Introduction
Bladder cancer is the most common tumor of the
urinary system. In 2010, bladder cancer was the third and
thirteenth most commonly diagnosed type of cancer in males and
females, respectively, in Poland (1).
Various carcinogenesis pathways in bladder cells
have been proposed, including one which assumes that a single
distinct molecular pathway exists for low-grade non-invasive tumors
and another exists for muscle-invasive tumors. The first type of
tumor develops from hyperplasia, and is characterized by molecular
alternations in the RAF/MEK/ERK and PIK3CA signal transduction
pathways, while the second, the muscle-invasive tumor type,
progresses from a dysplastic urothelium that is characterized by
disruptions in the RB and p53 signaling pathways
(2). Furthermore, chromosomal
aberrations at a number of sites, including 1q, 5p, 17p, 3p, 13q,
18q and 10q are involved during carcinogenesis in bladder tissue.
Epigenetic regulation of gene expression is also common and
predominantly affects genes associated with tumor development and
survival, such as RUNX3, RASSF1A, p16, RARβ and CDH1
(2–5).
Genetic mapping and DNA sequencing has revealed the
role of loss of heterozygosity (LOH) on chromosome 16 in the
development of bladder cancer. Yoon et al (6) reported allelic loss at 16q24 in 20–45%
of bladder tumors. This region overlaps with the fragile
chromosomal site, FRA16D where the tumor suppressor gene,
WWOX is located. Alterations in WWOX expression have
been reported in various types of cancer, including breast
(7), prostate (8), ovarian (9) and bladder cancer (10–12).
However, the mechanisms responsible for the loss of WWOX
expression remain unclear. The WWOX gene is not considered
to be a classical tumor suppressor; for example, the two-hit model
of cancer development, proposed by Knudson in 1985 (13), is not applicable. The susceptibility
of WWOX to LOH, due to a location in a common fragile site,
indicates that haploinsufficiency is a primary reason for reduced
WWOX expression levels (14,15).
Furthermore, epigenetic mechanisms have been proposed to be crucial
in the regulation of WWOX expression (14).
The WWOX (WW-domain containing oxidoreductase)
protein contains two N-terminal WW domains of protein-protein
interactions and a C-terminal short-chain dehydrogenase domain
(7). Numerous WWOX protein
partners have been identified among the critical members of signal
transduction pathways; proteins such as ERBB4 (16,17),
JUN (18), TP73 (19), RUNX (20) and EZR (21).
In healthy tissues, high WWOX expression
levels have been observed in endocrine organs, including the
prostate, testis and mammary glands, which indicates involvement in
sex hormone metabolism and the regulation of steroid signaling
pathways (22). Furthermore,
Aqeilan et al (23) observed
that the WWOX gene is involved in the regulation of
steroidogenesis and proper functioning of the gonads, i.e. the
testis and ovary. WWOX knock-out mice exhibit downregulated
expression of genes coding for enzymes in the cytochrome P450
family, including renin 1 structural and carbonyl reductase 2.
The aim of the present study was to analyze the
alterations in mRNA expression levels of selected genes associated
with proliferation (MKI67), apoptosis (BCL2,
BAX and BIRC5), the cell cycle (CCND1 and
CCNE1), signal transduction (EGFR and VEGF)
and tumor suppression (WWOX) in bladder tumor samples, and
to identify any association between gene expression levels and
clinicopathological factors, such as gender, grade or stage. The
roles of promoter methylation status and LOH in the regulation of
WWOX expression were also investigated.
Materials and methods
Tissue samples
Papillary urothelial cancer tissues were obtained
from 32 patients treated at the Kopernik Hospital (Lodz, Poland)
between 2003 and 2007. All patients had undergone transurethral
resection of bladder tumors. The tumor tissue samples were stored
at −80°C in RNAlater buffer (Ambion®; Thermo Fisher
Scientific, Waltham, MA, USA).
The experimental group consisted of 26 males and six
females. The tumors were graded according to the World Health
Organization classification of Tumors (2004) (24) and staged using the tumor, node,
metastasis (TNM) classification system. In the sample population,
16 tumors were classified as grade 1, nine as grade 2, three as
grade 3 and four were unclassified. According to the TNM
classification, 19 cases were non-invasive papillary carcinoma,
five were T1, two were T2, one was T3 and five were unclassified.
This study was conducted according to the Declaration of Helsinki
and was approved by the Ethics Committee of the Medical University
of Lodz (RMM/115/12/KE). Consent was obtained from the families of
the patients.
RNA and DNA isolation, and cDNA
synthesis
RNA was isolated from the frozen tissue samples
using TRIzol® reagent (Invitrogen Life Technologies,
Carlsbad, CA, USA). Reverse transcriptase from the ImProm Reverse
Transcription (RT)-II™ system (Promega Corporation, Madison, WI,
USA) was used to transcribe 10 μg total RNA to cDNA to obtain a
final volume of 100 μl. The RT reaction was performed under the
following conditions: Primer annealing at 25°C for 5 min, and
elongation at 42°C for 60 min, followed by a 15 min pause in the
reaction at 70°C. Following synthesis, 50 μl deionized water was
added to each sample, which were stored at −20°C. Subsequent to RNA
isolation, DNA was recovered using 0.5 ml back extraction buffer
containing 1 M Tris Base, 4 M guanidinium thiocyanate and 50 mM
sodium citrate, according to the manufacturer’s instructions.
