Introduction
Intravenous leiomyomatosis (IVL) is a rare,
histologically benign, smooth muscle tumor. It is typically
associated with a mesenchymal tumor of the uterus with macroscopic
intravascular proliferation (1).
Although IVL is histologically benign, it may occasionally exhibit
malignant behavior, due to its growth along the pelvic veins and
the inferior vena cava (IVC), extending into the cardiac chambers
and pulmonary vasculature (2). Due to
its rarity and atypical clinical features, the condition may be
misdiagnosed as a primary cardiac tumor or a venous thrombus, which
may lead to potentially life threatening consequences. Hence, early
and accurate diagnosis and appropriate treatment choices are
important for the patient prognosis. Complete surgical resection
(single or staged procedures) is the treatment option for IVL, as
it is key to preventing recurrence (3). The present study reports 2 cases of IVL
that were diagnosed using dual-source computed tomography (CT) and
magnetic resonance imaging (MRI), as well as clinical and
pathological examinations. A review of the English literature on
IVL was also performed.
Case report
Case 1
A 46-year-old female patient was referred to the
West China Hospital of Sichuan University (Chengdu, China) in
December 2013, presenting with a 10-day history of palpitations and
shortness of breath that were exacerbated upon exertion. Physical
examination revealed slight bilateral leg edema and no other
abnormalities. Echocardiography showed a mobile, solid mass in the
right atrium that originated from the IVC. The lesion, which almost
blocked the tricuspid valve, was initially diagnosed as atrial
myxoma or thrombus. The serum levels of the tumor marker
carbohydrate antigen (CA) 125 were mildly elevated (41.93 U/ml;
normal value, <35 U/ml), while all other blood and biochemical
markers were within the normal ranges. The patient's medical
history included a myomectomy (on October 2000), with no notable
family history.
Thoracic and abdominal CT scans (Somatom Definition
Flash; Siemens AG, Munich, Germany) were performed with and without
contrast media. On the CT scans, a filling defect was observed in
the IVC and right atrium, with a soft tissue density of 20–22 HU on
plain images and 28–62 HU on contrast-enhanced images. The lesion
stretched into the right ventricle through the tricuspid valve, and
stretched as far as the left common iliac vein and internal iliac
vein inferiorly. In addition, an ill-defined mass with
heterogeneous attenuation was detected in the pelvic region; the
mass originated from the uterus and involved the left gonadal vein,
resulting in luminal stenosis. The CT value of the pelvic lesion
was 15–31 HU on plain images and 31–52 HU on contrast-enhanced
