Introduction
Gastric cancer is a malignant tumor with a poor
prognosis, and the various treatments available at present,
including surgery, chemotherapy and radiotherapy, remain
unsatisfactory (1). Development of
gastric cancer is associated with a number of molecular
abnormalities, the majority of which affect the downstream signal
transduction pathways involved in cell growth and differentiation
(2,3).
Investigation into such molecules is expected to provide useful
prognostic biomarkers of gastric cancer that will aid in
determining the treatment plan for individual patients. For
example, methylation of the XIAP-associated factor 1 promoter
(4), and expression of 14–3-3σ
(5) and miR-200c (6) have been reported to be important for the
prediction of poor prognosis in gastric cancer patients; however,
further investigation is required.
Induced pluripotent stem (iPS) cells are cells that
have acquired pluripotency following the introduction of various
factors; octamer-binding transcription factor (Oct)3/4 and
sex-determining region Y-box 2 (SOX2) plus Krüppel-like factor 4
(KLF4) and avian myelocytomatosis viral oncogene homolog (c-Myc),
or Nanog and LIN28 have been shown to induce pluripotency in
various murine and human cells (e.g., fibroblasts) (7,8). These
pluripotency-inducing factors have been detected in embryonic stem
cells, as well as in normal cells and cancer cells, including
gastric cancer (9). Although these
factors are necessary in order for stem cells to acquire
pluripotency, it has been suggested that they may have oncogenic
potential in normal cells (10).
Expression of SOX2 has been reported to be important
for tumorigenicity and chemoresistance (11). However, the inhibition of gastric
cancer cell growth and the induction of apoptosis by SOX2 has also
been reported (12); thus, the
precise role of SOX2 remains to be clarified. Similarly, the
transcription factor KLF4 has also been reported to be associated
with tumor suppression as well as oncogenesis (13). KLF4 has been detected in cancer cells
in gastric cancer (14), and has been
proposed to be a useful biomarker; however, its exact role in
gastric cancer cells remains unclear.
In the present study, the expression of five
pluripotency-inducing factors in human gastric cancer specimens
were investigated by immunohistochemistry and analyzed with respect
to clinicopathological characteristics, revealing that decreased
KLF4 expression was associated with poor prognosis in these
patients. These data indicate that KLF4 may be useful a molecular
marker for poor prognosis in gastric cancer.
Materials and methods
Patients
Out of 130 consecutive primary gastric cancer
patients who underwent surgery at the Department of Surgery and
Science, Graduate school of Medicine and Pharmaceutical Sciences
for Research, University of Toyama (Toyama, Japan) between January
2001 and June 2006, 108 cases were evaluated. A total of 22 cases
were excluded in which the expression of the markers (C-Myc, Sox2,
Nanog, KLF4 and Oct4) could not be evaluated due to peeling of the
specimen from the slide. The depth of tumor invasion, the extent of
lymph node metastasis and lymphovascular and vascular invasion, and
the histological types were classified by the pathologists of
Toyama University Hospital. The final pathological stage was
confirmed according to the Union for International Cancer Control
(UICC) classification system (15).
The study protocol was approved by the Ethics Committee of the
University of Toyama.
Construction of tissue microarray
blocks
The expression of KLF4, Nanog, Oct4, SOX2 and c-MYC
were investigated using a tissue microarray (TMA1150) created from
resected gastric cancer specimens at Toyama University Hospital.
Tumor areas with matched hematoxylin- and eosin-stained slides were
selected and marked directly on the donor block. A cylindrical
tissue sample (diameter, 0.6 mm) was cored from the selected region
in the donor block and inserted directly into the recipient block.
A total of 108 gastric cancer tissues were included in the array
block. Multiple 4-µm sections were cut with a microtome and
transferred to Superfrost Plus glass slides (Thermo Fisher
Scientific, Inc., Waltham, MA, USA).
Antibodies
The primary antibodies used in
immunohistochemical staining were as follows: Anti-c-Myc
(IgG1 mouse monoclonal antibody; clone 9E10; #sc-40;
Santa Cruz Biotechnology, Inc., Santa Cruz, CA, USA); anti-KLF4
(IgG rabbit polyclonal antibody; #ab34814; Abcam, Cambridge, UK);
anti-Nanog (IgG rabbit polyclonal antibody; #IHC-00205; Bethyl
Laboratories, Inc., Montgomery, TX, USA); anti-Oct4 (IgG rabbit
polyclonal antibody; #ab19857; Abcam); and anti-SOX2 (IgG rabbit
polyclonal antibody; #AB5603; EMD Millipore, Billerica, MA,
USA).
Immunohistochemical staining
Slides were incubated for 60 min with the primary
antibodies at an optimized titer, diluted using Universal Blocking
Reagent (BioGenex, Fremont, CA, USA). The antibodies were used at
the following dilutions: KLF4, 1:100; Oct4, 1:100; Sox2, 1:3,200;
C-Myc, 1:50; and Nanog, 1:500, and incubated at room temperature
for 30 min. Following three washes in PBS, each series of sections
was incubated for 30 min at room temperature with anti-mouse IgG1
goat polyclonal antibody (#A90-105B; Bethyl Laboratories, Inc.) and
anti-rabbit IgG-Fc fragment goat polyclonal antibody (#A120-111B;
Bethyl Laboratories, Inc.). diluted 1:250 in Universal Blocking
Reagent. Following a further three washes in PBS, the slides were
incubated for 45 min with avidin-biotin complex reagent (Vectastain
Elite ABC kit; Vector Laboratories, Inc.) at room temperature. The
reaction products were rinsed twice with PBS, placed in 0.05 M
Tris-HCl buffer (pH 7.5) for 5 min, and then developed in liquid
3,3-diaminobenzidine (Dako, Glostrup, Denmark) for 3 min. Following
the development, sections were washed twice with distilled water,
lightly counterstained with Mayer's hematoxylin, dehydrated,
cleared, and mounted with resinous mounting medium. All procedures
were conducted at room temperature.