RT-quantitative polymerase chain reaction
(qPCR)
Gene expression levels were analyzed using
Rotor-Gene™ 6000 (Corbett Research, Cambridge, UK). The reaction
products were detected using SYBR® Green I and a qPCR
Core kit for SYBR® Green I (Eurogentec, Southampton,
UK). Each reaction was performed in duplicate. The expression
levels of the following genes were analyzed: WWOX,
MKI67, BAX, BCL2, BIRC5, EGFR,
VEGF, CCND1, and CCNE1 and the results were
compared with the expression levels of the RPS17, H3F3A and
RPLP0 reference genes. The primer sequences, PCR reaction
conditions and the length of the obtained products are listed in
Table I. Due to the low levels of
the WWOX gene present in the tissue samples, semi-nested
RT-qPCR was performed.
 | Table IRT-PCR primer sequences. |
Table I
RT-PCR primer sequences.
| Primer sequences
(5′-3′) | Product length
(bp) | Annealing
temperature °(C) | Detection
temperature (°C) |
|---|
| H3F3A | 76 | 65 | 72 |
| F:
AGGACTTTAAAACAGATCTGCGCTTCCAGAG | | | |
| R:
ACCAGATAGGCCTCACTTGCCTCCTGC | | | |
| RPLP0 | 69 | 65 | 72 |
| F:
ACGGATTACACCTTCCCACTTGCTGAAAAGGTC | | | |
| R:
AGCCACAAAGGCAGATGGATCAGCCAAG | | | |
| RPS17 | 87 | 64 | 72 |
| F:
AAGCGCGTGTGCGAGGAGATCG | | | |
| R:
TCGCTTCATCAGATGCGTGACATAACCTG | | | |
| MK167 | 156 | 56 | 81 |
| F:
TCCTTTGGTGGGCACCTAAGACCTG | | | |
| R:
TGATGGTTGAGGCTGTTCCTTGATG | | | |
| BAX | 137 | 56 | 81 |
| F:
AGAGGTCTTTTTCCGAGTGGCAGC | | | |
| R:
TTCTGATCAGTTCCGGCACCTTG | | | |
| BCL2 | 122 | 56 | 81 |
| F:
TTGGCCCCCGTTGCTTTTCCTC | | | |
| R:
TCCCACTCGTAGCCCCTCTGCGAC | | | |
| BIRC5 | 83 | 65 | 72 |
| F:
AGTGTTTCTTCTGCTTCAAGGAGCTGGAAG | | | |
| R:
ACCGGACGAATGCTTTTTATGTTCCTCTATG | | | |
| EGFR | 106 | 58 | 81 |
| F:
AGCTTCTTGCAGCGATACAGCTCAGAC | | | |
| R:
TGGGAACGGACTGGTTTATGTATTCAGG | | | |
| VEGF | 267 | 60 | 72 |
| F:
TGCTGTAGGAAGCTCATCTC | | | |
| R:
ATCACGAAGTGGTGAAGTTC | | | |
| CCND1 | 160 | 03 | 86 |
| F:
TGTCCTACTACCGCCTCACACGCTTCCTCTCCAG | | | |
| R:
TCCTCTTCCTCCTCCTCGGCGGCCTTG | | | |
| CCNE1 | 138 | 68 | 68 |
| F:
TTCTTGAGCAACACCCTCTTCTGCAGCC | | | |
| R:
TCGCCATATACCGGTCAAAGAAATCTTGTGCC | | | |
| WWOX |
| I step | 171 | 63 | 72 |
| F:
TGCAACATCCTCTTCTCCAACGAGCTGCAC | | | |
| R:
TCCCTGTTGCATGGACTTGGTGAAAGGC | | | |
| II step | 150 | 63 | 77 |
| F:
GAGCTGCACCGTCGCCTCTCCCCAC | | | |
| R:
TCCCTGTTGCATGGACTTGGTGAAAGGC | | | |
The primer sequences and the PCR conditions have
been described in previous studies (25,26).
Briefly, PCR cycling included one cycle at 95°C for 10 min
(denaturation) followed by 35 cycles at 94°C for 30 sec (repeated
denaturation); 56°C (for D16S3096) or 55°C (for D16S518) for 30 sec
(annealing), and 72°C for 60 sec (elongation). In order to avoid
detection of non-specific products for each reaction, melting curve
analysis was performed and the expression levels of the genes were
calculated according to the Roche method (27). Universal Human Reference RNA
(Stratagene, La Jolla, CA, USA) at a concentration of 0.5 mg/ml
served as a calibrator.
LOH analysis
Allelic losses were analyzed by high resolution
melting using a LightCycler® 480 (Roche Diagnostics
GmbH, Mannheim, Germany). Two microsatellite markers, located on
chromosome 16 in two intron regions of the WWOX gene, were
used: D16S3096 and D16S518 on introns 8 and 1, respectively.
Information regarding the sequences for these microsatellite
markers was obtained from the Genome Database (www.ncbi.nlm.nih.gov/probe?term=45798[unists+id];
www.ncbi.nlm.nih.gov/probe/?term=d16s518).