images. The lesion in the right atrium and IVC appeared to be
anatomically associated with the mass located in the pelvic region
(Fig. 1). Furthermore, tortuous
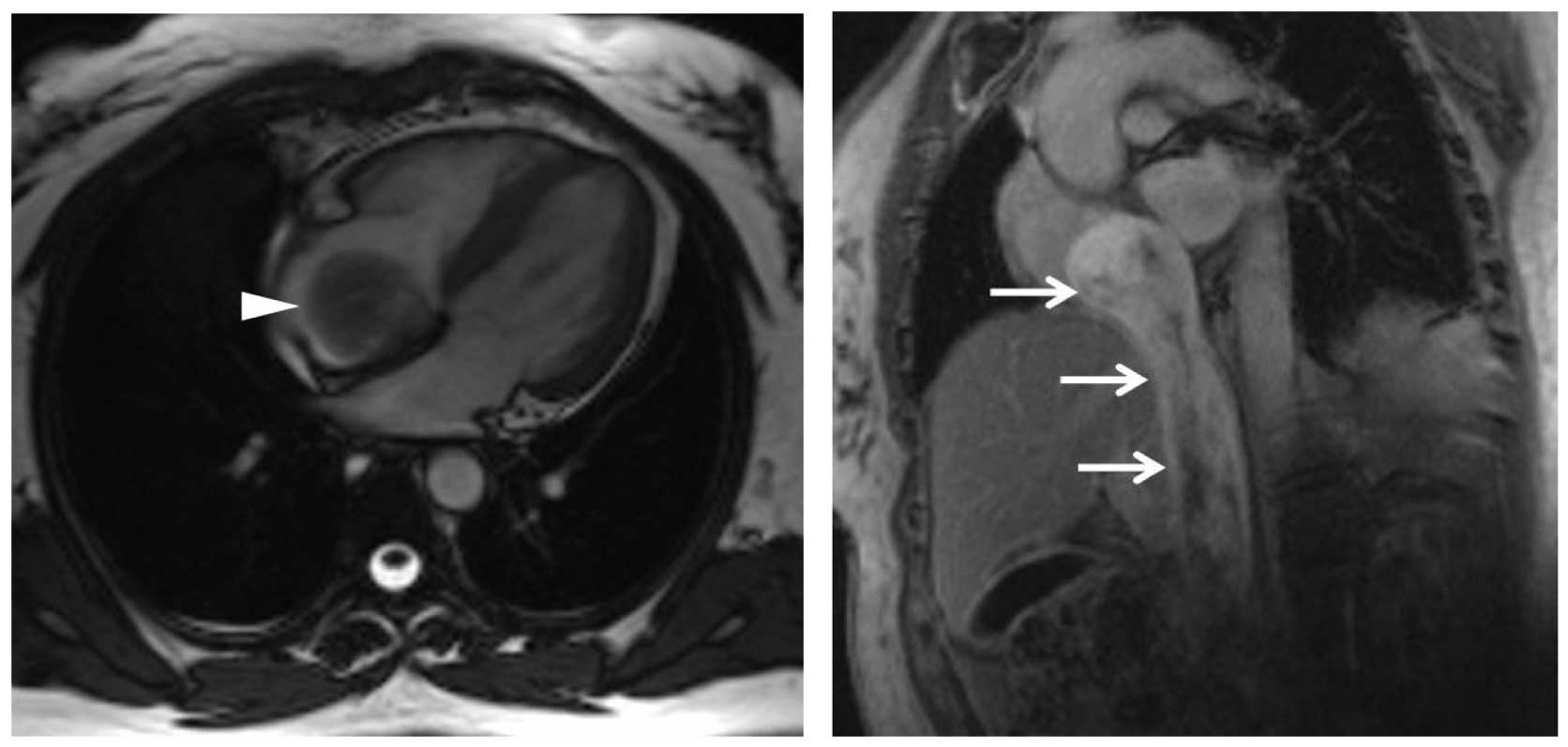
collateral veins were observed around the IVC. Cardiac cine MRI
(Magnetom Trio Tim; Siemens AG) showed that the circumscribed mass
moved in parallel with the cardiac motion in the right cardiac
cavities. Gadolinium-enhanced MRI of the heart revealed a large
streak-shaped filling defect in the IVC and right atrium that was
mildly hyperintense on T1- and T2-weighted imaging (WI), and
heterogeneously enhanced following contrast-enhanced scanning
(Fig. 2).
Considering the imaging findings, complete surgical
excision of the tumor in the IVC was performed carefully through a
right atriotomy and longitudinal venotomy in January 2014. The
tumor had no stalk or obvious adhesion with the wall of the right
atrium.
The resected gross intracaval specimen was a
yellowish-white tumor with a smooth border and a tip. The tumor
appeared as a sausage-shaped protrusion with a maximum diameter of
~20 cm. Immunohistochemical analysis using monoclonal antibodies
revealed positivity for the smooth muscle markers desmin (Biocare
Medical LLC, Concord, CA, USA) and smooth muscle actin (SMA;
OriGene Technologies Inc., Rockville, MD, USA), and negativity for
h-caldesmon (Epitomics, Burlingame, CA, USA), human melanoma black
45 (HMB45) and S-100 (both Leica Microsystems Inc., Buffalo Grove,
IL, USA). Upon microscopy (CX31-72C02 microscope; Olympus,
Corporation, Tokyo, Japan), the hematoxylin-eosin staining of tumor
sections revealed smooth muscle cell proliferation without nuclear
atypia or mitotic index. The MIB-1/Ki-67 (OriGene Technologies
Inc.) labeling index was ~2%, confirming the non-malignant nature
of the tumor. In addition, estrogen and progesterone (Epitomics)
expression was detected in the nucleus (3).
The postoperative course of the patient was
uneventful, and no signs of recurrence were observed at the 1-year
follow-up examination in February 2015.
Case 2
A 45-year-old female patient presented to the West
China Hospital of Sichuan University in November 2014 with a
4-month history of persistent palpitations and occasional syncope.
The patient's past medical history consisted of a myomectomy on
June 2007, with nothing of particular note in the family medical
history. Upon physical examination, a diastolic murmur was
auscultated in the tricuspid region. Laboratory test results were
normal, with the exception of an increased level of CA 125 (56.93
U/ml). Echocardiography demonstrated a hypoechogenic mass in the
right atrium and ventricle, suggesting a diagnosis of thrombi.
