Introduction
Lung cancer is the leading cause of
cancer-associated death worldwide, ~85% of which is non-small cell
lung cancer (NSCLC) (1). The two
major histological subtypes of NSCLC are adenocarcinoma (30–50% of
cases) and squamous cell carcinoma (SQCC; ~30% of cases) (2). There have been advances in
molecularly-targeted agents for the treatment of lung
adenocarcinoma (3,4), however, progress in the treatment of
lung SQCC has been limited. An increasing number of studies have
supported the notion that adenocarcinoma and SQCC are not a
homogeneous group of tumors and that they should be examined
separately to identify potential molecular targets (5,6).
Thus, the identification of novel, potential therapeutic targets
for lung SQCC is required to improve treatment of this type of
cancer.
Podoplanin is a mucin-like transmembrane
glycoprotein that is highly and specifically expressed in lymphatic
endothelial cells (7). Multiple
studies have demonstrated that podoplanin is upregulated in a
number of cancers, including NSCLC (8) and it has been identified as a
candidate cancer stem cell marker (9). Notably, podoplanin is frequently
detected in lung SQCC tumor cells, however, it is rarely observed
in lung adenocarcinoma tumor cells (8).
Our previous study demonstrated that the expression
level of fibroblast growth factor (FGF) 1 was also significantly
higher in lung SQCC compared with lung adenocarcinoma, and FGF1 was
associated with poor prognosis in lung SQCC, which was not the case
in lung adenocarcinoma (10).
Furthermore, our previous study indicated that FGF1 was
predominantly located on the edge of tumor nests in certain lung
SQCC sections, which resembles the characteristic expression
pattern of podoplanin (11). Based
on the consistently specific expression of podoplanin and FGF1 in
lung SQCC tissues and their similar location pattern, the present
study investigated whether tumor-cell expression of podoplanin is
correlated with that of FGF1, and whether co-expression is
associated with clinicopathological factors and prognosis in lung
SQCC. To the best of our knowledge, the correlation between
podoplanin and FGF1 expression and the clinicopathological
significance of their co-expression has not been previously
investigated.
As a potent mitogenic growth factor, FGF1 promotes
the proliferation, migration and survival of vascular (12) and lymphatic endothelial cells
(13), which are essential for
angiogenesis and lymphangiogenesis, respectively. Similarly,
podoplanin has certain roles in tumor lymphangiogenesis and
angiogenesis. Researchers have previously demonstrated that
podoplanin regulates the expression of vascular endothelial growth
factor C (VEGFC) (14) and
endothelin-1 (15), which affects
lymphangiogenesis. Pula et al (16) reported that podoplanin expression
in cancer-associated fibroblasts (CAFs) was positively correlated
with intratumoral microvessel density (MVD), which suggested a role
for podoplanin in angiogenesis. However, clinical correlations
between podoplanin expression and lymphangiogenesis/angiogenesis in
human lung SQCC tissues have not previously been reported.
Therefore, the present study aimed to investigate whether
podoplanin may regulate the expression of FGF1 to influence tumor
lymphangiogenesis and/or angiogenesis in lung SQCC.
The current study examined the correlation between
podoplanin and FGF1 expression in cancer cells of 82 lung SQCC
cases (stage I–IV) by immunohistochemical (IHC) staining and
investigated the association between podoplanin/FGF1 co-expression
and clinicopathological factors, such as MVD in these samples. In
addition, the prognostic value of co-expression of podoplanin and
FGF1 in lung SQCC tumor cells was examined, and the potential
regulation of FGF1 expression and angiogenesis by podoplanin in
vitro in a human lung SQCC cell line was investigated.
Materials and methods
Patients
Tumor specimens were obtained from 82 patients with
primary lung SQCC who underwent surgery at the Jinan Central
Hospital of Shandong University (Jinan, China) between January 2006
and May 2009. Patients had not received radiation therapy or
chemotherapy prior to biopsy or surgical resection. Written
informed consent was obtained from each patient. The study was
approved by the Institutional Review Board of Jinan Central
Hospital of Shandong University. Patients included 74 men and 8
women with a median age of 62 (range, 41–82) years at the time of
diagnosis. The tumor, node, metastasis (TNM) classification was
performed according to the Union for International Cancer Control
7th edition staging system for NSCLC (17). Patients were followed up for a
median follow-up period of 19.5 months (range, 3–60 months)
following surgery.
Cell lines and cell culture
NCI-H226 human lung SQCC cell line and human
umbilical vein endothelial cells (HUVECs) were obtained from
American Type Culture Collection (Manassas, VA, USA). NCI-H226 SQCC
cells were cultured in RPMI-1640 medium supplemented with 10% fetal
bovine serum (both from Hyclone; GE Healthcare Life Sciences,
Logan, UT, USA) and 100 U/ml penicillin-streptomycin. HUVECs were
cultured in endothelial cell medium (ScienCell Research
Laboratories, Inc., Carlsbad, CA, USA). Cells were maintained at
37°C with 5% CO2 in a humidified incubator.
Gene silencing
Small interfering RNAs (siRNAs; 21-nucleotides-long)
targeting podoplanin (siRNA-1 and siRNA-2; Shanghai GenePharma Co.,
Ltd., Shanghai, China) were transfected into NCI-H226 cells using
Lipofectamine® 2000 transfection reagent (Invitrogen; Thermo Fisher
Scientific, Inc., Waltham, MA, USA) according to the manufacturer's
instructions. Scrambled siRNA was used as a negative control (NC).
siRNA sequences were as follows: siRNA-1,
5′-GCGCAAGAACAAAGUCCAATT-3′; siRNA-2, 5′-GACCCUGGUUGGAAUCAUATT-3′;
and NC, 5′-UUCUCCGAACGUGUCACGUTT-3′. Transfected cells were
harvested after 48 and 72 h, the effect on podoplanin expression
was assessed and cells were subsequently used for further
experiments.
Reverse transcription-quantitative
polymerase chain reaction (RT-qPCR)
Total RNA was isolated from cultured cells using
TRIzol reagent (Invitrogen; Thermo Fisher Scientific, Inc.) and
reverse transcription was performed using the RevertAid First
Strand cDNA Synthesis kit (Thermo Fisher Scientific, Inc.). qPCR
was performed using Maxima SYBR-Green qPCR Master Mix (Thermo
Fisher Scientific, Inc.) on a CFX96™ Real-Time PCR Detection System
(Bio-Rad Laboratories, Inc., Hercules, CA, USA). The following
primers were used for qPCR: Human podoplanin,
5′-GATGGAGACACACAGACAACAGT-3′ (forward) and
5′-TTTTCGCATAACCACAACGAT-3′ (reverse); human FGF1,
5′-GTGGATGGGACAAGGGACAG-3′ (forward) and 5′-GGCAGGGGGAGAAACAAGAT-3′
(reverse); and human GAPDH 5′-AGAAGGCTGGGGCTCATTTG-3′ (forward) and
5′-AGGGGCCATCCACAGTCTTC-3′ (reverse). The reaction conditions
consisted of 50°C for 2 min and 94°C for 10 min (initial
denaturation), followed by 40 cycles of 94°C for 15 sec and 60°C
for 60 sec. This was followed by melting curve analysis to verify
the specificity and identity of the PCR product. Amplification
results for qPCR were calculated using the 2−ΔΔCq method
(18) and expression was
normalized to that of GAPDH. The experiments were repeated at least
three times.