PCR cycling included one cycle at 95°C for 10 min,
followed by 35 cycles at 94°C for 30 sec, 56°C (for D16S3096) or
55°C (for D16S518) for 30 sec, and 72°C for 60 sec.
Methylation analysis of the WWOX
gene
The methylation status of two fragments of the
WWOX gene was analyzed; the first site in the promoter
region between −508 and −174 bp, and the second between −171 and
+239 bp, covering the 3′ end of the promoter and part of exon 1.
The procedures for genomic DNA extraction, digestion and performing
a MethylScreen™ assay (New England Biolabs, Hitchin, UK) have
previously been described (25,26).
Statistical analysis
A nonparametric Spearman linear correlation test was
used in the analysis of the correlation between gene expression
levels. The analysis of the dependence between WWOX gene
expression levels and LOH, as well as methylation status and
various clinical factors, was performed using the Aspin-Welsh test.
P<0.05 was considered to indicate a statistically significant
difference.
Results
LOH analysis
D16S518 and D16S3096 LOH was observed in 64.5 and
25.8% bladder cancer samples, respectively. Assuming that the
population homozygosity values are 17% for D16S518 and 26% for
D16S3096, according to the Genome Database, the predicted LOH were
47.5 and 0%, respectively. No correlation was observed between the
LOH for either microsatellite loci, D16S518 or D16S3096, and the
expression levels of the WWOX gene (P>0.05).
WWOX methylation status
MethylScreen™ analysis revealed WWOX
methylation in the −508 to −174 bp promoter region in 31% of
bladder cancer specimens. Furthermore, WWOX expression
levels in the methylated samples were almost half those of the
unmethylated samples (means ± standard error of the mean [SE],
0.47±0.04 methylated vs. 0.90±0.14 unmethylated; P<0.05).
Correlation between LOH and WWOX
methylation status
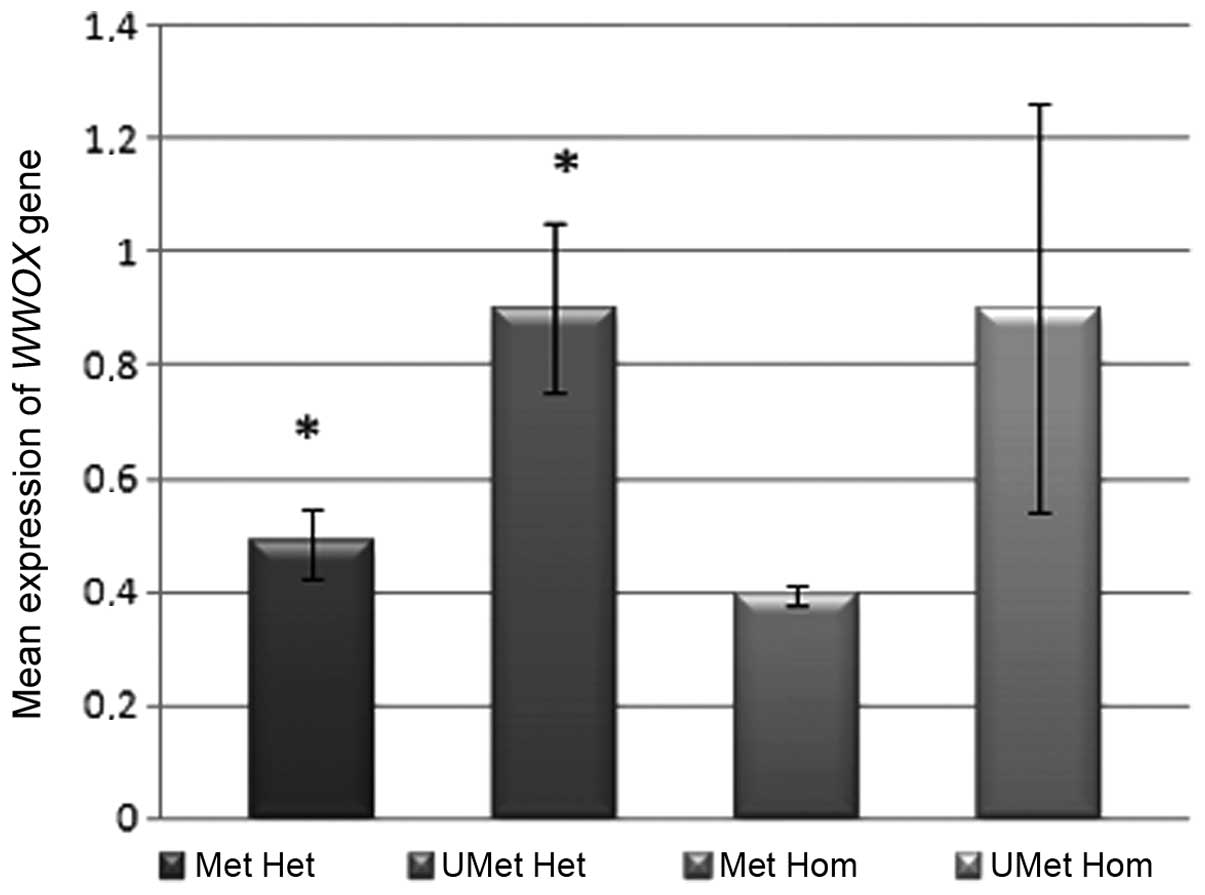
Promoter methylation in the −508 to −174 bp fragment
appeared to reduce the expression levels of the WWOX gene in
hetero- and homozygous cases of D16S3096 (Fig. 1). However, a statistically
significant difference in the WWOX gene expression levels
was observed between the heterozygous, unmethylated and the
heterozygous, methylated samples (means ± SE, 0.90±0.15 vs.
