Introduction
Individualized chemotherapy is an increasingly
popular type of tumor treatment. Daunorubicin (DNR) is a
chemotherapeutic of the anthracycline family, which is used as a
treatment for acute leukemia (1).
However, this drug has a higher affinity to myocardial tissue than
other tissues, which limits the application of DNR due to
accumulated cardiotoxicity (2–4).
Several studies have confirmed that cytochrome P450 family 3
subfamily A member 5 (CYP3A5) is involved in the clearance of DNR
metallization (5). Studies of
CYP3A5 have predominantly focused on osteosarcoma, breast cancer
and the use of immunosuppressants following liver or kidney
transplantation (6–9), however, few studies have reported on
the association between CYP3A5 and acute leukemia (9,10).
Thus, the present study examined the association between CYP3A5
gene polymorphisms and CYP3A enzyme activity, and plasma
concentrations of DNR. The study aimed to provide primary
experimental evidence for the use of DNR and reduction of adverse
reactions, and improve the individualized treatment of
leukemia.
Materials and methods
Subjects
According to the CCLG-ALL-2008 protocol (11), 36 children with acute lymphatic
leukemia (ALL), who were first diagnosed and hospitalized at the
Department of Hematology of the Second Affiliated Hospital and
Yuying Children's Hospital of Wenzhou Medical University (Wenzhou,
China) were enrolled in the present study between January 2009 and
July 2013. All patient diagnoses were confirmed by clinical,
morphological and immunological examinations, histochemical
staining and chromosome karyotype analysis, and included nine cases
in the low risk group, 17 cases in the moderate risk group and 10
cases in the high risk group. The ALL treatment regimen comprised
vincristine, DNR, L-asparaginase and prednisone administration for
4 weeks. DNR was injected at 30 mg/m−2 (1 h) for 2–3
days (2 days in low-risk group, 3 days in moderate and high-risk
group). Children who did not complete a course of chemotherapy and
were discharged from hospital or those who succumbed to mortality
were excluded from the investigation. The present study was
approved by the ethics committee of The Second Affiliated Hospital
and Yuying Children's Hospital of Wenzhou Medical University. All
family members of the patients provided signed informed
consent.
Genotype detection at site 6,986 of
CYP3A5
A 300 µl sample of bone marrow was collected and
stored in tubes with 2% EDTA. DNA extraction was performed
according to the manufacturer's protocol of the Wizard DNA kit
(Promega Corporation, Madison, WI, USA). Primer sequences were as
follows: Sense 5′-CATCAGTTAGTAGACAGATGA-3′ and antisense
5′-GGTCCAAACAGGGAAGAAATA-3′. A polymerase chain reaction (PCR)
amplification instrument (ABI 9600; Applied Biosystems; Thermo
Fisher Scientific, Inc., Waltham, MA, USA) was used. The reaction
volume was as follows: 0.4 µmol-l sense primer, 0.4 µmol-l
antisense primer, 2 ng DNA template, 4 mmol-l MgCl2,
0.05 U-µl Taq DNA polymerase (Promega Corporation), dNTPs (dATP,
dCTP, dGTP and dTTP, 0.4 mmol-l each), and ddH2O was added to bring
the final volume to 50 µl. The PCR conditions were as follows:
Denaturation at 94°C for 5 min, followed by 35 cycles of 94°C for
30 sec, 55°C for 30 sec, extension at 72°C for 1 min, and final
extension at 72°C for 7 min. The PCR product (20 µl) and
restriction enzyme, SspI (New England Biolabs, Ipswich, MA,
USA) were incubated at 37°C for 4 h, which was followed by 2%
agarose gel electrophoresis, staining with ethidium bromide,
observation and capturing of images using a gel image analyzer,
respectively. To confirm the results of the gel electrophoresis,
the PCR products from seven specimens were directly sequenced to
ensure the genotypes of gene variation. The sequencing results were
compared with the human genome database of NCBI (https://www.ncbi.nlm.nih.gov/gene/1577),
if A became G, it was defined as gene variation.