Western blot analysis
Cells were lysed with lysis buffer (Beyotime
Institute of Biotechnology, Haimen, China) containing protease
inhibitor phenylmethane sulfonyl fluoride (Beyotime Institute
Biotechnology), and the supernatant of the lysed cells was
recovered. Protein concentrations were quantified using a
bicinchoninic acid protein assay. Protein samples (50 µg per lane)
were separated by 10% SDS-PAGE and transferred onto polyvinylidene
difluoride membranes. Non-specific binding was blocked with 5% skim
milk in TBS containing 0.1% Tween-20 for 1 h at room temperature.
Subsequently, blotted membranes were incubated overnight at 4°C
with specific primary antibodies. The following primary antibodies
were used: Monoclonal rabbit anti-human podoplanin antibody
(1:1,000; cat. no. 9047; Cell Signaling Technology, Inc., Danvers,
MA, USA); monoclonal mouse anti-human FGF1 antibody (1:500; cat.
no. H00002246-M02; Abnova Corporation, Taipei, Taiwan); and
monoclonal mouse anti-human α-tubulin antibody (1:5,000; cat. no.
66031-1-Ig; ProteinTech Group, Inc., Chicago, IL, USA) as a loading
control. Detection was performed using horseradish
peroxidase-conjugated secondary antibodies (1:5,000; cat. nos.
SA00001-1 and SA00001-2; ProteinTech Group, Inc.). Finally, blots
were immersed in ECL detection reagent (EMD Millipore, Billerica,
MA, USA) and exposed to a ChemiDoc™ XRS+ system (Bio-Rad
Laboratories, Inc.).
Preparation and concentration of
culture supernatants
To prepare culture supernatants, 2.5×105 NCI-H226
cells were plated in 6-well plates and transfected with podoplanin
siRNAs as described above. Culture medium was replaced with
serum-free medium at 12 h after transfection and cells were
cultured for a further 60 h. Subsequently, supernatants were
harvested and centrifuged at 1,000 × g for 10 min. For western blot
analysis, culture supernatants were concentrated with Amicon
Ultra-0.5 Centrifugal Filter Unit with Ultracel-3 membrane (EMD
Millipore) according to the manufacturer's instructions.
Capillary tube formation assay
For investigation of capillary tube formation,
96-well plates were coated with 60 µl growth factor-reduced
Matrigel (BD Biosciences, Franklin Lakes, NJ, USA) and incubated at
37°C for 1 h to allow gelling. Tumor cell culture supernatants were
prepared as described above. HUVECs were resuspended using
supernatants collected from cultured tumor cells and seeded on
Matrigel-coated 48-well plates at a density of 2×104 cells/well.
HUVECs were incubated for 8 h. The branch points of the formed
tubes, which represent the degree of angiogenesis in vitro,
were imaged under a light microscope and quantified in 10
microscopic fields.
IHC analysis of tumor specimens
Formalin-fixed, paraffin-embedded tissue sections (4
µm-thick) were deparaffinized and rehydrated. For FGF1, antigen
retrieval was performed by incubating specimens for 5 min in 1% SDS
in TBS at room temperature. For podoplanin, CD34 and D2-40, antigen
retrieval was performed by heating specimens in a microwave oven
for 10 min with 10 mmol/l sodium citrate (pH 6.0). Endogenous
peroxidase activity was blocked with 0.3% hydrogen peroxide for 10
min. Sections were blocked with 5% normal goat serum (cat. no. SP
Kit-B1; Fuzhou Maixin Biotech. Co., Ltd., Fuzhou, China) for 20 min
at room temperature and were subsequently incubated overnight at
4°C with primary antibodies; monoclonal rabbit anti-human
podoplanin antibody (1:600; cat. no. 9047; Cell Signaling
Technology), monoclonal mouse anti-human FGF1 antibody (1:300; cat.
no. H00002246-M02; Abnova Corporation), monoclonal mouse anti-human
CD34 antibody (1:100; cat. no. Kit-0004; Fuzhou Maixin Biotech.
Co., Ltd.) and monoclonal mouse anti-human D2-40 antibody (1:100;
cat. no. MAB-0567, Fuzhou Maixin Biotech Co., Ltd.). To detect
primary antibody binding, sections were incubated with Elivision
super Polymer horseradish peroxidase (Mouse/Rabbit) IHC kit (cat.
no. Kit-9922, Fuzhou Maixin Biotech Co., Ltd.) according to the
manufacturer's protocol. Sections were visualized with
3,3′-diaminobenzidine solution and counterstained with hematoxylin.
Human tonsil tissues and lymphatic vessels in tumors were selected
as positive controls for FGF1 and podoplanin, respectively.
Negative controls were prepared using normal mouse and rabbit IgG
instead of the primary antibody. The expression was quantified
simultaneously by two independent observers who were blind to the
details of the patients. The percentage of stained cells was
recorded at ×400 magnification in ≤5 random fields. Evaluation of
the cell staining reaction was performed using the immunoreactive
score (IRS) as follows: IRS=staining intensity (SI) × percentage of
positive cells (PP), as previously described (19). SI was assigned as 0, negative; 1,
weak; 2, moderate; and 3, strong. PP was defined as 0, negative; 1,
1–10% positive cells; 2, 11–50% positive cells; 3, 51–80% positive
cells; and 4, >80% positive cells. For statistical analyses,
cases with scores 0–3 were defined as negative and all others were
considered positive.
MVD and lymphatic MVD (LMVD) were assessed according
to a modification of Weidner's method (20). MVD was detected by CD34 antibody
and LMVD was detected by D2-40 antibody. The immunostained sections
were viewed using light-microscopy at low magnification (x40) and
the areas of tissue with the greatest number of distinctly
highlighted microvessels (hotspots) were selected. MVD and LMVD
were determined by counting all immunostained vessels at a total
magnification of ×400 from 5 areas for each case. Determination of
the staining reaction was strictly confined to the hotspots and the
mean number of the vessels in each case was evaluated.
Statistical analysis
SPSS version 18.0 (SPSS, Inc., Chicago, IL, USA) was
used for statistical analyses. Spearman correlation analysis was
used to analyze the correlation between podoplanin and FGF1
expression. The association between co-expression of podoplanin and
FGF1, and clinicopathological variables were analyzed using the χ2
test. Associations between podoplanin/FGF1 expression and LMVD/MVD
were analyzed by a two-tailed Student's t-test. Comparisons of mRNA
expression in NC and siRNA groups were performed by two-tailed
Student t-test. Overall survival time was defined as the period
from the date of surgery to the date of death from any cause or the
last day of follow-up evaluation. Survival curves were produced
using the Kaplan-Meier method and compared with log-rank test. For
all tests, P<0.05 was considered to indicate a statistically
significant difference.