0.49±0.06 respectively; P=0.019) at the D16S3096 locus, however,
not at the D16S518 locus.
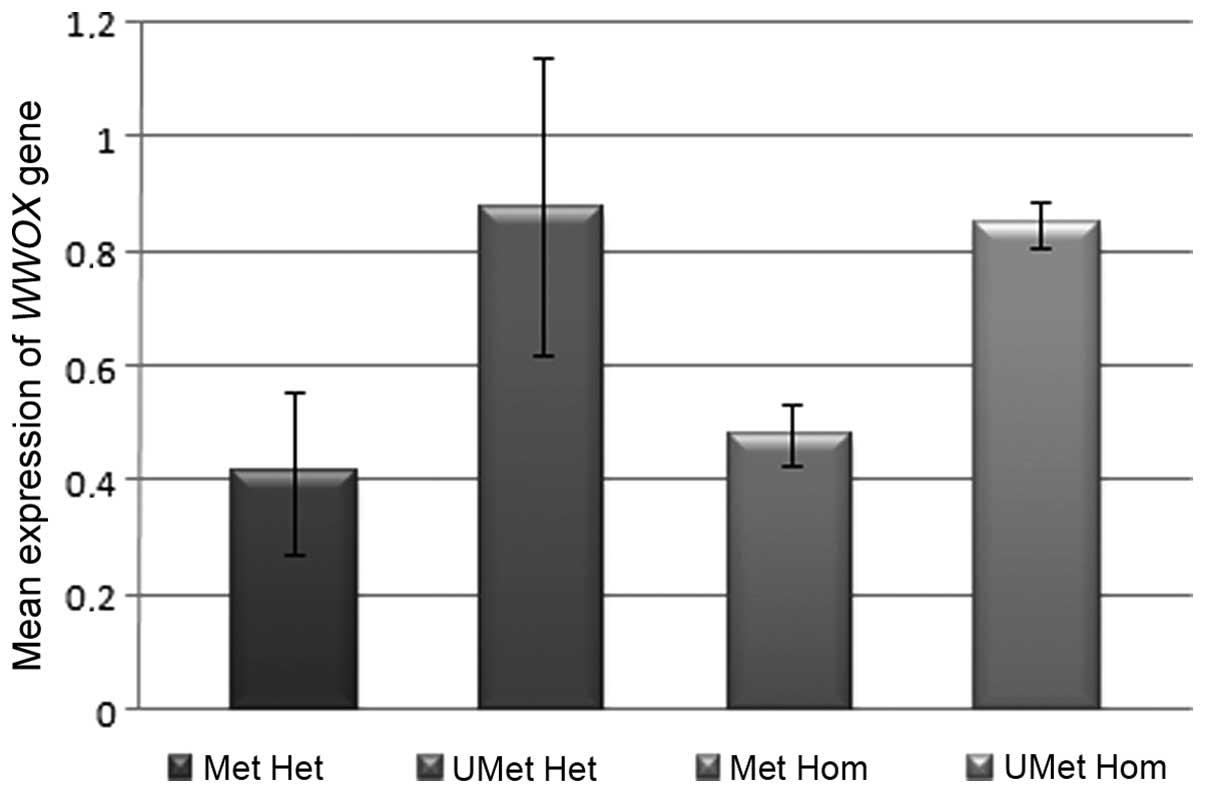
Similar associations between methylation and LOH in
WWOX gene expression were observed for marker D16S518,
located in intron 1 of the WWOX gene, although the results
were not identified to be statistically significant; 0.88±0.26 for
heterozygous, unmethylated vs. 0.41±0.14 for heterozygous,
methylated (P=0.16), and 0.85±0.04 for homozygous, unmethylated vs.
0.48±0.05 for homozygous, methylated (P=0.07; Fig. 2).
Correlation between genes
Numerous statistically significant correlations were
identified between the selected genes associated with
proliferation, apoptosis, cell cycle regulation and signal
transduction. Significant positive correlations were observed
between the expression levels of BIRC5 (survivin) and those
of the MKI67 (Rs=0.8170; P<0.0001) and
CCNE1 (Rs=0.6578; P<0.0001) genes. Significant
positive correlations were also observed between the expression
levels of the BIRC5 gene and two genes associated with
signal transduction, EGFR and VEGF
(Rs=0.4753; P=0.006 and Rs=0.3568; P=0.045,
respectively). A positive correlation was also observed between the
expression levels of the MKI67 gene and the expression
levels of EGFR (Rs=0.3636; P=0.0408) and
CCNE1 (Rs=0.7117; P<0.0001). Furthermore, a
positive correlation was identified between the EGFR and
VEGF expression levels (Rs=0.5385; P=0.0015). The
correlations between the expression levels of the analyzed genes
are presented in Table II.
