Soft tissue sarcomas (STS) are a heterogeneous group
of solid tumours arising from transformed cells of mesenchymal
origin. They may occur throughout the body and represent ~1% of all
adult malignancies (1). In
patients with primary diagnosed STS without distant metastasis,
standard treatment involves surgical resection with negative
margins, typically followed by adjuvant radiation to decrease the
risk of recurrence (2,3). However, almost half of all patients
with STS develop distant metastases, rendering them unsuitable for
surgery (4,5). If metastasis has occurred, the median
survival time regardless of chemotherapeutic treatment is <12
months (6,7). A limited number of chemotherapeutic
agents, including doxorubicin and ifosfamide, are effective for the
treatment of metastatic STS (2).
However, the response rates of these agents are poor and often do
not result in significant extension of survival (8). Doxorubicin is the predominant
chemotherapeutic agent used for the treatment of metastatic STS,
and has a response rate of ~30% (9,10).
The combination of doxorubicin and ifosfamide exhibits greater
response rates compared with doxorubicin alone; however, it is
associated with severe short- and long-term adverse effects,
including bone marrow suppression and cardiomyopathy (11–13).
A multicentre analysis by the European Organisation
for Research and Treatment of Cancer (trial 62012) on 455 patients
with advanced STS indicated that an intensified combination
treatment with doxorubicin and ifosfamide is not suitable for
treatment of locally advanced or metastatic STS as a result of the
serious adverse effects, and should therefore only be used with a
view to tumour shrinkage (13).
Furthermore, the versatility of doxorubicin is limited by
dose-associated and cumulative myocardial toxicity, particularly in
older patients with a history of cardiac disease (14). However, the incidence of STS
increases markedly >50 years of age, when the prevalence of
cardiac diseases is also greater (15). Currently, there are no efficacious
and safe agents for the palliative treatment of patients who may
not undergo doxorubicin-based chemotherapy due to underlying
cardiac disease. Therefore, the development of novel therapeutic
agents is required for the treatment of STS.
A review of the literature reveals various potential
well-tolerated and natural phytochemicals that exhibit
anti-neoplastic effects on malignant cells, including the compounds
epigallocatechin-3-gallate (EGCG), silibinin and noscapine. EGCG is
the most abundant catechin in green tea and demonstrates
anti-inflammatory, antioxidant and antineoplastic activities
(16–18). Various in vitro studies have
revealed that EGCG exhibits anticancer activity in lung (19), prostate (20), colon (21), gastric (22), breast (23) and cervical carcinoma cells
(24). To date, EGCG has undergone
various phase II trials and has been demonstrated to be
well-tolerated following oral administration (25–29).
The most frequent adverse reactions observed were gastrointestinal
reactions, including nausea and vomiting. In rare cases, patients
presented with elevated serum alanine aminotransferase levels
following the administration of high doses of oral EGCG; however,
liver function tests returned to baseline following discontinuation
of ECGC (30). Therefore, EGCG is
considered to be a safe and well-tolerated agent for the treatment
of cancer patients (31,32).
Silibinin is the primary active constituent of
silymarin, a standardized extract from the seeds of the milk
thistle plant (Silybum marianum). Silibinin is available as
a therapeutic agent in various European countries and is used for
the treatment of toxic liver damage, particularly due to Amanita
phalloides intoxication (33).
It is well tolerated in cancer patients (34,35)
and has demonstrated anti-neoplastic effects in various malignant
cell lines including HT1080 fibrosarcoma cells (36–40).
Noscapine is a naturally occurring opium alkaloid
and a widely used antitussive drug that is non-addictive and has a
low toxicity profile (41). As a
tubulin-binding agent, various preclinical studies have established
its tumour-inhibitory effects in a wide range of malignancies
(42–45). Currently, noscapine is undergoing
phase II clinical trials for cancer chemotherapy (46).
Based on these results, the present study aimed to
investigate the anti-proliferative activity of EGCG, silibinin and
noscapine on eight different STS cell lines, including
fibrosarcoma, liposarcoma, synovial sarcoma and pleomorphic sarcoma
cells.
Eight different human STS cell lines were used in
the present study: HT1080 (fibrosarcoma), SW872 (liposarcoma), T778
(liposarcoma), MLS-402 (liposarcoma), SW982 (synovial sarcoma),
SYO1 (synovial sarcoma), 1273 (synovial sarcoma) and U2197
(pleomorphic sarcoma/malignant fibrous histiocytoma). HT1080, SW872
and SW982 were purchased from CLS Cell Lines Service GmbH
(Eppelheim, Germany) and were cultured in Dulbecco's modified
Eagle's medium (DMEM; PAN-Biotech GmbH, Aidenbach, Germany)
supplemented with 10% foetal bovine serum (FBS; Thermo Fisher
Scientific, Inc., Waltham, MA, USA), 1% penicillin (100 U/ml) and
1% streptomycin (100 µg/ml; PAN-Biotech GmbH). The
well-differentiated T778 liposarcoma cell line and the MLS-402
myxoid liposarcoma cell line were donated by Professor Pierre Åman
(University of Gothenburg, Gothenburg, Sweden) and Professor Ola
Myklebost (Oslo University Hospital, Oslo, Norway), respectively.
