Introduction
Although in vitro fertilization (IVF) is a
safe and common treatment approach for infertility, there still
remain some undesired side effects. As a serious iatrogenic
complication, ovarian hyperstimulation syndrome (OHSS) is
encountered during controlled ovarian stimulation (COS).
Classification of OHSS is based on laboratory findings and clinical
characteristics. The mild forms of OHSS are common, occurring in up
to 30% of all IVF cycles, while the incidence of moderate and
severe forms was 3–6% and 0.2–1% of IVF cycles, respectively
(1,2). As the most severe complication of
COS, OHSS is characterized by a dramatic ovarian enlargement and an
acute shift of intravascular fluid, which is caused by increased
vascular permeability and ovarian neoangiogenesis (3). Severe forms can cause thrombus
formation (4), and can even become
life threatening. However, despite many years of clinical
experience, the pathogenesis of OHSS remains ambiguous.
Risk factors that relate to the development of OHSS
include young age, low body weight, PCOS, previous episodes of
OHSS, multiple pregnancy, rapidly rising estradiol (E2) levels and
follicle number (>20–25) (5–7).
Serum levels of vascular endothelial growth factor (VEGF) in
follicular fluid, pleural effusion and ascites are higher in OHSS
patients compared with healthy people (8). VEGF may serve as an inflammatory
factor to increase vascular permeability and neovascularization,
which may explain the clinical symptoms of OHSS. Ingman and
Robertson (9) suggested that human
chorionic gonadotropin (hCG) participates in OHSS by activating the
renin-angiotensin system (RAS). The ovarian RAS is involved in
regulating endothelial proliferation, vascular permeability,
angiogenesis and prostaglandin release (10). The increase of renin, angiotensin
II and angiotensin-converting enzyme also lead to pathological
changes in OHSS patients. The roles of genetic predisposition,
luteinizing hormone (LH), inflammatory mediators and follicle
stimulating hormone (FSH) variability are already discussed in the
pathophysiology of OHSS (1–3,11).
However, there is still a lack of an effective approach for the
prevention and treatment of OHSS as the pathogenesis has not yet
been fully elucidated.
Prevention is often better than cure. However, using
only body mass index (BMI) and age to predict OHSS prior to COH
remains an arduous task in an individual IVF cycle. Monitoring the
serum E2 level and antral follicle count (AFC) are conventional
means for OHSS prevention (11).
Serum hormonal markers, such as anti-müllerian hormone (AMH) are
increasingly being applied to predict ovarian response to
stimulation (12). However, these
diagnosis indices cannot accurately predict OHSS prior to starting
COH, a better alternative for early diagnosis is needed. Now,
proteomics have been widely used to discover biomarkers for various
diseases. Markel et al (13) reported that CEACAM1 and MICA could
serve as novel serum biomarkers in patients with acute and
recurrent pericarditis. Xu et al (14) demonstrated that the candidate serum
biomarkers (S100A9, SOD3 and MMP9) performed high sensitivity and
specificity in discriminating pulmonary tuberculosis. These
findings indicate that serum protein biomarkers serve an important
role in the prediction and diagnosis of diseases. Therefore, the
authors hypothesize that serum proteins may serve as effective
biomarkers for OHSS prediction. Thus, there is a need for a
comprehensive analysis on OHSS patient's serum proteins for
predicting and preventing OHSS.
As a proven well-known factor of OHSS in all
populations, PCOS is a common endocrine disorder syndrome that
leads to infertility in child-bearing age women, with a prevalence
of 5–10% (15). In the present
study, the authors compared the expression profiles of serum
protein in OHSS patients and non-OHSS patients with PCOS through
iTRAQ-coupled liquid chromatography-mass spectrometry (LC-MS)
before COH was initiated, in order to reveal the potential markers.
Three candidate protein biomarkers (haptoglobin, lipoprotein lipase
and fibrinogen) were validated by ELISA and western blotting.
Further receiver operating characteristic (ROC) curves analysis of
these biomarkers presented sufficient predictive values for
clinical applications. The potential implications of clinical
symptoms for OHSS precaution were also discussed.
Materials and methods
Study design and population
The authors conducted the present study in the
Nanjing Maternity and Child Health Care Hospital (Nanjing, China).
The research was approved by the Human Research Ethics Committee of
Nanjing Medical University (Nanjing, China) and informed consent
was provided by each participant prior to research. A total of 88
patients who suffered from PCOS and were undergoing IVF treatment
were recruited. The diagnosis of PCOS was in accordance with the
Rotterdam criteria revised in 2003; the patient should suffer with
at least two of the three indicators: (A) Menstruation or
non-ovulation; (B) clinical and/or biochemical display
hyperandrogenism; (C) ultrasound examination presented polycystic
ovaries, and exclusion of other diseases, such as adrenal
hyperplasia, Cushing's syndrome, androgen-secreting tumors and
hyperprolactinemia. Diane-35 had been used in all the patients who
have PCOS to let the serum testosterone levels decrease to normal.