Contrast-enhanced CT scans performed from the chest
to the pelvis revealed unilateral heterogeneous uterine masses in
the right iliac vein and IVC that were indicative of multiple
leiomyoma. The mass that caused almost complete occlusion of the
IVC demonstrated enhancement similar to that of the uterine
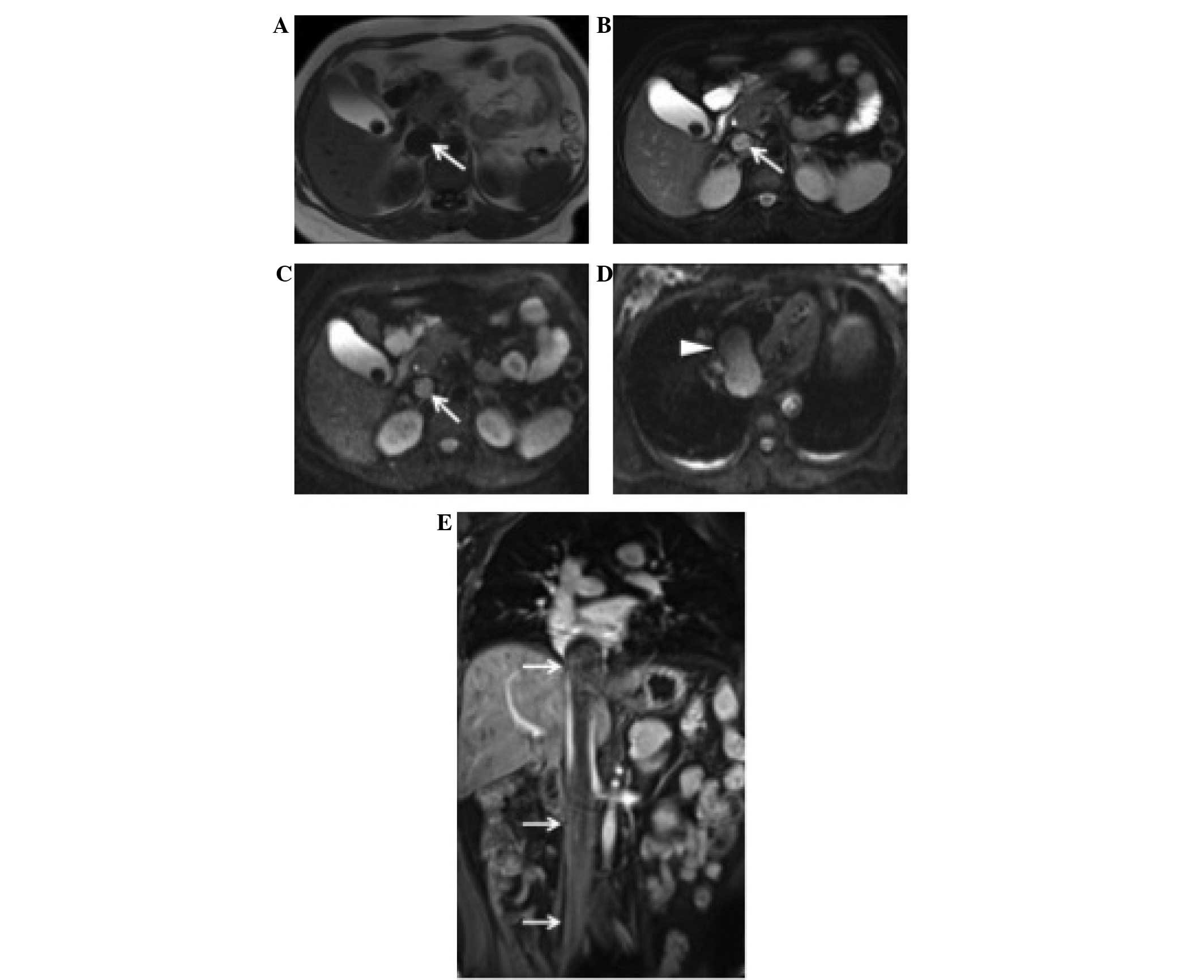
leiomyoma (Fig. 3). MRI of the chest
and upper abdomen revealed a cord-like mass extending from the IVC
into the right cardiac chambers and almost completely occupying the
IVC lumen. The tumor exhibited low to intermediate signal intensity
on T1WI and heterogeneous high signal intensity on T2WI, with mild
enhancement observed in the late phase. The top of the mass
extended from the right atrium into the right ventricle at the
diastolic phase (Fig. 4). Based on
these findings, the patient was diagnosed with IVL of the uterus
with intravascular and cardiac extension.
Total abdominal hysterectomy, bilateral
salpingo-oophorectomy, and intracardiac and intravenous mass
excision were performed as a two-stage procedure under
cardiopulmonary bypass in April 2013 and July 2013. Gross
examination of the intravascular specimen revealed a smooth,
wormlike mass, 3–4 cm in circumference and 26 cm in length, with a
bulbous end corresponding to the intracardiac portion that almost
blocked the tricuspid valve.
The excised tumor had a white cut surface, and was
rubbery and firm on palpation. Immunohistochemical analysis of the
IVL cells indicated positive staining for the smooth muscle markers
desmin (Biocare Medical LLC) and SMA (OriGene Technologies Inc.),
and negative staining for Ki-67 (OriGene Technologies Inc.), HMB45,
S-100 (both Leica Microsystems Inc.), h-caldesmon (Epitomics) and
p53 (OriGene Technologies Inc.), confirming its smooth muscle
nature without signs of malignancy. Nuclear estrogen and
progesterone receptor expression was observed in the intravascular
tumor and uterine leiomyoma. The postoperative course was
uneventful. The patient continued to recover well, and at the
18-month follow-up, there was no recurrence of the symptoms or
tumor, and the patient resumed normal activities thereafter.
Discussion
IVL, which was first described by Brich-Hirschfeld
in 1896 (4), is a rare benign tumor
that is histologically characterized by nodular masses of smooth
muscle cells growing within systemic veins. It typically originates
from the uterus and may involve ovarian veins. Occasionally, the
tumor occurs in other intravascular locations, distant from the
uterus. Durck reported the first case of IVL with intracardiac
extension in 1907 (5). The tumors
were described as nodular or spiral within pelvic veins and the
IVC, or extending to the right cardiac chambers and bilateral
pulmonary arteries (2,6,7). Two major
hypotheses have been established regarding the etiology of IVL
(1,8).
The first hypothesis suggests that the tumor arises from the vein
walls, while the second proposes that the uterine leiomyoma is a
primary tumor with intravascular projections into an adjacent
venous channel. Fukuyama et al (9) suggested that the tumor does not invade
the vessel by breaking the venous wall, but rather stretches the
vascular wall to extend along the vascular lumen, while covered in
endothelium.
