the present study demonstrated that, in the
expansion groups, a natural healing process occurred, in which
mesenchymal progenitors in the surrounding soft tissues migrated
into the injured midpalatal bone and repaired the damaged bone by
differentiating into chondroblasts and osteoblasts. BMMC
transplantation accelerated midpalatal bone formation by increasing
the number of mesenchymal stem cells, which differentiated into
osteoblasts directly. Previous studies have suggested that
transplanted BMMCs induce bone regeneration by enhancing the
migration of host stem cells into injury sites in an endocrine
manner (5,27,28).
These regenerative cells migrate from the surrounding soft tissues
and replace the endochondral bone formation with intramembranous
bone formation, possibly due blood supply being increased (29), resulting in a microenvironment that
favored stem cell differentiation into osteoblasts, rather than
chondroblasts, due to the augmentation in oxygen content (30,31).
These observations indicate the critical effect of
microenvironmental cues on cell fate. However, tissues with
non-specific stem cells may become more tissue-specific under the
effect of environmental factors (32). Multipotent stem cells exist in all
tissues and have the ability to migrate among tissues in response
to certain chemical signals. The mobilization patterns of stem
cells may follow the laws of 'near to distant' and 'concentrated to
diluted' in relation to various chemokines.
The regeneration consequence is a result of the
combination of donor and endogenous stem cell migration to the
injured midpalatal bone, either through osteogenic differentiation
directly or through the production of cytokines (33,34).
In the present study, BMMC transplantation via masseter injection
presents a potential dynamic process to repair injured midpalatal
bone. A number of the transplanted BMMCs appeared to be located in
the sub-laminar position, usually occupied by satellite cells. In
addition, certain transplanted BMMCs anchored and migrated along
the collagenic fibers over large distances. These results are
concordant with those of Laird et al (35) who demonstrated that the
interstitial migration or active amoeboid movement of stem cells
are induced by extravascular cues, and this migration occurs
independently of blood flow. Frimberger et al (36) reported rapid motility of
hematopoietic stem cells, directed migration to stromal cells and
marked membrane modulation. In the present study, a number of the
transplanted BMMCs transformed into vessel pericytes and had the
ability to enter into the circulation, acquiring systemic
characteristics. Following maxilla incision and stimulation by
mechanical expansion, the stem cells were mobilized and migrated to
the enveloped soft tissue of the midpalatal bone. The capillary
wall and the membrane surrounding the vascular bundles served as
delivery sites for the donor cells and other sources of host stem
cells to reconstruct the midpalatal bone. These results suggested
that BMMCs mobilized other host stem cells, which contributed to
the replenishment of osteoblasts for regeneration of the injured
bone.
Further investigation into the mechanisms underlying
the migration of stem cells from surrounding tissues or the
circulation during injury healing and diseases are required to
develop alternative novel therapies. In inflamed regions,
mesenchymal stem cells rapidly exit the blood by integrating into
the endothelium and migrating through the endothelial barrier,
prior to penetrating the basement membrane and invading the
surrounding tissue (37). Tumor
formation has been suggested to be the result of continuously
healing wound (38). Experimental
and clinical studies have revealed that bone marrow-derived
progenitor cells can migrate into the circulation, incorporate into
tumor microenvironments and contribute to the growth of various
tumors (33,39). Chemotactic cytokines released by
the damaged tissues mobilize progenitor cells by establishing
mechanisms from the bone marrow, which may also regulate the
mobilization of tissue-specific stem cells via other signaling
pathways (40). Undifferentiated
tumor cells may enter the circulation and result in distant solid
tumor formation when the balance of a stem cell niche in various
tissues is disrupted. This suggests that malignant tumor formation
may be a type of systemic disease, which exhausts all the stem
cells that maintain the physiological activities and restorative
capacity of organisms. Therefore, it may prove useful to use
chemical cytokines, which mobilize repair cells throughout the
whole body, as targets for treating malignant tumors (41,42).
In conclusion, the results of the present study
demonstrated that BMMCs were able to enter the circulation, migrate
from the muscle to bone tissue and were subsequently involved in
tissue injury healing. These stem cells may be useful in the
treatment of several types of cancer due to stem cell mobilization
in the whole body.
Acknowledgments
The present study was funded by the National Natural
Science Foundation of China (grant no. 81070804), the Shandong
Province Science and Technique Foundation of China (grant no.
2014GSF118093) and Hubei-MOST KLOS & KLOBME (grant no. 201101).
The authors would like to thank Professor Xiaofei Tang for her
advice on the interpretation of the histochemical experimental
results.
References
|
1
|
Levi B, James AW, Nelson ER, Peng M, Wan
DC, Commons GW, Lee M, Wu B and Longaker MT: Acute skeletal injury
is necessary for human adipose-derived stromal cell-mediated
calvarial regeneration. Plast Reconstr Surg. 127:1118–1129. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ren G, Chen X, Dong F, Li W, Ren X, Zhang
Y and Shi Y: Concise review: Mesenchymal stem cells and
translational medicine: Emerging issues. Stem Cells Transl Med.
