Introduction
Various investigators have studied the prognostic
factors of esophageal squamous cell carcinoma (ESCC) treated with
concurrent chemoradiation therapy (CCRT). In previous studies, it
was considered that the expression levels of p53 (1–3),
p21waf1(4), molecular
immunology borstel-1 (MIB-1) (2,5),
p16INK4A(6), cyclin D1
(2,7,8),
E-cadherin (8), Bcl-2 (1), tumor necrosis factor (TNF)-α (9), nuclear factor (NF)-κB (10), transforming growth factor (TGF)-β
(11), matrix metalloproteinase
(MMP)-7 (12), cyclooxygenase
(COX)-2 (13,14), epidermal growth factor receptor
(EGFR) (15) and hypoxia-inducible
factor (HIF)-1α (16) may be used
as prognostic factors for ESCC. However, these studies included
patients treated with surgery or neoadjuvant chemoradiation therapy
(CRT). In the case of definitive CRT, the prognostic factors may be
different from those of surgery or neoadjuvant CRT. Unlike surgical
resection alone, which is not reliant on the therapeutic response,
and neoadjuvant CRT, which is able to achieve complete responses in
the majority of cases by resecting (even for cases without marked
responses), in definitive CRT it is important to be able to predict
therapeutic responses before starting treatment. Identifying
predictive parameters may aid the selection of primary therapies.
The present study was conducted using biopsy specimens excised from
patients prior to CCRT. The expression levels of 16 proteins were
analyzed to identify prognostic correlations in ESCC treated with
CCRT.
Patients and methods
Patients
A total of 10 patients who received CCRT for ESCC at
the University of Tokyo Hospital (Japan) between June 2000 and June
2010 were selected retrospectively. Only 10 patients (5 long-term
survivors and 5 who had succumbed to cancer) were selected and
examined, since this was a preliminary study to determine which
type of immunostaining should be used in the following larger
study. ESCC was confirmed histologically in all 10 patients. The
patients consisted of 4 cases of good responses and 6 recurrent
cases. The patients were staged according to the American Joint
Committee for Cancer Staging and End Results Reporting 1997 staging
system (17). The initial staging
consisted of a patient history and medical examination, routine
blood tests, chest X-rays, upper magnifying endoscopy, chest and
upper abdomen computerized tomography (CT), barium contrast X-rays
and pulmonary function tests. Bone scans and CT or magnetic
resonance imaging of the brain were performed only in cases of
clinical suspicion of metastases. Patients with technically
unresectable cancer, patients who refused to undergo surgery or
those considered medically unfit for surgery were eligible for
definitive CCRT.
The study was approved by the ethics committee of
the University of Tokyo, Tokyo, Japan. Informed consent was
obtained from all patients or the patient’s families.
CRT method
The details of the treatment method have been
previously reported (18–20). All patients received extended
elective nodal irradiation and were treated with 50–50.4 Gy
delivered at 1.8–2 Gy per fraction over 5–5.6 weeks. The clinical
target volume (CTV) was defined as the whole thoracic esophagus
(from the supra-clavicular fossae to the esophagogastric junction).
The CTV comprised the M1a and regional lymph nodes (LNs), including
positive LNs. The planning target volume was caluclated by adding
margins of 5–10 mm to the respective CTVs. The treatment planning
was entirely 3-dimensional. At least 4 fields were used (2
anterior-posterior opposed fields and 2 anterior-posterior oblique
opposed fields to remove the spinal cord from the radiation fields)
and 1 or 2 beams were added using the field-in-field technique if
necessary. Treatment was delivered by linear accelerators with 6–10
MV photons.
All patients received chemotherapy (CTx)
concurrently with irradiation. The CTx consisted of 2 cycles of
5-fluorouracil (800 mg/m2/day, days 1–4 and 29–32,
continuous) combined with nedaplatin (80 mg/m2, days 1
and 29, bolus) and standard techniques were used for hydration and
alkalization. The CTx began on the first day of irradiation. After
CCRT, in the adjuvant setting, an additional 1 or 2 cycles of the
same doses of CTx were administered to patients who had sufficient
bone marrow function and performance status and did not refuse
additional CTx.
Follow-up
Patients were followed up on a regular basis, with
visits at 1 month following treatment, every 3 months thereafter
during the first 2 years and every 6 months thereafter. Chest
X-rays were performed at every visit, while chest and upper abdomen
CT was performed every 6 months or more frequently at the suspicion
of tumor progression. When tumor growth was identified by CT and/or
PET, this was defined as local recurrence.
Immunohistochemistry (IHC)
Specimens obtained from biopsies under endoscopy
before the treatment were used. Tumor samples were fixed with 10%
formaldehyde in phosphate-buffered saline (PBS), embedded in
paraffin and 4-μm thick sections were prepared. The sections
were deparaffinized and pretreated with various methods, including
microwaving, EDTA and heating, that are known to be effective at
unmasking reactive sites for antibodies. The characteristics of the
16 primary antibodies used in IHC and their pretreatments are shown
in Table I. Subsequently, IHC
staining was performed with an automated IHC stainer. The slides
were then rinsed briefly in water and counterstained with
haematoxylin.
 | Table IImmunohistchemistry: characteristics
of the primary antibodies. |
Table I
Immunohistchemistry: characteristics
of the primary antibodies.