Detection of gene expression levels of
CYP3A5
A 3–4 ml sample of marrow was collected under
sterile conditions and stored in tubes with EDTA, followed by
immediate single karyocyte extraction, extraction of RNA (TRIzol
kit; Invitrogen; Thermo Fisher Scientific, Inc.) and cDNA synthesis
(SuperScript Double-Stranded cDNA Synthesis kit; Thermo Fisher
Scientific, Inc.) were performed according to the manufacturer's
protocols. Primer Express Software v.2.0 was used to design primers
according to the CYP3A5 mRNA sequence in GeneBank (https://www.ncbi.nlm.nih.gov/nuccore/NM_001190484.2).
Primers and probes of CYP3A5, wild-type (wt)-CYP3A5, SV1-CYP3A5 and
GAPDH (Shanghai Sangon Pharmaceutical Co., Ltd., Shanghai, China)
are listed in Table I. The PCR
conditions were as follows: Denaturation at 94°C for 5 min,
followed by 50 cycles of 95°C for 15 sec, 55°C for 60 sec, and
final extension at 72°C for 5 min. The PCR product was stored at
4°C.
 | Table I.Primers and probes used to determine
gene expression of CYP3A5. |
Table I.
Primers and probes used to determine
gene expression of CYP3A5.
| Gene | Forward primer
(5′-3′) | Reverse primer
(5′-3′) | Probe (5′-3′) |
|---|
| wt-CYP3A5 |
GGGTCTCTGGAAATTTGACACAGAG |
CTGTTCTGATCACGTCGGGATCT |
6FAM-ATGTGGGGAACGTATGAAGGTCAACTCCCT |
| SV1-CYP3A5 |
TCTCTGGAAATTTGACACAGAGTGC |
CAGCAAGAGTCTCACACAGGAGC |
6FAM-AATGTGGGGTATCTCTTCCCTGTTTGGACCA |
| GAPDH |
TCCTGCACCACCAACTGCTT |
GAGGGGCCATCCACAGTCTT |
6FAM-CACTCATGACCACAGTCCATGCCATCAC-TAMRA |
Detection of CYP3A activity using
amidazolam (MDZ) probe assay
In the morning following a period of nil-by-mouth,
the children were injected with 0.1 mg-kg MDZ solution (Jiangsu
Nhwa Pharma Co., Ltd, Jiangsu, China), and 2 ml blood was collected
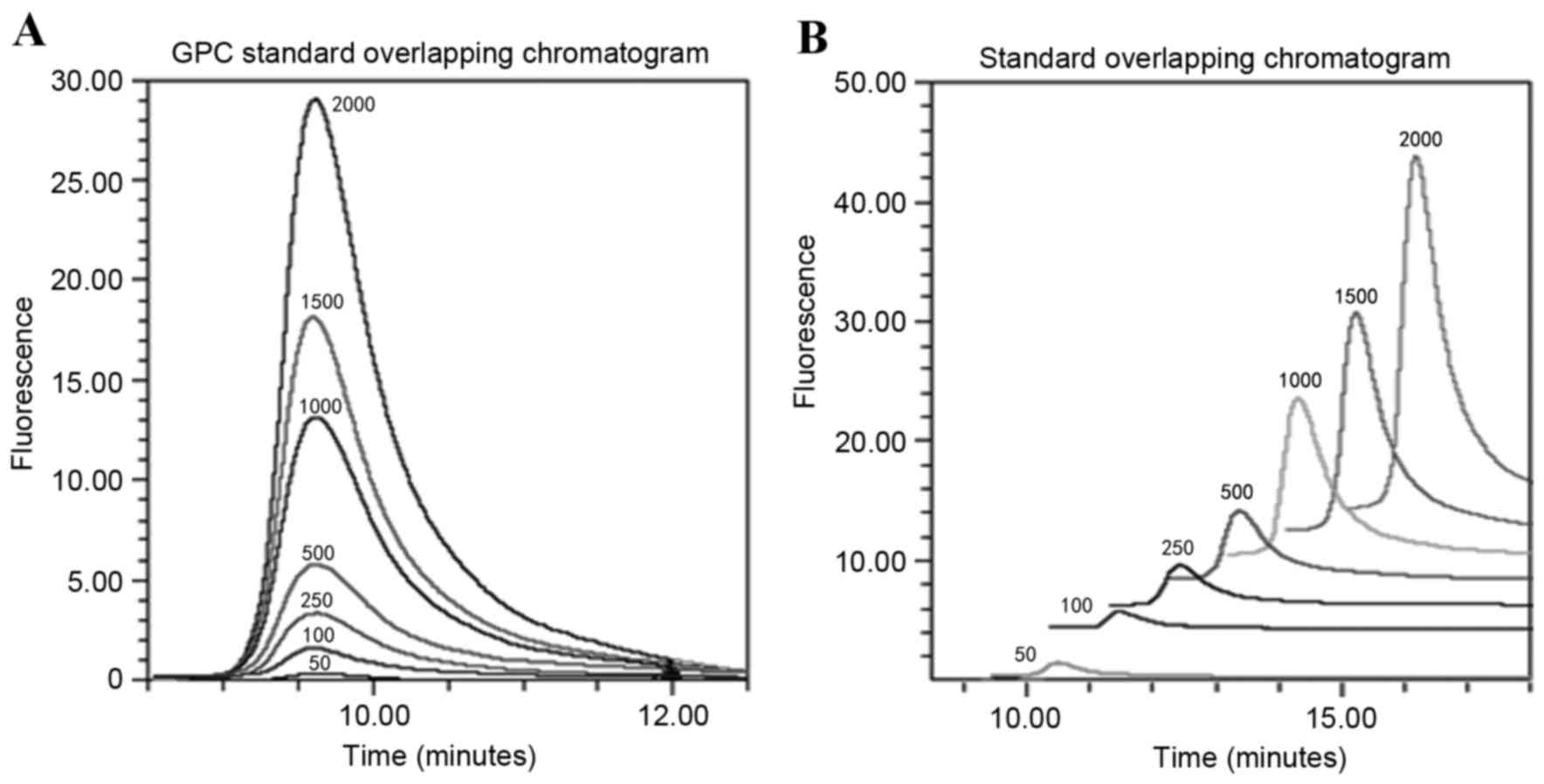
at 0, 0.25, 0.5, 1, 2, 4 and 6 h post-injection, respectively. MDZ