A review of the English literature included by
PubMed between January 2000 and January 2015 was performed using
the keywords ‘intravenous leiomyomatosis’ AND ‘last 15
years’[PDat], and 52 cases of IVL with CT or MRI descriptions were
identified, as indicated in Table I
(2,6,7,10–46). The
median age of the patients was 44.8 years old (age range, 20–70
years). The majority of cases were diagnosed intraoperatively.
Common initial symptoms included pelvic pain or abnormal uterine
bleeding; however, certain patients presented with chest pain,
palpitation, shortness of breath, dyspnea on exertion, edema of the
lower extremities or even sudden mortality. The clinical signs and
symptoms predominantly depended on the degree of intravascular
obstruction caused by the tumor. Heart failure may result in
misdiagnosis or delayed diagnosis of IVL until further examination
or sudden mortality due to fatal intracardiac obstruction.
 | Table I.Clinical features of all 52 cases
diagnosed as intravenous leiomyomatosis. |
Table I.
Clinical features of all 52 cases
diagnosed as intravenous leiomyomatosis.
| No. | Author, year | Cases, n | Age years, | Symptoms | Extension | Treatment | Outcome | Refs. |
|---|
| 1 | Osawa et al,
2013 | 1 | 66 | Asymptomatic | IVC | One-stage complete
resection | No recurrence for 6
months | (10) |
| 2 | Yaguchi et
al, 2010 | 1 | 70 | Asymptomatic | IVC | One-stage complete
resection | No recurrence for 2
years | (11) |
| 3 | Leitman et
al, 2008 | 2 | 52 | Transient ischemic
attack | IVC, RA | One-stage complete
resection | / | (12) |
|
|
|
| 49 | Asymptomatic | IVC, RA | One-stage complete
resection | / |
|
| 4 | Rispoli et
al, 2010 | 1 | 60 | Asymptomatic | IVC, RA | One-stage complete
resection | No recurrence for
22 months | (13) |
| 5 | Bender et
al, 2011 | 1 | 55 | Hypertension | IVC, RA, RV | One-stage complete
resection | No recurrence for 4
months | (14) |
| 6 | Ozer et al,
2005 | 1 | 43 | Abdominal pain,
dizziness, bilateral leg edema | IVC, RA | Refused any
treatment | / | (15) |
| 7 | Liu et al,
2013 | 1 | 33 | Asymptomatic | IVC, RA | One-stage complete
resection | No recurrence for
13 months | (16) |
| 8 | Matos et al,
2013 | 1 | 45 | Fatigue, shortness
of breath and precordial discomfort | IVC, RA | Two-stage
resection | / | (17) |
| 9 | Wakiyama et
al, 2000 | 1 | 47 | Syncopic | IVC, RA | One-stage complete
resection | No recurrence for 6
months | (18) |
| 10 | Lou et al,
2011 | 1 | 42 | Debilitation and
engorgement of both lower extremities | IVC, RA | One-stage complete
resection | / | (19) |
| 11 | Robert-Ebadi et
al, 2009 | 1 | 41 | Asymptomatic | IVC | One-stage complete
resection | / | (20) |
| 12 | Barksdale et
al, 2011 | 1 | 44 | Increasing
lethargy, abdominal pain, bilateral lower extremity edema, and
increasing abdominal girth | IVC, hepatic
veins | Two-stage
resection | No recurrence for 3
months | (21) |
| 13 | Biri et al,
2008 | 1 | 31 | Shortness of breath
and orthopnea | IVC, RA | Refused surgery,
treatment with aromatase inhibitor | Tumor size was
decrease in a 6-month follow-up | (22) |
| 14 | Saitoh et
al, 2004 | 1 | 47 | Asymptomatic | IVC, RA | One-stage complete
resection | No recurrence for
17 months | (23) |
| 15 | Harris and
Karakousis et al, 2000 | 1 | 48 | Shortness of
breath, recurrent palpitations and dizziness | IVC, RA, RV | One-stage complete
resection | No recurrence for 6
months | (24) |
| 16 | Fang et al,
2007 | 1 | 40 | Dyspnea on
exertion, mild leg edema, and syncope | IVC, RA | Two-stage
resection | No recurrence for 6
months | (25) |
| 17 | Liu et al,
2009 | 6 | 48 | Menstruation
increase | IVC, RA | Two-stage
resection | 1 case with
residual tumor, the | (26) |
|
|
|
| 41 | Intermittently
flustered, chest tightness | IVC, RA | Two-stage
resection | other 4 cases had
no recurrence (average follow-up time: 58.5±26.8 months) |
|
|
|
|
| 49 | Edema of both lower
legs, with increasing abdominal distention | IVC, RA | No surgical
intervention due to serious heart and lung dysfunction |
|
|
|
|
|
| 20 | Asymptomatic | IVC | One-stage complete
resection |
|
|
|
|
|
| 43 | Asymptomatic | IVC | One-stage complete
resection |
|
|
|
|
|
| 38 | Asymptomatic | IVC | One-stage complete
resection |
|
|
| 18 | Clay et al,
2013 | 1 | 40 | Lower abdominal and
rectal discomfort | IVC, RA, RV | Two-stage
resection | No recurrence for
18 months | (27) |
| 19 | Wu et al,
2009 | 1 | 39 | Chest tightness and