T778 and MLS-402 cells were cultured in RPMI (PAN-Biotech GmbH)
supplemented with 10% FBS and 1% penicillin/streptomycin as
previously described (47,48). The SYO-1 and 1273 cell lines were
donated by Dr Akira Kawai (National Cancer Center, Tokyo, Japan)
and Professor Olle Larsson (Karolinska Institutet, Stockholm,
Sweden) (49,50). The SYO-1 cells were cultured in
DMEM supplemented with 10% FBS, 1% penicillin/streptomycin and 0.5%
sodium pyruvate. The 1273 cells were cultivated in Ham's F12
(PAN-Biotech GmbH) supplemented with 10% FBS and 1%
penicillin/streptomycin. The U2197 cell line was obtained from the
German Collection of Microorganisms and Cell Cultures
(Braunschweig, Germany) and was cultured in minimum essential
medium (PAN-Biotech GmbH) supplemented with 20% FBS, 0.165% sodium
bicarbonate and 1% penicillin/streptomycin (51). All cultures were maintained at 37°C
in a humidified 5% CO2 atmosphere.
EGCG, silibinin and noscapine were obtained from
Sigma-Aldrich; Merck Millipore (Darmstadt, Germany). The stock
solution was dissolved in dimethyl sulfoxide (DMSO; Carl Roth GmbH
& Co. KG, Karlsruhe, Germany) and further diluted in DMEM to
concentrations of 50 µM (EGCG), 150 µM (silibinin) and 30 µM
(noscapine) for all assays. These concentrations have been
demonstrated to inhibit proliferation and induce apoptosis in
various malignant cell lines (36,52,53).
Metabolic activity was measured using an MTT assay.
Cells were seeded in 96-well plates (Corning Incorporated, Corning,
NY, USA) at 1×104 cells per well. The following day, the
three agents were added in the aforementioned concentrations for 24
h. Subsequently, 50 µl 0.5 mg/ml MTT (Sigma-Aldrich; Merck
Millipore) was added for 4 h. MTT is a yellow dye that is reduced
to purple formazan in the mitochondria of vital cells. Cells were
lysed following the addition of 200 µl DMSO and 25 µl glycine
buffer (containing 0.1 M glycine and 0.1 M NaCl, adjusted to pH
10.5 with NaOH) per well. The quantity of integrated dye
represented the level of metabolism and was measured at a
wavelength of 562 nm using an Elx808 Ultra Microplate Reader
(BioTek Instruments GmbH, Bad Friedrichshall, Germany).
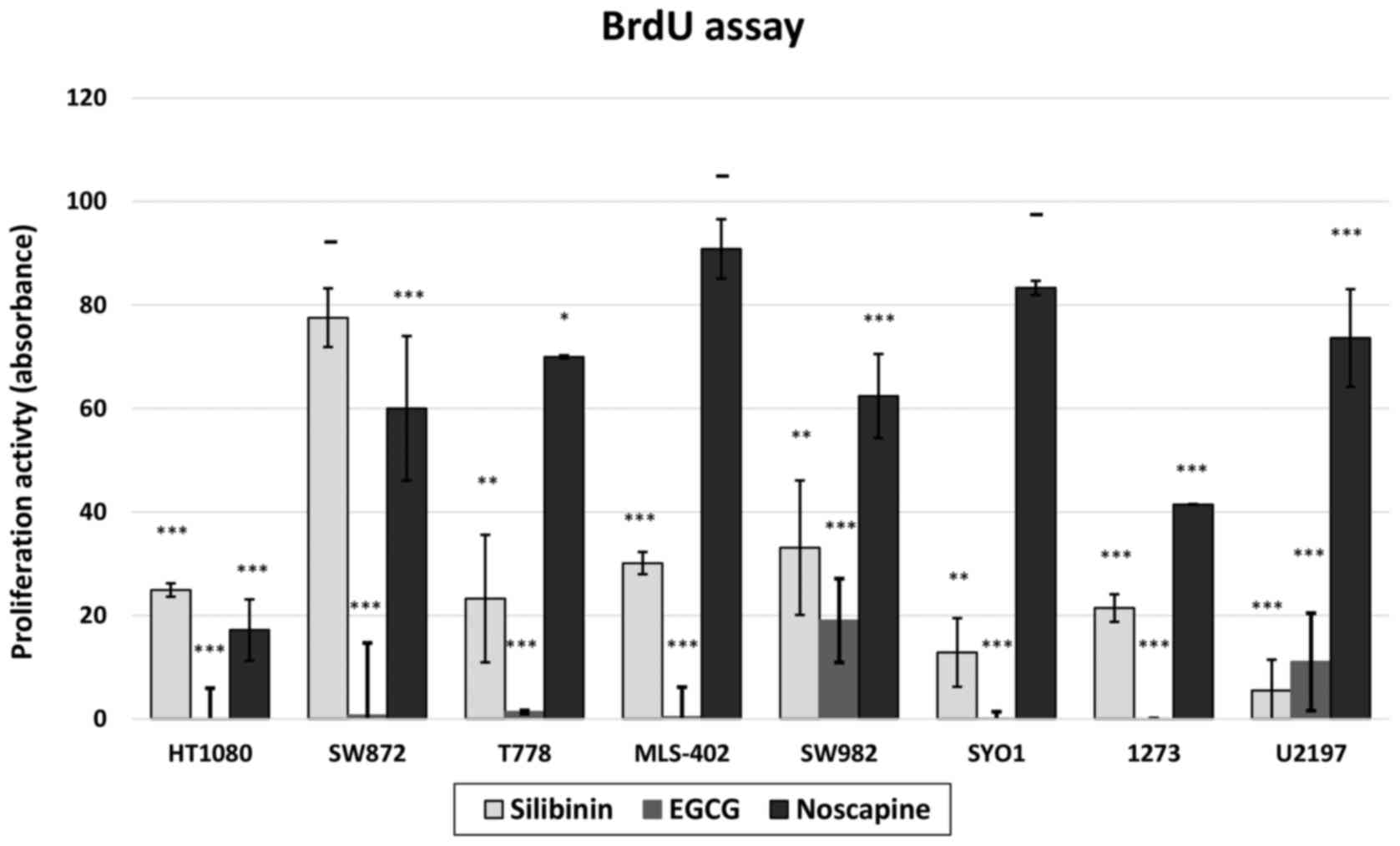
To quantify the effects of EGCG, silibinin and
noscapine on cell proliferation, a colorimetric cell proliferation
5-bromo-2′-deoxyuridine (BrdU)-ELISA assay (Roche Diagnostics GmbH,
Mannheim, Germany) was performed according to the manufacturer's
protocol. Briefly, cells were seeded at 1×104 cells/well
in 96-well plates and cultured for 24 h. The phytotherapeutic
agents were subsequently added in the appropriate concentrations
for 24 h. The BrdU labelling solution was added and incubated for a
further 24 h. BrdU, a pyrimidine analogue, integrates into the DNA
of proliferating cells. The level of proliferation was quantified
by the light emission detected via an Orion Microplate Luminometer
(Berthold Detection Systems GmbH, Pforzheim, Germany). Cell
proliferation was determined in quadruplicate. The results are
expressed as a percentage of the proliferation of DMSO-treated
control cells.