standard solutions were prepared at concentrations of 25, 50, 100,
200, 400, 800 and 1,600 ng-ml. Chromatography was performed via
Waters 2695 high performance liquid chromatography (HPLC; Waters
2487 UV-VIS detector; Waters Corporation, Milford, MA, USA) on a
C18 chromatographic column (250×4.6 mm; 5 µm) maintained at a flow
rate of 0.6 ml-min. The mobile phase consisted of methanol,
acetonitrile and potassium phosphate buffer solution (0.02 mol-l;
pH7.4) at a ratio of 65:25:10 (v-v), and a 0.45 µm filter membrane
was used. The wavelength detection was 221 nm and a quantity of 50
µl was added. CYP3A activity was denoted as MDZ clearance (CL) and
area under the curve (AUC) (0-t).
HPLC determination of concentrations
of DNR and associated metabolized products
A 1 ml sample of blood was collected 15 min, 30 min,
and 1, 2, 3, 4, 6, 12 and 24 h following injection, respectively,
and stored in tubes with EDTA. The tubes were centrifuged at 4°C
for 10 min at 800 x g, and the upper plasma was collected
and stored at −80°C. An appropriate standard of DNR was weighed and
then dissolved in methanol solution (2 mg-ml). Following
extraction, blood specimens were added to 200 µl mobile phase,
followed by mixing for 10 sec. The chromatogram conditions were as
follows: C18 chromatographic column (5 µm; 250×4.6 mm; Fuji Silysia
Chemical Ltd., Tokyo, Japan); mobile phase, 0.4% ammonium acetate
solution:acetonitrile at 65:35 ratio (v-v); pH=4.0; temperature,
40.0°C; flow rate, 1.0 ml-min; volume of sample, 50 µl.
Additionally, the fluorescence detector had a 480 nm excitation
wavelength and 560 nm emission wavelength. Following appearance,
the AUC was calculated. A standard curve was drawn according to the
DNR concentration with abscissa and peak area as coordinates.