dyspnea | IVC, RA | Two-stage
resection | / | (28) |
| 20 | Singh et al,
2010 | 1 | 43 | Right upper
abdominal pain, bloating and swelling of the left leg | IVC, RA | One-stage complete
resection | / | (29) |
| 21 | Li et al,
2011 | 4 | 36 | Sudden and
transient syncope | IVC, RA, RV | One-stage complete
resection | / | (30) |
|
|
|
| 48 | Recurrent sudden
syncope | IVC, RA | One-stage | / |
|
|
|
|
| 51 | Recurrent sudden
syncope | IVC, RA, RV | One-stage | / |
|
|
|
|
| 43 | Asymptomatic | IVC, RA | One-stage | / |
|
| 22 | Wong et al,
2006 | 1 | 54 | Acute-onset left
lower limb swelling | IVC, RA |
Gonadotropin-releasing hormone + one-stage
complete resection + tamoxifen | A follow-up CT scan
showed rapid progression of disease with intravascular tumor
extending into the right atrium, abdominal lymphadenopathy, and an
increase in the number and size of lung metastases | (31) |
| 23 | Peng et al,
2012 | 4 | 37,40, 43,48 | 2 cases of edema of
the lower, extremity; 1 case of bulk-related symptoms of recurrent,
leiomyoma 1 case of chest distress on breath-holding | IVC (1 case) RA (2
cases) RV (1 case) | / | / | (32) |
| 24 | Ahmed et al,
2004 | 1 | 48 | Bulk-related
symptoms of recurrent leiomyoma | IVC | One-stage complete
resection | / | (33) |
| 25 | Bilyeu et
al, 2006 | 1 | 51 | Left arm discomfort
and palpitations | IVC, RA | Two-stage
resection | / | (34) |
| 26 | Moorjani et
al, 2005 | 1 | 64 | Left calf
swelling | IVC, RA | One-stage complete
resection and adjuvant radiotherapy | A subsequent CT
scan showed recurrence of the tumor on the pelvic wall, as well as
sacral metastases | (35) |
| 27 | Lai et al,
2005 | 1 | 47 | Menorrhagia | IVC | Two-stage
resection | / | (36) |
| 28 | Demirkiran et
al, 2013 | 1 | 39 | Asymptomatic | IVC, RA | One-stage complete
resection | No recurrence for 4
months | (37) |
| 29 | Izzat et al,
2011 | 1 | 45 | Dyspnea | IVC, RA, PA | One-stage complete
resection | No recurrence for 8
months | (9) |
| 30 | Nam et al,
2003 | 1 | 46 | Abdominal pain and
discomfort | IVC, RA | One-stage complete
resection | No recurrence for
12 months | (38) |
| 31 | Kokawa et
al, 2002 | 1 | 49 | Syncope | IVC, RA | One-stage complete
resection | No recurrence for
17 months | (39) |
| 32 | Lee et al,
2011 | 1 | 43 | Palpitation,
dizziness, dyspnea, and chest pain | IVC, RA, PA | One-stage complete
resection | No recurrence for 2
years | (7) |
| 33 | Rajaii-Khorasani
et al, 2012 | 1 | 25 | Deteriorating
fatigue, dyspnea on exertion | IVC, RA, PA | One-stage complete
resection | No recurrence for 2
years | (2) |
| 34 | Esmaeilzadeh et
al, 2007 | 1 | 46 | Worsening dyspnea
on exertion | IVC, RA RV | Tamoxifen and
decapeptide + reoperation 6 months later | Early recurrence
was secondary to the incomplete resection | (40) |
| 35 | Elkington et
al, 2005 | 1 | 53 | Asymptomatic | IVC | two-stage
resection | / | (41) |
| 36 | Cea-Calvo et
al, 2000 | 1 | 41 | Swollen legs and
abdominal distension | IVC, RA | One stage complete
resection | / | (42) |
| 37 | Xu et al,
2013 | 1 | 36 | Shortness of breath
after activities | IVC, RA | One stage complete
resection | / | (43) |
| 38 | Sogabe et
al, 2014 | 1 | 45 | Repeated syncopal
attacks | IVC, RA | One-stage complete
resection | No recurrence for
10 months | (44) |
| 39 | Moniaga et
al, 2012 | 1 | 44 | Dyspnea and lower
extremity edema | IVC, RA | Two-stage
resection | Recovered well | (45) |
| 40 | Kocaoglu et
al, 2003 | 1 | 43 | Dyspnea, lower
extremity swelling, and syncope | IVC, RA, RV | Incomplete
resection | Lost to
follow-up | (46) |
In the majority of the reviewed cases, the initial
pathway of extension for IVL was unilateral through the common
iliac veins, while certain cases exhibited IVL with intracardiac
extension and concomitant uterine leiomyoma. Various unusual
patterns of intravenous growth were observed in the 52 recorded
tumors; the distal end of 11 tumors (21.2%) were confined to the
IVC, 30 (57.7%) extended to right atrium, 8 (15.4%) to the right
ventricle and 3 (5.8%) to the pulmonary arteries. Tumor mobility
was recorded in 42 of these cases, however, due to the varying
diameters of the tumors, adherence to the wall of the IVC or the
right chambers were reported in 26 cases. The distal end of the
tumor in the present cases extended intracardially to the right
atrium and right ventricle. Both of these tumors moved in parallel
with cardiac motion.