Results
Expression of podoplanin and FGF1 in
human primary lung SQCC tissues
The expression of podoplanin and FGF1 was examined
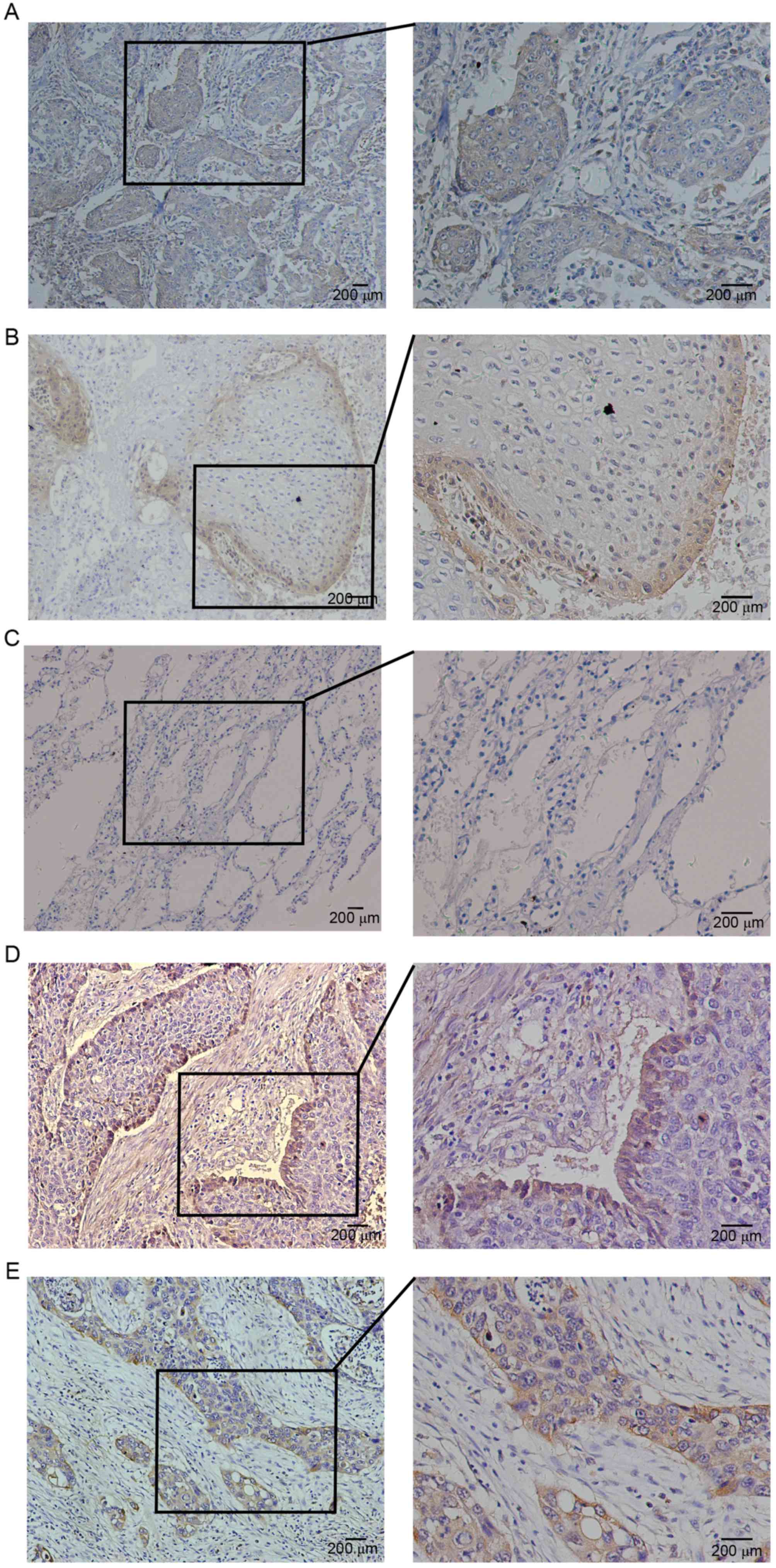
by IHC staining in 82 human lung SQCC specimens. Consistent with
previous reports, expression of podoplanin was detected on the
membrane and/or cytoplasm of tumor cells (Fig. 1A and B). Negative cases were
determined by the staining of lymphatic vessels as an internal
control. In addition, podoplanin expression was observed in stromal
spindle cells that were morphologically identified as fibroblasts.
There was negative or weak staining for podoplanin in peritumoral
normal lung tissues (Fig. 1C).
Positive expression of podoplanin (IRS >3) in tumor cells was
detected in 73.17% (60/82) cases. Higher than previously reported
(11), 38.3% (23/60) of positive
cases exhibited diffuse immunoreactions in almost the entire cancer
nest (Fig. 1A). Other positive
cases exhibited a peripheral expression pattern; expression was
restricted to the outer cell layer of tumor nests (Fig. 1B).
Immunostaining of FGF1 in the majority of cases was
cytoplasmic, while a few cases exhibited nuclear and/or perinuclear
staining in cancer cells. Positive expression of FGF1 in tumor
cells was detected in 70.73% (58/82) lung SQCC samples. Notably,
34.48% (20/58) cases with positive FGF1 expression exhibited a
non-homogeneous peripheral expression pattern (Fig. 1D), which is similar to the
expression pattern of podoplanin. The remaining positive cases
exhibited diffuse expression of FGF1 in the entire cancer nest
(Fig. 1E). In addition, there was
frequent expression of FGF1 in lung SQCC tumor stromal cells.
Co-expression of podoplanin and FGF1
in primary lung SQCC tissues, and the association between
co-expression and clinicopathological factors
Podoplanin and FGF1 were demonstrated to be
co-expressed in lung SQCC tumor cells (Fig. 2A and B), and there was a
significant, positive correlation between podoplanin and FGF1
expression in tumor cells (R=0.591, P<0.0001; Fig. 2C). The cohort of patients was
classified into 4 groups according to the expression of podoplanin
and FGF1 in the same patient. As presented in Table I, 60.98% (50/82) had positive
expression of podoplanin and FGF1 (P+F+), 12.20% (10/82) had
positive expression of podoplanin but negative expression of FGF1
(P+F-), 9.76% (8/82) patients had positive expression of FGF1 but
negative expression of podoplanin (P-F+), and 17.07% (14/82)
patients had negative expression of podoplanin and FGF1 (P-F-). The
P+F+ group was significantly associated with larger primary tumor
size (P=0.042) and advanced TNM stages (P=0.042) compared with the
P-F- group. Whereas, no clinicopathological factors were
demonstrated to be associated with the P+F- or P-F+ groups when
compared with the P-F- group (Table
I).