Finally, the DNR concentration was calculated through the peak area
and using the standard curve formula (Y=481.91, X=985.01; R=0.995;
with Y being the peak area and X the DNR concentration).
Monitoring heart function
According to the standard of acute and subacute
toxicity reaction of anticancer drugs (12), echocardiography (ECG), myocardial
enzymes and cardiac troponin were monitored at different
chemotherapeutic stages in the children with ALL. The DNR
accumulated dose and adverse cardiac reactions were observed
through follow-up.
Statistical analysis
All statistical analysis was performed using SPSS
19.0. (IBM SPSS, Armonk, NY, USA). One-way analysis of variance was
used to compare the difference between two groups. A Games-Howell
test was used for multiple comparisons. DAS software (version
2.1.1; Mathematical Pharmacology Professional Committee of China,
Shanghai, China) was used to calculate the pharmacokinetic
parameters of MDZ and DNR.
Results
General data
A total of 36 children with ALL were recruited in
the present study, including 22 boys and 14 girls with an average
age of 7.1±2.3 years (range, 3–14 years old).
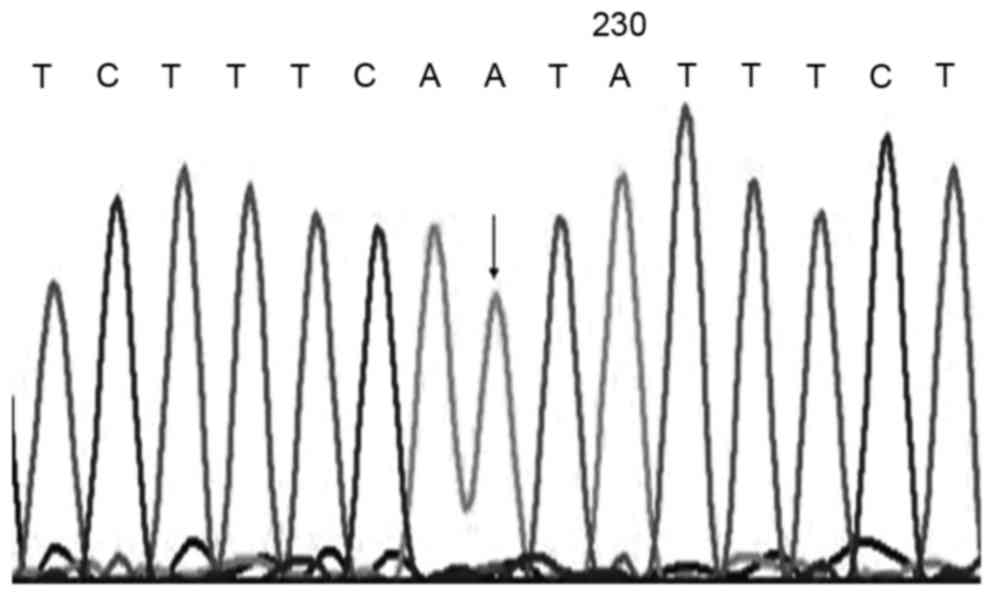
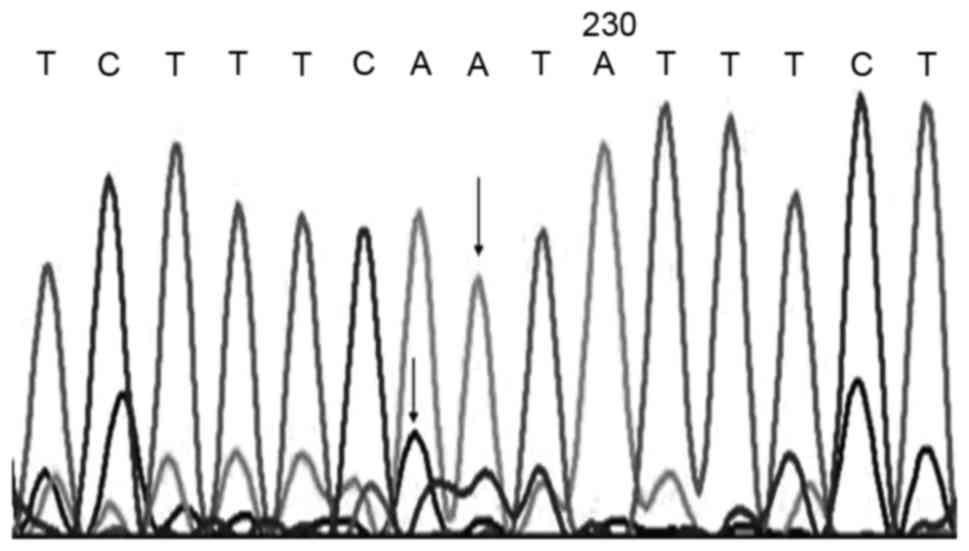
Distribution of CYP3A5 genotypes
In the ALL cases, 22 cases were CYP3A5*3-*3, 10
cases were CYP3A5*1-*3 and four cases were CYP3A5*1-*1. Sequence
analysis was performed on the three genotypes in the site of 6,986,
and the results indicated that the CYP3A5*3-*3 genotype had only
one peak of G, CYP3A5*1-*1 also had one peak of A, however, two
peaks of A and G were detected in the CYP3A5*1-*3 genotype
(Figs. 1–3).