Blood samples were obtained prior to gonadotropin injection and
were centrifuged at 1,000 × g at 4°C for 10 min to obtain the sera
and then stored at −80°C for further use.
Patients involved in the present study were divided
into two groups according to the results of COH: Women who develop
moderate or severe OHSS were selected as the ‘OHSS group’ and
others without OHSS or with mild OHSS were assigned to the ‘control
group’. Firstly, the mixed serum of ten women from each group to
identified the altered proteins through analysis by LC-MS/MS. The
authors revealed the expression levels of serum proteins and
selected significantly different expression proteins in the OHSS
group for further analysis. Next, the screened proteins were
validated in the other samples by ELISA and western blotting.
Classification of OHSS
The classification of OHSS was defined by Golan and
Weissman (16). The following
features were classified as moderate OHSS: Stomach pains and
discomfort, abdominal distension, nausea, ascites and the size of
ovary (8–12 cm). Severe OHSS were characterized by massive ascites,
hydrothorax, 45% hematocrit edema/anasarca, liver dysfunction, and
white blood cell count >15,000.
Protein preparation and LC-MS/MS
analysis
The depletion of abundant serum proteins was carried
out using ProteoMiner Protein Enrichment kit (Bio-Rad Laboratories,
Inc., Hercules, CA, USA), so as to identify more low abundance
proteins, according to the manufacturer's protocol. Then, 100 µg
total protein from each mixed sample was taken out and incubated
with Trypsin Gold (Promega Corporation, Madison, WI, USA). Next,
the peptides were labeled with the iTRAQ reagents (Applied
Biosystems; Thermo Fisher Scientific, Inc., Waltham, MA, USA).
Strong cation exchange (SCX) chromatography was conducted by a
high-performance liquid chromatography pump system LC-20AB
(Shimadzu, Kyoto, Japan). The iTRAQ-labeled peptide mixtures were
dissolved and then loaded onto a Ultremex SCX column (Phenomenex,
Torrance, CA, USA; 4.6×250 mm). The fractions collected from SCX
chromatography were performed MS/MS analysis.
Validation by ELISA and western
blotting
Fold changes of candidate biomarkers were further
validated by ELISA and western blotting techniques. A total of 68
serum samples were screened, including 38 OHSS women and 30
controls. ELISA quantifications for haptoglobin, fibrinogen and
lipoprotein lipase (Abcam, Cambridge, MA, USA) were performed
according to the manufacturers' instructions of commercial ELISA
kits. For western blotting, 30 µg serum proteins were
electrophoretically separated on a 10–12% SDS-PAGE gel and then
transferred to polyvinylidene difluoride membranes (EMD Millipore,
Billerica, MA, USA). Following blocking with 5% skimmed milk,
membranes were incubated with the primary antibodies at the
indicated dilutions: anti-haptoglobin (1:10,000; cat no. ab13429;
Abcam), anti-fibrinogen (1:10,000; cat no. ab119948; Abcam) and
anti-lipoprotein lipase (1:1,000; cat no. ab21356; Abcam) at 4°C
overnight. The blots were then washed with TBS containing 0.05%
Tween-20 and incubated with horseradish peroxidase (HRP)-conjugated
secondary antibody (1:10,000; cat no. 31439; Thermo Fisher
Scientific, Inc.) at room temperature for 2 h. Immunopositive bands
were visualized using Luminata Western HRP Substrates (EMD
Millipore) and densitometry of the bands were estimated by
FluorChem M system (ProteinSimple, San Jose, CA, USA).
Data and bioinformatics analysis
Protein identification and quantification were
performed by using the Mascot search engine (Matrix Science, Ltd.,
London, UK). These proteins with a fold changes of >1.2 or
<0.83 (OHSS vs. control) were considered as significant
(P<0.05). Functional annotations of the proteins were conducted
using Gene Ontology (GO) database (http://geneontology.org/), which can describe cellular
component, molecular function and biological process, respectively.
The Cluster of Orthologous Groups (COGs) database (http://www.ncbi.nlm.nih.gov/COG/) was used to
group and classify all the proteins identified in both groups.
Every protein in COG is supposed to derive from the same protein
ancestor.
Statistical analysis
All statistical analyses of this study were
performed using SPSS software (version 20.0.0; IBM SPSS, Armonk,
NY, USA). Data were presented as mean ± standard deviation.
Inter-group differences in the clinical characteristics and
experimental data were estimated by the Student's t-test and
P<0.05 was considered to indicate a statistically significant
difference. ROC curves were generated to evaluate the diagnostic
value of candidate biomarkers.