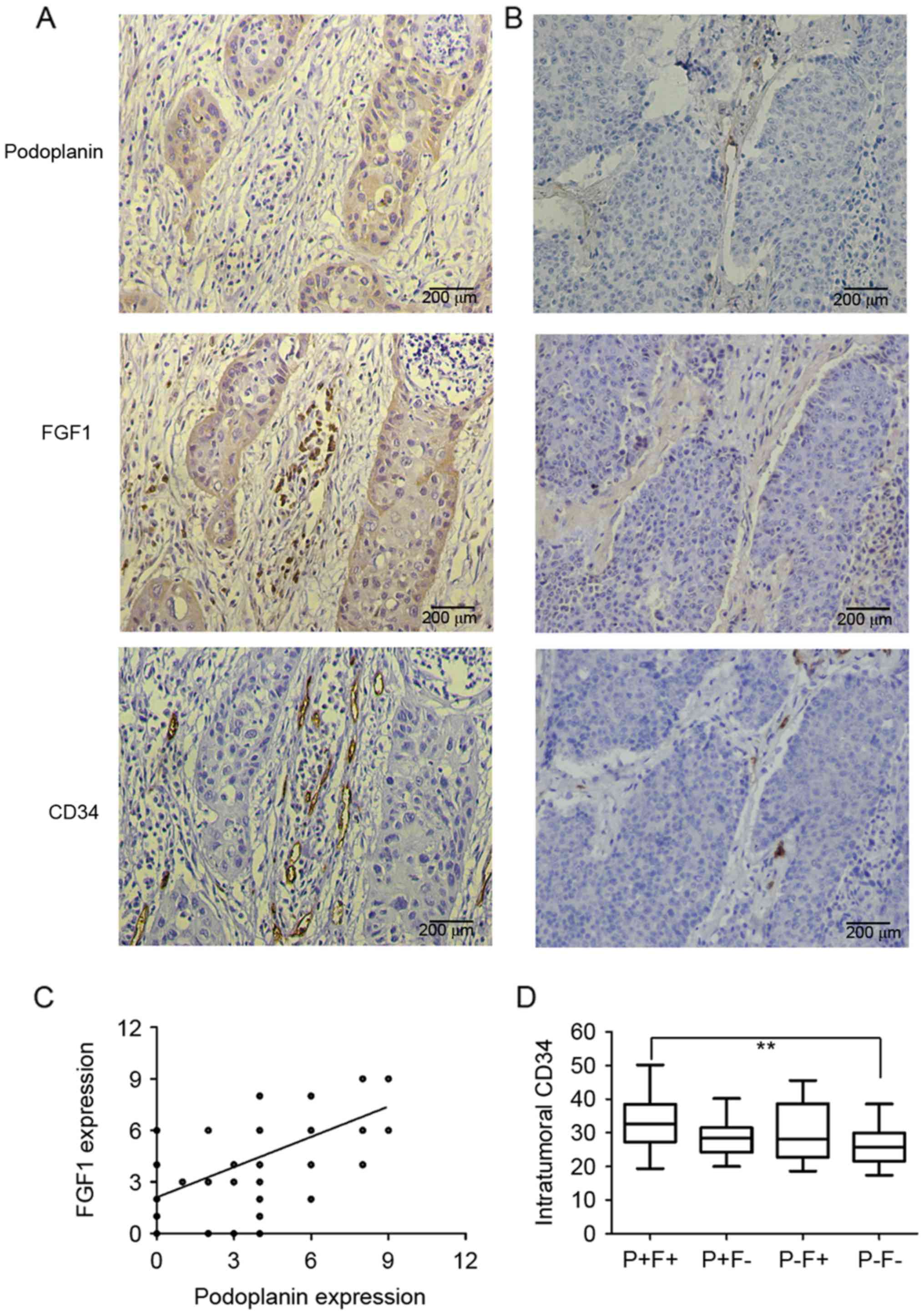 | Figure 2.Consecutive sections of lung squamous
cell carcinoma were stained for podoplanin, FGF1 and CD34.
Representative images of sections of cancer tissue with (A)
positive podoplanin expression and (B) negative podoplanin
expression stained for podoplanin, FGF1 and CD34. (C) Significant
correlation between podoplanin and FGF1 expression in tumor cells
by Spearman correlation analysis (R=0.591, P<0.0001). (D)
Comparison of intratumoral MVD among patients with P+F+, P+F-, P-F+
and P-F-. MVD in P+F+ group was significantly higher than that in
P-F- group. **P<0.01. FGF1, fibroblast growth factor 1; MVD,
microvessel density; P+F+, podoplanin-positive/FGF1-positive; P+F-,
podoplanin-positive/FGF1-negative; P-F+,
podoplanin-negative/FGF1-positive; P-F-,
podoplanin-negative/FGF1-negative. |
 | Table I.Association between podoplanin and
FGF1 co-expression and clinicopathological factors in lung squamous
cell carcinoma patients. |
Table I.
Association between podoplanin and
FGF1 co-expression and clinicopathological factors in lung squamous
cell carcinoma patients.
| Variables | P+F+n | P-value | P+F-n | P-value | P-F+n | P-value | P-F-n |
|---|
| Age, years |
|
≤60 | 22 | 0.299 | 4 | 0.673 | 3 | 1 | 4 |
|
>60 | 28 |
| 6 |
| 5 |
| 10 |
| Sex |
|
Male | 44 | 0.976 | 9 | 1 | 8 | 1 | 13 |
|
Female | 6 |
| 1 |
| 0 |
| 1 |
| Smoking index,
packs/year |
|
≤400 | 17 | 0.568 | 1 | 0.615 | 1 | 1 | 3 |
|
>400 | 33 |
| 9 |
| 7 |
| 11 |
|
Differentiation |
|
Well/moderate | 26 | 0.545 | 5 | 1 | 5 | 0.659 | 6 |
|
Poor | 24 |
| 5 |
| 3 |
| 8 |
| Primary tumor size,
cm |
| ≤5 | 24 | 0.042a | 7 | 0.665 | 5 | 0.624 | 11 |
|
>5 | 26 |
| 3 |
| 3 |
| 3 |
| Lymph node
metastasis |
|
Yes | 35 | 0.061 | 6 | 0.68 | 4 | 1 | 6 |
| No | 15 |
| 4 |
| 4 |
| 8 |
| Vascular
invasion |
|
Yes | 9 | 0.201 | 0 | NA | 1 | 0.364 | 0 |
| No | 41 |
| 10 |
| 7 |
| 14 |
| Pleural
metastasis |
|
Yes | 9 | 0.201 | 1 | 0.417 | 1 | 0.364 | 0 |
| No | 41 |
| 9 |
| 7 |
| 14 |
| TNM stage |
|
I–II | 28 | 0.042a | 7 | 0.615 | 6 | 0.602 | 12 |
|
III–IV | 22 |
| 3 |
| 2 |
| 2 |
Co-expression of podoplanin and FGF1
are associated with intratumoral MVD in primary lung SQCC
tissues
Given the reported effects of podoplanin and FGF1 on
lymphangiogenesis and angiogenesis, the present study evaluated the
association between their separate expression, and MVD and LMVD in
samples. The intratumoral MVD was significantly lower in
podoplanin-negative cases compared with podoplanin-positive cases,
and the same was observed for FGF1 (data not shown). However, there
was no significant difference in intratumoral or peritumoral LMVD
between the podoplanin-positive group and podoplanin-negative
group, as was also the case for FGF1 (data not shown). The
association between co-expression of podoplanin and FGF1, and
intratumoral MVD was also investigated; intratumoral MVD (observed
by CD34 staining) was demonstrated to be associated with the
co-expression of podoplanin and FGF1. The mean MVD was 33.32±8.01
in P+F+ specimens, 28.72±5.93 in P+F-specimens, 29.35±9.30 in P-F+
specimens and 26.64±6.22 in P-F- specimens. The MVD in the P+F+
group was significantly higher compared with the P-F- group
(Fig. 2D). No significant
difference was identified between other pairwise comparisons.