1:51–58. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Claes L, Recknagel S and Ignatius A:
Fracture healing under healthy and inflammatory conditions. Nat Rev
Rheumatol. 8:133–143. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Doherty MJ, Ashton BA, Walsh S, Beresford
JN, Grant ME and Canfield AE: Vascular pericytes express osteogenic
potential in vitro and in vivo. J Bone Miner Res. 13:828–838. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Khosla S, Westendorf JJ and Mödder UI:
Concise review: Insights from normal bone remodeling and stem
cell-based therapies for bone repair. Stem Cells. 28:2124–2128.
2010. View
Article : Google Scholar : PubMed/NCBI
|
|
6
|
Phinney DG, Kopen G, Isaacson RL and
Prockop DJ: Plastic adherent stromal cells from the bone marrow of
commonly used strains of inbred mice: Variations in yield, growth,
and differentiation. J Cell Biochem. 72:570–585. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Stamm C, Westphal B, Kleine HD, Petzsch M,
Kittner C, Klinge H, Schümichen C, Nienaber CA, Freund M and
Steinhoff G: Autologous bone-marrow stem-cell transplantation for
myocardial regeneration. Lancet. 361:45–46. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Yamada M, Kubo H, Kobayashi S, Ishizawa K,
Numasaki M, Ueda S, Suzuki T and Sasaki H: Bone marrow-derived
progenitor cells are important for lung repair after
lipopolysac-charide-induced lung injury. J Immunol. 172:1266–1272.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Parr AM, Tator CH and Keating A: Bone
marrow-derived mesenchymal stromal cells for the repair of central
nervous system injury. Bone Marrow Transplant. 40:609–619. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Strauer BE, Brehm M, Zeus T, Köstering M,
Hernandez A, Sorg RV, Kögler G and Wernet P: Repair of infarcted
myocardium by autologous intracoronary mononuclear bone marrow cell
transplantation in humans. Circulation. 106:1913–1918. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Fodor WL: Tissue engineering and cell
based therapies, from the bench to the clinic: The potential to
replace, repair and regenerate. Reprod Biol Endocrinol. 1:1022003.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Chanda D, Kumar S and Ponnazhagan S:
Therapeutic potential of adult bone marrow-derived mesenchymal stem
cells in diseases of the skeleton. J Cell Biochem. 111:249–257.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Fong EL, Chan CK and Goodman SB: Stem cell
homing in musculoskeletal injury. Biomaterials. 32:395–409. 2011.
View Article : Google Scholar
|
|
14
|
Sundelacruz S and Kaplan DL: Stem cell-
and scaffold-based tissue engineering approaches to osteochondral
regenerative medicine. Semin Cell Dev Biol. 20:646–655. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Hatch HM, Zheng D, Jorgensen ML and
Petersen BE: SDF-1alpha/CXCR4: A mechanism for hepatic oval cell
activation and bone marrow stem cell recruitment to the injured
liver of rats. Cloning Stem Cells. 4:339–351. 2002. View Article : Google Scholar
|
|
16
|
Lee K, Sugiyama H, Imoto S and Tanne K:
Effects of bisphosphonate on the remodeling of rat sagittal suture
after rapid expansion. Angle Orthod. 71:265–273. 2001.PubMed/NCBI
|
|
17
|
Tuli R, Seghatoleslami MR, Tuli S, Wang
ML, Hozack WJ, Manner PA, Danielson KG and Tuan RS: A simple,
high-yield method for obtaining multipotential mesenchymal
progenitor cells from trabecular bone. Mol Biotechnol. 23:37–49.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Haynesworth SE, Baber MA and Caplan AI:
Cytokine expression by human marrow-derived mesenchymal progenitor
cells in vitro: Effects of dexamethasone and IL-1 alpha. J Cell
Physiol. 166:585–592. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Hsiao SP and Chen SL: Myogenic regulatory
factors regulate M-cadherin expression by targeting its proximal
promoter elements. Biochem J. 428:223–233. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Kobayashi ET, Hashimoto F, Kobayashi Y,
Sakai E, Miyazaki Y, Kamiya T, Kobayashi K, Kato Y and Sakai H:
Force-induced rapid changes in cell fate at midpalatal suture
cartilage of growing rats. J Dent Res. 78:1495–1504. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Shi Y, Hu G, Su J, Li W, Chen Q, Shou P,
Xu C, Chen X, Huang Y, Zhu Z, et al: Mesenchymal stem cells: A new
strategy for immunosuppression and tissue repair. Cell Res.
20:510–518. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Haas AJ: The treatment of maxillary
deficiency by opening the midpalatal suture. Angel Orthod.