Pathological and immunohistochemical
analysis
Two pathologists investigated the
Tumor-Node-Metastasis (TNM) classification, according to the
American Joint Committee on Cancer (AJCC)/UICC criteria (16), for each patient who underwent surgery
for the treatment of gastric cancer. The pathologist also analyzed
the expression of each gene independently, and scored the intensity
of expression [0 (no expression), 1 (weak expression), 2 (moderate
expression) or 3 (strong expression)] as well as the distribution
of expression [0 (no staining), 1 (1–50% of tumor cells stained),
or 2 (50–100% of tumor cells stained)]. On the basis of the total
score (the sum of the intensity and distribution scores), each
patient was classified into one of two groups: The low expression
group (total score, 0–2) or the high expression group (total score,
3–5) (17,18).
Statistical methods
The χ2 test was used to compare
clinicopathological data. The overall survival (OS) rate following
surgery was estimated for each group using the Kaplan-Meier method,
and differences were assessed by the log-rank test and Wilcoxon
test. P<0.05 was considered to indicate statistical
significance. All analyses were performed with JMP 11.0 software
(SAS Institute, Inc., Cary, NC, USA).
Results
Patient characteristics
The clinical characteristics of the 108 gastric
cancer patients are summarized in Table
I. The median age of the patients was 70 years (range, 44–86
years), and the number of males (n=77; 71.3%) was more than twice
that of the females (n=31; 28.7%). Tumor invasion of pT3 or above
was present in 81 patients (75.0%), including 50 cases with pT4.
Lymph node metastasis was identified in 72.2% of the patients.
Lymphovascular and vascular invasion were present in 85.2 and 73.1%
of patients, respectively. Advanced gastric cancer (stage II or
higher) was present in 79 patients (73.1%). Chemotherapy was
administered preoperatively to 19 patients (17.6%) and
postoperatively to 61 patients (56.5%), and 21 (34.4%) of those
that received postoperative chemotherapy relapsed. During the
post-surgical follow-up period, relapse of gastric cancer occurred
in 72 patients (66.7%), of which 64 patients (88.9% of relapses)
succumbed to the disease. Factors involved in relapse were as
follows: Peritoneal metastasis (34 patients), local recurrence (1
patient), liver metastasis (5 patients), bone metastasis (2
patients), lymph node metastasis (10 patients) and brain metastasis
(1 patient). The median post-surgical follow-up period was 56
months (range, 1–165 months).