| Protein | Type | Source | Pretreatment | Titer | Incubation | Staining |
|---|
| p53 | Mouse MC | DO7 NCL-p53-DO7,
Leica | Microwave 1 mM EDTA
(pH 8.0) | 1:200 | 30 min, 37°C | Nucleus |
|
p21waf1 | Mouse MC | SNCL-WAF-1,
Novocastra | Heating (121°C, 15
min), citrate buffer (pH6.0) | 1:100 | Overnight, 4°C | Nucleus |
| MIB-1 | Mouse MC | MIB-1 M7240,
DAKO | Microwave, 1 mM EDTA
(pH 8.0) | 1:25 | 30 min, 37°C | Nucleus |
|
p16INK4A | Mouse MC | Z2117, Zeta | Heating (121°C, 15
min), citrate buffer (pH 6.0) | 1:200 | Overnight, 4°C | Cytoplasmic and
nucleus |
| cyclin D1 | Rabbit MC | SP4 RM-9104-S,
Thermo | Microwave, 1 mM EDTA
(pH 8.0) | 1:250 | 30 min, 37°C | Cytoplasmic |
| E-cadherin | Mouse MC | 36B5 NCL-E-Cad,
Leica | Microwave, 1 mM EDTA
(pH 8.0) | 1:25 | 30min, 37°C | Membrane
(cytoplasmic) |
| Bcl-2 | Mouse MC | 124 M0887, DAKO | Microwave, 1 mM EDTA
(pH 8.0) | 1:80 | 30 min, 37°C | Cytoplasmic |
| TNF-α | Mouse MC | 2C8 sc-52250, Santa
Cruz | Heating (121°C, 20
min), citrate buffer (pH 6.4) | 1:100 | Overnight, 4°C | Cytoplasmic |
| NF-κB | Rabbit PC | sc-7178, Santa
Cruz | Heating (121°C, 20
min), Citrate buffer (pH 6.0), | 1:1000 | Overnight, 4°C | Cytoplasmic |
| TGF-β1 | Rabbit PC | Y241,
Yanaihara | None | 1:200 | Overnight, 4°C | Cytoplasmic |
| MMP-7 | Rabbit PC | AB19135, Chemicon
International | None | 1:500 | Overnight, 4°C | Cytoplasmic |
| COX-2 | Rabbit PC | 18515, IBL | None |
0.5μg/ml | Overnight, 4°C | Cytoplasmic |
| EGFR | Mouse MC | K1492, DAKO | Proteinase K
(kit) | R-to-U | 30 min, RT | Membrane
(cytoplasmic) |
| HER2 | Rabbit PC | K5204, DAKO | Water bath (99°C),
citrate buffer (pH 6.0) | R-to-U | 30 min, RT | Membrane |
| ER | Mouse MC | 790-4325,
Roche | Microwave, 0.01 M
citrate buffer (pH 6.0) | 1:100 | 60 min, RT | Membrane
(cytoplasmic) |
| HIF-1α | Rabbit PC | 07-628,
MILLIPORE | None | 1:200 | Overnight, 4°C | Nucleus |
The level of expression was assessed
semi-quantitatively using the immunoreactive scoring (IRS) system
(21). The IRS score was determined
by considering the intensity, graded on a scale of 0–3 (0 = no
staining, 1 = weak staining, 2 = moderate staining and 3 = marked
staining) and extent (percentage of positive tumor cells) of
staining. The extent of staining was graded on a scale of 0–4 (0 =
no staining; 1 = 1–10% staining, 2 = 11–50% staining, 3 = 51–80%
staining and 4 = 81–100% staining). The IRS score (range, 0–12) was
the product obtained by multiplying the intensity and extent of
staining.
The IRS scores from 0–12 were interpreted as
follows: 0, negative; 1–4, weak; 5–8, moderate; and 9–12, markedly
positive.
The low and high cut-off values for the scores of
the biochemical markers were established as follows: i) p53,
p16INK4A, cyclin D1, E-cadherin, TGF-β, MMP-7, COX-2,
EGFR and HIF-1α: low, 0–2; high, 3–12; ii) Bcl-2 and HER2/neu: low,
0–8; high, 9–12; iii) MIB-1 (Ki-67): low, 0–3; high, 4–12; iv)
p21waf1, estrogen receptor (ER) and TNF-α: low, 0–3;
high, 4–12; and v) NF-κB: low, 0–11; high, 12.
Statistical analysis
Statistical analyses of the correlations between the
clinical results (alive vs. deceased, with vs. without local
recurrence and with vs. without disease) and molecular markers were
performed using Fisher’s exact test. The association between each
pair of proteins expressed was determined using the Pearson
product-moment correlation coefficient.
The Kaplan-Meier product-limit method was used to
estimate the probabilities of overall survival (OS), disease-free
survival (DFS) and locoregional recurrence-free survival, while the
log-rank test was used to estimate any differences. OS was
calculated in months from the first day of CCRT to the date of
mortality from any cause or to February 2012. Patients who remained
alive in February 2012 were censored. P<0.05 was considered to
indicate statistically significant differences.
Results
Patients
The characteristics of the 10 patients are shown in
Table II. The median age was 68.1
years (range, 46–80 years). The sub-sites of the primary tumors
included the middle (n=2) or lower (n=8) thoracic portions. The TNM
classifications were as follows: T1/T2/T3/T4, 2/3/5/0; N0/N1, 3/7;
M0/M1a/M1b, 7/0/3; and stages I/II/III/IV, 2/2/3/3, respectively.