Results
Characteristics of the study
population
A total of 88 PCOS patients were enrolled in our
study and 40 had confirmed OHSS, their characteristics were
summarized in Table I. As
indicated, there was no difference between the two groups on age,
basal E2, basal testosterone, basal FSH, fasting insulin, duration
of infertility and gonadotropin dose (P>0.05). The values of
basal LH, basal LH/FSH, number of oocytes and number of good
embryos were significantly higher in the OHSS group than in the
control group (P<0.05), whereas the values of BMI and estradiol
on the hCG day were significantly lower in the OHSS group than in
the control group (P<0.05).
 | Table I.Comparison of clinical characteristics
between patients with OHSS and without OHSS. |
Table I.
Comparison of clinical characteristics
between patients with OHSS and without OHSS.
|
| OHSS (n=40) | Control (n=48) | P-value |
|---|
| Age (years) | 28.1±3.8 | 28.5±3.2 | NS |
| Body mass index
(kg/m2) | 21.3±2.6 | 24.3±3.7 | <0.001 |
| Fasting insulin
(mU/l) | 14.7±2.5 | 13.8±3.6 | NS |
| Infertility
duration (years) | 3.5±2.5 | 3.7±2.1 | NS |
| Basal serum FSH
(U/l) | 6.1±1.8 | 6.4±1.7 | NS |
| Basal serum LH
(U/l) | 7.7±3.9 | 5.3±2.4 | <0.01 |
| Basal LH/FSH
(L) | 1.2±0.5 | 0.81±0.32 | <0.01 |
| Basal serum E2
(U/l) | 43.5±18.1 | 42.3±25.7 | NS |
| Basal serum T
(ng/ml) | 0.53±0.14 | 0.49±0.17 | NS |
| Dose of
gonadotrophins (U) | 1423.5±342.3 | 1617.3±456.1 | NS |
| Oestradiol on day
of HCG (pg/ml) | 10278.3±2654.2 | 3324.4±953.4 | <0.001 |
| No. of oocytes | 17.9±2.4 | 7.8±2.5 | <0.001 |
| No. of good
embryos | 10.7±7.9 | 4.5±2.6 | <0.001 |
Identification of differentially
expressed serum proteins in women with OHSS
To identify potential biomarkers of OHSS, 20 serum
samples from OHSS and control groups were divided into four main
groups with five samples from each group. The mixtures were
employed using iTRAQ combined with LC-MS/MS technologies. A total
of 418 unique proteins were identified by MS in both groups. A
total of 57 significant different proteins were screened in OHSS
serum samples, compared with the control group, of which 28
proteins were overexpressed (>1.2-fold) and 29 proteins were
underexpressed (<0.83-fold; Fig.
1). The full list of differentially expressed proteins can be
identified in Table II.
| Table II.List of proteins with significant
difference in levels between OHSS and control groups. |
Table II.
List of proteins with significant
difference in levels between OHSS and control groups.
| Accession no. | Protein name | MW (kDa) | Ratio
(OHSS/control) |
|---|
| P30043 | Flavin
reductase | 25,262 | 2.46 |
| P49060 | Lipoprotein
lipase | 63,225 | 2.31 |
| P78371 | T-complex protein 1
subunit beta | 69,354 | 1.92 |
| P0DJI8 | Serum amyloid A-1
protein | 15,436 | 1.87 |
| P08603 | Complement factor
H | 168,175 | 1.84 |
| P02675 | Fibrinogen beta
chain | 48,076 | 1.71 |
| Q16610 | Extracellular
matrix protein 1 | 20,792 | 1.60 |
| P06732 | Creatine kinase
M-type | 54,181 | 1.53 |
| P01788 | Ig heavy chain V
region H8 | 13,100 | 1.53 |
| P02679 | Fibrinogen gamma