Association between podoplanin/FGF1
co-expression and overall survival of lung SQCC patients
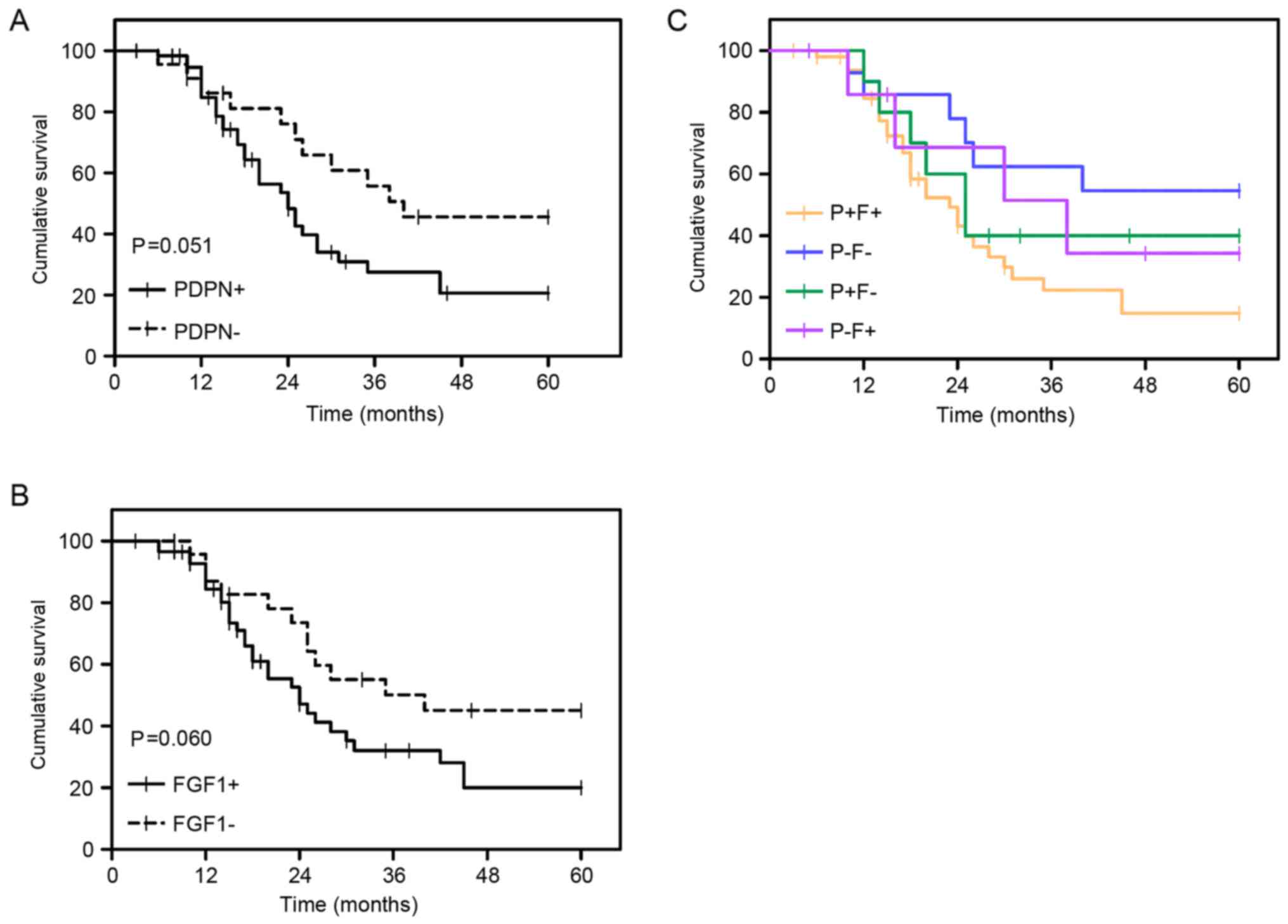
The prognostic value of podoplanin and FGF1
expression in the samples was assessed. The was a difference in the
overall survival rate between podoplanin-positive and
podoplanin-negative, however, the P-value was marginally above that
considered to be significant (P=0.051; Fig. 3A), which was also observed for FGF1
(P=0.060; Fig. 3B). Subsequently,
the prognostic significance of co-expression of podoplanin and FGF1
for lung SQCC patients was investigated. Survival analyses
demonstrated that the P+F+ group exhibited a significantly lower
survival rate compared with the P-F- group (P=0.017; Fig. 3C). No significant differences were
observed between all other pairwise comparisons.