35:200–217. 1965.
|
|
23
|
Hall B, Andreeff M and Marini F: The
participation of mesenchymal stem cells in tumor stroma formation
and their application as targeted-gene delivery vehicles. Handb Exp
Pharmacol. 263–283. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Takahashi I, Mizoguchi I, Nakamura M,
Sasano Y, Saitoh S, Kagayama M and Mitani H: Effects of expansive
force on the differentiation of midpalatal suture cartilage in
rats. Bone. 18:341–348. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Kitoh H, Kitakoji T, Tsuchiya H, Mitsuyama
H, Nakamura H, Katoh M and Ishiguro N: Transplantation of
marrow-derived mesenchymal stem cells and platelet-rich plasma
during distraction osteogenesis-a preliminary result of three
cases. Bone. 35:892–898. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Qi M, Hu J, Zou S, Zhou H and Han L:
Mandibular distraction osteogenesis enhanced by bone marrow
mesenchymal stem cells in rats. J Craniomaxillofac Surg.
34:283–289. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Bi B, Schmitt R, Israilova M, Nishio H and
Cantley LG: Stromal cells protect against acute tubular injury via
an endocrine effect. J Am Soc Nephrol. 18:2486–2496. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Kumagai K, Vasanji A, Drazba JA, Butler RS
and Muschler GF: Circulating cells with osteogenic potential are
physiologically mobilized into the fracture healing site in the
parabiotic mice model. J Orthop Res. 26:165–175. 2008. View Article : Google Scholar
|
|
29
|
Matsumoto T, Kuroda R, Mifune Y, Kawamoto
A, Shoji T, Miwa M, Asahara T and Kurosaka M: Circulating
endothelial/skeletal progenitor cells for bone regeneration and
healing. Bone. 43:434–439. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Zuscik MJ, Hilton MJ, Zhang X, Chen D and
O'keefe RJ: Regulation of chondrogenesis and chondrocyte
differentiation by stress. J Clin Invest. 118:429–438. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Colnot C, Zhang X and Knothe Tate ML:
Current insights on the regenerative potential of the periosteum:
Molecular, cellular and endogenous engineering approaches. J Orthop
Res. 30:1869–1878. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Peng H and Huard J: Stem cells in the
treatment of muscle and connective tissue diseases. Curr Opin
Pharmacol. 3:329–333. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Iacovoni A, De Maria R and Gavazzi A:
Alcoholic cardiomyopathy. J Cardiovasc Med (Hagerstown).
11:884–892. 2010. View Article : Google Scholar
|
|
34
|
Gharaibeh B, Lavasani M, Cummins JH and
Huard J: Terminal differentiation is not a major determinant for
the success of stem cell therapy-cross-talk between muscle-derived
stem cells and host cells. Stem Cell Res Ther. 2:312011. View Article : Google Scholar
|
|
35
|
Laird DJ, Von Andrian UH and Wagers AJ:
Stem cell trafficking in tissue development, growth and disease.
Cell. 132:612–630. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Frimberger AE, Mcauliffe CI, Werme KA,
Tuft RA, Fogarty KE, Benoit BO, Dooner MS and Quesenberry PJ: The
fleet feet of haematopoietic stem cells: Rapid motility,
interaction and proteopodia. Br J Haematol. 112:644–654. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Steingen C, Brenig F, Baumgartner L,
Schmidt J, Schmidt A and Bloch W: Characterization of key
mechanisms in transmigration and invasion of mesenchymal stem
cells. J Mol Cell Cardiol. 44:1072–1084. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Park CC, Bissell MJ and Barcellos-Hoff MH:
The influence of the microenvironment on the malignant phenotype.
Mol Med Today. 6:324–329. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Roorda BD, Ter Elst A, Kamps WA and De
Bont ES: Bone marrow-derived cells and tumor growth: Contribution
of bone marrow-derived cells to tumor micro-environments with
special focus on mesenchymal stem cells. Crit Rev Oncol Hematol.
69:187–198. 2009. View Article : Google Scholar
|
|
40
|
Pitchford SC, Hahnel MJ, Jones CP and
Rankin SM: Troubleshooting: Quantification of mobilization of
progenitor cell subsets from bone marrow in vivo. J Pharmacol
Toxicol Methods. 61:113–121. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Glass R, Synowitz M, Kronenberg G,
Walzlein JH, Markovic DS, Wang LP, Gast D, Kiwit J, Kempermann G
and Kettenmann H: Glioblastoma-induced attraction of endogenous
neural precursor cells is associated with improved survival. J
Neurosci. 25:2637–2646. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Walzlein JH, Synowitz M, Engels B,
Markovic DS, Gabrusiewicz K, Nikolaev E, Yoshikawa K, Kaminska B,
Kempermann G, Uckert W, et al: The antitumorigenic response of
neural precursors depends on subventricular proliferation and age.
Stem Cells. 26:2945–2954. 2008. View Article : Google Scholar : PubMed/NCBI
|