Gene expression of CYP3A5
The CYP3A5*1-*1 genotype had wt-mRNA (wt-CYP3A5),
whereas the CYP3A5*1-*3 and CYP3A5*3-*3 genotypes had two types of
mRNA (wt-CYP3A5 and SV1-CYP3A). The wt-mRNA in the different
genotypes showed statistical significance (Table II).
| Table II.mRNA expression levels of CYP3A5 in
patients with acute leukemia with different genotypes. |
Table II.
mRNA expression levels of CYP3A5 in
patients with acute leukemia with different genotypes.
| Genotype | n (%) | Expression of
wt-CYP3A5 | P-value |
|---|
| CYP3A5*3-*3 | 22 (61.1) | 0.73±1.29 | 0.032a |
| CYP3A5*1-*3 | 10 (27.8) | 6.12±2.23 | 0.014b |
| CYP3A5*1-*1 | 4
(11.1) | 21.36±12.57 | 0.042c |
Detection of CYP3A enzyme activity and
DNR concentration
The CL of MDZ ranged between 0.047 and 0.181, and
the AUC (0–6 h) ranged between 390.124 and 1637.427 in the 36
cases. The plasma chromatogram of DNR showed no disturbed peaks
prior to or following DNR, and the storage duration was 9.618 min,
which suggested that the DNR identification was distinct and that
the spots were clear (Fig. 4).
The DNR was gradually reduced in the blood as a two
compartment model, and the results of pharmacokinetic parameters
were as follows: Half-life (t1–2)α, 0.02–1.25 h;
t1–2β, 3.56–112.72 h; CL, 14.72–136.69
l·h−1·m−2; AUC0–24 h,
116.73–832.01 µg/l−1·h; maximum concentration
(Cmax), 6.85–127.76 µg/l−1, time to maximum
concentration (tmax), 0.35–1.80 h. These results showed
that the DNR parameters were different between individuals; the
maximum CL was nine times higher than the minimum, the maximum AUC
was seven times higher than the minimum, and the maximum
Cmax was four times higher than the minimum.
The children with ALL were divided into three
groups, and the pharmacokinetic parameters were analyzed for all
cases. The AUC0–24 h and AUC0-∞ were
significantly different among the groups, however, no statistically
significant differences were observed in
t1–2orCmax (Table III).
| Table III.Pharmacokinetics of patients with
different genotypes of cytochrome P450 family 3 subfamily A member
5 followinginjection of daunorubicin. |
Table III.