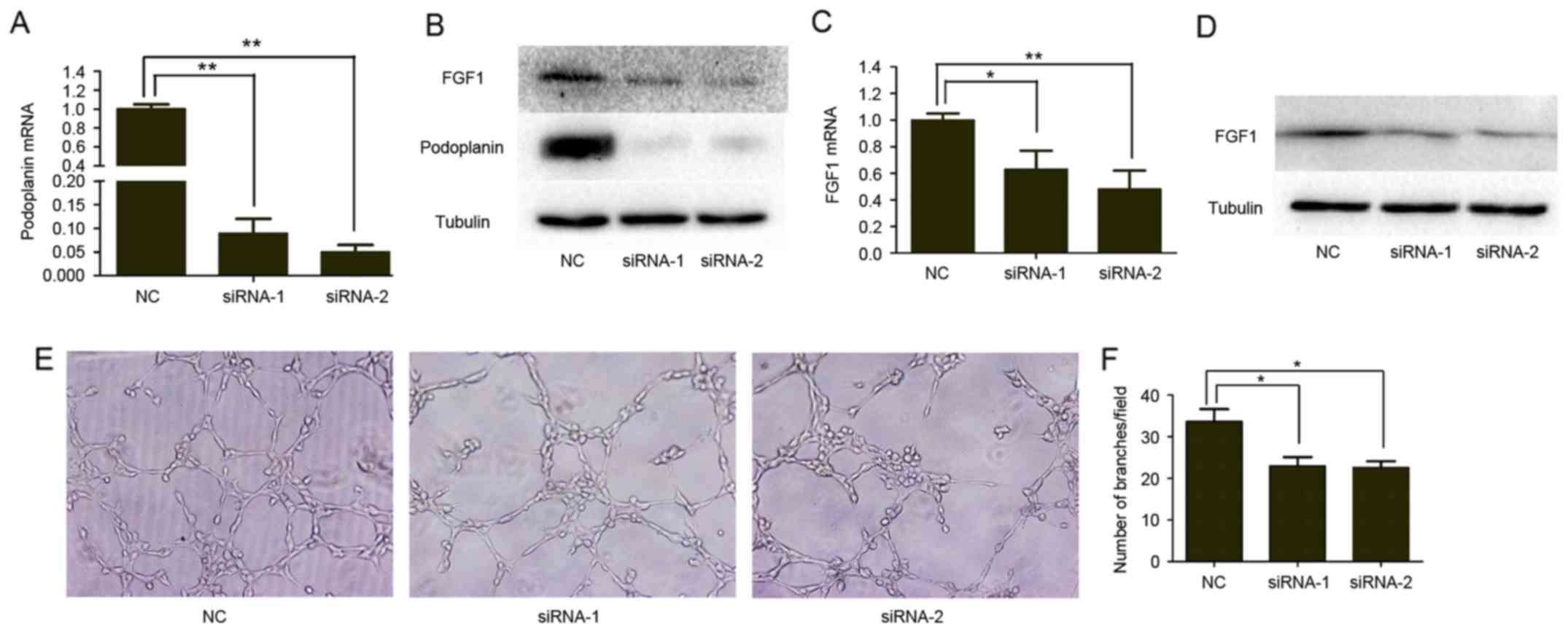
Podoplanin regulates the expression of
FGF1 and angiogenesis in vitro
Based on the proven effect of podoplanin on VEGFC
and endothelin-1 (14,15), which are established
lymphangiogenic and angiogenic factors, we hypothesized that the
clinicopathological association between podoplanin and FGF1 may be
due to the regulatory effect of podoplanin on FGF1 expression. To
investigate whether podoplanin regulates the expression of FGF1
in vitro, the present study used siRNA transfection to
transiently suppress the expression of podoplanin in the NCI-H226
lung SQCC cell line (Fig. 4A and
B). Subsequently, the expression level of FGF1 in
podoplanin-knockdown (podoplanin-KD) and NC NCI-H226 cells was
investigated. RT-qPCR and western blotting revealed that the
expression level of FGF1 mRNA and protein were reduced in
podoplanin-KD NCI-H226 cells compared with NC NCI-H226 cells
(Fig. 4B and C). As FGF1 is a
secreted protein, the level of FGF1 protein in cell culture
supernatants was also determined. Compared with NC NCI-H226 cells,
podoplanin-KD cells secreted a reduced amount of FGF1 (Fig. 4D).
Considering the association between podoplanin
expression and intratumoral MVD, the present study further
investigated whether podoplanin affected angiogenesis in
vitro. As presented in Fig. 4E and
F, HUVECs cultured with tumor cell-conditioned medium from
podoplanin-KD NCI-H226 cells exhibited reduced tube formation and a
reduced number of branch points compared with the control
group.
Discussion
Podoplanin is upregulated in tumor cells in several
cancer types and has been identified as a useful prognostic
biomarker to determine the malignancy of tumors (8,21,22).
Anti-podoplanin monoclonal antibodies have been validated to
suppress the growth and hematogenous metastasis of
podoplanin-expressing tumors (23). Researchers have identified several
potential pathways that may be invoked by podoplanin to promote
tumor progression, including the promotion of
epithelial-to-mesenchymal transition (EMT) (24), inducing collective cell migration
(25), triggering platelet
activation and aggregation (26–28)
and enhancing lymphangiogenesis (15). The present study demonstrated that
podoplanin was co-expressed with FGF1 in cancer cells and was
associated with intratumoral MVD in primary lung SQCC tissues. In
addition, knockdown of podoplanin downregulated the expression of
FGF1 and decreased the formation of tubular networks by HUVECs
in vitro. Co-expression of podoplanin and FGF1 was
significantly associated with larger primary tumor size, advanced
TNM stage, higher intratumoral MVD and worse overall survival.
Combined, the results indicate that podoplanin was implicated in
tumor progression in lung SQCC when co-expressed with FGF1.
Podoplanin−/− mice exhibit systemic edema
due to aplasia of lymphatic vessels during fetal development and
neonatal death due to respiratory failure (29,30),
indicating an important role of podoplanin in normal lymphatic
vessel development. Furthermore, a previous study demonstrated
podoplanin expression was significantly decreased in preeclamptic
placental tissues compared with normotensive placental controls,
indicating that podoplanin may support fetal vessel angiogenesis
during placental development (31). However, several studies concerned
with the involvement of podoplanin in
lymphangiogenesis/angiogenesis in malignant tumors have produced
inconsistent results in different experimental models. Research by
Cueni et al (15)
demonstrated that podoplanin upregulated endothelin-1 to enhance
lymphangiogenesis and metastasis to regional lymph nodes in breast
carcinoma xenografts (15). In
addition, Suzuki et al (14) reported that podoplanin attenuated
lymphogenous metastasis and lymphangiogenesis by downregulating
VEGFC in a lung squamous cancer cell line, with no impact observed
on angiogenesis (14). The present
study did not demonstrate a significant association between the
expression of podoplanin in cancer cells and
intratumoral/peritumoral LMVD in human lung SQCC tissues. This
inconsistency may be due to the specificity of different cancer
types. As demonstrated by previous studies, podoplanin does not
exert the same function in all cell types. For example, although
podoplanin upregulates RhoA activity and induces EMT in MDCK cells
(24), it attenuated RhoA activity
and did not induce EMT in a breast carcinoma cell line (25). In fact, Suzuki et al
(14) demonstrated that podoplanin
decreased the area and perimeter of lymphatic vessels, however, it
had no significant effect on the number of lymphatic vessels in an
animal model (14), which was
consistent with the results of the present study.
The present study, in contrast to the results of
Suzuki et al (14),
demonstrated that podoplanin was associated with intratumoral MVD
and was co-expressed with FGF1 in primary lung SQCC tissues.
Similarly, Pula et al (16)
observed that podoplanin expression in CAFs was positively
correlated with cancer cell VEGFC expression and intratumoral MVD
in invasive ductal carcinoma of breast by immunohistochemistry
(16). These experimental results
indicated that podoplanin may participate in tumor angiogenesis
mediated by specific angiogenic growth factors. VEGFC, a regulator
of lymphangiogenesis, also contributes to angiogenesis (32). The present study validated the
regulation FGF1 expression and angiogenesis by podoplanin in
vitro and hypothesized that podoplanin may exert angiogenic
action through FGF1, an established angiogenic growth factor.