 | Table I.Patient characteristics (all cases,
n=108). |
Table I.
Patient characteristics (all cases,
n=108).
| Characteristic | Value | % |
|---|
| Age (years) |
|
|
|
Median | 70 | – |
|
Range | 44–86 | – |
| Gender, n |
|
|
|
Male | 77 | 71.3 |
|
Female | 31 | 28.7 |
| Tumor invasion,
n |
|
|
| T1 | 8 | 7.4 |
| T2 | 19 | 17.6 |
| T3 | 31 | 28.7 |
| T4 | 50 | 46.3 |
| Lymph node
metastasis, n |
|
|
|
Positive | 78 | 72.2 |
|
Negative | 30 | 27.8 |
| Lymphovascular
invasion, n |
|
|
|
Positive | 92 | 85.2 |
|
Negative | 16 | 14.8 |
| Vascular invasion,
n |
|
|
|
Positive | 79 | 73.1 |
|
Negative | 29 | 26.9 |
| Histology, n |
|
|
|
Intestinal | 48 | 44.4 |
|
Diffuse | 60 | 55.6 |
| Preoperative
chemotherapy, n |
|
|
|
Administered | 19 | 17.6 |
| Not
administered | 89 | 82.4 |
| Postoperative
chemotherapy, n |
|
|
|
Administered | 61 | 56.5 |
| Not
administered | 47 | 43.5 |
| UICC stage, n |
|
|
| I | 29 | 26.9 |
| II | 31 | 28.7 |
|
III | 17 | 15.7 |
| IV | 31 | 28.7 |
Expression of pluripotency-inducing
factors
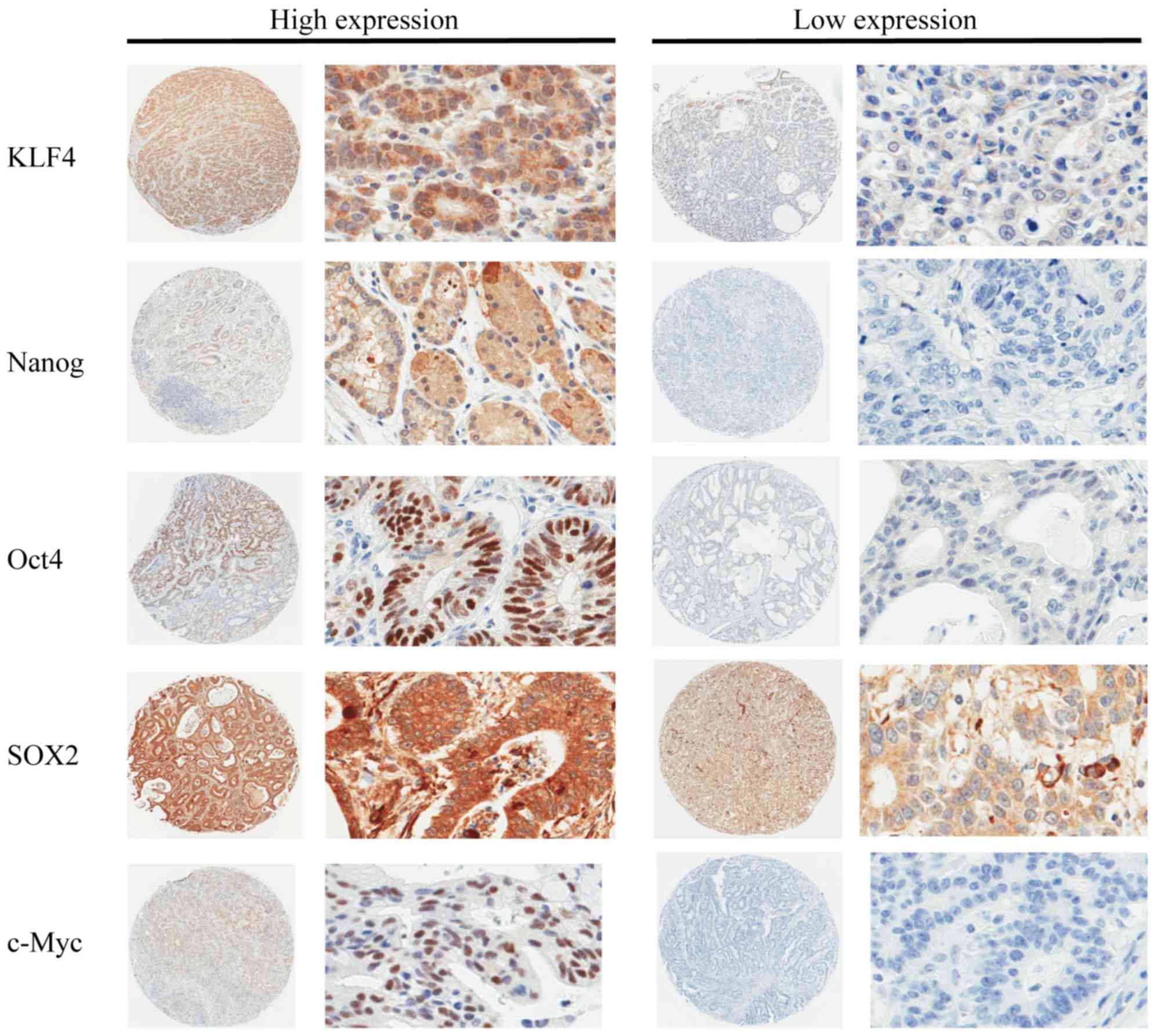
The expression levels of KLF4, Nanog, Oct4, SOX2 and
c-Myc were analyzed in tissue specimens from the 108 patients.
Representative stained samples from the high and low expression
groups for each factor are shown in Fig.
1. Following incubation with the anti-Nanog, anti-Oct4, and
anti-c-Myc antibodies, staining was predominantly observed in the
nuclei, while a lower rate of cytoplasmic staining was also
visible. Nuclear and cytoplasmic staining were present to the same
degree following immunohistochemical staining with anti-KLF4 and
anti-SOX2 antibodies. The cell membranes in the gastric cancer
specimens were not stained in this immunohistochemical analysis.
Among the 108 cases, the overall ratios of patients in the high:low
expression groups for each factor were as follows: KLF4, 72:36;
Nanog, 59:49; OCT4, 41:67; SOX2, 42:66; and c-Myc, 13:95.
Furthermore, the mean immunohistochemistry scores (high:low
expression group) for each factor were as follows: KLF4,
3.527:1.444; Nanog, 3.556:0.551; OCT4, 3.390:0.026; SOX2,
4.333:2.803; and c-Myc, 2.538:0.00.
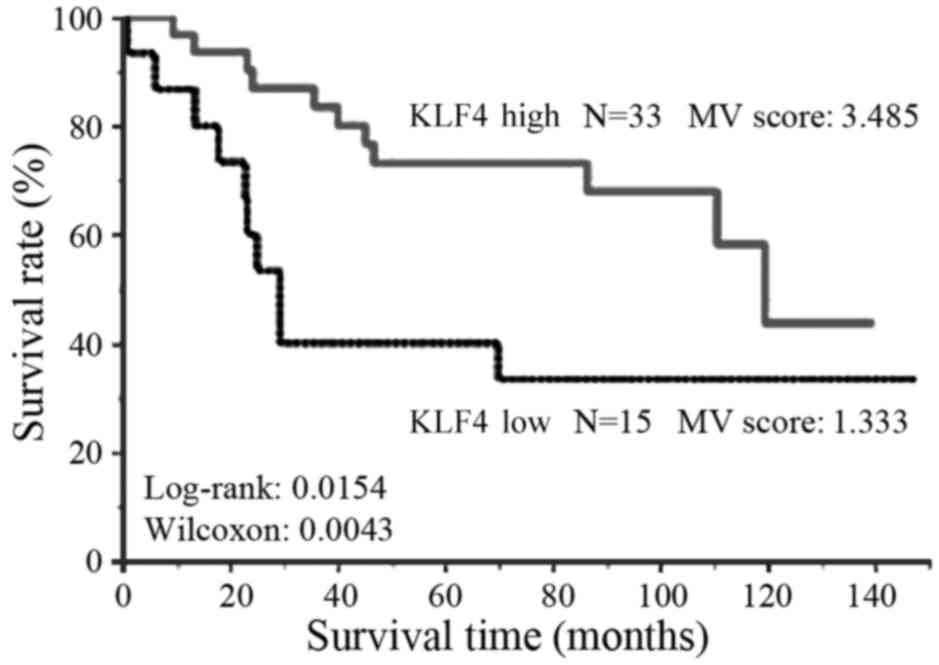
The expression level of KLF4 was also analyzed in
the group of 48 patients who underwent R0 resection for stage
II–III gastric cancer. High KLF4 expression was observed in 33
cases, while the remaining 15 cases exhibited low expression. These
data indicate that the expression level of KLF4 was not
significantly altered as the cancer stage increased.