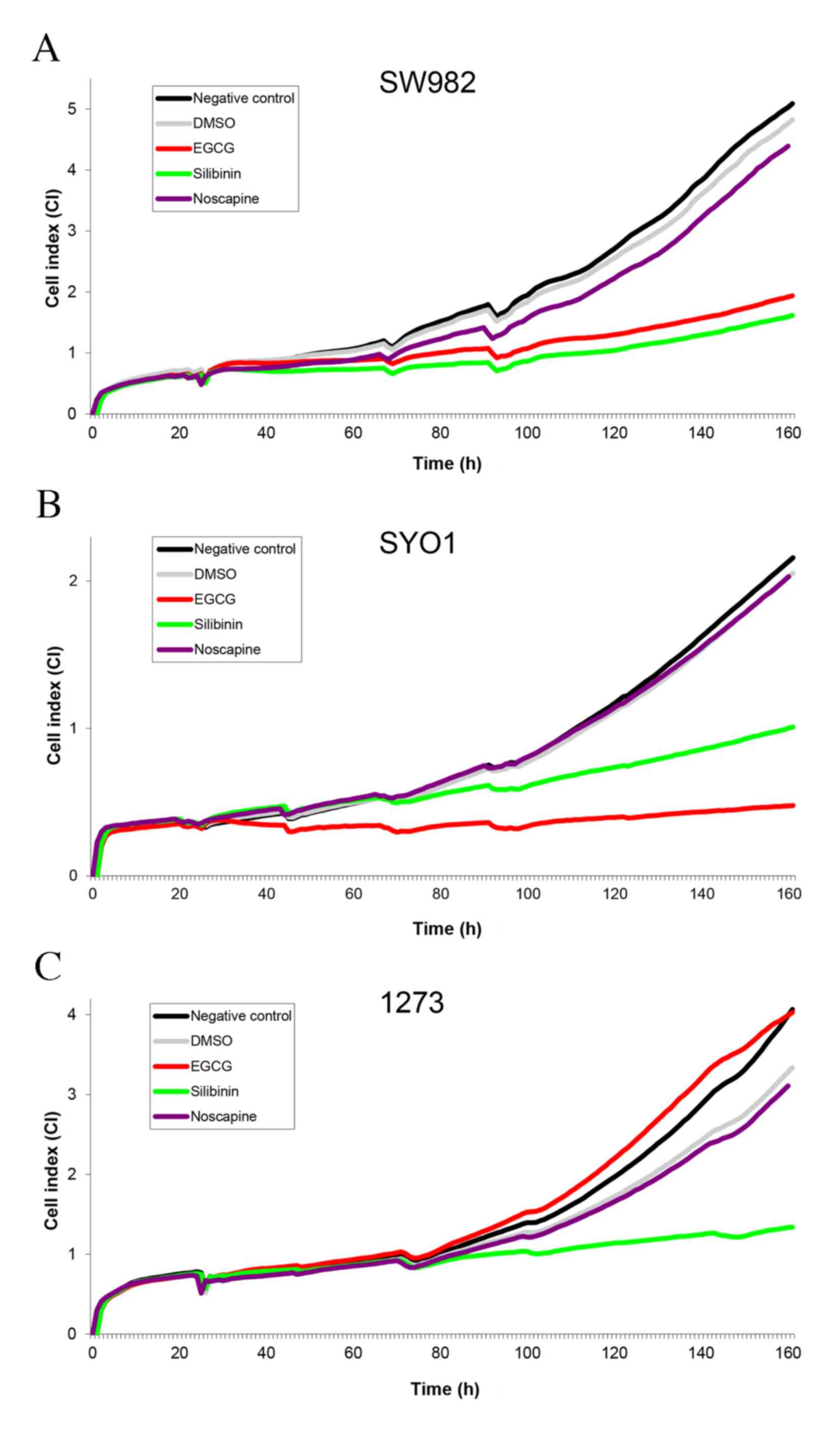
Cells were seeded in two 8-well plates with an
integrated microelectronic sensor array in 600 µl culture medium
(iCELLigence Real Time Cell Analyser; ACEA Biosciences, San Diego,
CA, USA). After 24 h, the therapeutic agents were added for a total
volume of 50 µl. The cell proliferation and survival were monitored
in real-time by measuring the cell-to-electrode responses of the
seeded cells. In each individual E-well, the cell impedance was
measured and converted to cell index (CI) values by the RTCA
software version 1.2 (Roche Diagnostics GmbH) (54). The graphs were generated in
real-time by the iCELLigence system. Untreated and DMSO-treated
cells served as controls.