However, the current study did not demonstrate any direct evidence
proving the association between the podoplanin-FGF1 axis and
podoplanin-dependent angiogenesis, which requires further research.
Furthermore, it was previously reported that FGF1 induced the
expression of CD44s (33), and
podoplanin interacted with CD44s to drive directional cell
migration in tumor cells (34).
Therefore, the association between podoplanin and FGF1 may not be
confined to tumor angiogenesis, they may also work together to
regulate tumor cell motility.
Consistent with the results of our previous study,
FGF1 expression was detected at the periphery of cell nests in
certain lung SQCC specimens, which was similar to podoplanin and
CD44, which are candidate cancer stem cell markers (11). FGF1 has been reported to be
upregulated in cancer stem cells of small cell lung cancer
(35) and it contributes to
sustaining neural stem cell growth and self-renewal capacity in
glioblastoma (36). Therefore,
FGF1 may be a candidate cancer stem cell marker, and the
double-positive expression of podoplanin and FGF1 may have
potential as a more accurate screening method for the detection of
cancer stem cells. However, the current study did not investigate
the molecular pathway by which podoplanin regulated the expression
of FGF1, which requires further investigation.
According to the survival analysis performed in the
present study, the overall survival was lower in patients with
podoplanin-positive lung SQCC compared with patients with
podoplanin-negative lung SQCC, although not to a significant
extent. In fact, previous studies have produced controversial
results regarding the prognostic role of podoplanin in lung SQCC.
Kadota et al (8) reported
tumor cell podoplanin immunoreactivity to be a significant
indicator of poor prognosis in NSCLC patients, particularly in lung
SQCC patients, which was consistent with the results of the present
study. By contrast, other studies have demonstrated that low
podoplanin expression in tumor cells predicts poor prognosis in
lung SQCC (11,37,38).
The reason behind the conflicting results remains unclear;
differences in the way that a positive or high expression of
podoplanin is defined across different studies may be one of the
reasons behind this discrepancy. However, a significant correlation
has been observed between the pattern of podoplanin expression and
tumor grade, that is, diffuse infiltrating positivity was detected
in undifferentiated tumors and a peripheral pattern in
well-differentiated ones (22,39).
In the current study, a higher proportion of lung SQCC patients
exhibited positive reactions in the majority of the cancer cell
nest than previously reported. This may partially explain the
disagreement between results of previous studies. Furthermore, the
present study demonstrated that cases with double-positive
podoplanin and FGF1 staining had significantly shorter survival
times compared with those with double negative staining, indicating
that integrated assessment of podoplanin and FGF1 may more
accurately predict the prognosis of lung SQCC patients compared
with either of them alone.
In conclusion, the present study confirmed that
podoplanin was co-expressed with FGF1 in lung SQCC and that
co-expression was associated with higher intratumoral MVD and poor
prognosis of patients with lung SQCC. In vitro experiments
demonstrated that podoplanin regulated the FGF1 expression and tube
formation of HUVECs. The results indicate that podoplanin may
participate in angiogenesis and tumor progression mediated by FGF1
in lung SQCC. Further investigated is necessary to establish the
mechanism by which podoplanin regulates FGF1 expression and the
synergistic effect mechanism of the two molecules.
Acknowledgements
This study was supported by the Project of Jinan
Science and Technology Plan (grant no. 201101112). We thank Dong
Zhao and Ling Wang of Department of Pathology, Jinan Central
Hospital, Shandong University (Jinan, China) for assisting with the
collection of NSCLC samples and preparing tissue sections. We
acknowledge Dr Huiping Liu of the Department of Pathology, Jinan
Central Hospital, Shandong University for quantifying
immunohistochemical sections.
References
|
1
|
World Health Organization Media Centre, .
Cancer. Fact sheet no. 297. http://www.who.int/mediacentre/factsheets/fs297/en/February.
2017
|
|
2
|
Herbst RS, Heymach JV and Lippman SM: Lung
Cancer. N Engl J Med. 359:1367–1380. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Pao W, Miller V, Zakowski M, Doherty J,
Politi K, Sarkaria I, Singh B, Heelan R, Rusch V, Fulton L, et al:
EGF receptor gene mutations are common in lung cancers from ‘never
smokers’ and are associated with sensitivity of tumors to gefitinib
and erlotinib. Proc Natl Acad Sci USA. 101:13306–13311. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kwak EL, Bang YJ, Camidge DR, Shaw AT,
Solomon B, Maki RG, Ou SH, Dezube BJ, Jänne PA, Costa DB, et al:
Anaplastic lymphoma kinase inhibition in non-small-cell lung
cancer. N Engl J Med. 363:1693–1703. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Daraselia N, Wang Y, Budoff A, Lituev A,
Potapova O, Vansant G, Monforte J, Mazo I and Ossovskaya VS:
Molecular signature and pathway analysis of human primary squamous
and adenocarcinoma lung cancers. Am J Cancer Res. 2:93–103.
2012.PubMed/NCBI
|
|
6
|
Heist RS, Sequist LV and Engelman JA:
Genetic changes in squamous cell lung cancer: A review. J Thorac
Oncol. 7:924–933. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kahn HJ and Marks A: A new monoclonal
antibody, D2-40, for detection of lymphatic invasion in primary
tumors. Lab Invest. 82:1255–1257. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kadota K, Huang CL, Liu D, Nakashima N,
Yokomise H, Ueno M and Haba R: The clinical significance of the
tumor cell D2-40 immunoreactivity in non-small cell lung cancer.
Lung Cancer. 70:88–93. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Atsumi N, Ishii G, Kojima M, Sanada M,
Fujii S and Ochiai A: Podoplanin, a novel marker of
tumor-initiating cells in human squamous cell carcinoma A431.
Biochem Biophys Res Commun. 373:36–41. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Li J, Wei Z, Li H, Dang Q, Zhang Z, Wang
L, Gao W, Zhang P, Yang D, Liu J, et al: Clinicopathological
significance of fibroblast growth factor 1 in non-small cell lung
cancer. Hum Pathol. 46:1821–1828. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Shimada Y, Ishii G, Nagai K, Atsumi N,
Fujii S, Yamada A, Yamane Y, Hishida T, Nishimura M, Yoshida J, et
al: Expression of podoplanin, CD44, and p63 in squamous cell
carcinoma of the lung. Cancer Sci. 100:2054–2059. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Presta M, Dell'Era P, Mitola S, Moroni E,
Ronca R and Rusnati M: Fibroblast growth factor/fibroblast growth
factor receptor system in angiogenesis. Cytokine Growth Factor Rev.
16:159–178. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Shin JW, Min M, Larrieu-Lahargue F, Canron
X, Kunstfeld R, Nguyen L, Henderson JE, Bikfalvi A, Detmar M and
Hong YK: Prox1 promotes lineage-specific expression of fibroblast
growth factor (FGF) receptor-3 in lymphatic endothelium: A role for
FGF signaling in lymphangiogenesis. Mol Biol Cell. 17:576–584.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Suzuki H, Onimaru M, Yonemitsu Y, Maehara
Y, Nakamura S and Sueishi K: Podoplanin in cancer cells is
experimentally able to attenuate prolymphangiogenic and
lymphogenous metastatic potentials of lung squamoid cancer cells.