| Table IISpearman rank correlation for
selected genes in patients with bladder cancer. |
Table II
Spearman rank correlation for
selected genes in patients with bladder cancer.
| Gene | Parameter | CCNE1 | EGFR | VEGF | MKI67 | BCL-2 | BAX | BIRC5 | WWOX |
|---|
| CCND1 | Rs
value | 0.0689 | 0.3405 | 0.5830 | 0.2319 | 0.4661* | 0.3430 | 0.0590 | 0.3780* |
| P-value | >0.05 | >0.05 | >0.05 | >0.05 | 0.0082* | >0.05 | >0.05 | 0.0329* |
| CCNE1 | Rs
value | | 0.3101 | 0.2936 | 0.7117* | 0.1435 | 0.2590 | 0.6578* | 0.0002 |
| P-value | | >0.05 | >0.05 | <0.0001* | >0.05 | >0.05 | <0.001* | >0.05 |
| EGFR | Rs
value | | | 0.5385* | 0.3636* | 0.313 | 0.1960 | 0.4753* | 0.1162 |
| P-value | | | 0.0015* | 0.0408* | >0.05 | >0.05 | 0.0060* | >0.05 |
| VEGF | Rs
value | | | | 03047 | 0.1552 | 0.3598* | 0.3568* | 0.2038 |
| P-value | | | | >0.05 | >0.05 | 0.0431* | 0.045* | >0.05 |
| MKI67 | Rs
value | | | | | 0.1076 | 0.0126 | 0.8170* | −0.0676 |
| P-value | | | | | >0.05 | >0.05 | <0.0001* | >0.05 |
| BCL-2 | Rs
value | | | | | | 0.3849* | −0.0426 | 0.1424 |
| P-value | | | | | | 0.0296* | >0.05 | >0.05 |
| BAX | Rs
value | | | | | | | 0.0125 | 0.3018 |
| P-value | | | | | | | >0.05 | >0.05 |
| BIRC5 | Rs
value | | | | | | | | −0.0896 |
| P-value | | | | | | | | >0.05 |
No statistically significant correlations between
the expression levels of the above-mentioned genes and clinical
factors, such as grade or stage were detected (P>0.05).
Discussion
The molecular profile of bladder cancer has not been
well recognized or described. However, numerous aspects of the
underlying molecular mechanisms that affect the control of gene
expression have been identified. LOH and methylation are processes
that interfere with proper gene function. These mechanisms have
been shown to be important in the regulation of the expression of
WWOX, a tumor suppressor gene whose expression is frequently
altered in a number of tumor types. This suppressor gene spans
>1,000,000 base pairs and is located at 16q. The chromosomal
section is characterized by frequent allelic losses in at least
three regions. High frequencies of these deletions were initially
observed in breast cancer samples (28). Further studies have revealed that
LOH is associated with a reduction in WWOX expression in
gastric (29), esophageal (15), pancreatic (14), lung (30) and breast cancer (31), as well as in glioblastoma multiforme
(25). Examination of bladder
cancer samples in the present study revealed that LOH occurred at a
higher frequency in intron 1 (marker D16S518) than in intron 8
(marker D16S3096) of the WWOX gene: 64.5 vs. 25.8%,
respectively. However, the influence of LOH on WWOX
expression was considered to be negligible. Comparable results have
been obtained for breast cancer (7). A similar percentage of WWOX
gene LOH was also observed in pancreatic primary tumors (27%)
(14), gastric carcinoma (31%)
(29) and primary non-small cell
lung cancer samples (37%) (30).
The present study also addressed the regulation of
WWOX gene expression by an epigenetic mechanism, promoter
methylation. The −508 to −174 bp region of the WWOX gene
promoter was methylated in 31% of bladder cancer samples and was
also associated with reduced levels of WWOX gene mRNA, which
is consistent with results observed in glioblastoma multiforme
specimens (25). Furthermore,
regarding the D16S3096 locus, the present study revealed that the
expression levels of the WWOX gene in unmethylated
heterozygotes were almost twice of those in methylated
heterozygotes; which was identified to be a statistically
significant difference. Thus, methylation appeared to be the
critical mechanism in the regulation of WWOX expression.
Similar trends with regard to promoter methylation status were
observed on intron 1, although no statistically significant
differences between methylated and unmethylated hetero- or
homozygotes were identified (D16S518; P>0.05).
A similar proportion of WWOX methylation has
been observed in transitional carcinomas of the bladder (12). This hypermethylation within the
WWOX promoter and exon 1 regions may be a result of
cigarette smoking, a habit commonly observed in cancer bladder
patients (10).
No statistically significant correlations between
WWOX gene expression levels and clinical factors, such as
grade and stage, were observed in the present study. However, an
analysis of 101 primary bladder tumor samples by Ramos et al
(11) revealed that lower levels of
WWOX protein were significantly associated with a higher
histological grade, as well as a more advanced stage, greater tumor
size and further cancer progression. The authors proposed that
WWOX may be a potential predictive marker for a more
aggressive disease stage. However, a large number of tumor samples
is required to demonstrate the influence of WWOX gene
alternations on the clinical status of bladder cancer.