chain | 63,883 | 1.53 |
| P67936 | Tropomyosin alpha-4
chain | 33,316 | 1.52 |
| P68872 | Hemoglobin subunit
beta | 14,272 | 1.52 |
| Q9UBX5 | Fibulin-5 | 19,441 | 1.50 |
| P02671 | Fibrinogen alpha
chain | 109,041 | 1.48 |
| Q13790 | Apolipoprotein
F | 39,039 | 1.42 |
| Q08380 | Galectin-3-binding
protein | 72,286 | 1.40 |
| P04114 | Apolipoprotein
B-100 | 222,441 | 1.38 |
| P04206 | Ig kappa chain
V–III region GOL | 13,154 | 1.37 |
| P01599 | Ig kappa chain V–I
region Gal | 11,818 | 1.35 |
| P0CG05 | Ig lambda-2 chain C
regions | 27,347 | 1.35 |
| P01743 | Ig heavy chain V–I
region HG3 | 19,786 | 1.34 |
| Q9HDC9 | Adipocyte plasma
membrane-associated protein | 50,834 | 1.34 |
| P23381 | Tryptophan-tRNA
ligase, cytoplasmic | 64,425 | 1.32 |
| P01591 | Immunoglobulin J
chain | 21,450 | 1.31 |
| Q9CWF2 | Tubulin beta-2B
chain | 46,571 | 1.31 |
| O60462 | Neuropilin-2 | 115,991 | 1.31 |
| P04431 | Ig kappa chain V–I
region Walker | 14,314 | 1.30 |
| Q9UHG3 | Prenylcysteine
oxidase 1 | 63,740 | 1.22 |
| P01042 | Kininogen-1 | 57,836 | 0.81 |
| P04264 | Keratin, type II
cyt | 75,006 | 0.81 |
| P43652 | Afamin | 86,781 | 0.80 |
| P01011 |
Alpha-1-antichymotrypsin | 59,285 | 0.79 |
| P06310 | Ig kappa chain V–II
region RPMI-6410 | 14,040 | 0.79 |
| P04217 |
Alpha-1B-glycoprotein | 58,440 | 0.78 |
| Q9NZP8 | Complement C1r
subcomponent-like protein | 59,681 | 0.78 |
| P02774 | Vitamin D-binding
protein | 67,663 | 0.77 |
| P05543 | Thyroxine-binding
globulin | 55,459 | 0.77 |
| P00740 | Coagulation factor
IX | 61,901 | 0.77 |
| Q13275 | Semaphorin-3F | 86,066 | 0.76 |
| Q96IY4 | Carboxypeptidase
B2 | 51,257 | 0.75 |
| P26927 | Hepatocyte growth
factor-like protein | 91,508 | 0.73 |
| P0C0L5 | Complement
C4-B | 43,077 | 0.71 |
| P10643 | Complement
component C7 | 111,446 | 0.71 |
| P07996 |
Thrombospondin-1 | 150,327 | 0.70 |
| Q6Q759 | Sperm-associated
antigen 17 | 150,152 | 0.70 |
| P25311 |
Zinc-alpha-2-glycoprotein | 40,854 | 0.70 |
| P08571 | Monocyte
differentiation antigen CD14 | 43,702 | 0.70 |
| P06396 | Gelsolin | 96,753 | 0.69 |
| Q5R767 | SPARC | 43,328 | 0.68 |
| P00751 | Complement factor
B | 168,440 | 0.68 |
| P36980 | Complement factor
H-related protein 2 | 34,920 | 0.68 |
| P02763 | Alpha-1-acid
glycoprotein 1 | 28,288 | 0.67 |
| P00352 | Retinal
dehydrogenase 1 | 56,272 | 0.59 |
| P02787 |
Serotransferrin | 97,259 | 0.58 |
| P02768 | Serum albumin | 89,874 | 0.55 |
| P00738 | Haptoglobin | 56,812 | 0.48 |
| P00325 | Alcohol
dehydrogenase 1B | 49,155 | 0.43 |
Functional classification of
identified proteins
The authors categorized these identified proteins
according to their biological functions using GO analysis. The
promising biological functions are presented in Fig. 2A-C. Cellular component analysis
demonstrated that these proteins were mainly enriched in membrane
(13.7%), organelle (19.1%) and extracellular regions (19.6%).
According to the analysis of molecular function, proteins were
categorized into groups of enzyme regulator activity (8.4%),
catalytic activity (25.0%) and binding (48.7%). The identified