Mol Cancer. 9:2872010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Cueni LN, Hegyi I, Shin JW, Albinger-Hegyi
A, Gruber S, Kunstfeld R, Moch H and Detmar M: Tumor
lymphangiogenesis and metastasis to lymph nodes induced by cancer
cell expression of podoplanin. Am J Pathol. 177:1004–1016. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Pula B, Wojnar A, Witkiewicz W, Dziegiel P
and Podhorska-Okolow M: Podoplanin expression in cancer-associated
fibroblasts correlates with VEGF-C expression in cancer cells of
invasive ductal breast carcinoma. Neoplasma. 60:516–524. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Sobin LHGM and Wittekind C: UICC TNM
Classification of Malignant Tumours. 7th. Wiley-Liss; New York, NY:
2009
|
|
18
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(−Delta Delta C(T)) Method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Engels K, Knauer SK, Metzler D, Simf C,
Struschka O, Bier C, Mann W, Kovács AF and Stauber RH: Dynamic
intracellular survivin in oral squamous cell carcinoma: Underlying
molecular mechanism and potential as an early prognostic marker. J
Pathol. 211:532–540. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Weidner N, Semple JP, Welch WR and Folkman
J: Tumor angiogenesis and metastasis-correlation in invasive breast
carcinoma. N Engl J Med. 324:1–8. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Yuan P, Temam S, El-Naggar A, Zhou X, Liu
DD, Lee JJ and Mao L: Overexpression of podoplanin in oral cancer
and its association with poor clinical outcome. Cancer.
107:563–569. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Minardi D, d'Anzeo G, Lucarini G, Filosa
A, Zizzi A, Simonetti O, Polito M Jr, Offidani AM, Di Primio R,
Montironi R and Muzzonigro G: D2-40 immunoreactivity in penile
squamous cell carcinoma: A marker of aggressiveness. Hum Pathol.
42:1596–1602. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Nakazawa Y, Takagi S, Sato S, Oh-hara T,
Koike S, Takami M, Arai H and Fujita N: Prevention of hematogenous
metastasis by neutralizing mice and its chimeric
anti-Aggrus/podoplanin antibodies. Cancer Sci. 102:2051–2057. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Martín-Villar E, Megías D, Castel S,
Yurrita MM, Vilaró S and Quintanilla M: Podoplanin binds ERM
proteins to activate RhoA and promote epithelial-mesenchymal
transition. J Cell Sci. 119:4541–4553. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Wicki A, Lehembre F, Wick N, Hantusch B,
Kerjaschki D and Christofori G: Tumor invasion in the absence of
epithelial-mesenchymal transition: Podoplanin-mediated remodeling
of the actin cytoskeleton. Cancer Cell. 9:261–272. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kunita A, Kashima TG, Morishita Y,
Fukayama M, Kato Y, Tsuruo T and Fujita N: The platelet
aggregation-inducing factor aggrus/podoplanin promotes pulmonary
metastasis. Am J Pathol. 170:1337–1347. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Suzuki-Inoue K, Kato Y, Inoue O, Kaneko
MK, Mishima K, Yatomi Y, Yamazaki Y, Narimatsu H and Ozaki Y:
Involvement of the Snake Toxin Receptor CLEC-2, in
Podoplanin-mediated platelet activation, by cancer cells. J Biol
Chem. 282:25993–26001. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Nakazawa Y, Sato S, Naito M, Kato Y,
Mishima K, Arai H, Tsuruo T and Fujita N: Tetraspanin family member
CD9 inhibits Aggrus/podoplanin-induced platelet aggregation and
suppresses pulmonary metastasis. Blood. 112:1730–1739. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Ramirez MI, Millien G, Hinds A, Cao Y,
Seldin DC and Williams MC: T1alpha, a lung type I cell
differentiation gene, is required for normal lung cell
proliferation and alveolus formation at birth. Dev Biol. 256:61–72.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Schacht V, Ramirez MI, Hong YK, Hirakawa
S, Feng D, Harvey N, Williams M, Dvorak AM, Dvorak HF, Oliver G and
Detmar M: T1alpha/podoplanin deficiency disrupts normal lymphatic
vasculature formation and causes lymphedema. EMBO J. 22:3546–3556.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Wang Y, Sun J, Gu Y, Zhao S, Groome LJ and
Alexander JS: D2-40/podoplanin expression in the human placenta.
Placenta. 32:27–32. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Nagai N and Minami T: Emerging role of
VEGFC in pathological angiogenesis. EBioMedicine. 2:1588–1589.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Palen KA, Jing W, Weber JJ, Tilkens SB,
Chan AM, Johnson BD and Gershan JA: Separation and characterization
of epithelial and mesenchymal-like murine mammary tumor cells
reveals epithelial cell differentiation plasticity and enhanced
tumorigenicity of epithelial-enriched tumor cells. Cancer
Microenviron. 6:79–89. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Martin-Villar E, Fernández-Muãoz B,
Parsons M, Yurrita MM, Megias D, Pérez-Gómez E, Jones GE and
Quintanilla M: Podoplanin associates with CD44 to promote
directional cell migration. Mol Biol Cell. 21:4387–4399. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Salcido CD, Larochelle A, Taylor BJ,
Dunbar CE and Varticovski L: Molecular characterisation of side
population cells with cancer stem cell-like characteristics in
small-cell lung cancer. Br J Cancer. 102:1636–1644. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Hsu YC, Lee DC, Chen SL, Liao WC, Lin JW,
Chiu WT and Chiu IM: Brain-specific 1B promoter of FGF1 gene
facilitates the isolation of neural stem/progenitor cells with
self-renewal and multipotent capacities. Dev Dyn. 238:302–314.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Ito T, Ishii G, Nagai K, Nagano T, Kojika
M, Murata Y, Atsumi N, Nishiwaki Y, Miyazaki E, Kumamoto T and
Ochiai A: Low podoplanin expression of tumor cells predicts poor
prognosis in pathological stage IB squamous cell carcinoma of the
lung, tissue microarray analysis of 136 patients using 24
antibodies. Lung Cancer. 63:418–424. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Suzuki H, Onimaru M, Koga T, Takeshita M,
Yano T, Maehara Y, Nakamura S and Sueishi K: High podoplanin
expression in cancer cells predicts lower incidence of nodal
metastasis in patients with lung squamous cell carcinoma. Pathol
Res Pract. 207:111–115. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Ikoma Y, Kijima H, Masuda R, Tanaka M,
Inokuchi S and Iwazaki M: Podoplanin expression is correlated with
the prognosis of lung squamous cell carcinoma. Biomed Res.
36:393–402. 2015. View Article : Google Scholar : PubMed/NCBI
|