Survival
The associations between the expression of each
pluripotency-inducing factor and OS rate were assessed in all 108
patients (Fig. 2) and in the stage
II–III patients who underwent R0 resection (Fig. 3). The results indicated that high
expression KLF4 was significantly associated with a more favorable
OS rate (P=0.0359); this difference in prognosis became more
pronounced in the stage II–III cases (P=0.0042). No significant
associations were identified between the other
pluripotency-inducing factors and OS rate.
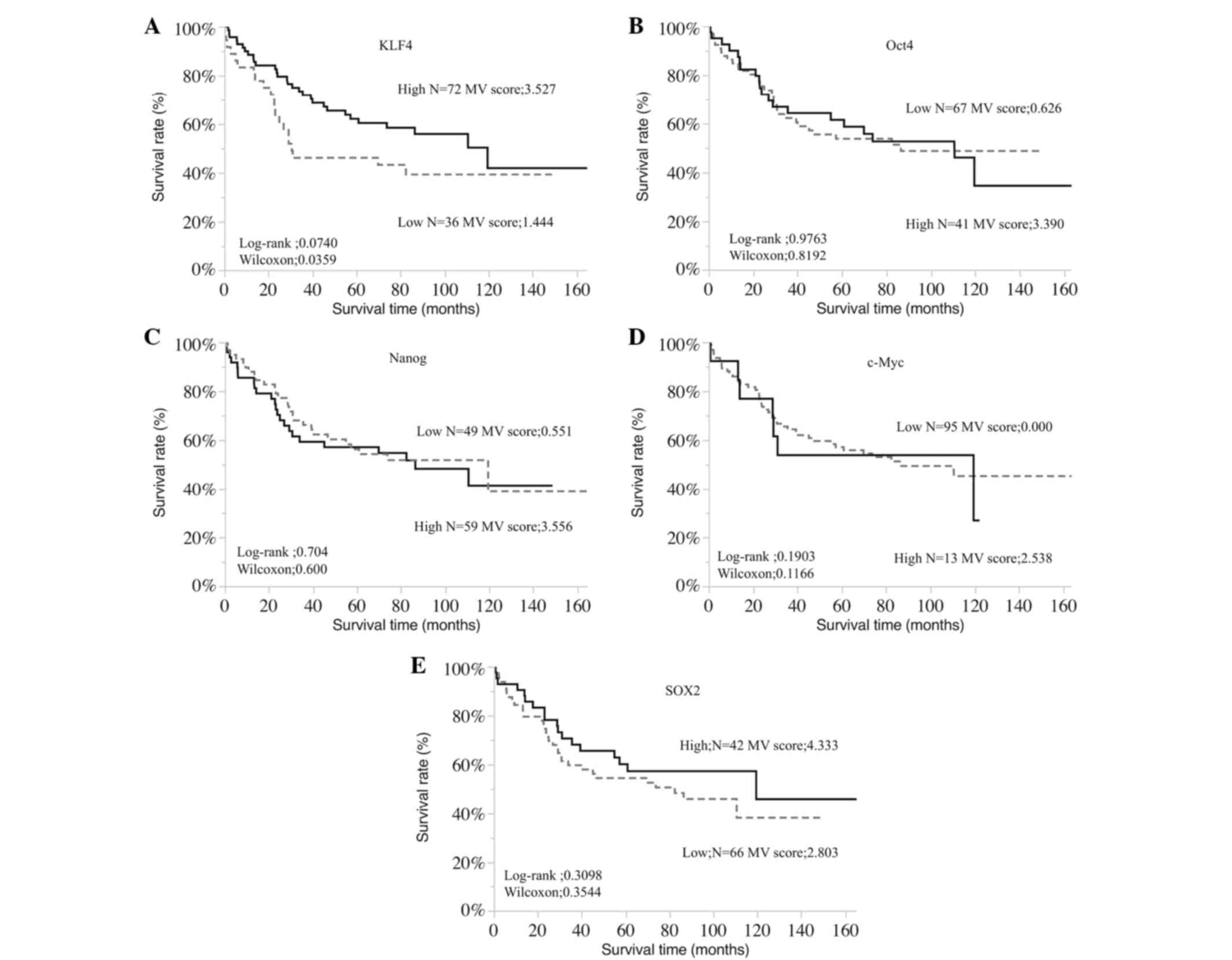 | Figure 2.Overall survival rates of gastric
cancer patients according to the expression of (A) KLF4, (B) Oct4,
(C) Nanog, (D) c-Myc and (E) SOX2. Kaplan-Meier analysis revealed a
significantly less favorable overall survival rate in patients with
low KLF4 expression compared with those with high expression
(log-rank, P=0.0740; Wilcoxon, P=0.0359). MV, mean value of
immunohistochemistry scores. KLF4, Krüppel-like factor 4; Oct4,
octamer-binding transcription factor 4; c-Myc, avian
myelocytomatosis viral oncogene homolog; SOX2, sex-determining
region Y-box 2. |
Associations between KLF4 and
clinicopathological factors
Table II shows the
correlations between the expression of KLF4 and the
clinicopathological characteristics of gastric cancer patients.