Pharmacokinetics of patients with
different genotypes of cytochrome P450 family 3 subfamily A member
5 followinginjection of daunorubicin.
| Parameter | 6986GG (n=22) | 6986AG (n=10) | 6986AA (n=4) |
|---|
| t1–2α
(h) |
0.59±0.14 |
0.43±0.29 |
0.38±0.11 |
| Vd
(l·m−2) | 319.27±120.11 | 263.91±256.49 | 157.04±92.38 |
| CL
(l·h·m−2) |
70.02±24.63 |
79.81±29.14 |
82.14±22.57 |
|
AUC0–24h(µg·l-1·h) |
465.61±231.05a | 430.16±221.62 | 305.16±241.62 |
| AUC0-∞
(µg·l-1·h) |
586.10±382.15a | 503.10±282.24 | 452.30±210.71 |
| Tmax
(h) |
1.51±0.17 |
1.37±0.25 |
1.12±0.48 |
| Cmax
(µg·l−1) |
89.01±33.52 |
74.66±33.52 |
65.64±29.67 |
Adverse reactions of DNR
Heart ultrasonography and monitoring of cardiac
troponin were normal prior to and following chemotherapy in the 36
children. Of these, four children had cardiac dysfunction; three
children suffered from an aberrant increase in the myocardial
enzyme spectrum, including a lactate dehydrogenase range of
528.1–879.6 U/l, an α-hydroxybutyrate dehydrogenase range of
498.2–769.3 U/l and an aspartate aminotransferase range of
118.2–186.7 U/l. In addition, one child with an abnormal ECG was
treated with DNR for 5 months, which was followed by right bundle
branch block. A year later, the child succumbed to mortality from
acute myocarditis.
Discussion
In previous years, there has been substantial
development in understanding the chemotherapeutics mechanisms of
pharmacogenetics and pharmacogenomics (13–15).
The cytotoxic effect of chemotherapeutics against tumor cells has
significant associations with the expression of specific genes or
gene polymorphisms. The detection of associated genes to predict
effects in order to select appropriate drugs for individualized
chemotherapy has become a rationale for improving effects and
reducing the occurrence of ineffective treatment.
DNR is an anthracycline anticancer drug used to
treat common acute leukemia. The effect and toxicity of DNR is
correlated with blood-concentrations and duration of action,
however, there are certain differences among individuals. Studies
have confirmed that the CYP3A5 enzyme is involved in the metabolism
and clearance of DNR, however, the activity of CYP3A5 is affected
by gene polymorphisms, which present with individual differences
(16). Thus, the present study
aimed to investigate the gene expression of CYP3A5, its enzyme
activity and DNR concentrations, in order to provide experimental
evidence for the use of DNR and reducingthe cardiac toxicity caused
by DNR.
The present study identified three genotypes,
CYP3A5*1-*1, CYP3A5*1-*3 and CYP3A5*3-*3, in 36 children with ALL.
PCR analysis was used to detect the mRNA expression of CYP3A5,
which detected only a wt-mRNA (wt-CYP3A5) in the CYP3A5*1-*1
genotype, but identified two types of mRNA, wt and variant type
(SV1-CYP3A5) in the CYP3A5*1-*3 and CYP3A5*3-*3 genotypes. The
metabolized clearance rate of MDZ ranged between 0.047 and 0.181
l-h-kg in the 36 children with leukemia. CYP3A enzyme activity
combined with CYP3A5 genotype were analyzed, which revealed that
CYP3A enzyme activity was higher in children with the CYP3A5*1
allele, compared with that in children with CYP3A5*3. Kuehl et
al (17) indicated that the
hydroxylation reaction rate to MDZ of individuals with a single
CYP3A5*1 allele was at least twice as high as individuals with the
CYP3A5*3-*3 allele. Seng et al (18) found the CYP3A activity was higher
in children with the CYP3A5*1 allele, compared with that in
children with the CYP3A*3 allele, which was in accordance with the
results of the present study.
In the present study, the monitoring of DNR blood
concentrations was performed for 24 h in the 36 children with ALL
on their initial visit to hospital using RHPLC. The results showed
that the pharmacokinetics of DNR were significantly different in
the 36 individuals, the difference in CL was over three times
higher, and the AUC was four times higher in certain individuals.