The median follow-up for the 5 surviving patients was 76.2 (±24.8)
months.
| Table IIPatient charactaristics. |
Table II
Patient charactaristics.
| Patient no. | Age (years) | Gender | Primary site | Stage | cTNM | Hb (units) | BW loss (kg) | Dysphagia
score | Tumor length
(cm) | Differentiate | Chemotherapy total
cylcle | Radiation dose
(Gy) | Survival | Local
recurrence | Recurrence |
|---|
| 1 | 68 | Male | Lt | I | T1N0M0 | 14.8 | 0 | 0 | 7 | M/D | 2 | 50.4 | Alive | Without | Without |
| 2 | 70 | Male | Lt | I | T1N0M0 | 15.9 | 0 | 1 | 7 | P/D | 3 | 50 | Dead | Without | With |
| 3 | 46 | Male | Lt | IVB | T3N1M1b | 10.9 | 13 | 3 | 4 | P/D | 2 | 60 | Alive | Without | Without |
| 4 | 66 | Male | Lt | IIA | T3N0M0 | 10.9 | 0 | 3 | 3.5 | NA | 4 | 50.4 | Dead | Without | With |
| 5 | 80 | Male | Lt | III | T3N1M0 | 11.3 | 0 | 3 | 5 | W/D | 4 | 50.4 | Dead | Without | With |
| 6 | 70 | Female | Mt | IVB | T2N1M1b | 11.5 | 0 | 1 | 6 | W/D | 3 | 50.4 | Dead | With | With |
| 7 | 68 | Female | Lt | III | T3N1M0 | 12.1 | 0 | 0 | 4 | M/D | 4 | 50.4 | Alive | Without | Without |
| 8 | 79 | Male | Lt | III | T3N1M0 | 13.5 | 8 | 2 | 7 | P/D | 2 | 50.4 | Alive | Without | Without |
| 9 | 69 | Male | Mt | IVB | T2N1M1b | 11.6 | 0 | 1 | 2 | M/D | 2 | 50 | Dead | With | With |
| 10 | 65 | Male | Lt | IIB | T2N1M0 | 14.8 | 7 | 2 | NA | P/D | 4 | 60 | Alive | With | With |
IHC
Staining evaluations, (negative, weak, moderate or
marked for each of the 16 primary antibodies, were performed for
the 10 patients. The results may be summarized as follows (with the
numbers representing how many of the 10 patients showed expression
for the antibody): a) negative: 1 p16INK4A, 4 Bcl-2, 4
TNF-α, 1 EGFR, 5 HER2/neu and 4 ER; b) Moderate: 1 p53, 1
p21waf1, 3 MIB-1 (Ki-67), 1 p16INK4A, 1
cyclin D1, 2 E-cadherin, 4 TGF-β, 4 MMP-7, 6 COX-2, 4 EGFR and 4
HIF-1α; c) Strong: 7 p53, 1 p21waf1, 7 MIB-1 (Ki-67), 6
p16INK4A, 7 cyclin D1, 7 E-cadherin, 3 TGF-β, 6 MMP-7, 3
COX-2, 4 EGFR and 5 HIF-1α. In addition, correlation analysis
revealed the following results with respect to the pairs of
expression levels: p53 vs. cyclin D1, r=0.791, P=0.045; EGFR vs.
p53, r=0.803, P=0.0034; MIB-1 vs. p21, r=0.752, P=0.0097; HER2 vs.
ER, r=0.823, P=0.020; TNF-α vs. p21, r=0.739, P=0.012; TGF-β vs.
COX-2, r=0.714, P=0.018; TGFβ vs. HIF-1α, r=0.730, P=0.014; and
COX-2 vs. HIF-1α, r=0.794, P=0.0042.
Clinical outcome
Significant 2-year OS rates were observed for
patients with high (MIB-1 IRS ≥9) and low (MIB-1 IRS <9) MIB-1
levels (71 vs. 0%, P=0.019; Fig.
1A) and high (NF-κB IRS = 12) and low (NF-κB IRS <12) NF-κB
levels (0 vs. 100%, P<0.018; Fig.
1B). The correlations between the OS and expression levels of
p53, p21waf1, p16INK4A, cyclin D1,
E-cadherin, Bcl-2, TNF-α, TGF-β, MMP-7, COX-2, EGFR, HER2/neu, ER
and HIF-1α were not found to be significant (Table III).