proteins involved in diverse biological processes, such as
regulation of biological process (7.7%), response to stimulus
(7.9%), biological regulation (8.3%), metabolic process (9.0%),
cellular process (9.5%) and single-organism process (9.8%). COG
analysis indicated the participation of identified proteins in a
diverse number of biological processes, including posttranslational
modification, cytoskeleton, protein turnover chaperones, lipid
transport and metabolism (Fig.
2D).
Validation of candidate
biomarkers
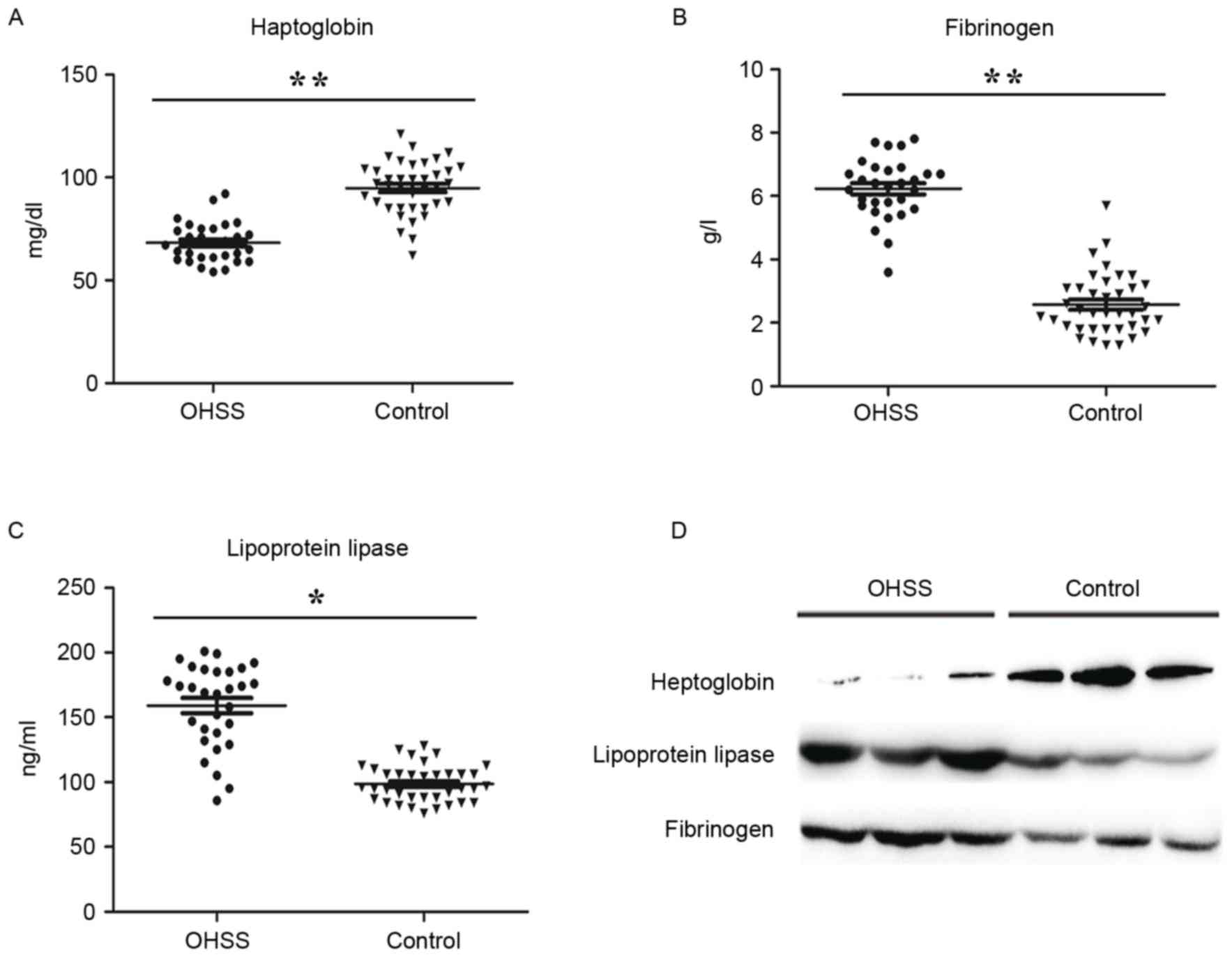
Based on bioinformatics analysis, the authors
selected three abnormally expressed proteins between two groups for
further study, haptoglobin, fibrinogen and lipoprotein lipase.
These three proteins involved in inflammatory responses, immune
responses and angiogenesis, which are the pathogenic basis of OHSS.
The ratios of haptoglobin, lipoprotein lipase and the fibrinogen
subunit (alpha chain, beta chain and gamma chain) were 0.48, 2.31,
1.48, 1.71 and 1.53, respectively, compared to the control group
(Table II). Verification of those
candidate biomarkers was performed by ELISA assay and western
blotting in a large and independent cohort. In accordance with the
result from MS analysis, haptoglobin was significantly
downregulated in OHSS patients, while lipoprotein lipase and
fibrinogen were upregulated, compared with the control group
(Fig. 3).
Prediction value of candidate
biomarkers for OHSS
ROC curve analysis revealed that the relative
expression level of haptoglobin, fibrinogen and lipoprotein lipase
in serum performed more accurately for OHSS prediction.
Specificity, sensitivity and the area under the curve (AUC) value
of haptoglobin were 0.875, 0.933, 0.913, respectively (Fig. 4A). When fibrinogen individually
served as a biomarker, specificity, sensitivity and AUC value was
0.811, 0.937 and 0.925, respectively (Fig. 4B). In addition, lipoprotein lipase
may discriminate OHSS from control patients; the specificity,
sensitivity and AUC value were 0.775, 0.907 and 0.882, respectively
(Fig. 4C). The combination of all
three proteins resulted in an AUC of 0.917, and the sensitivity and
specificity were 0.882 and 0.923, respectively (Fig. 4D). Furthermore, the authors
evaluated the discriminating effect of the basal LH/FSH ratio and
BMI for the prediction of OHSS, the AUC value of LH/FSH ratio and
BMI were 0.741 and 0.729 (Fig. 4E and
F). The sensitivity and specificity of the basal LH/FSH ratio
were 0.709 and 0.821, and BMI were 0.833 and 0.787, respectively
(Fig. 4E and F).
Discussion
As the most common endocrine disorder, PCOS is a
clear risk factor for OHSS in reproductive-age women. However, the
specific etiology of OHSS in PCOS patients is still poorly
understood, its accurate prediction in an individual IVF cycle is
difficult. OHSS often occurs in the absence of currently reported
risk factors, so a more effective early prevention measure is
needed. Comparative proteomic analysis has been widely used in
screening promising diagnosis biomarkers for diseases (17–19).