Kokenberg et al (19)
investigated the pharmacokinetics of DNR in 21 patients with acute
myeloid leukemia and found the AUC ranged between 0.06 and 0.37
nmol-m*h between individuals. Bogason et al (20) also found the blood concentrations
of DNR varied markedly in individuals 1 h following injection of
DNR in 40 cases of acute myeloid leukemia, which ranged between 60
and 1,370 nM. The factors affecting the pharmacokinetics of DNR
include heritage, age, pathology and environment, and hereditary
factors determine the effect and toxicity of drugs (21). In the present study, correlation
analysis between the mRNA expression of wt-CYP3A5 and metabolized
clearance of DNR was performed in 36 children with ALL, and it was
found that there was correlation between the two factors. The
increase in the expression level of wt-mRNA led to an increase in
metabolized drug clearance (r=0.769). Therefore, the detection of
CYP3A5 genotype and phenotype are necessary for children with
primary ALL prior to chemotherapy using DNR, in order to predict
the metabolized clearance of DNR in the body, and to enhance the
scientific value and rationality of DNR use.
The present study found that the AUC was markedly
higher in four children with ALL with cardiac toxicity, compared
with those without cardiac toxicity, which indicated that the DNR
had high bioavailability, increasing the risk of cardiac toxicity.
Therefore, the timely use of cardiac protectors is required, or a
reduction in DNR dose is recommended. No reduction in the activity
of CYP3A was observed in these four children, compared with
children without cardiac toxicity. The detection of DNR
pharmacokinetics required the collection of blood samples several
times, which introduced difficulty in specimen collection. It is
suggested that CYP3A activity is included in routine examinations
prior to chemotherapy with DNR to predict the occurrence of cardiac
toxicity following treatment with DNR.
In the process of treating leukemia, the detection
of CYP3A5 gene polymorphisms and CYP3A enzyme activity, and
monitoring the blood concentrations of anticancer drugs may provide
objective indicators for individualized treatment and references
for planning effective blood drug concentration rages to assist
establishing individual treatment schemes.
In the present study, relatively few cases were
enrolled and the observation duration was short. In addition,
certain children may suffer from toxicity reactions as time
progresses. Therefore, to confirm the association between efficacy
and DNR pharmacokinetics, a larger sample size and longer
observation period is required.
Acknowledgements
The present study was supported by a grant from the
Wenzhou City Science Plan (grant no. Y20160228).
References
|
1
|
Carvalho C, Santos RX, Cardoso S, Correia
S, Oliveira PJ, Santos MS and Moreira PI: Doxorubicin: The good,
the bad and the ugly effect. Curr Med Chem. 16:3267–3285. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Singal PK and Iliskovic N:
Doxorubicin-induced cardiomyopathy. N Engl J Med. 339:900–905.
1998. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Wang Y, Zheng D, Wei M, Ma J, Yu Y, Chen
R, Lacefield JC, Xu H and Peng T: Over-expression of calpastatin
aggravates cardiotoxicity induced by doxorubicin. Cardiovasc Res.
98:381–390. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ohtake S, Miyawaki S, Fujita H, Kiyoi H,
Shinagawa K, Usui N, Okumura H, Miyamura K, Nakaseko C, Miyazaki Y,
et al: Randomized study of induction therapy comparing
standard-dose idarubicin with high-dose daunorubicin in adult
patients with previously untreated acute myeloid leukemia: The
JALSG AML201 study. Blood. 117:2358–2365. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Goh BC, Lee SC, Wang LZ, Fan L, Guo JY,
Lamba J, Schuetz E, Lim R, Lim HL, Ong AB and Lee HS: Explaining
interindividual variability of docetaxel pharmacokinetics and
pharmacodynamics in Asians through phenotyping and genotyping
strategies. J Clin Oncol. 20:3683–3690. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ro H, Min SI, Yang J, Moon KC, Kim YS, Kim
SJ, Ahn C and Ha J: Impact of tacrolimus intraindividual
variability and CYP3A5 genetic polymorphism on acute rejection in
kidney transplantation. Ther Drug Monit. 34:680–685. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kim KP, Ahn JH, Kim SB, Jung KH, Yoon DH,
Lee JS and Ahn SH: Prospective evaluation of the drug-metabolizing
enzyme polymorphisms and toxicity profile of docetaxel in Korean
patients with operable lymph node-positive breast cancer receiving
adjuvant chemotherapy. Cancer Chemother Pharmacol. 69:1221–1227.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Afsar NA, Ufer M, Haenisch S, Remmler C,
Mateen A, Usman A, Ahmed KZ, Ahmad HR and Cascorbi I: Relationship
of drug metabolizing enzyme genotype to plasma levels as well as
myelotoxicity of cyclophosphamide in breast cancer patients. Eur J
Clin Pharmacol. 68:389–395. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lopes BA, Emerenciano M, Gonçalves BA,
Vieira TM, Rossini A and Pombo-de-Oliveira MS: Polymorphisms in
CYP1B1, CYP3A5, GSTT1, and SULT1A1 are associated with early age
acute leukemia. PLoS One. 10:e01273082015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ma LM, Liu HC, Ruan LH and Feng YM:
CYP3A5*3 genetic polymorphism is associated with childhood acute
lymphoblastic leukemia risk: A meta-analysis. Biomed J. 38:428–432.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Liu X, Zou Y, Wang H, Chen X, Ruan M, Chen
Y, Yang W, Guo Y, Liu T, Zhang L, et al: Treatment outcome of
childhood standard-risk and median-risk acute lymphoblastic
leukemia with CCLG-2008 protocol. Zhonghua Er Ke Za Zhi.