Patient age and gender, tumor invasion, number of metastatic lymph
nodes, lymphovascular and vascular invasion, histology, stage,
preoperative chemotherapy and postoperative chemotherapy were
analyzed, revealing no correlations with the KLF4 expression.
Similarly, in patients of stage II–III (n=48) who underwent R0
resection, the same clinicopathological variables were not
identified to be significantly associated with the expression of
KLF4 (Table II).
| Table II.Association between patient
characteristics and KLF4 expression in gastric cancer of various
stages. |
Table II.
Association between patient
characteristics and KLF4 expression in gastric cancer of various
stages.
|
| All stages | Stage II–III |
|---|
|
|
|
|
|---|
|
| KLF4
expression |
| KLF4
expression |
|
|---|
|
|
|
|
|
|
|---|
| Variable | Low (n=36) | High (n=72) | P-value | Low (n=15) | High (n=33) | P-value |
|---|
| Age (years),
median | 69 | 70 | 0.76 | 70 | 69 | 0.76 |
| Gender, n |
|
| 0.75 |
|
| 0.36 |
|
Male | 25 | 57 |
| 10 | 26 |
|
|
Female | 11 | 15 |
| 5 | 7 |
|
| Tumor invasion,
n |
|
| 0.27 |
|
| 0.27 |
|
≤T2 | 20 | 35 |
| 13 | 28 |
|
|
>T2 | 16 | 37 |
| 2 | 5 |
|
| LN metastasis,
n |
|
| 0.65 |
|
| 0.21 |
|
Positive | 27 | 51 |
| 14 | 26 |
|
|
Negative | 9 | 21 |
| 1 | 7 |
|
| Number of
metastatic LNs, n |
|
| 0.87 |
|
| 0.38 |
|
<7 | 26 | 53 |
| 9 | 24 |
|
| ≥7 | 10 | 19 |
| 6 | 9 |
|
| M stage, n |
|
| 0.76 |
|
| – |
| 0 | 25 | 52 |
| – | – |
|
| 1 | 11 | 20 |
| – | – |
|
| Lymphovascular
invasion, n |
|
| 0.41 |
|
| 0.23 |
|
Positive | 22 | 38 |
| 15 | 30 |
|
|
Negative | 14 | 34 |
| 0 | 3 |
|
| Vascular invasion,
n |
|
| 0.54 |
|
| 0.29 |
|
Positive | 25 | 54 |
| 13 | 24 |
|
|
Negative | 11 | 18 |
| 2 | 9 |
|
| Histology, n |
|
| 0.41 |
|
| 0.33 |
|
Intestinal | 22 | 38 |
| 10 | 17 |
|
|
Diffuse | 14 | 34 |
| 5 | 16 |
|
| Tumor size
(cm) |
|
|
|
|
|
|
|
Median | 5.0 | 5.6 | 0.43a | 6.0 | 5.0 | 0.35a |
| <5,
n | 15 | 27 |
| 7 | 14 |
|
| ≥5,
n | 21 | 45 | 0.67b | 8 | 19 | 0.78b |
| Preoperative
chemotherapy, n |
|
| 0.37 |
|
| 0.5 |
|
Administered | 8 | 11 |
| 4 | 6 |
|
| Not
administered | 28 | 61 |
| 11 | 27 |
|
| Postoperative
chemotherapy, n |
|
| 0.33 |
|
| 0.28 |
|
Administered | 18 | 43 |
| 10 | 27 |
|
| Not
administered | 18 | 29 |
| 5 | 6 |
|
Prognostic relevance of KLF4
expression
The associations of various clinicopathological
factors with the prognosis of gastric cancer patients (all cases,
n=108) are shown in Table IIIA.
According to the results of the log-rank univariate analysis, the
negative prognostic factors included tumor invasion ≥T3
(P<0.001), positive lymphovascular invasion (P<0.001) and
vascular invasion (P=0.0256), ≥7 metastatic lymph nodes (P=0.0012),
tumor size ≥5 cm (P=0.0287), and low expression of KLF4 (P=0.0359).
The multivariate Cox proportional hazards analysis also revealed
that low expression of KLF4 was an independent poor prognostic
factor (P=0.0331).
| Table III.Univariate (log-rank) and
multivariate (Cox proportional hazards) analyses of the association
between patient characteristics and prognosis in gastric
cancer. |
Table III.
Univariate (log-rank) and
multivariate (Cox proportional hazards) analyses of the association
between patient characteristics and prognosis in gastric
cancer.
| A, All stages |
|---|
|
|---|
|
| Univariate | Multivariate |
|---|
|
|
|
|
|---|
| Factor | P-value | Risk ratio | 95% CI | P-value |
|---|
| Gender (male vs.
female) | 0.157 | 1.58 | 0.768–1.928 | 0.426 |
| Age (≥70 vs. <70
years) | 0.135 | 1.20 | 0.917–2.803 | 0.100 |
| Tumor invasion (≥T3
vs. <T3) |
<0.001a | 1.83 | 1.159–2.892 | 0.007a |
| Number of
metastatic LNs (≥7 vs. <7) |
<0.001a | 1.28 | 0.754–2.211 | 0.358 |
| M stage (1 vs.
0) |
<0.001a | 1.98 | 1.143–3.366 | 0.015a |
| Lymphovascular
invasion (+ vs. −) |
<0.001a | 1.82 | 1.127–2.935 | 0.010a |
| Vascular invasion
(+ vs. −) | 0.026a | 1.33 | 0.858–2.056 | 0.200 |
| Tumor size (≥5 vs.