The present study attempted to screen candidate diagnostic serum
proteins in OHSS patients with PCOS. A total of 57 significantly
different proteins were identified and three significant different
proteins, including haptoglobin, fibrinogen and lipoprotein lipase
were validated by ELISA and western blotting. Finally, the
predictive value of these three candidate biomarkers was further
evaluated. To the best of the authors' knowledge, this is the first
expression pattern study of serum proteins in PCOS women with or
without severe OHSS.
Age, BMI, hormonal markers, as well as infertility
cause in general were considered as significant variables for OHSS
precaution (11). In the present
study, the authors observed no difference in age, estradiol,
testosterone, FSH and insulin in PCOS patients suffering from OHSS,
when compared to PCOS women without OHSS. A reverse correlation
between BMI and propensity for OHSS in PCOS patients was
identified, most of OHSS patients had BMI <24 and it is possible
that these patients are at greater risk to develop OHSS. This
difference may somewhat explain the high incidence of OHSS, since
it is more frequent in lean patients. Further analysis demonstrated
the AUC value of BMI was 0.729, the sensitivity and specificity
were 0.833 and 0.787, respectively. However, obese women have been
presented to be more prone to anovulation, and symptoms and PCOS
are aggravated by obesity (20).
Thus, a larger cohort study is required to assess BMI as a
predictor for OHSS in PCOS patients.
The LH/FSH ratio is another important baseline
parameter for predicting the risk of facing a high ovarian response
to COS (1,2). The authors observed a significantly
higher LH level and LH/FSH ratio in OHSS recruits compared to mean
serum levels of control patients in the present study. FSH and LH
serve different physiological roles within ovulation and are
required for follicular growth and estrogen secretion in the ovary
(21,22). The sensitivity and specificity of
LH/FSH ratio for prediction of OHSS were 0.709 and 0.821,
respectively. The AUC value of LH/FSH for OHSS was 0.741, which is
very close to the value of BMI (AUC=0.821) found in the current
study. Despite limited data on the role of hormonal in predicting
OHSS, these markers have being increasingly utilized in predicting
ovarian response to stimulation. AMH levels have been previously
evaluated (23,24) and the results obtained presented
much promise. A previous study demonstrated that AMH levels can
identify women at high risk of developing OHSS (sensitivity 90.5%,
specificity 81.3%), as a useful predictor of developing OHSS
(12).
The present work especially focused on the
bioinformatics analysis of identified proteins. 19.6% of these
proteins were from extracellular region of the cell, and 19.1% were
from organelles. These proteins were involved in many biological
processes, such as metabolic process, energy production and
conversion, as well as lipid transport and metabolism. As the most
common endocrine and metabolic disease in reproductive age
spectrum, PCOS frequently develop metabolic complications, such as
glucose intolerance, insulin resistance, hyperinsulinemia and
dyslipidemia (25,26). These abnormalities put PCOS
patients at high risk of cardiovascular disease, obesity and type 2
diabetes at a young age. Previous experimental evidence have
demonstrated the intimate connection between endocrine disrupting
chemicals and metabolic disturbances through impaired normal lipid
and glucose homeostasis (27,28).
Therefore, the authors speculate that metabolic disorders may be a
key risk factor of OHSS incidence in lean PCOS women.
Haptoglobin, fibrinogen and lipoprotein lipase were
chosen as candidate protein markers for the prediction of OHSS in
the study. It was observed that all these three proteins are
precise markers at discriminating OHSS. Haptoglobin is an
inflammatory factor, its functions include in antioxidant activity,
hemoglobin binding, acute-phase response, immune system process,
arterial restructuring and vascular disease (29). Inflammatory factors as key OHSS
risk factors may lead to the increase of vascular permeability,
angiogenesis, protein-rich fluid accumulates in peritoneum, pleura
and pericardial space (30).
Fibrinogen is an acute phase protein and the marker of coagulation
potential, which involves in blood coagulation, cell-matrix
adhesion, innate immune response, platelet activation and positive
regulation of exocytosis (31).
Moreover, it can be a hemostatic agent (32), which may explain the formation of
thrombosis in severe OHSS. A previous study had already revealed
that OHSS patients present an imbalance to homeostasis and this was
characterized by high levels of fibrinogen and inflammatory
factors, such as interleukin-6 and tumor necrosis factor-α
(33). The biological processes of
lipoprotein lipase include heparin binding, which associated with
patients who have a low BMI (34).
Above all, the three proteins that have been selected for the
present study have never been reported as a predictive marker of
OHSS in PCOS patients, and their potential roles in OHSS occurrence
deserve further studies.
In summary, the present study successfully
identified diagnostic biomarkers that may have a role in predicting
severe OHSS among PCOS patients. The proteins of haptoglobin,
fibrinogen and lipoprotein lipase presented higher sensitivity and
specificity in OHSS. The proteomic results reported in the current
study may help to gain deeper insights into the pathophysiology of
OHSS in PCOS patients. Future studies should assess the quality of
these three proteins as serum biomarkers of OHSS in PCOS patients
in a larger population.