The present study used the molecular expression
level profiles of bladder cancer samples to investigate the mRNA
levels of cancer-related genes. Changes in the following cell cycle
genes: Cyclin E1, the master regulator of progression from the the
G1 to the S phase, and cyclin D1, which is associated
with prompting entry into the cell cycle, were also evaluated.
Shariat et al (32)
demonstrated that a reduction in cyclin E1 expression levels was
associated with an advanced tumor stage, lymph vessel invasion and
lymph node metastases. In addition, reduced cyclin D1 and E1
expression levels were commonly correlated with altered expression
levels of pRB and p27. The observed correlations were
found to be associated with a poorer prognosis and reduced survival
times in patients with bladder cancer. The results of the present
study demonstrate a positive correlation between the levels of
CCND1 expression, and inhibition of apoptosis by the
antiapoptotic BCL2 gene and the WWOX tumor suppressor
gene. Furthermore, a positive correlation was observed between the
levels of CCNE1 gene expression and the levels of inhibitor
of apoptosis, BIRC5, accompanied by increased expression
levels of the proliferation marker, MKI67. However, no
association was identified between the levels of cyclin E1/D1
expression and clinical and pathological factors, such as grade or
stage.
An imbalance in apoptosis may result in
carcinogenesis in bladder tissues. However, the association between
BCL2 gene expression and cancer progression remains unclear.
Shiina et al (33)
demonstrate that increased expression levels of the BCL2
gene are observed in numerous types of urinary tract cancers, are
connected with a less aggressive tumor phenotype and are not
significant in tumor progression. Conversely, Bilim et al
(34) reported that high
BCL2 expression levels were associated with greater cancer
progression. However, the results of the present study reveal a
positive correlation between the expression levels of BCL2
and BAX genes in bladder cancer.
A key process in bladder cancer progression is
considered to involve a member of the inhibitor of apoptosis
family, BIRC5 (survivin). Studies have demonstrated associations
between overexpression of survivin and higher tumor stage, lymph
node invasion (35,36) and possible shorter survival times
(37).
The results of the present study demonstrate a
marked positive correlation between the expression levels of
BIRC5, CCNE1 and EGFR. Furthermore, a
dependence was observed between the levels of BIRC5 mRNA and
those of the MKI67 marker of proliferation, which may
indicate that cell survival and proliferation are closely
associated in bladder cancer. Certain studies also report an
association between increased MKI67 expression levels and
higher grade and stage (38). The
results of the present study do not reveal any association between
the expression levels of the genes regulating apoptosis
(BCL2, BAX and BIRC5) and the MKI67
gene that regulates proliferation, and clinical prognostic factors,
such as grade or stage.
However, a marked positive correlation was observed
between genes connected with angiogenesis (VEGF) and signal
transduction (EGFR). Increased VEGF gene expression
levels were observed in the transitional-epithelial type of bladder
tumor and the expression levels were correlated with progression
(39). These results are consistent
with those of Crew et al (40), which demonstrated threefold higher
VEGF expression levels in tumor samples, when compared with
healthy bladder tissue samples. These results underline the value
of VEGF in the prediction of disease recurrence and thus
indicate an appropriate target for intravesical therapy. Previous
studies have indicated that processes associated with the cell
cycle, signal transduction, apoptosis and proliferation may be
relevant in assessing the risk of local recurrence and survival
rates in patients suffering from cancer of the bladder (41–46).
In addition, a significant increase in EGFR
gene expression levels has been detected in invasive bladder
tumors, compared with tumors of low malignancy, and EGFR has
been associated with poor histological differentiation (47). However, in the present study, no
association was observed between the expression levels of the
above-mentioned genes, and gender, stage or grade.
The reduced expression levels of tumor suppressor
genes may be one factor that initiates neoplastic lesion
development. The results of the present study indicate that, in
bladder cancer, WWOX gene expression levels may be reduced
by two mechanisms: LOH or promoter region methylation. In this type
of tumor, apoptosis may also be inhibited by increased expression
levels of the BCL2 gene. In addition, progression may be
influenced as a result of the positive correlation between the
MKI67 proliferation index and the BIRC5 apoptosis
inhibitor gene expression levels.
In conclusion, the results of the present study
provide an overview of the molecular changes that are apparent in
bladder tumors. However, further molecular studies with a greater
number of patients are required for an improved understanding of
the biology of this disease and for the introduction of more
effective therapeutic strategies.
Acknowledgements
The present study was funded by the Medical
University of Lodz (grant no. 503/0-078-02/503-01).
References
|
1
|
Ministry of Health, Poland. National
Cancer Registry. http://epid.coi.waw.pl/krn/.
Accessed June 30, 2010
|
|
2
|
Luis NM, López-Knowles E and Real FX:
Molecular biology of bladder cancer. Clin Transl Oncol. 9:5–12.