CT and MRI scans are the most useful imaging
modalities for the diagnosis of IVL. The high-density resolution
and multiplanar capability of CT, as well as the excellent soft
tissue resolution of MRI, render these modalities particularly
favorable for characterizing the continuity of intraluminal tumors.
In the two cases in the present study, the IVLs appeared as soft
masses in the right atrium and IVC on CT scans; the IVL completely
occupied the IVC, iliac veins and internal iliac vein in a
continuous manner in each case. A portion of the irregular uterine
mass appeared to be anatomically connected to the tumor in the
adjacent iliac veins. The IVLs of the two patients shared similar
soft tissue density and enhanced features on CT or MRI scans with
those reported in previous studies (40,47). Of
the 52 cases identified in the literature, 45 (86.5%) underwent a
contrast-enhanced CT scan or CT angiography. Heterogeneous
enhancement of the tumors was observed in 27 (60.0%) cases,
consistent with the present cases, with mildly homogeneous or no
enhancement in 13 (28.9%) cases and homogeneous enhancement in 5
(11.1%) cases.
The signal intensity of the lesions on MRI depends
on the number of smooth muscle cells and vessels containing
hyalinized fibrous tissue (48). The
tumor in case 1 of the present study was mildly hyperintense on
T1WI and T2WI, whereas the tumor in case 2 had a low to
intermediate signal intensity on T1WI and heterogeneous
hyperintensity on T2WI; both tumors exhibited heterogeneous
enhancement. There are conflicting reports with regards to the
signal intensity of IVL on MRI scans; in certain studies, IVL
presents as iso- to mildly hyperintense (46,48), while
in others it presents as hypointense (49,50) on
T1WI. The predominant findings on T2WI are
heterogeneous-homogeneous hyperintense signals (46); however, Fasih et al (48) reported low signal intensity and Kang
et al (49) reported
isointensity to the myocardium. Of the 24 reported cases that
underwent contrast-enhanced MRI scans, the intraluminal tumors
exhibited mild heterogeneous enhancement in 45.8% cases, mild
homogeneous enhancement in 29.2% and marked enhancement in 25.0%,
while the two present cases showed mild heterogeneous enhancement.
We propose that the diverse pattern of phase-based enhancement may
result from the nourishing vessels of the tumor originating from
the pelvic vasculature.
The differential diagnosis of IVL predominantly
includes thrombi within systemic veins, leiomyosarcoma arising from
the wall of the IVC, right atrial myxoma and malignant thrombosis
with carcinoma (34), as these
entities have similar CT or MRI characteristics to IVL. However,
intravenous thrombi show no enhancement following contrast agent
administration due to their lack of vascular supply. Distinguishing
between IVL and leiomyosarcoma of the IVC is challenging in the
early stages of the disease, however, when the latter presents with
visible infiltration and invasion around structures, diagnosis
becomes more simple (51).
Leiomyosarcoma arises from the vascular wall, and a gap between the
tumor and vascular wall may not be visible on cross-sectional CT
images from a certain point of view. Furthermore, current research
indicates that IVL only occurs in women (52). Right atrial myxoma typically involves
the cardiac chamber and does not normally extend into the IVC. The
features of malignant thrombosis are similar to those of the
primary tumor and the lesion is generally considerably smaller than
the IVL. In addition, malignant thrombosis is not associated with a
history of uterine myoma or surgery for uterine myoma (10). Complete surgical excision of the tumor
is an appropriate treatment option for IVL, and the final diagnosis
is dependent on histopathological analysis.
In conclusion, IVL should be considered upon
presentation of a soft mass in the systemic veins, with or without
extension to the right cardiac chamber, in female patients,
particularly in patients with a history of uterine myoma.
Furthermore, imaging modalities able to display the precise
location and full-scale extension path of the tumor, such as CT and
MRI, are of great importance in the presurgical assessment of
IVL.
References
|
1
|
Norris HJ and Parmley T: Mesenchymal
tumors of the uterus. V. Intravenous leiomyomatosis. A clinical and
pathologic study of 14 cases. Cancer. 36:2164–2178. 1975.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Rajaii-Khorasani A, Kahrom M, Hashemzadeh
M, Tayebi S, Ghazi M and Hamedanchi A: Pulmonary artery extension
of uterine leiomyoma. J Card Surg. 27:466–469. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Dalainas I: Vascular smooth muscle tumors:
Review of the literature. Int J Surg. 6:157–163. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Birch-Hirschfeld FV: Textbook of
Pathological Anatomy (5th). F.C.W. Vogel. Leipzig: 226–258.
1896.(In German).
|
|
5
|
Durck H: Ueber ien kontinvierlich durch
die entere holhlvene in das herz vorwachsendes: Fibromyom des
uterus. Munch Med Wochenschr. 54:11541907.(In German).
|
|
6
|
Borland DS and Wotring JW: Intravenous
leiomyomatosis of the uterus and broad ligament: Report of a case.
Am J Clin Pathol. 42:182–188. 1964. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Lee S, Kim DK, Narm KS and Cho SH:
Pulmonary artery embolization of intravenous leiomyomatosis
extending into the right atrium. Korean J Thorac Cardiovasc Surg.