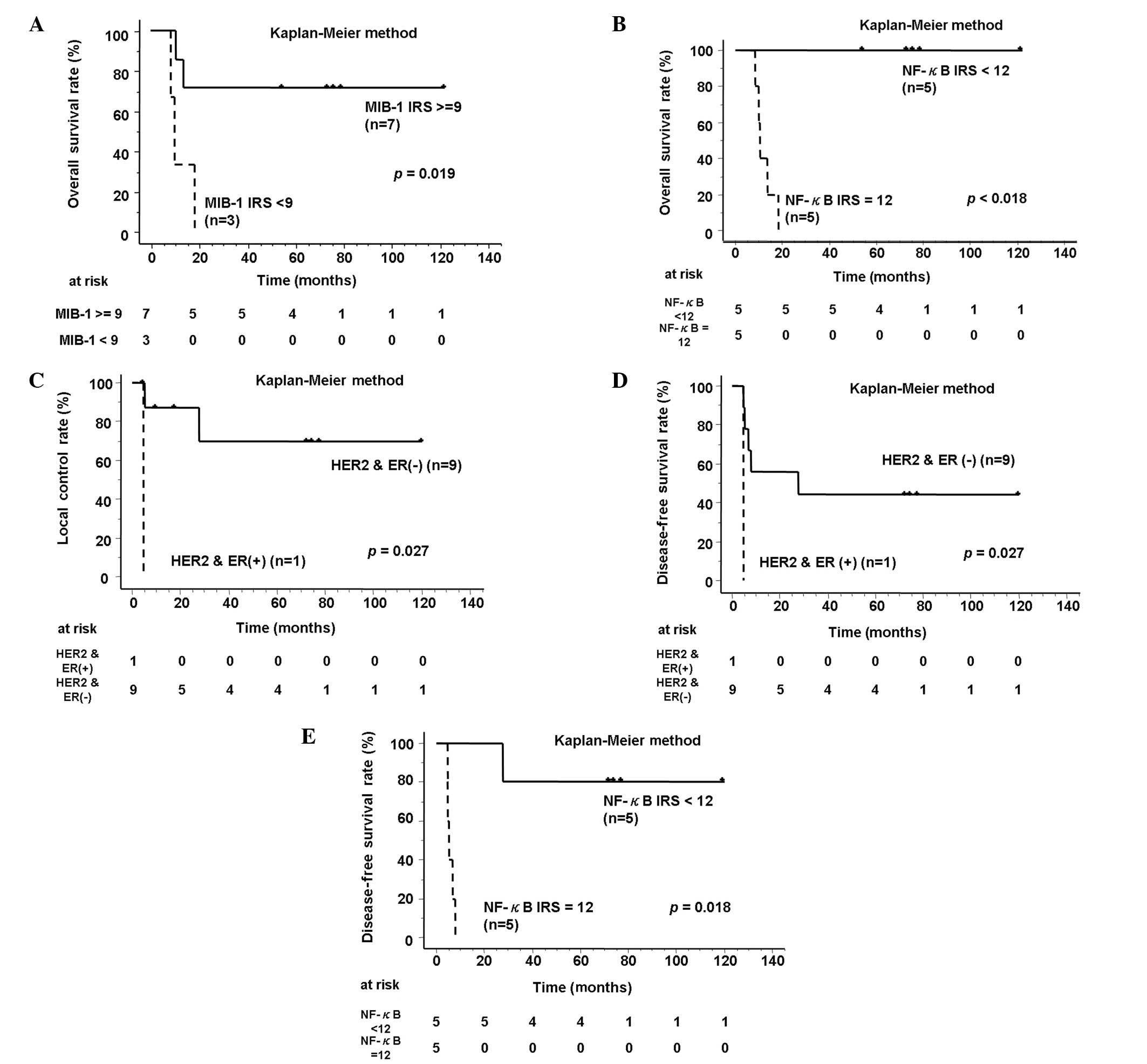 | Figure 1Survival curves for ESCC treated with
CCRT. (A) OS curves according to high (IRS ≥9) and low (IRS <9)
MIB-1 levels. (B) OS curves according to high (IRS = 12) and low
(IRS <12) NF-κB levels. (C) LC curves according to high
(HER2/neu IRS ≥3, ER IRS ≥4) and low (HER2/neu IRS = 1 or 2, ER IRS
<4) levels of both HER2/neu and the ER. (D) DFS curves according
to high and low levels of both HER2/neu and the ER. (E) DFS curves
according to both the high and low levels of NF-κB. ESCC,
esophageal squamous cell carcinoma; CCRT, concurrent chemoradiation
therapy; MIB-1, molecular immunology borstel-1; IRS, immunoreactive
score; OS, overall survival; NF-κB; nuclear factor-κB; LC, local
control; HER2/neu, human epidermal growth factor receptor type 2;
ER, estrogen receptor; DFS, disease-free survival. |
| Table IIIClinical outcome by the expression
levels of biomarkers. |
Table III
Clinical outcome by the expression
levels of biomarkers.