Acknowledgements
The present work was supported by grants from
Science and Technology Development Foundation Item of Nanjing
Medical University (grant no. 2013NJMU141) and the Nanjing Medical
Science and Technique Development Foundation of Nanjing Department
of Health (grant no. YKK14131).
Glossary
Abbreviations
Abbreviations:
|
IVF
|
in vitro fertilization
|
|
OHSS
|
ovarian hyperstimulation syndrome
|
|
COS
|
controlled ovarian stimulation
|
|
PCOS
|
polycystic ovarian syndrome
|
|
E2
|
estradiol
|
|
RAS
|
renin-angiotensin system
|
|
LH
|
luteinizing hormone
|
|
FSH
|
follicle stimulating hormone
|
|
BMI
|
body mass index
|
|
AFC
|
antral follicle count
|
|
AMH
|
anti-müllerian hormone
|
|
ROC
|
receiver operating characteristic
|
|
GO
|
gene ontology
|
|
COG
|
clusters of orthologous groups of
proteins
|
|
T
|
testosterone
|
References
|
1
|
Smith V, Osianlis T and Vollenhoven B:
Prevention of ovarian hyperstimulation syndrome: A review. Obstet
Gynecol Int. 2015:5141592015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Nastri CO, Teixeira DM, Moroni RM, Leitão
VM and Martins WP: Ovarian hyperstimulation syndrome: Patho
physiology, staging, prediction and prevention. Ultrasound Obstet
Gynecol. 45:377–393. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kumar P, Sait SF, Sharma A and Kumar M:
Ovarian hyperstimulation syndrome. J Hum Reprod Sci. 4:70–75. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Sukul SP, Pekelharing JE, van Hooff MH,
van der Weiden RM and van Asten JC: Thrombosis in ovarian
hyperstimulation syndrome. Ned Tijdschr Geneeskd. 158:A71082014.(In
Dutch). PubMed/NCBI
|
|
5
|
Halupczok J, Kluba-Szyszka A,
Bidzińska-Speichert B and Knychalski B: Ovarian hyperstimulation
caused by gonadotroph pituitary adenoma-review. Adv Clin Exp Med.
24:695–703. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Nouri K, Tempfer CB, Lenart C,
Windischbauer L, Walch K, Promberger R and Ott J: Predictive
factors for recovery time in patients suffering from severe OHSS.
Reprod Biol Endocrinol. 12:592014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Guo JL, Zhang DD, Zhao Y, Zhang D, Zhang
XM, Zhou CQ and Yao SZ: Pharmacologic interventions in preventing
ovarian hyperstimulation syndrome: A systematic review and network
meta-analysis. Sci Rep. 6:190932016. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Miller I, Chuderland D, Ron-El R, Shalgi R
and Ben-Ami I: GnRH agonist triggering modulates PEDF to VEGF ratio
inversely to hCG in granulosa cells. J Clin Endocrinol Metab.
100:E1428–E1436. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Ingman WV and Robertson SA: Transforming
growth factor-beta1 null mutation causes infertility in male mice
associated with testosterone deficiency and sexual dysfunction.
Endocrinology. 148:4032–4043. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Herr D, Bekes I and Wulff C: Local
renin-angiotensin system in the reproductive system. Front
Endocrinol (Lausanne). 4:1502013.PubMed/NCBI
|
|
11
|
Ashrafi M, Bahmanabadi A, Akhond MR and
Arabipoor A: Predictive factors of early moderate/severe ovarian
hyper stimulation syndrome in non-polycystic ovarian syndrome
patients: A statistical model. Arch Gynecol Obstet. 292:1145–1152.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ocal P, Sahmay S, Cetin M, Irez T, Guralp
O and Cepni I: Serum anti-Müllerian hormone and antral follicle
count as predictive markers of OHSS in ART cycles. J Assist Reprod
Genet. 28:1197–1203. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Markel G, Imazio M, Koren-Morag N,
Galore-Haskel G, Schachter J, Besser M, Cumetti D, Maestroni S,
Altman A, Shoenfeld Y, et al: CEACAM1 and MICA as novel serum
biomarkers in patients with acute and recurrent pericarditis.
Oncotarget. 7:17885–17895. 2016.PubMed/NCBI
|
|
14
|
Xu D, Li Y, Li X, Wei LL, Pan Z, Jiang TT,
Chen ZL, Wang C, Cao WM, Zhang X, et al: Serum protein S100A9,
SOD3, and MMP9 as new diagnostic biomarkers for pulmonary
tuberculosis by iTRAQ-coupled two-dimensional LC-MS/MS. Proteomics.