<5 cm) | 0.029a | 1.16 | 0.738–1.855 | 0.507 |
| KLF4 expression
(low vs. high) | 0.036a | 2.04 | 1.118–3.682 | 0.033a |
| Nanog expression
(low vs. high) | 0.600 | – | – | – |
| Oct4 expression
(high vs. low) | 0.819 | – | – | – |
| SOX2 expression
(high vs. low) | 0.354 | – | – | – |
| c-Myc expression
(high vs. low) | 0.896 | – | – | – |
|
| B, Stage
II–III |
|
|
|
|
|
|
| Univariate | Multivariate |
|
|
|
|
| Factor | P-value | Risk ratio | 95% CI | P-value |
|
| Gender (male vs.
female) | 0.103 | 4.68 | 1.143–32.195 | 0.030a |
| Age (≥70 vs. <70
years) | 0.175 | 1.91 | 0.607–5.512 | 0.256 |
| Tumor invasion (≥T3
vs. <T3) | 0.027a | 1.93 | 0.740–5.162 | 0.176 |
| Lymphovascular
invasion (+ vs. −) |
<0.001a | 4.52 | 1.178–22.472 | 0.027a |
| Vascular invasion
(+ vs. −) | 0.010a | 3.42 | 0.792–13.944 | 0.096 |
| Number of
metastatic LNs (≥7 vs. <7) | 0.001a | 1.12 | 0.342–3.379 | 0.854 |
| KLF4 expression
(low vs. high) | 0.004a | 4.39 | 1.578–12.808 | 0.005a |
In the patients with stage II–III gastric cancer
(n=48) who underwent R0 resection, the results of the log-rank
univariate analysis revealed that the poor prognostic factors
included tumor invasion ≥T3 (P=0.0271), positive lymphovascular
invasion (P<0.001) and vascular invasion (P=0.0098), ≥7
metastatic lymph nodes (P=0.0014), and low expression of KLF4
(P=0.0042). Furthermore, the Cox's proportional hazards analysis
revealed that low expression of KLF4 was an independent poor
prognostic factor (P=0.0048) (Table
IIIB).
Discussion
KLF4 is a zinc-finger transcription factor that is
highly expressed in post-mitotic and terminally differentiated
epithelial tissues, including those of the gastrointestinal tract,
skin and lungs (19,20). In the present study, KLF4 was found to
be expressed in the cytoplasm and nuclei of gastric cancer cells,
and its decreased expression was associated with a poor prognosis.
It has been proposed that the regulation of KLF4 expression is
involved in transcriptional and post-transcriptional regulation in
gastric cancer (21). Liu et
al (22) reported that KLF4 was
predominantly expressed in the cytoplasm, rather than the nuclei,
of nasopharyngeal carcinoma cells, and that the decreased
expression of KLF4 in the cytoplasm was associated with poor
prognosis in these cancer patients. Chen et al (23) reported that KLF4 existed predominantly
in the nuclei of oral cancer cells, and also that the loss of KLF4
in the nuclei was associated with poor prognosis. These reports
suggest that the localization of KLF4 may differ between organs or
according to the role of KLF4; however, it is notable that the
decrease in KLF4 was associated with the progression of the
cancer.
With regard to the presence of KLF4 in tumor cells,
various studies have revealed decreased KLF4 expression in patients
with nasopharyngeal (22), colorectal
(24), renal (25), lung (26), cervical (27) and breast cancer (28) who had poor prognosis. Based on these
results, KLF4 was suggested to function as a tumor suppressor.
Accordingly, the overexpression of KLF4 was demonstrated to inhibit
cell growth, migration, invasion and metastasis in liver, lung and
colorectal cancer (29–31), and induce tumor cell apoptosis in
esophageal cancer (32) and bladder
cancer (33). These functional
investigations also suggested that the loss of KLF4 expression may
be involved in the initiation and formation of precancerous lesions
in various cancer types. Previous multivariate analyses revealed
that decreased expression of KLF4 protein was a significant
predictor of poor prognosis for patients with several cancer types
regardless of the clinical stage (30,34). Thus,
KLF4 downregulation appears to be an independent prognostic factor
in various types of malignant tumors.
Japanese gastric cancer treatment guidelines
recommend that adjuvant chemotherapy is administered following the
standard surgical treatment for patients with gastric cancer of
stage II–III (35). The standard
surgical treatment for gastric cancer in Japan is defined as the
excision of more than two-thirds of the stomach and the dissection
of lymph nodes up to the D2 area. This procedure is widely
performed in Japan, with few prognostic differences between
gastrectomy and D2 area lymph node dissection. In the present
study, when the analysis was limited to patients with stage II–III
gastric cancer, a more pronounced difference in prognosis according
to KLF4 expression was observed, as compared with the analysis of
all stages. Thus, it is hypothesized that the expression of KLF4 is
an independent prognostic factor that is not affected by the
progression of the tumor or the treatment methods.
Several reports have indicated that KLF4 is an
important regulator of tumor cell proliferation. Wei et al
(14) reported that increased
expression of KLF4 induced cell cycle arrest and apoptosis in
gastric cancer cells. Consistently, KLF4 has been shown to induce
apoptosis in bladder cancer (33),
colon cancer (36) and leukemia
(37) cells. The mechanism of
apoptosis induction by KLF4 has not been elucidated. In HT-29 human
colon adenocarcinoma cells, KLF4 overexpression was revealed to
significantly inhibit the mRNA expression of cyclin D1, as well as
the activity of the cyclin D1 gene promoter, and induce cell cycle
arrest at the G1/S boundary (38).