| IHC | IRS score | No. | 2-year OS | SD | P-value
log-rank | 2 year LC | SD | P-value
log-rank | 2 year DFS | SD | P-value
log-rank |
|---|
| Bcl-2 | | | | | | | | | | | |
| High | 3–12 | 3 | 67 | 27 | 0.55 | 67 | 27 | 0.19 | 67 | 27 | 0.85 |
| Low | 0–2 | 7 | 43 | 19 | | 83 | 15 | | 43 | 19 | |
| Cyclin D1 | | | | | | | | | | | |
| High | 6–12 | 7 | 43 | 19 | 0.38 | 69 | 19 | <0.19 | 43 | 19 | 0.32 |
| Low | 0–5 | 3 | 67 | 27 | | 100 | 0 | | 67 | 27 | |
| E-cadherin | | | | | | | | | | | |
| High | 6–12 | 8 | 50 | 18 | 0.76 | 73 | 17 | <0.90 | 50 | 18 | 0.75 |
| Low | 0–5 | 2 | 50 | 35 | | 100 | 0 | | 50 | 35 | |
| EGFR | | | | | | | | | | | |
| High | 6–12 | 5 | 60 | 22 | 0.57 | 80 | 18 | 0.75 | 60 | 22 | 0.67 |
| Low | 0–5 | 5 | 40 | 22 | | 80 | 18 | | 40 | 22 | |
| MIB-1 | | | | | | | | | | | |
| High | 9–12 | 7 | 71 | 17 | 0.019a | 71 | 17 | <0.83 | 71 | 17 | 0.90 |
| Low | 0–8 | 3 | 0 | 0 | | 100 | 0 | | 0 | 0 | |
| p53 | | | | | | | | | | | |
| High | 6–12 | 8 | 50 | 18 | 0.76 | 73 | 17 | <0.98 | 50 | 18 | 0.75 |
| Low | 0–5 | 2 | 50 | 35 | | 100 | 0 | | 50 | 35 | |
| HER2 | | | | | | | | | | | |
| High | 3–12 | 1 | 0 | 0 | 0.22 | 0 | 0 | 0.027a | 0 | 0 | 0.027a |
| Low | 0–2 | 9 | 56 | 17 | | 88 | 12 | | 56 | 17 | |
| ER | | | | | | | | | | | |
| High | 4–12 | 1 | 0 | 0 | 0.22 | 0 | 0 | 0.027a | 0 | 0 | 0.027a |
| Low | 0–3 | 9 | 56 | 17 | | 88 | 12 | | 56 | 17 | |
|
p16INK4A | | | | | | | | | | | |
| High | 6–12 | 7 | 50 | 18 | 0.75 | 75 | 15 | <0.23 | 50 | 17 | 0.95 |
| Low | 0–5 | 3 | 50 | 35 | | 100 | 0 | | 50 | 35 | |
| TNF-α | | | | | | | | | | | |
| High | 4–12 | 0 | - | - | - | - | - | - | - | - | - |
| Low | 0–3 | 10 | - | - | - | - | - | - | - | - | - |
|
p21waf1 | | | | | | | | | | | |
| High | 4–12 | 6 | 50 | 20 | 0.70 | 67 | 19 | <0.16 | 50 | 20 | 0.65 |
| Low | 0–3 | 4 | 50 | 25 | | 100 | 0 | | 50 | 25 | |
| TGF-β | | | | | | | | | | | |
| High | 6–12 | 7 | 44 | 17 | <0.17 | 76 | 15 | 0.34 | 44 | 17 | 0.19 |
| Low | 0–5 | 3 | 100 | 0 | | 100 | 0 | | 100 | 0 | |
| NF-κB | | | | | | | | | | | |
| High | 12 | 5 | 0 | 0 | <0.0018a | 53 | 25 | 0.11 | 0 | 0 | 0.0018a |
| Low | 0–11 | 5 | 100 | 0 | | 100 | 0 | | 80 | 18 | |
| MMP-7 | | | | | | | | | | | |
| High | 6–12 | 9 | 44 | 17 | <0.90 | 76 | 15 | <0.66 | 44 | 17 | <0.92 |
| Low | 0–5 | 1 | 100 | 0 | | 100 | 0 | 100 | 0 | | |
| COX-2 | | | | | | | | | | | |
| High | 6–12 | 7 | 43 | 19 | 0.38 | 69 | 19 | 0.93 | 43 | 19 | 0.88 |
| Low | 0–5 | 3 | 67 | 27 | | 100 | 0 | | 67 | 27 | |
| HIF-1α | | | | | | | | | | | |
| High | 6–12 | 7 | 29 | 17 | <0.19 | 69 | 19 | 0.74 | 29 | 17 | 0.19 |
| Low | 0–5 | 3 | 100 | 0 | | 100 | 0 | | 67 | 27 | |
The 2-year local control rates were 0 vs. 88% (±12%,
P=0.027; Fig. 1C) for patients with
high (HER2/neu IRS ≥3, ER IRS ≥4) and low (HER2/neu IRS ≤2, ER IRS
<4) levels of both HER2/neu and ER. The 2-year DFS rates of the
same patients were 0 vs. 56% (±17%; P=0.027; Fig. 1D) and 0 vs. 80% (±18%; P=0.018;
Fig. 1E) for patients with high and
low levels of NF-κB, respectively. No significant correlations were
observed between the expression levels of the other 12 proteins and
clinical outcomes (Table III).
Discussion
The clinical outcomes of 10 ESCC patients treated
with radical CCRT were correlated with 16 molecular biomarkers. The
present retrospective study was performed on patients treated
between 2000 and 2010. A number of previous studies were designed
for patients treated with radical surgery or preoperative CCRT
(1–16). The present study is the first to
conduct a comprehensive analysis of 16 proteins simultaneously in
patients treated with definitive CCRT-alone. Additionally, the
study showed for the first time that 4 biomarkers, including MIB-1,
NF-κB, HER2 and ER, are prognostic factors for ESCC treated with
CCRT.
In the present study, 10 patients were treated using
a standard CCRT regimen. The 2-year OS, local control (LC) and DFS
rates were all 50% and these results were comparable to previous
reports (18–20). There was little difference in the
clinical backgrounds between the 6 living and 4 deceased patients.
In the cases of higher MIB-1 expression, the OS was significantly
improved following definitive CCRT. In the cases with lower NF-κB
expression, the OS and DFS rates were significantly improved
following definitive CCRT. In the cases of lower HER2 and ER
levels, the LC and DFS rates were significantly improved following
definitive CCRT. TNF-α showed negative or extremely weak staining
in all cases. There was no correlation between MIB-1 and NF-κB,
which were independent prognostic factors. There was a strong
correlation between HER2 and ER. All patients with high/low HER2
expression also expressed high/low ER. The results of the HER2
staining were entirely in accordance with those of ER.