15:58–67. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Palioura E and Diamanti-Kandarakis E:
Polycystic ovary syndrome (PCOS) and endocrine disrupting chemicals
(EDCs). Rev Endocr Metab Disord. 16:365–371. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Golan A and Weissman A: Symposium: Update
on prediction and management of OHSS. A modern classification of
OHSS. Reprod Biomed Online. 19:28–32. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Nhi DM, Huy NT, Ohyama K, Kimura D, Lan
NT, Uchida L, Thuong NV, Nhon CT, le Phuc H, Mai NT, et al: A
proteomic approach identifies candidate early biomarkers to predict
severe dengue in children. PLoS Negl Trop Dis. 10:e00044352016.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Zhang Y, Kang Y, Zhou Q, Zhou J, Wang H,
Jin H, Liu X, Ma D and Li X: Quantitative proteomic analysis of
serum from pregnant women carrying a fetus with conotruncal heart
defect using isobaric tags for relative and absolute quantitation
(iTRAQ) labeling. PLoS One. 9:e1116452014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Chen L, Gu H, Li J, Yang ZY, Sun X, Zhang
L, Shan L, Wu L, Wei X, Zhao Y, et al: Comprehensive maternal serum
proteomics identifies the cytoskeletal proteins as non-invasive
biomarkers in prenatal diagnosis of congenital heart defects. Sci
Rep. 6:192482016. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Ezeh U, Yildiz BO and Azziz R: Referral
bias in defining the phenotype and prevalence of obesity in
polycystic ovary syndrome. J Clin Endocrinol Metab. 98:E1088–E1096.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ezcurra D and Humaidan P: A review of
luteinising hormone and human chorionic gonadotropin when used in
assisted reproductive technology. Reprod Biol Endocrinol.
12:952014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Lehert P, Kolibianakis EM, Venetis CA,
Schertz J, Saunders H, Arriagada P, Copt S and Tarlatzis B:
Recombinant human follicle-stimulating hormone (r-hFSH) plus
recombinant luteinizing hormone versus r-hFSH alone for ovarian
stimulation during assisted reproductive technology: Systematic
review and meta-analysis. Reprod Biol Endocrinol. 12:172014.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Peluso C, Fonseca FL, Gastaldo GG,
Christofolini DM, Cordts EB, Barbosa CP and Bianco B: AMH and AMHR2
polymorphisms and AMH serum level can predict assisted reproduction
outcomes: A cross-sectional study. Cell Physiol Biochem.
35:1401–1412. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Salmassi A, Mettler L, Hedderich J, Jonat
W, Deenadayal A, von Otte S, Eckmann-Scholz C and Schmutzler AG:
Cut-off levels of anti-mullerian hormone for the prediction of
ovarian response, in vitro fertilization outcome and ovarian
hyperstimulation syndrome. Int J Fertil Steril. 9:157–167.
2015.PubMed/NCBI
|
|
25
|
Sam S: Adiposity and metabolic dysfunction
in polycystic ovary syndrome. Horm Mol Biol Clin Investig.
21:107–116. 2015.PubMed/NCBI
|
|
26
|
Carreau AM and Baillargeon JP: PCOS in
adolescence and type 2 diabetes. Curr Diab Rep. 15:5642015.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Polyzos SA, Kountouras J, Deretzi G, Zavos
C and Mantzoros CS: The emerging role of endocrine disruptors in
pathogenesis of insulin resistance: A concept implicating
nonalcoholic fatty liver disease. Curr Mol Med. 12:68–82. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Alonso-Magdalena P, Quesada I and Nadal A:
Endocrine disruptors in the etiology of type 2 diabetes mellitus.
Nat Rev Endocrinol. 7:346–353. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Levy AP, Asleh R, Blum S, Levy NS,
Miller-Lotan R, Kalet-Litman S, Anbinder Y, Lache O, Nakhoul FM,
Asaf R, et al: Haptoglobin: Basic and clinical aspects. Antioxid
Redox Signal. 12:293–304. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Orvieto R, Dratviman-Storobinsky O,
Lantsberg D, Haas J, Mashiach R and Cohen Y: Interleukin-2 and
SOCS-1 proteins involvement in the pathophysiology of severe
ovarian hyperstimulation syndrome-a preliminary proof of concept. J
Ovarian Res. 7:1062014. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Elliott BM and Aledort LM: Restoring
hemostasis: Fibrinogen concentrate versus cryoprecipitate. Expert
Rev Hematol. 6:277–286. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Wang S, Moustaid-Moussa N, Chen L, Mo H,
Shastri A, Su R, Bapat P, Kwun I and Shen CL: Novel insights of
dietary polyphenols and obesity. J Nutr Biochem. 25:1–18. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Chistyakova GN, Remizova II, Gazieva IA
and Chermyaninova OV: Immunological and hemostasiological disorders
in women with ovarian hyperstimulation syndrome. Gynecol
Endocrinol. 30:(Suppl 1). S39–S42. 2014. View Article : Google Scholar
|
|
34
|
Olivecrona G: Role of lipoprotein lipase
in lipid metabolism. Curr Opin Lipidol. 27:233–241. 2016.
View Article : Google Scholar : PubMed/NCBI
|