Data analyses were performed using the statistical
program SPSS 16 (SPSS, Inc., Chicago, IL, USA). Data are expressed
as the mean ± standard deviation. Comparisons between the
experimental groups in BrdU and MTT assays were performed using
one-way analysis of variance followed by post-hoc Tukey's
test. P<0.05 was considered to indicate a statistically
significant difference.
As indicated by the BrdU assay, the proliferation of
all eight human STS cell lines was inhibited by EGCG (Fig. 1). By MTT analysis, EGCG decreased
the viability of seven cell lines (Fig. 2). To evaluate the proliferation and
viability of cells continuously over a longer time period, RTCA was
performed. The viability, adhesion and proliferation of the cells
were monitored prior to and during EGCG treatment in real time for
160 h (Figs. 3–5). EGCG markedly decreased the CI of all
STS cell lines except the 1273 synovial sarcoma cell line. The
administration of EGCG reduced the CI of the HT1080 fibrosarcoma
cell line and the U2197 pleomorphic sarcoma cell line (Fig. 3). All three liposarcoma cell lines
(SW872, T778 and MLS-402) exhibited a continuously decreased CI
during EGCG treatment compared with untreated or DMSO-treated cells
(Fig. 4), as did the remaining two
synovial sarcoma cells lines (SW982 and SYO1; Fig. 5).
Treatment with silibinin significantly reduced the
proliferation of seven STS cell lines (Fig. 1), and significantly decreased the
cell viability of all eight assessed STS cell lines, as analysed by
MTT assay (Fig. 2). By RTCA,
silibinin was the only compound that exhibited a strong inhibitory
effect on all three synovial sarcoma cells (Fig. 5). In addition, silibinin reduced
the CI of all liposarcoma cell lines; however, not to the extent of
EGCG. Only the U2197 pleomorphic sarcoma cell line did not respond
to silibinin treatment.
STS are a heterogeneous group of rare mesenchymal
malignancies. To date, systemic treatment options are limited
following metastasis. Patients with distant metastases have a
median survival time of less than one year despite systemic
chemotherapy (6,7). Due to the infrequent and
heterogeneous nature of STS the development of novel systemic
therapeutic agents is challenging and novel chemotherapy strategies
are lacking. Therefore, the development of well-tolerated and
effective chemotherapeutic agents for the treatment of STS is
required.
The present study assessed the cytostatic effects of
the naturally occurring compounds noscapine, silibinin and EGCG on
eight STS cell lines. By RTCA, noscapine did not exhibit any
relevant anti-proliferative effects (Table I). In contrast, silibinin and EGCG
exerted cytostatic effects in almost all examined STS cell lines,
as assessed by BrdU, MTT and RTCA. Administration of EGCG decreased
proliferation and viability of all liposarcoma cell lines and two
synovial sarcoma cell lines for more than five days. In addition,
it inhibited HT1080 fibrosarcoma and U2197 pleomorphic sarcoma
cells. Of the three analysed compounds, EGCG exerted the greatest
anti-proliferative activity in the three assessed liposarcoma cell
lines, rendering it a potential agent of interest. Liposarcomas
represent the most frequent somatic STS subtype and respond poorly
to anthracycline-based chemotherapy, with well-differentiated and
de-differentiated tumours exhibiting response rates of only 12 and
13%, respectively (55).
Pleomorphic liposarcomas are the least responsive to chemotherapy,
with a response rate of 5%, whereas myxoid liposarcomas have been
revealed to be the most sensitive to chemotherapy, exhibiting
response rates of 44–48% (56–58).
In the present study, EGCG exhibited a distinct inhibitory effect
on T778 cells from a well-differentiated liposarcoma, SW872 cells
from a pleomorphic liposarcoma and MLS-402 cells from a myxoid
liposarcoma. Although these findings were in vitro, they
suggested a potential anti-proliferative activity of EGCG on
liposarcoma cells that should be further investigated in
vivo.
In comparison with EGCG, the inhibitory effect of
silibinin was reduced in liposarcoma cells, but greater in synovial
sarcoma cells. Silibinin significantly decreased proliferation and
viability in all three synovial sarcoma cell lines. Although
synovial sarcomas have typically been considered relatively
chemosensitive, the European Organisation for Research and
Treatment of Cancer recently reported a chemotherapy response rate
of only 28% for patients with advanced synovial sarcoma (59). Therefore, there remains a
requirement for alternative cytostatic agents for the treatment for
synovial sarcomas, and the in vitro effects of silibinin
demonstrated in the present study should be further examined in
vivo.
A literature review revealed that the green tea
polyphenol EGCG has further notable properties. Various in
vivo studies have confirmed that EGCG mitigates
doxorubicin-induced cardiotoxicity by suppressing oxidative stress
(60–63). The oxygen free radical scavenging
ability of EGCG has been demonstrated to protect cardiomyocytes
from doxorubicin-mediated cardiotoxicity according to
histopathological analysis (64).