MIB-1 monoclonal antibody recognizes proliferating
cells in the G1, S, G2 and M phases of the cell cycle (22). The correlation between a high MIB-1
index and poor prognosis is well known in breast cancer (23). However, in the present study, in the
cases of higher MIB-1 expression, the OS was significantly improved
following definitive CCRT. Ressiot et al(5) concluded that the over-expression of
MIB-1 was a significant factor for complete endoscopic response
following CCRT in 56 patients with esophageal cancer, which is
similar to the present results. The correlation between MIB-1
expression and a good response to CCRT is explained by the fact
that MIB-1 expression is a marker of cellular proliferation.
NF-κB is a protein complex that controls the
transcription of DNA. TNF-α and other transcription factors
activate NF-κB. NF-κB activates interleukin (IL)-1 and others and
is therefore involved in apoptosis or inflammation. Blocking NF-κB
causes tumor cells to stop proliferating, die or become more
sensitive to the action of antitumor agents. Thus, NF-κB is the
subject of much active research among pharmaceutical companies as a
target for anticancer therapy (24). Izzo et al(10) reported that activated NF-κB prior to
therapy in 80 patients with esophageal cancer was associated with
the lack of a complete pathological response, which supports the
present result showing that patients with high expression levels of
NF-κB had significantly poorer OS and DFS rates than those showing
low levels.
HER2 is a member of the EGFR family which is
involved in the complex regulation of cell growth, proliferation
and survival. HER2 protein has been implicated in the development
of cancer. In addition to breast cancer, HER2 overexpression and
gene amplification have also been reported in carcinomas of the
colon, bladder, ovary, endometrium, lung, head and neck, esophagus
and stomach (25). Akamatsu et
al(26) reported that HER2
immunostaining was suitable for predicting resistance to CRT in 34
patients with ESCC. Additionally, according to Mimura et
al(27), the survival rate of
66 patients with ESCC showing HER2 gene amplification was
significantly worse than those without amplification.
The main function of ER is as a DNA-binding
transcription factor regulating gene expression. Estrogen and ER
have also been implicated in breast, ovarian, colon, prostate and
endometrial cancer. Wang et al(28) suggested that ER expression may
predict a better outcome for patients with ESCC.
These results concurred with the present results
where patients showing high staining for HER2 and ER had
significantly poorer LC and DRS rates than those with low staining.
Estrogen promotes tumor proliferation through ER and in cells with
overexpression of HER2, tumor proliferation is considered to be
increased. The present result demonstrating that the prognosis of
cases with overexpression of ER or HER2 was worse is therefore
understandable.
In the present study, p53, p21waf1,
p16INK4A, cyclin D1, E-cadherin, Bcl-2, TNF-α, TGF-β,
MMP-7, COX-2, EGFR and HIF-1α were also investigated. The p53 gene
is one of the well-known anti-oncogenes involved in apoptosis and
the cell cycle (29–31). Also, the p21 and the
p16INK4A proteins are involved in the cell cycle and
induce G1 arrest. Cyclin D1 is a member of the cyclin protein
family involved in regulating cell cycle progression. Bcl-2 is a
member of the anti-apoptotic family (32,33).
E-cadherin is important in cell adhesion and loss of E-cadherin
function or expression has been implicated in cancer progression
and metastasis. TGF-β is important in stopping the proliferation of
normal epithelial cells and promoting the invasion of cancer cells.
TNF, being an endogenous pyrogen, is able to induce fever,
apoptotic cell death, sepsis through IL-1 and 6 production,
cachexia and inflammation, as wells as inhibit tumorigenesis and
viral replication. The expression of COX-2 is induced by several
stimuli, including growth factors, inflammation and cytokines.
COX-2 is upregulated in numerous types of cancer (34). EGFR is the cell-surface receptor for
epidermal growth factors and is a growth factor involved in the
regulation of cell growth, proliferation and differentiation.
Proteins of the MMP family are involved in the breakdown of the
extracellular matrix in normal physiological processes, such as
embryonic development, reproduction and tissue remodeling, as well
as in disease processes, such as arthritis and metastasis (35). HIF-1α is a transcription factor that
responds to changes in available oxygen in the cellular
environment, particularly to decreases in oxygen or hypoxia
(36). In the present study, these
cancer growth-causing proteins did not appear to be prognostic
factors for ESCC treated with CCRT.
However, the present study had a number of
limitations. Firstly, the power may be poor since it involved only
10 patients in a retrospective setting. Secondly, the IHC method
used was only able to examine protein expression levels and DNA
mutation and amplification were not examined as with the polymerase
chain reaction method.
We expect to continue these studies, thereby
increasing the number of cases in a retrospective setting and
confirming the conclusions of the present study.
In the present study, high levels of MIB-1 and NF-κB
and low levels of HER2 and ER were good prognostic factors
following definitive CCRT for ESCC. There was no significant
correlation between the expression levels of the other proteins
(p53, p21waf1, p16INK4A, cyclin D1,
E-cadherin, Bcl-2, TNF-α, TGF-β, MMP-7, COX-2, EGFR and HIF-1α) and
clinical outcomes.
References
|
1
|
Sarbia M, Stahl M, Fink U, Willers R,
Seeber S and Gabbert HE: Expression of apoptosis-regulating
proteins and outcome of esophageal cancer patients treated by
combined therapy modalities. Clin Cancer Res. 4:2991–2997.