2007.
|
|
3
|
Kim WJ and Bae SC: Molecular biomarkers in
urothelial bladder cancer. Cancer Sci. 99:646–652. 2008.
|
|
4
|
Jung I and Messing E: Molecular mechanisms
and pathways in bladder cancer development and progression. Cancer
Control. 7:325–334. 2000.
|
|
5
|
Mitra AP, Datar RH and Cote RJ: Molecular
pathways in invasive bladder cancer: new insights into mechanisms,
progression, and target identification. J Clin Oncol. 24:5552–5564.
2006.
|
|
6
|
Yoon DS, Li L, Zhang RD, Kram A, et al:
Genetic mapping and DNA sequence-based analysis of deleted regions
on chromosome 16 involved in progression of bladder cancer from
occult preneoplastic conditions to invasive disease. Oncogene.
20:5005–5014. 2001.
|
|
7
|
Bednarek AK, Laflin KJ, Daniel RL, et al:
WWOX, a novel WW domain-containing protein mapping to human
chromosome 16q23.3–24.1, a region frequently affected in breast
cancer. Cancer Res. 60:2140–2145. 2000.
|
|
8
|
Qin HR, Iliopoulos D, Semba S, et al: A
role for the WWOX gene in prostate cancer. Cancer Res.
66:6477–6481. 2006.
|
|
9
|
Lan C, Chenggang W, Yulan B, et al:
Aberrant expression of WWOX protein in epithelial ovarian cancer: a
clinicopathologic and immunohistochemical study. Int J Gynecol
Pathol. 31:125–132. 2012.
|
|
10
|
Yang W, Cui S, Ma J, et al: Cigarette
smoking extract causes hypermethylation and inactivation of WWOX
gene in T-24 human bladder cancer cells. Neoplasma. 59:216–223.
2012.
|
|
11
|
Ramos D, Abba M, Lopez-Guerrero JA, et al:
Low levels of WWOX protein immunoexpression correlate with tumour
grade and a less favourable outcome in patients with urinary
bladder tumours. Histopathology. 52:831–839. 2008.
|
|
12
|
Iliopoulos D, Guler G, Han SY, et al:
Fragile genes as biomarkers: epigenetic control of WWOX and FHIT in
lung, breast and bladder cancer. Oncogene. 24:1625–1633. 2005.
|
|
13
|
Knudson AG Jr: Hereditary cancer,
oncogenes, and antioncogenes. Cancer Res. 45:1437–1443. 1985.
|
|
14
|
Kuroki T, Yendamuri S, Trapasso F, et al:
The tumor suppressor gene WWOX at FRA16D is involved in pancreatic
carcinogenesis. Clin Cancer Res. 10:2459–2465. 2004.
|
|
15
|
Kuroki T, Trapasso F, Shiraishi T, et al:
Genetic alterations of the tumor suppressor gene WWOX in esophageal
squamous cell carcinoma. Cancer Res. 62:2258–2260. 2002.
|
|
16
|
Aqeilan RI, Donati V, Palamarchuk A, et
al: WW domain-containing proteins, WWOX and YAP, compete for
interaction with ErbB-4 and modulate its transcriptional function.
Cancer Res. 65:6764–6772. 2005.
|
|
17
|
Aqeilan RI, Donati V, Gaudio E, et al:
Association of Wwox with ErbB4 in breast cancer. Cancer Res.
67:9330–9336. 2007.
|
|
18
|
Gaudio E, Palamarchuk A, Palumbo T, et al:
Physical association with WWOX suppresses c-Jun transcriptional
activity. Cancer Res. 66:11585–11589. 2006.
|
|
19
|
Aqeilan RI, Pekarsky Y, Herrero JJ, et al:
Functional association between Wwox tumor suppressor protein and
p73, a p53 homolog. Proc Natl Acad Sci USA. 101:4401–4406.
2004.
|
|
20
|
Aqeilan RI, Hassan MQ, de Bruin A, et al:
The WWOX tumor suppressor is essential for postnatal survival and
normal bone metabolism. J Biol Chem. 283:21629–21639. 2008.
|
|
21
|
Jin C, Ge L, Ding X, et al: PKA-mediated
protein phosphorylation regulates ezrin-WWOX interaction. Biochem
Biophys Res Commun. 341:784–791. 2006.
|
|
22
|
Nunez MI, Ludes-Meyers J and Aldaz CM:
WWOX protein expression in normal human tissues. J Mol Histol.
37:115–125. 2006.
|
|
23
|
Aqeilan RI, Hagan JP, de Bruin A, et al:
Targeted ablation of the WW domain-containing oxidoreductase tumor
suppressor leads to impaired steroidogenesis. Endocrinology.
150:1530–1535. 2009.
|
|
24
|
World Health Organization Classification
of Tumours. World Health Organization, IARC Press; Lyon: 2004
|
|
25
|
Kosla K, Pluciennik E, Kurzyk A,
Jesionek-Kupnicka D, et al: Molecular analysis of WWOX expression
correlation with proliferation and apoptosis in glioblastoma
multiforme. J Neurooncol. 101:207–213. 2011.
|
|
26
|
Płuciennik E, Nowakowska M, Wujcicka WI,
et al: Genetic alterations of WWOX in Wilms’ tumor are involved in
its carcinogenesis. Oncol Rep. 28:1417–1422. 2012.
|
|
27
|
Pfaffl MW, Horgan GW and Dempfle L:
Relative expression software tool (REST) for group-wise comparison
and statistical analysis of relative expression results in
real-time PCR. Nucleic Acids Res. 30:e362002.
|
|
28
|
Maeda N, Semba S, Nakayama S, et al: Loss
of WW domain-containing oxidoreductase expression in the
progression and development of gastric carcinoma: clinical and
histopathologic correlations. Virchows Arch. 457:423–432. 2010.
|
|
29
|
Aqeilan RI, Kuroki T, Pekarsky Y, et al:
Loss of WWOX expression in gastric carcinoma. Clin Cancer Res.