52:449–454. 2014.(In Chinese). PubMed/NCBI
|
|
12
|
Florescu M, Cinteza M and Vinereanu D:
Chemotherapy-induced cardiotoxicity. Maedica (Buchar). 8:59–67.
2013.PubMed/NCBI
|
|
13
|
Stankov K, Sabo A and Mikov M:
Pharmacogenetic biomarkers as tools for pharmacoepidemiology of
severe adverse drug reactions. Drug Dev Res. 74:1–14. 2013.
View Article : Google Scholar
|
|
14
|
Francis J, Dubashi B, Sundaram R, Pradhan
SC and Chandrasekaran A: A study to explore the correlation of
ABCB1, ABCG2, OCT1 genetic polymorphisms and trough level
concentration with imatinib mesylate-induced thrombocytopenia in
chronic myeloid leukemia patients. Cancer Chemother Pharmacol.
76:1185–1189. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Hareedy MS, El Desoky ES, Woillard JB,
Thabet RH, Ali AM, Marquet P and Picard N: Genetic variants in
6-mercaptopurine pathway as potential factors of hematological
toxicity in acute lymphoblastic leukemia patients.
Pharmacogenomics. 16:1119–1134. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Fetterly GJ, Aras U, Lal D, Murphy M,
Meholick PD and Wang ES: Development of a preclinical PK-PD model
to assess antitumor response of a sequential aflibercept and
doxorubicin-dosing strategy in acute myeloid leukemia. AAPS J.
15:662–673. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kuehl P, Zhang J, Lin Y, Lamba J, Assem M,
Schuetz J, Watkins PB, Daly A, Wrighton SA, Hall SD, et al:
Sequence diversity in CYP3A promoters and characterization of the
genetic basis of polymorphic CYP3A5 expression. Nat Genet.
27:383–391. 2001. View
Article : Google Scholar : PubMed/NCBI
|
|
18
|
Seng KY, Hee KH, Soon GH, Sapari NS, Soong
R, Goh BC and Lee LS: CYP3A5*3 and bilirubin predict midazolam
population pharmacokinetics in Asian cancer patients. J Clin
Pharmacol. 54:215–224. 2014. View
Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kokenberg E, Sonneveld P, Delwel R, Sizoo
W, Hagenbeek A and Löwenberg B: In vivo uptake of daunorubicin by
acute myeloid leukemia (AML) cells measured by flow cytometry.
Leukemia. 2:511–517. 1988.PubMed/NCBI
|
|
20
|
Bogason A, Quartino AL, Lafolie P,
Masquelier M, Karlsson MO, Paul C, Gruber A and Vitols S: Inverse
relationship between leukaemic cell burden and plasma
concentrations of daunorubicin in patients with acute myeloid
leukaemia. Br J Clin Pharmacol. 71:514–521. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Chien JY and Ho RJ: Drug delivery trends
in clinical trials and translational medicine: Evaluation of
pharmacokinetic properties in special populations. J Pharm Sci.
100:53–58. 2011. View Article : Google Scholar : PubMed/NCBI
|