1998.PubMed/NCBI
|
|
2
|
Takeuchi H, Ozawa S, Ando N, Kitagawa Y,
Ueda M and Kitajima M: Cell-cycle regulators and the Ki-67 labeling
index can predict the response to chemoradiotherapy and the
survival of patients with locally advanced squamous cell carcinoma
of the esophagus. Ann Surg Oncol. 10:792–800. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Makino T, Yamasaki M, Miyata H, Yoshioka
S, Takiguchi S, Fujiwara Y, Nakajima K, Nishida T, Mori M and Doki
Y: p53 Mutation status predicts pathological response to
chemoradiotherapy in locally advanced esophageal cancer. Ann Surg
Oncol. 17:804–811. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ishida M, Morita M, Saeki H, Ohga T,
Sadanaga N, Watanabe M, Kakeji Y and Maehara Y: Expression of p53
and p21 and the clinical response for hyperthermochemoradiotherapy
in patients with squamous cell carcinoma of the esophagus.
Anticancer Res. 27:3501–3506. 2007.PubMed/NCBI
|
|
5
|
Ressiot E, Dahan L, Liprandi A, Giorgi R,
Djourno XB, Padovani L, Alibert S, Ries P, Laquière A, Laugier R,
Thomas P and Seitz JF: Predictive factors of the response to
chemoradiotherapy in esophageal cancer. Gastroenterol Clin Biol.
32:567–577. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Malik SM, Nevin DT, Cohen S, Hunt JL and
Palazzo JP: Assessment of immunohistochemistry for p16INK4 and
high-risk HPV DNA by in situ hybridization in esophageal squamous
cell carcinoma. Int J Surg Pathol. 19:31–34. 2011.PubMed/NCBI
|
|
7
|
Sarbia M, Stahl M, Fink U, Heep H,
Dutkowski P, Willers R, Seeber S and Gabbert HE: Prognostic
significance of cyklin D1 in esophageal squamous cell carcinoma
patients treated with surgery alone or combined therapy modalities.
Int J Cancer. 84:86–91. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
No authors listed:. Prognostic
significance of CyclinD1 and E-Cadherin in patients with esophageal
squamous cell carcinoma: multiinstitutional retrospective analysis.
Research Committee on Malignancy of Esophageal Cancer, Japanese
Society for Esophageal Diseases. J Am Coll Surg. 192:708–718. 2001.
View Article : Google Scholar
|
|
9
|
Kuwahara A, Yamamori M, Fujita M, Okuno T,
Tamura T, Kadoyama K, Okamura N, Nakamura T and Sakaeda T: TNFRSF1B
A1466G genotype is predictive of clinical efficacy after treatment
with a definitive 5-fluorouracil/cisplatin-based chemoradiotherapy
in Japanese patients with esophageal squamous cell carcinoma. J Exp
Clin Cancer Res. 29:1002010. View Article : Google Scholar
|
|
10
|
Izzo JG, Correa AM, Wu TT, Malhotra U,
Chao CK, Luthra R, Ensor J, Dekovich A, Liao Z, Hittelman WN,
Aggarwal BB and Ajani JA: Pretherapy nuclear factor-kappaB status,
chemoradiation resistance, and metastatic progression in esophageal
carcinoma. Mol Cancer Ther. 5:2844–2850. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Pühringer-Oppermann F, Sarbia M, Ott N and
Brücher BL: The predictive value of genes of the TGF-beta1 pathway
in multi-modally treated squamous cell carcinoma of the esophagus.
Int J Colorectal Dis. 25:515–521. 2010.PubMed/NCBI
|
|
12
|
Yamashita K, Mori M, Shiraishi T, Shibuta
K and Sugimachi K: Clinical significance of matrix
metalloproteinase-7 expression in esophageal carcinoma. Clin Cancer
Res. 6:1169–1174. 2000.PubMed/NCBI
|
|
13
|
Takatori H, Natsugoe S, Okomura H,
Matsumoto M, Ishigami S, Owaki T and Aikou T: Predictive value of
COX-2 for the effect of chemoradiotherapy on esophageal squamous
cell carcinoma. Oncol Rep. 13:697–701. 2005.PubMed/NCBI
|
|
14
|
Akutsu Y, Hanari N, Yusup G,
Komatsu-Akimoto A, Ikeda N, Mori M, Yoneyama Y, Endo S, Miyazawa Y
and Matsubara H: COX2 expression predicts resistance to
chemoradiotherapy in esophageal squamous cell carcinoma. Ann Surg
Oncol. 18:2946–2951. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Gotoh M, Takiuchi H, Kawabe S, Ohta S, Kii
T, Kuwakado S and Katsu K: Epidermal growth factor receptor is a
possible predictor of sensitivity to chemoradiotherapy in the
primary lesion of esophageal squamous cell carcinoma. Jpn J Clin
Oncol. 37:652–657. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ogawa K, Chiba I, Morioka T, Shimoji H,
Tamaki W, Takamatsu R, Nishimaki T, Yoshimi N and Murayama S:
Clinical significance of HIF-1alpha expression in patients with
esophageal cancer treated with concurrent chemoradiotherapy.