10:3053–3058. 2004.
|
|
30
|
Yendamuri S, Kuroki T, Trapasso F, et al:
WW domain containing oxidoreductase gene expression is altered in
non-small cell lung cancer. Cancer Res. 63:878–881. 2003.
|
|
31
|
Chen T, Sahin A and Aldaz CM: Deletion map
of chromosome 16q in ductal carcinoma in situ of the breast:
refining a putative tumor suppressor gene region. Cancer Res.
56:5605–5609. 1996.
|
|
32
|
Shariat SF, Ashfaq R, Sagalowsky AI and
Lotan Y: Correlation of cyclin D1 and E1 expression with bladder
cancer presence, invasion, progression, and metastasis. Hum Pathol.
37:1568–1576. 2006.
|
|
33
|
Shiina H, Igawa M, Urakami S, et al:
Immunohistochemical analysis of Bcl-2 expression in transitional
cell carcinoma of the bladder. J Clin Pathol. 49:395–399. 1996.
|
|
34
|
Bilim VN, Tomita Y, Kawasaki T, et al:
Variable Bcl-2 phenotype in benign and malignant lesions of
urothelium. Cancer Lett. 128:87–92. 1998.
|
|
35
|
Wang H, Xi X, Kong X, et al: The
expression and significance of survivin mRNA in urinary bladder
carcinomas. J Cancer Res Clin Oncol. 130:487–490. 2004.
|
|
36
|
Shariat SF, Ashfaq R, Karakiewicz PI, et
al: Survivin expression is associated with bladder cancer presence,
stage, progression, and mortality. Cancer. 109:1106–1113. 2007.
|
|
37
|
Kitamur H, Torigoe T, Honma I, et al:
Expression and antigenicity of survivin, an inhibitor of apoptosis
family member, in bladder cancer: Implications for specific
immunotherapy. Urology. 67:955–959. 2006.
|
|
38
|
Gonzalez-Campora R, Davalos-Casanova G,
Beato-Moreno A, et al: Apoptotic and proliferation indexes in
primary superficial bladder tumors. Cancer Lett. 242:266–272.
2006.
|
|
39
|
Yang CC, Chu KC and Yeh WM: The expression
of vascular endothelial growth factor in transitional cell
carcinoma of urinary bladder is correlated with cancer progression.
Urol Oncol. 22:1–6. 2004.
|
|
40
|
Crew JP, O’Brien T, Bradburn M, et al:
Vascular endothelial growth factor is a predictor of relapse and
stage progression in superficial bladder cancer. Cancer Res.
57:5281–5285. 1997.
|
|
41
|
Pfister C, Moore L, Allard P, Larue H,
Lacombe L, Têtu B, Meyer F and Fradet Y: Predictive value of cell
cycle markers p53, MDM2, p21, and Ki-67 in superficial bladder
tumor recurrence. Clin Cancer Res. 5:4079–4084. 1999.
|
|
42
|
Behnsawy HM, Miyake H, Abdalla MA, Sayed
MA, Ahmed Ael-F and Fujisawa M: Expression of cell cycle-associated
proteins in non-muscle-invasive bladder cancer: correlation with
intravesical recurrence following transurethral resection. Urol
Oncol. 29:495–501. 2011.
|
|
43
|
Chen L, Wang X, Mei H and Chen W:
Apoptosis and expression of PCNA in superficial transitional cell
bladder cancer as related to recurrence. Zhonghua Wai Ke Za Zhi.
36:484–486. 1998.(In Chinese).
|
|
44
|
Gazzaniga P, Gradilone A, Giuliani L,
Gandini O, Silvestri I, Nofroni I, Saccani G, Frati L and Aglianò
AM: Expression and prognostic significance of LIVIN, SURVIVIN and
other apoptosis-related genes in the progression of superficial
bladder cancer. Ann Oncol. 14:85–90. 2003.
|
|
45
|
Jeong IG, Kim SH, Jeon HG, Kim BH, Moon
KC, Lee SE and Lee E: Prognostic value of apoptosis-related markers
in urothelial cancer of the upper urinary tract. Hum Pathol.
40:668–677. 2009.
|
|
46
|
Chow NH, Liu HS, Lee EI, Chang CJ, Chan
SH, Cheng HL, Tzai TS and Lin JS: Significance of urinary epidermal
growth factor and its receptor expression in human bladder cancer.
Anticancer Res. 17:1293–1296. 1997.
|
|
47
|
Neal DE, Marsh C, Bennett MK, et al:
Epidermal-growth-factor receptors in human bladder cancer:
comparison of invasive and superficial tumours. Lancet. 1:366–368.
1985.
|