Furthermore, EGCG has been revealed to synergistically enhance the
anticancer activity of doxorubicin in various in vivo
studies on prostate and liver cancer (65–67).
Notably, similar chemosensitizing and chemopreventive activities
have been described for silibinin; in vivo studies revealed
that silibinin synergistically enhances the apoptosis-inducing
activity of doxorubicin and ameliorates doxorubicin-induced
cardiotoxicity (68–73). Therefore, EGCG and silibinin may
additionally function as chemopreventives and chemosensitizers for
doxorubicin, which remains the first-line cytostatic for the
systemic treatment of disseminated STS.
The present study was supported by a FoRUM grant
from the Ruhr-University Bochum (Bochum, Germany; grant no.
K090-15).
|
1
|
Hoos A, Lewis JJ and Brennan MF:
Weichgewebssarkome-prognostische Faktoren und multimodale Therapie.
Der Chirurg. 71:787–794. 2000. View Article : Google Scholar
|
|
2
|
Patrikidou A, Domont J, Cioffi A and Le
Cesne A: Treating soft tissue sarcomas with adjuvant chemotherapy.
Curr Treat Options Oncol. 12:21–31. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kaushal A and Citrin D: The role of
radiation therapy in the management of sarcomas. Surg Clin North
Am. 88629–646. (viii)2008.PubMed/NCBI
|
|
4
|
O'Brien GC, Cahill RA, Bouchier-Hayes DJ
and Redmond HP: Co-immunotherapy with interleukin-2 and taurolidine
for progressive metastatic melanoma. Ir J Med Sci. 175:10–14. 2006.
View Article : Google Scholar
|
|
5
|
Solomon LR, Cheesbrough JS, Bhargava R,
Mitsides N, Heap M, Green G and Diggle P: Observational study of
need for thrombolytic therapy and incidence of bacteremia using
taurolidine-citrate-heparin, taurolidine-citrate and heparin
catheter locks in patients treated with hemodialysis. Semin Dial.
25:233–238. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Karavasilis V, Seddon BM, Ashley S,
Al-Muderis O, Fisher C and Judson I: Significant clinical benefit
of first-line palliative chemotherapy in advanced soft-tissue
sarcoma: Retrospective analysis and identification of prognostic
factors in 488 patients. Cancer. 112:1585–1591. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Billingsley KG, Lewis JJ, Leung DH, Casper
ES, Woodruff JM and Brennan MF: Multifactorial analysis of the
survival of patients with distant metastasis arising from primary
extremity sarcoma. Cancer. 85:389–395. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Pezzi CM, Pollock RE, Evans HL, Lorigan
JG, Pezzi TA, Benjamin RS and Romsdahl MM: Preoperative
chemotherapy for soft-tissue sarcomas of the extremities. Ann Surg.
211:476–481. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Di Paola Donato E and Nielsen OS: EORTC
Soft Tissue and Bone Sarcoma Group: The EORTC soft tissue and bone
sarcoma group. European Organisation for Research and Treatment of
Cancer. Eur J Cancer. 38:(Suppl 4). S138–S141. 2002.PubMed/NCBI
|
|
10
|
Nedea EA and DeLaney TF: Sarcoma and skin
radiation oncology. Hematol Oncol Clin North Am. 20:401–429. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Brodowicz T, Schwameis E, Widder J, Amann
G, Wiltschke C, Dominkus M, Windhager R, Ritschl P, Pötter R, Kotz
R and Zielinski CC: Intensified adjuvant IFADIC chemotherapy for
adult soft tissue sarcoma: A prospective randomized feasibility
trial. Sarcoma. 4:151–160. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Frustaci S, Gherlinzoni F, De Paoli A,
Bonetti M, Azzarelli A, Comandone A, Olmi P, Buonadonna A, Pignatti
G, Barbieri E, et al: Adjuvant chemotherapy for adult soft tissue
sarcomas of the extremities and girdles: Results of the Italian
randomized cooperative trial. J Clin Oncol. 19:1238–1247.
2001.PubMed/NCBI
|
|
13
|
Judson I, Verweij J, Gelderblom H,
Hartmann JT, Schöffski P, Blay JY, Kerst JM, Sufliarsky J, Whelan
J, Hohenberger P, et al: Doxorubicin alone versus intensified
doxorubicin plus ifosfamide for first-line treatment of advanced or
metastatic soft-tissue sarcoma: A randomised controlled phase 3
trial. Lancet Oncol. 15:415–423. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Swain SM, Whaley FS and Ewer MS:
Congestive heart failure in patients treated with doxorubicin: A
retrospective analysis of three trials. Cancer. 97:2869–2879. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Burningham Z, Hashibe M, Spector L and
Schiffman JD: The epidemiology of sarcoma. Clin Sarcoma Res.
2:142012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Jiang L, Tao C, He A and He X:
Overexpression of miR-126 sensitizes osteosarcoma cells to
apoptosis induced by epigallocatechin-3-gallate. World J Surg
Oncol. 12:3832014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Lambert JD, Sang S, Hong J and Yang CS:
Anticancer and anti-inflammatory effects of cysteine metabolites of
the green tea polyphenol, (−)-epigallocatechin-3-gallate. J Agric
Food Chem. 58:10016–10019. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Kalaiselvi P, Rajashree K, Bharathi Priya
L and Padma VV: Cytoprotective effect of epigallocatechin-3-gallate
against deoxynivalenol-induced toxicity through anti-oxidative and
anti-inflammatory mechanisms in HT-29 cells. Food Chem Toxicol.