Anticancer Res. 31:2351–2359. 2011.
|
|
17
|
Greene FL, Page DL, Fleming ID, Fritz AG,
Balch CM, Haller DG and Morrow M: AJCC Cancer Staging Handbook. 5th
edition. Lippincott-Raven; Philadelphia, PA: 1997
|
|
18
|
Yamashita H, Okuma K, Wakui R,
Kobayashi-Shibata S, Ohtomo K and Nakagawa K: Details of recurrence
sites after elective nodal irradiation (ENI) using 3D-conformal
radiotherapy (3D-CRT) combined with chemotherapy for thoracic
esophageal squamous cell carcinoma - a retrospective analysis.
Radiother Oncol. 98:255–260. 2011. View Article : Google Scholar
|
|
19
|
Yamashita H, Okuma K, Seto Y, Mori K,
Kobayashi S, Wakui R, Ohtomo K and Nakagawa K: A retrospective
comparison of clinical outcomes and quality of life measures
between definitive chemoradiation alone and radical surgery for
clinical stage II–III esophageal carcinoma. J Surg Oncol.
100:435–441. 2009.PubMed/NCBI
|
|
20
|
Yamashita H, Nakagawa K, Yamada K,
Kaminishi M, Mafune K and Ohtomo K: A single institutional
non-randomized retrospective comparison between definitive
chemoradiotherapy and radical surgery in 82 Japanese patients with
resectable esophageal squamous cell carcinoma. Dis Esophagus.
21:430–436. 2008. View Article : Google Scholar
|
|
21
|
Krajewska M, Krajewski S, Epstein JI,
Shabaik A, Sauvageot J, Song K, Kitada S and Reed JC:
Immunohistochemical analysis of bcl-2, bax, bcl-X, and mcl-1
expression in prostate cancers. Am J Pathol. 148:1567–1576.
1996.PubMed/NCBI
|
|
22
|
Scholzen T and Gerdes J: The Ki-67
protein: from the known and the unknown. J Cell Physiol.
182:311–322. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Yerushalmi R, Woods R, Ravdin PM, Hayes MM
and Gelmon KA: Ki67 in breast cancer: prognostic and predictive
potential. Lancet Oncol. 11:174–183. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Escárcega RO, Fuentes-Alexandro S,
García-Carrasco M, Gatica A and Zamora A: The transcription factor
nuclear factor-kappa B and cancer. Clin Oncol (R Coll Radiol).
19:154–61. 2007.
|
|
25
|
Koltz BR, Hicks DG and Whitney-Miller CL:
HER2 testing in gastric and esophageal adenocarcinoma: new
diagnostic challenges arising from new therapeutic options. Biotech
Histochem. 87:40–45. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Akamatsu M, Matsumoto T, Oka K, Yamasaki
S, Sonoue H, Kajiyama Y, Tsurumaru M and Sasai K: c-erbB-2
oncoprotein expression related to chemoradioresistance in
esophageal squamous cell carcinoma. Int J Radiat Oncol Biol Phys.
57:1323–1327. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Mimura K, Kono K, Hanawa M, Mitsui F,
Sugai H, Miyagawa N, Ooi A and Fujii H: Frequencies of HER-2/neu
expression and gene amplification in patients with oesophageal
squamous cell carcinoma. Br J Cancer. 92:1253–1260. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Wang QM, Yuan L, Qi YJ, Ma ZY and Wang LD:
Estrogen analogues: promising target for prevention and treatment
of esophageal squamous cell carcinoma in high risk areas. Med Sci
Monit. 16:HY19–HY22. 2010.PubMed/NCBI
|
|
29
|
Lane DP: A death in the life of p53.
Nature. 362:786–787. 1993. View
Article : Google Scholar : PubMed/NCBI
|
|
30
|
Xiong Y, Hannon GJ, Zhang H, Casso D,
Kobayashi R and Beach D: p21 Is a universal inhibitor of cyclin
kinase. Nature. 366:701–704. 1993. View
Article : Google Scholar : PubMed/NCBI
|
|
31
|
el-Deiry WS, Harper JW, O’Connor PM,
Velculescu VE, Canman CE, Jackman J, Pietenpol JA, Burrell M, Hill
DE and Wang Y: WAF1/CIP1 is induced in p53-mediated G1 arrest and
apoptosis. Cancer Res. 54:1169–1174. 1994.PubMed/NCBI
|
|
32
|
Oltvai ZN, Milliman CL and Korsmeyer SJ:
Bcl-2 heterodimerizes in vivo with a conserved homolog, Bax, that
accelerates programmed cell death. Cell. 74:609–619. 1993.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Adams JM and Cory S: The Bcl-2 protein
family: arbiters of cell survival. Science. 281:1322–1326. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Legan M: Cyclooxygenase-2, p53 and glucose
transporter-1 as predictors of malignancy in the development of
gallbladder carcinomas. Bosn J Basic Med Sci. 10:192–196.
2010.PubMed/NCBI
|
|
35
|
Ii M, Yamamoto H, Adachi Y, Maruyama Y and
Shinomura Y: Role of matrix metalloproteinase-7 (matrilysin) in
human cancer invasion, apoptosis, growth, and angiogenesis. Exp
Biol Med (Maywood). 231:20–27. 2006.PubMed/NCBI
|
|
36
|
Smith TG, Robbins PA and Ratcliffe PJ: The
human side of hypoxia-inducible factor. Br J Haematol. 141:325–334.
2008. View Article : Google Scholar : PubMed/NCBI
|