These data indicate that KLF4 may function as a transcriptional
repressor of cyclin D1 to regulate colon cell growth. Tiwari et
al (39) reported that
suppressing KLF4 in breast cancer cells induces mitogen-activated
protein kinase 8-mediated epithelial-mesenchymal transition. KLF4
may therefore be involved in cancer metastasis.
In summary, the present study investigated the
expression levels of five pluripotency-inducing factors (c-Myc,
KLF4, Nanog, Oct4, and SOX2) in gastric cancer specimens, and the
association between the expression of KLF4 and the prognosis of
gastric cancer patients was also assessed, indicating that low KLF4
expression was an independent negative prognostic factor. It is
suggested that KLF4 may exert a suppressive effect on the
proliferation and metastasis of this type of cancer. Furthermore,
the expression and activity of pluripotency-inducing factors in
CSCs may be an important direction for cancer research in the
future.
Acknowledgements
The authors are grateful to Dr Takashi Hori
(Department of Pathology, University of Toyama) for providing
valuable technical assistance. This study was supported by grants
from the Ministry of Education, Culture, Sports, Science and
Technology of Japan.
References
|
1
|
Catalano V, Labianca R, Beretta GD, Gatta
G, de Braud F and Van Cutsem E: Gastric cancer. Crit Rev Oncol
Hematol. 71:127–164. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chan AO, Luk JM, Hui WM and Lam SK:
Molecular biology of gastric carcinoma: From laboratory to bedside.
J Gastroenterol Hepatol. 14:1150–1160. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Fenoglio-Preiser CM, Wang J, Stemmermann
GN and Noffsinger A: TP53 and gastric carcinoma: A review. Hum
Mutat. 21:258–270. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Lin ZQ, Lv P, Lu XX, Yu JL, Han J, Ying
LS, Zhu X, Zhu WY, Fang XH, Wang S and Wu YC: Circulating
methylated XAF1 DNA indicates poor prognosis for gastric cancer.
PLoS One. 8:e671952013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Li YL, Liu L, Xiao Y, Zeng T and Zeng C:
14-3-3σ is an independent prognostic biomarker for gastric cancer
and is associated with apoptosis and proliferation in gastric
cancer. Oncol Lett. 9:290–294. 2015.PubMed/NCBI
|
|
6
|
Valladares-Ayerbes M, Reboredo M,
MedinaVillaamil V, Iglesias-Díaz P, Lorenzo-Patiño MJ, Haz M,
Santamaria I, Blanco M, Fernández-Tajes J, Quindós M, et al:
Circulating miR-200c as a diagnostic and prognostic biomarker for
gastric cancer. J Transl Med. 10:1862012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Takahashi K and Yamanaka S: Induction of
pluripotent stem cells from mouse embryonic and adult fibroblast
cultures by defined factors. Cell. 126:663–676. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Yu J, Vodyanik MA, SmugaOtto K,
AntosiewiczBourget J, Frane JL, Tian S, Nie J, Jonsdottir GA,
Ruotti V, Stewart R, et al: Induced pluripotent stem cell lines
derived from human somatic cells. Science. 318:1917–1920. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Li N, Deng W, Ma J, Wei B, Guo K, Shen W,
Zhang Y and Luo S: Prognostic evaluation of Nanog, Oct4, Sox2,
PCNA, Ki67 and E-cadherin expression in gastric cancer. Med Oncol.
32:4332015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Al-Marzoqee FY, Kholder G, AlAwadhi H,
John R, Beg A, Vincze A, Branicki F and Karam SM: Upregulation and
inhibition of the nuclear translocation of Oct4 during multistep
gastric carcinogenesis. Int J Oncol. 41:1733–1743. 2012.PubMed/NCBI
|
|
11
|
Tian T, Zhang Y, Wang S, Zhou J and Xu S:
Sox2 enhances the tumorigenicity and chemoresistance of cancer
stem-like cells derived from gastric cancer. J Biomed Res.
26:336–345. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Otsubo T, Akiyama Y, Yanagihara K and
Yuasa Y: SOX2 is frequently downregulated in gasyric cancers and
and inhibits cell growth through cell-cycle arrest and apoptosis.
Br J Cancer. 98:824–831. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Evans PM and Liu C: Roles of Krüpel-like
factor 4 in normal homeostasis, cancer and stem cells. Acta Biochim
Biophys Sin (Shanghai). 40:554–564. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Wei D, Gong W, Kanai M, Schlunk C, Wang L,
Yao JC, Wu TT, Huang S and Xie K: Drastic down-regulation of
Krüppel-like factor 4 Expression is critical in human gastric
cancer development and progression. Cancer Res. 65:2746–2754. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Sobin LH, Gospodarowicz MK and Wittekind
C: International Union Against Cancer (UICC) TNM Classification of
Malignant Tumors. 7th. Wiley-Blackwell; New York: 2010
|
|
16
|
McGhan LJ, Pockaj BA, Gray RJ, Bagaria SP
and Wasif N: Validation of the updated 7th edition AJCC TNM staging
criteria for gastric adenocarcinoma. J Gastrointest Surg. 16:53–61.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Fukuoka J, Fujii T, Shih JH, Dracheva T,
Meerzaman D, Player A, Hong K, Settnek S, Gupta A, Buetow K, et al:
Chromatin remodeling factors and BRM/BRG1 expression as prognostic
indicators in non-small cell lung cancer. Clin Cancer Res.