56:110–118. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Deng YT and Lin JK: EGCG inhibits the
invasion of highly invasive CL1-5 lung cancer cells through
suppressing MMP-2 expression via JNK signaling and induces G2/M
arrest. J Agric Food Chem. 59:13318–13327. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Kobalka AJ, Keck RW and Jankun J:
Synergistic anticancer activity of biologicals from green and black
tea on DU 145 human prostate cancer cells. Cent Eur J Immunol.
40:1–4. 2015.PubMed/NCBI
|
|
21
|
Park IJ, Lee YK, Hwang JT, Kwon DY, Ha J
and Park OJ: Green tea catechin controls apoptosis in colon cancer
cells by attenuation of H2O2-stimulated COX-2 expression via the
AMPK signaling pathway at low-dose H2O2. Ann N Y Acad Sci.
1171:538–544. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Park JS, Khoi PN, Joo YE, Lee YH, Lang SA,
Stoeltzing O and Jung YD: EGCG inhibits recepteur d'origine nantais
expression by suppressing Egr-1 in gastric cancer cells. Int J
Oncol. 42:1120–1126. 2013.PubMed/NCBI
|
|
23
|
Braicu C, Gherman CD, Irimie A and
Berindan-Neagoe I: Epigallocatechin-3-Gallate (EGCG) inhibits cell
proliferation and migratory behaviour of triple negative breast
cancer cells. J Nanosci Nanotechnol. 13:632–637. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Zou C, Liu H, Feugang JM, Hao Z, Chow HH
and Garcia F: Green tea compound in chemoprevention of cervical
cancer. Int J Gynecol Cancer. 20:617–624. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Shanafelt TD, Call TG, Zent CS, Leis JF,
LaPlant B, Bowen DA, Roos M, Laumann K, Ghosh AK, Lesnick C, et al:
Phase 2 trial of daily, oral Polyphenon E in patients with
asymptomatic, Rai stage 0 to II chronic lymphocytic leukemia.
Cancer. 119:363–370. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
de la Torre R, de Sola S, Hernandez G,
Farré M, Pujol J, Rodriguez J, Espadaler JM, Langohr K, Cuenca-Royo
A, Principe A, et al: Safety and efficacy of cognitive training
plus epigallocatechin-3-gallate in young adults with Down's
syndrome (TESDAD): A double-blind, randomised, placebo-controlled,
phase 2 trial. Lancet Neurol. 15:801–810. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Zhao H, Xie P, Li X, Zhu W, Sun X, Sun X,
Chen X, Xing L and Yu J: A prospective phase II trial of EGCG in
treatment of acute radiation-induced esophagitis for stage III lung
cancer. Radiother Oncol. 114:351–356. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Trudel D, Labbé DP, Araya-Farias M, Doyen
A, Bazinet L, Duchesne T, Plante M, Grégoire J, Renaud MC,
Bachvarov D, et al: A two-stage, single-arm, phase II study of
EGCG-enriched green tea drink as a maintenance therapy in women
with advanced stage ovarian cancer. Gynecol Oncol. 131:357–361.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Dostal AM, Samavat H, Bedell S, Torkelson
C, Wang R, Swenson K, Le C, Wu AH, Ursin G, Yuan JM and Kurzer MS:
The safety of green tea extract supplementation in postmenopausal
women at risk for breast cancer: Results of the Minnesota Green Tea
Trial. Food Chem Toxicol. 83:26–35. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Garcia FA, Cornelison T, Nuño T, Greenspan
DL, Byron JW, Hsu CH, Alberts DS and Chow HH: Results of a phase II
randomized, double-blind, placebo-controlled trial of Polyphenon E
in women with persistent high-risk HPV infection and low-grade
cervical intraepithelial neoplasia. Gynecol Oncol. 132:377–382.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Singh BN, Shankar S and Srivastava RK:
Green tea catechin, epigallocatechin-3-gallate (EGCG): Mechanisms,
perspectives and clinical applications. Biochem Pharmacol.
82:1807–1821. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Shanafelt TD, Call TG, Zent CS, LaPlant B,
Bowen DA, Roos M, Secreto CR, Ghosh AK, Kabat BF, Lee MJ, et al:
Phase I trial of daily oral Polyphenon E in patients with
asymptomatic Rai stage 0 to II chronic lymphocytic leukemia. J Clin
Oncol. 27:3808–3814. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Mengs U, Pohl RT and Mitchell T:
Legalon® SIL: The antidote of choice in patients with
acute hepatotoxicity from amatoxin poisoning. Curr Pharm
Biotechnol. 13:1964–1970. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Flaig TW, Glodé M, Gustafson D, van
Bokhoven A, Tao Y, Wilson S, Su LJ, Li Y, Harrison G, Agarwal R, et
al: A study of high-dose oral silybin-phytosome followed by
prostatectomy in patients with localized prostate cancer. Prostate.
70:848–855. 2010.PubMed/NCBI
|
|
35
|
Flaig TW, Gustafson DL, Su LJ, Zirrolli
JA, Crighton F, Harrison GS, Pierson AS, Agarwal R and Glodé LM: A
phase I and pharmacokinetic study of silybin-phytosome in prostate
cancer patients. Invest New Drugs. 25:139–146. 2007.PubMed/NCBI
|
|
36
|
Kaur M, Velmurugan B, Tyagi A, Deep G,
Katiyar S, Agarwal C and Agarwal R: Silibinin suppresses growth and
induces apoptotic death of human colorectal carcinoma LoVo cells in
culture and tumor xenograft. Mol Cancer Ther. 8:2366–2374. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Singh RP and Agarwal R: Prostate cancer
chemoprevention by silibinin: Bench to bedside. Mol Carcinog.