44:243–246. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Izzat MB, Bayazid S and Shuaibi I: Pelvic
intravenous leiomyomatosis with trans-caval extension to the heart
and pulmonary arteries. J Card Surg. 26:630–631. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Fukuyama A, Yokoyama Y, Futagami M,
Shigeto T, Wada R and Mizunuma H: A case of uterine leiomyoma with
intravenous leiomyomatosis-histological investigation of the
pathological condition. Pathol Oncol Res. 17:171–174. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Osawa H, Hosaka S, Akashi O, Furukawa H
and Egi K: A case of intravenous leiomyomatosis of uterine origin,
extending through the inferior vena cava to right atrium. Gen
Thorac Cardiovasc Surg. 61:104–107. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Yaguchi C, Oi H, Kobayashi H, Miura K and
Kanayama N: A case of intravenous leiomyomatosis with high levels
of hyaluronan. J Obstet Gynaecol Res. 36:454–458. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Leitman M, Kuperstein R, Medalion B,
Stamler A, Porat E, Rosenblatt S, Konen E, Krakover R and Vered Z:
A highly unusual right atrial mass presented in two women. Eur J
Echocardiogr. 9:833–834. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Rispoli P, Santovito D, Tallia C, Varetto
G, Conforti M and Rinaldi M: A one-stage approach to the treatment
of intravenous leiomyomatosis extending to the right heart. J Vasc
Surg. 52:212–215. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Bender LC, Mitsumori LM, Lloyd KA and
Stambaugh LE III: AIRP best cases in radiologic-pathologic
correlation: Intravenous leiomyomatosis. Radiographics.
31:1053–1058. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Ozer N, Engin H, Akgül E, Sahiner L,
Atalar E, Aksöyek S, Ovünç K, Ozmen F and Kes S: An unusual case of
recurrent mass in the right atrium: Intravenous leiomyomatosis.
Echocardiography. 22:514–516. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Liu W, Liu M and Xue J: Detection of
intravenous leiomyomatosis with intracardiac extension by
ultrasonography: A case report. Oncol Lett. 6:336–338.
2013.PubMed/NCBI
|
|
17
|
Matos AP, Ramalho M, Palas J and Herédia
V: Heart extension of an intravenous leiomyomatosis. Clin Imaging.
37:369–373. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Wakiyama H, Sugimoto T, Ataka K, Yamashita
C, Tsuji Y, Nakagiri K, Inoue K and Okada M: Intravenous
leiomyomatosis extending into the right ventricular cavity:
One-stage radical operation using cardiopulmonary bypass - a case
report. Angiology. 51:505–509. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Lou YF, Shi XP and Song ZZ: Intravenous
leiomyomatosis of the uterus with extension to the right heart.
Cardiovasc Ultrasound. 9:252011. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Robert-Ebadi H, Terraz S, Mach N,
Dubuisson JB, Kalangos A and Bounameaux H: Intravenous
leiomyomatosis of the uterus: Link with new fertilisation methods?
Swiss Med Wkly. 139:4362009.PubMed/NCBI
|
|
21
|
Barksdale J, Abolhoda A and Saremi F:
Intravenous leiomyomatosis presenting as acute Budd-Chiari
syndrome. J Vasc Surg. 54:860–863. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Biri A, Korucuoglu U, Zumrutbas N, Tiras B
and Guner H: Intravenous leiomyomatosis treated with aromatase
inhibitor therapy. Int J Gynaecol Obstet. 1013:299–300. 2008.
View Article : Google Scholar
|
|
23
|
Saitoh M, Hayasaka T, Nakahara K, Ohmichi
M, Shimazaki Y and Kurachi H: Intravenous leiomyomatosis with
cardiac extension. Gynecol Obstet Invest. 58:168–170. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Harris LM and Karakousis CP: Intravenous
leiomyomatosis with cardiac extension: Tumor thrombectomy through
an abdominal approach. J Vasc Surg. 31:1046–1051. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Fang BR, Ng YT and Yeh CH: Intravenous
leiomyomatosis with extension to the heart: Echocardiographic
features: A case report. Angiology. 58:376–379. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Liu B, Liu C, Guan H, Li Y, Song X, Shen K
and Miao Q: Intravenous leiomyomatosis with inferior vena cava and
heart extension. J Vasc Surg. 50:897–902. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Clay TD, Dimitriou J, McNally OM, Russell
PA, Newcomb AE and Wilson AM: Intravenous leiomyomatosis with
intracardiac extension - a review of diagnosis and management with
an illustrative case. Surg Oncol. 22:e44–e52. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Wu CK, Luo JL, Yang CY, Huang YT, Wu XM,
Cheng CL, Chiang FT and Tseng CD: Intravenous leiomyomatosis with
intracardiac extension. Inter Med. 48:997–1001. 2009. View Article : Google Scholar
|
|
29
|
Singh T, Lamont PM, Otton GR and Thomson
DS: Intravenous leiomyomatosis with intracardiac extension: First
reported case in Australia. Heart Lung Circ. 19:50–52. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Li YQ, Mei F, Yang C, Lv P, Ouyang C and
Jin B: Intravenous leiomyomatosis with right heart involvement - a
report of 4 cases and literature review. J Huazhong Univ Sci
Technolog Med Sci. 31:586–588. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Wong YY, Chu WC and Lam WW: Intravenous
leiomyomatosis: Computed tomography diagnosis. Hong Kong Med J.