10:4314–4324. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Sekine S, Shimada Y, Nagata T, Moriyama M,
Omura T, Watanabe T, Hori R, Yoshioka I, Okumura T, Sawada S, et
al: Prognostic significance of aquaporins in human biliary tract
carcinoma. Oncol Rep. 27:1741–1747. 2012.PubMed/NCBI
|
|
19
|
Garrett-Sinha LA, Eberspaecher H, Seldin
MF and de Crombrugghe B: A gene for a novel zinc-finger protein
expressed in differentiated epithelial cells and transiently in
certain mesenchymal cells. J Biol Chem. 271:31384–31390. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Shields JM, Christy RJ and Yang VW:
Identification and characterization of a gene encoding a
gut-enriched Krüppel-like factor expressed during growth arrest. J
Biol Chem. 271:20009–20017. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Z Jun Z Neng, Leiyuan S, Lang Z, Miao H,
Zhen H and Ziwei W: Krüppel-like factor 4 negatively regulates
β-catenin expression and inhibits the proliferation, invasion and
metastasis of gastric cancer. Int J Oncol. 40:2038–2048.
2012.PubMed/NCBI
|
|
22
|
Liu Z, Yang H, Luo W, Jiang Q, Mai C, Chen
Y, Zhen Y, Yu X, Long X and Fang W: Loss of cytoplasmic KLF4
expression is correlated with the progression and poor prognosis of
nasopharyngeal carcinoma. Histopathology. 63:362–370. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Chen CJ, Hsu LS, Lin SH, Chen MK, Wang HK,
Hsu JD, Lee H and Yeh KT: Loss of nuclear expression of
Krüppel-like factor 4 is associated with poor prognosis in patients
with oral cancer. Hum Pathol. 43:1119–1125. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Li J, Zheng H, Yu F, Yu T, Liu C, Huang S,
Wang TC and Ai W: Deficiency of the Krüppel-like factor KLF4
correlates with increased cell proliferation and enhanced skin
tumorigenesis. Carcinogenesis. 33:1239–1246. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Liu Y, Zhang C, Fan J, Xiao L, Yin B, Zhou
K and Xia S: Comprehensive analysis of clinical significance of
stem-cell related factors in renal cell cancer. World J Surg Oncol.
9:1212011. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Hu W, Hofstetter WL, Li H, Zou Y, He Y,
Pataer A, Wang L, Xie K, Swisher SG and Fang B: Putative
tumor-suppressive function of Krüppel-like factor 4 in primary lung
carcinoma. Clin Cancer Res. 15:5688–5695. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Yang WT and Zheng PS: Krüppel-like factor
4 functions as a tumor suppressor in cervical carcinoma. Cancer.
118:3691–3702. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Nagata T, Shimada Y, Sekine S, Hori R,
Matsui K, Okumura T, Sawada S, Fukuoka J and Tsukada K: Prognostic
significance of NANOG and KLF4 for breast cancer. Breast Cancer.
21:96–101. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Tiwari N, MeyerSchaller N, Arnold P,
Antoniadis H, Pachkov M, van Nimwegen E and Christofiri G: Klf4 is
a transcriptional regulator of genes critical for EMT, including
Jnk1 (Mapk8). PLoS One. 8:e573292013. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Zhou Y, Hofstetter WL, He Y, Hu W, Pataer
A, Wang L, Wang J, Zhou Y, Yu L, Fang B and Swisher SG: KLF4
inhibition of lung cancer cell invasion by suppression of SPARC
expression. Cancer Biol Ther. 9:507–513. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Leng Z, Tao K, Xia Q, Tan J, Yue Z, Chen
J, Xi H, Li J and Zheng H: Krüppel-like factor 4 acts as an
oncogene in colon cancer stem cell-enriched spheroid cells. PLoS
One. 8:e560822013. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Yang Y, Goldstein BG, Chao HH and Katz JP:
KLF4 and KLF5 regulate proliferation, apoptosis and invasion in
esophageal cancer cells. Cancer Biol Ther. 4:1216–1221. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Ohnishi S, Ohnami S, Laub F, Aoki K,
Suzuki K, Kanai Y, Haga K, Asaka M, Ramirez F and Yoshida T:
Downregulation and growth inhibitory effect of epithelial-type
Krüppel-like transcription factor KLF4, but not KLF5, in bladder
cancer. Biochem Biophys Res Commun. 308:251–256. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Tang W, Zhu Y, Gao J, Fu J, Liu C, Liu Y,
Song C, Zhu S, Leng Y, Wang G, et al: MicroRNA-29 promotes
colorectal cancer metastasis by regulating matrix metalloproteinase
2 and E-cadherin via KLF4. Br J Cancer. 110:450–458. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Gastric Cancer treatment guidelines 2014,
version 4. Kodera Y and Sano T: Japanese Gastric Cancer
Association; 2014
|
|
36
|
Chen ZY, Shie J and Tsen C: Up-regulation
of gut-enriched krüppel-like factor by interferon-gamma in human
colon carcinoma cells. FEBS Lett. 477:67–72. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Yasunaga J, Taniguchi Y, Nosaka K, Yoshida
M, Satou Y, Sakai T, Mitsuya H and Matsuoka M: Identification of
aberrantly methylated genes in association with adult T-cell
leukemia. Cancer Res. 64:6002–6009. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Shie JL, Chen ZY, Fu M, Pestell RG and
Tseng CC: Gut-enriched Krüppel-like factor represses cyclin D1
promoter activity through Sp1 motif. Nucleic Acids Res.
28:2969–2976. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Tiwari N, MeyerSchaller N, Arnold P,
Antoniadis H, Pachkov M, van Nimwegen E and Chritofori G: Klf4 is a
transcriptional regulator of genes critical for EMT, including Jnk1
(Mapk8). PLoS One. 8:e573292013. View Article : Google Scholar : PubMed/NCBI
|