45:436–442. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Leon IE, Porro V, Di Virgilio AL, Naso LG,
Williams PA, Bollati-Fogolín M and Etcheverry SB: Antiproliferative
and apoptosis-inducing activity of an oxidovanadium (IV) complex
with the flavonoid silibinin against osteosarcoma cells. J Biol
Inorg Chem. 19:59–74. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Vue B, Zhang S, Zhang X, Parisis K, Zhang
Q, Zheng S, Wang G and Chen QH: Silibinin derivatives as
anti-prostate cancer agents: Synthesis and cell-based evaluations.
Eur J Med Chem. 109:36–46. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Duan WJ, Li QS, Xia MY, Tashiro S, Onodera
S and Ikejima T: Silibinin activated p53 and induced autophagic
death in human fibrosarcoma HT1080 cells via reactive oxygen
species-p38 and c-Jun N-terminal kinase pathways. Biol Pharm Bull.
34:47–53. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Ghaly PE, El-Magd RM Abou, Churchill CD,
Tuszynski JA and West FG: A new antiproliferative noscapine
analogue: Chemical synthesis and biological evaluation. Oncotarget.
7:40518–40530. 2016.PubMed/NCBI
|
|
42
|
Yang ZR, Liu M, Peng XL, Lei XF, Zhang JX
and Dong WG: Noscapine induces mitochondria-mediated apoptosis in
human colon cancer cells in vivo and in vitro. Biochem Biophys Res
Commun. 421:627–633. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Li S, He J, Li S, Cao G, Tang S, Tong Q
and Joshi HC: Noscapine induced apoptosis via downregulation of
survivin in human neuroblastoma cells having wild type or null p53.
PloS One. 7:e400762012. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Quisbert-Valenzuela EO and Calaf GM:
Apoptotic effect of noscapine in breast cancer cell lines. Int J
Oncol. 48:2666–2674. 2016.PubMed/NCBI
|
|
45
|
Lopus M and Naik PK: Taking aim at a
dynamic target: Noscapinoids as microtubule-targeted cancer
therapeutics. Pharmacol Rep. 67:56–62. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Mukkavilli R, Gundala SR, Yang C, Jadhav
GR, Vangala S, Reid MD and Aneja R: Noscapine recirculates
enterohepatically and induces self-clearance. Eur J Pharm Sci.
77:90–99. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Stratford EW, Castro R, Daffinrud J, Skårn
M, Lauvrak S, Munthe E and Myklebost O: Characterization of
liposarcoma cell lines for preclinical and biological studies.
Sarcoma. 2012:1486142012.PubMed/NCBI
|
|
48
|
Aman P, Ron D, Mandahl N, Fioretos T, Heim
S, Arheden K, Willén H, Rydholm A and Mitelman F: Rearrangement of
the transcription factor gene CHOP in myxoid liposarcomas with
t(12;16)(q13;p11). Genes, chromosomes cancer. 5:278–285. 1992.
View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Kawai A, Naito N, Yoshida A, Morimoto Y,
Ouchida M, Shimizu K and Beppu Y: Establishment and
characterization of a biphasic synovial sarcoma cell line, SYO-1.
Cancer Lett. 204:105–113. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Xie Y, Skytting B, Nilsson G, Gasbarri A,
Haslam K, Bartolazzi A, Brodin B, Mandahl N and Larsson O: SYT-SSX
is critical for cyclin D1 expression in synovial sarcoma cells: A
gain of function of the t(X;18)(p11.2;q11.2) translocation. Cancer
Res. 62:3861–3867. 2002.PubMed/NCBI
|
|
51
|
Becerikli M, Jacobsen F, Rittig A, Köhne
W, Nambiar S, Mirmohammadsadegh A, Stricker I, Tannapfel A,
Wieczorek S, Epplen JT, et al: Growth rate of late passage sarcoma
cells is independent of epigenetic events but dependent on the
amount of chromosomal aberrations. Exp Cell Res. 319:1724–1731.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Kang HG, Jenabi JM, Liu XF, Reynolds CP,
Triche TJ and Sorensen PH: Inhibition of the insulin-like growth
factor I receptor by epigallocatechin gallate blocks proliferation
and induces the death of Ewing tumor cells. Mol Cancer Ther.
9:1396–1407. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Chougule MB, Patel AR, Jackson T and Singh
M: Antitumor activity of Noscapine in combination with Doxorubicin
in triple negative breast cancer. PloS One. 6:e177332011.
View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Koval OA, Sakaeva GR, Fomin AS, Nushtaeva
AA, Semenov DV, Kuligina EV, Gulyaeva LF, Gerasimov AV and Richter
VA: Sensitivity of endometrial cancer cells from primary human
tumor samples to new potential anticancer peptide lactaptin. J
Cancer Res Ther. 11:345–351. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Italiano A, Toulmonde M, Cioffi A, Penel
N, Isambert N, Bompas E, Duffaud F, Patrikidou A, Lortal B, Le
Cesne A, et al: Advanced well-differentiated/dedifferentiated
liposarcomas: Role of chemotherapy and survival. Ann Oncol.