12:239–240. 2006.PubMed/NCBI
|
|
32
|
Peng HJ, Zhao B, Yao QW, Qi HT, Xu ZD and
Liu C: Intravenous leiomyomatosis: CT findings. Abdom Imaging.
37:628–631. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Ahmed M, Zangos S, Bechstein WO and Vogl
TJ: Intravenous leiomyomatosis. Eur Radiol. 14:1316–1317. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Bilyeu SP, Bilyeu JD and Parthasarathy R:
Intravenous lipoleiomyomatosis. Clin Imaging. 30:361–364. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Moorjani N, Kuo J, Ashley S and Hughes G:
Intravenous uterine leiomyosarcomatosis with intracardial
extension. J Card Surg. 20:382–385. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Lai TK, Huang HY, Chan RY, Chin AC, Wong
WC, Sit CY, Chan LK, Chung TK, Chu WS, Lo CF and Ng TW: Magnetic
resonance venogram of intravenous leiomyomatosis. Hong Kong Med J.
11:524–526. 2005.PubMed/NCBI
|
|
37
|
Demirkiran F, Sal V, Kaya U, Alhan C and
Tokgozoglu N: Intravenous leiomyoma with extension to the heart: A
case report and review of the literature. Case Rep Obstet Gynecol.
2013:6024072013.PubMed/NCBI
|
|
38
|
Nam MS, Jeon MJ, Kim YT, Kim JW, Park KH
and Hong YS: Pelvic leiomyomatosis with intracaval and intracardiac
extension: A case report and review of the literature. Gynecol
Oncol. 89:175–180. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Kokawa K, Yamoto M, Yata C, Mabuchi Y and
Umesaki N: Postmenopausal intravenous leiomyomatosis with high
levels of estradiol and estrogen receptor. Obstet Gynecol.
100:1124–1126. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Esmaeilzadeh M, Tavakolli A and Safaei A:
Recurrent intracardiac leiomyomatosis. Can J Cardiol. 23:1085–1086.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Elkington NM and Carlton M: Recurrent
intravenous leiomyomatosis with extension up the inferior vena
cava. Aust N Z J Obstet Gynaecol. 45:1672005. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Cea-Calvo L, Lozano F, Pombo M, Serrano A,
Rodríguez E, Porto J, Pozuelo A and González C: Images in
cardiovascular medicine. Uterine intravenous leiomyomatosis
extending through the inferior vena cava into the right cardiac
cavities. Circulation. 101:581–583. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Xu ZF, Yong F, Chen YY and Pan AZ: Uterine
intravenous leiomyomatosis with cardiac extension: Imaging
characteristics and literature review. World J Clin Oncol. 4:25–28.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Sogabe M, Kawahito K, Aizawa K, Sato H and
Misawa Y: Uterine intravenous leiomyomatosis with right ventricular
extension. Ann Thorac Cardiovasc Surg. 20(Suppl): 933–936. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Moniaga NC and Randall LM: Uterine
leiomyomatosis with intracaval and intracardiac extension. Gynecol
Oncol Rep. 2:130–132. 2012. View Article : Google Scholar
|
|
46
|
Kocaoglu M, Bulakbasi N, Ugurel MS, Ors F,
Tayfun C and Ucoz T: Value of magnetic resonance imaging in the
depiction of intravenous leiomyomatosis extending into the heart. J
Comput Assist Tomogr. 27:630–633. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Kawakami S, Sagoh T, Kumada H, Kimoto T,
Togashi K, Nishimura K, Honda H, Yamada M and Noguchi M:
Intravenous leiomyomatosis of uterus: MR appearance. J Comput
Assist Tomogr. 15:686–689. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Fasih N, Prasad Shanbhogue AK, Macdonald
DB, Fraser-Hill MA, Papadatos D, Kielar AZ, Doherty GP, Walsh C,
McInnes M and Atri M: Leiomyomas beyond the uterus: Unusual
locations, rare manifestations. Radiographics. 28:1931–1948. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Kang LQ, Zhang B, Liu BG and Liu FH:
Diagnosis of intravenous leiomyomatosis extending to heart with
emphasis on magnetic resonance imaging. Chin Med J (Engl).
125:33–37. 2012.PubMed/NCBI
|
|
50
|
Cohen DT, Oliva E, Hahn PF, Fuller AF Jr
and Lee SI: Uterine smooth-muscle tumors with unusual growth
patterns: Imaging with pathologic correlation. AJR Am J Roentgenol.
188:246–255. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
McDonald DK, Kalva SP, Fan CM and Vasilyev
A: Leiomyosarcoma of the uterus with intravascular tumor extension
and pulmonary tumor embolism. Cardiovasc Intervent Radiol.
30:140–142. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Huang J, Liu G, Lu JP, Wang F, Wang L and
Jin AG: Primary intraluminal leiomyosarcoma of the inferior vena
cava: Value of MRI with contrast-enhanced MR venography in
diagnosis and treatment. Abdom Imaging. 36:337–341. 2011.
View Article : Google Scholar : PubMed/NCBI
|