23:1601–1607. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Italiano A, Garbay D, Cioffi A, Maki RG
and Bui B: Advanced pleomorphic liposarcomas: Clinical outcome and
impact of chemotherapy. Ann Oncol. 23:2205–2206. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Jones RL, Fisher C, Al-Muderis O and
Judson IR: Differential sensitivity of liposarcoma subtypes to
chemotherapy. Eur J Cancer. 41:2853–2860. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Patel SR, Burgess MA, Plager C,
Papadopoulos NE, Linke KA and Benjamin RS: Myxoid liposarcoma.
Experience with chemotherapy. Cancer. 74:1265–1269. 1994.
View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Vlenterie M, Litière S, Rizzo E, Marréaud
S, Judson I, Gelderblom H, Le Cesne A, Wardelmann E, Messiou C,
Gronchi A and van der Graaf WT: Outcome of chemotherapy in advanced
synovial sarcoma patients: Review of 15 clinical trials from the
European Organisation for Research and Treatment of Cancer Soft
Tissue and Bone Sarcoma Group; setting a new landmark for studies
in this entity. Eur J Cancer. 58:62–72. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Saeed NM, El-Naga RN, El-Bakly WM,
Abdel-Rahman HM, Salah ElDin RA and El-Demerdash E:
Epigallocatechin-3-gallate pretreatment attenuates
doxorubicin-induced cardiotoxicity in rats: A mechanistic study.
Biochem Pharmacol. 95:145–155. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Khan MA, Singh M, Khan MS, Ahmad W, Najmi
AK and Ahmad S: Alternative approach for mitigation of
doxorubicin-induced cardiotoxicity using herbal agents. Curr Clin
Pharmacol. 9:288–297. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Zheng J, Lee HC, Bin Sattar MM, Huang Y
and Bian JS: Cardioprotective effects of epigallocatechin-3-gallate
against doxorubicin-induced cardiomyocyte injury. Eur J Pharmacol.
652:82–88. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Li W, Nie S, Xie M, Chen Y, Li C and Zhang
H: A major green tea component, (−)-epigallocatechin-3-gallate,
ameliorates doxorubicin-mediated cardiotoxicity in cardiomyocytes
of neonatal rats. J Agric Food Chem. 58:8977–8982. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Cheng T, Liu J, Ren J, Huang F, Ou H, Ding
Y, Zhang Y, Ma R, An Y, Liu J and Shi L: Green tea catechin-based
complex micelles combined with doxorubicin to overcome
cardiotoxicity and multidrug resistance. Theranostics. 6:1277–1292.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Stearns ME, Amatangelo MD, Varma D, Sell C
and Goodyear SM: Combination therapy with
epigallocatechin-3-gallate and doxorubicin in human prostate tumor
modeling studies: Inhibition of metastatic tumor growth in severe
combined immunodeficiency mice. Am J Pathol. 177:3169–3179. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Chen L, Ye HL, Zhang G, Yao WM, Chen XZ,
Zhang FC and Liang G: Autophagy inhibition contributes to the
synergistic interaction between EGCG and doxorubicin to kill the
hepatoma Hep3B cells. PloS One. 9:e857712014. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Liang G, Tang A, Lin X, Li L, Zhang S,
Huang Z, Tang H and Li QQ: Green tea catechins augment the
antitumor activity of doxorubicin in an in vivo mouse model for
chemoresistant liver cancer. Int J Oncol. 37:111–123.
2010.PubMed/NCBI
|
|
68
|
Singh RP, Mallikarjuna GU, Sharma G,
Dhanalakshmi S, Tyagi AK, Chan DC, Agarwal C and Agarwal R: Oral
silibinin inhibits lung tumor growth in athymic nude mice and forms
a novel chemocombination with doxorubicin targeting nuclear factor
kappaB-mediated inducible chemoresistance. Clin Cancer Res.
10:8641–8647. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Tyagi AK, Agarwal C, Chan DC and Agarwal
R: Synergistic anti-cancer effects of silibinin with conventional
cytotoxic agents doxorubicin, cisplatin and carboplatin against
human breast carcinoma MCF-7 and MDA-MB468 cells. Oncol Rep.
11:493–499. 2004.PubMed/NCBI
|
|
70
|
Tyagi AK, Singh RP, Agarwal C, Chan DC and
Agarwal R: Silibinin strongly synergizes human prostate carcinoma
DU145 cells to doxorubicin-induced growth Inhibition, G2-M arrest,
and apoptosis. Clin Cancer Res. 8:3512–3519. 2002.PubMed/NCBI
|
|
71
|
Rašković A, Stilinović N, Kolarović J,
Vasović V, Vukmirović S and Mikov M: The protective effects of
silymarin against doxorubicin-induced cardiotoxicity and
hepatotoxicity in rats. Molecules. 16:8601–8613. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Chlopcíková S, Psotová J, Miketová P and
Simánek V: Chemoprotective effect of plant phenolics against
anthracycline-induced toxicity on rat cardiomyocytes. Part I.
Silymarin and its flavonolignans. Phytother Res. 18:107–110. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Psotová J, Chlopcíková S, Grambal F,
Simánek V and Ulrichová J: Influence of silymarin and its
flavonolignans on doxorubicin-iron induced lipid peroxidation in
rat heart microsomes and mitochondria in comparison with quercetin.
Phytother Res. 16:(Suppl 1). S63–S67. 2002. View Article : Google Scholar : PubMed/NCBI
|