Introduction
Papillary thyroid carcinoma (PTC) is derived from
the thyroid follicular epithelium. PTC is the most common type of
endocrine cancer, and its rate of incidence has increased rapidly
over the past several decades (1,2).
Currently, the vast majority of newly detected PTCs are small,
localized, asymptomatic tumors that are identified incidentally
(3). Therefore, the tools for
diagnosing, treating and monitoring PTC are also adapting. The
current challenge regarding PTC is to revise follow-up paradigms to
ensure the most appropriate, cost-effective monitoring index of PTC
that guarantees the best management and the quality of life for a
disease that, despite an intrinsic low mortality, requires
life-long follow-up care.
Thyroid ultrasound (US) is a widespread technique
used as a first-line preoperative diagnostic procedure for
detecting and characterizing nodular thyroid disease. US features
that are associated with malignancy include hypoechogenicity,
microcalcifications, an absence of a peripheral halo, irregular
borders, solid aspects, intranodular blood flow and shape (taller
than wide). Taken individually, each of these patterns is poorly
predictive. However, when multiple patterns suggestive of
malignancy are simultaneously present in a nodule, the specificity
of US increases, but the sensitivity becomes unacceptably low
(4,5).
Fine needle aspiration cytology (FNAC) is currently
the best method for the differential diagnosis of thyroid nodules
(6,7).
However, FNAC has limitations associated with inadequate sampling
and difficulty in discriminating follicular lesions (8). The prevalence of non-diagnostic and
indeterminate FNAC remains high, at ~30%. The majority of these
patients undergo surgery, but <20% of surgically removed nodules
are malignant (6,9,10).
Various molecular markers, including BRAF, RAS,
RET/PTC, paired box 8/peroxisome proliferator-activated receptor γ
(PPARγ) and galecton-3, have been considered for indeterminate
cytology according to the American Thyroid Association guidelines
(5). Although these molecular markers
may aid clinicians in discriminating between PTC and BTN, the
Association of Clinical Endocrinologists and the European Thyroid
Association do not currently recommend these markers in routine
practice. Instead, assessments using molecular markers are reserved
for select cases due to their inconsistent results and relatively
high costs (11).
For the majority of patients with PTC, the prognosis
is excellent, with an overall 5-year survival rate of >95%.
However, up to 30% of patients with PTC suffer locoregional or
distant metastatic recurrence 10 years or even 20 years following
initial treatment (12,13). Therefore, a key issue in the
management of patients with PTC is minimizing the morbidity and
mortality associated with recurrent disease. Currently, there are a
limited number of biomarkers are available for PTC and consist
primarily of neck US or basal and recombinant human thyrotropin (rh
TSH)-stimulated serum thyroglobulin (TG) measurements that may be
used to identify individuals at risk of recurrence. These tests
have a higher negative predictive value but a low specificity and
positive predictive value (14–17).
Therefore, there is a risk of subjecting numerous patients, who are
likely free of disease, to extensive testing or unnecessary
treatment when there is a general lack of accuracy and consensus in
the diagnosis (18,19). Specific and sensitive non-invasive
biomarkers for the detection of PTC are required to reduce the
worldwide morbidity caused by cancer and as the treatment of a
disease is more effective if the underlying pathology is diagnosed
early.
MicroRNAs (miRNAs/miRs) are endogenous noncoding RNA
molecules that are 18–25 nucleotides in length. miRNAs have been
shown to perform a key role in the regulation of gene expression.
There is also evidence that miRNAs are involved in central
biological processes, including development, organogenesis, tissue
differentiation, cell cycles and metabolism (20,21).
Alterations in the expression of miRNA contribute to the
pathogenesis of the majority of human malignancies. Recently,
miRNAs have also been detected in serum, plasma, urine, saliva, and
other bodily fluids (22–25). Biochemical analyses have indicated
that miRNAs are resistant to RNase activity and extreme pH and
temperature. The expression patterns of circulating miRNAs,
particularly serum miRNAs, are clearly correlated with various
diseases, including cancer, and may have potential for use as novel
minimally invasive biomarkers for diagnosing and monitoring human
cancer.
miRNA expression is altered in thyroid tumors,
suggesting a role for miRNA in thyroid carcinogenesis (26–28).
Previous studies on miRNA deregulation have demonstrated increased
aberrant miRNA expression (particularly miR-222, miR-221 and
miR-146b) in PTCs when compared with normal thyroid tissues and BTN
(29–32). These data indicate that miRNAs may be
useful diagnostic and prognostic markers for PTC and may even
function as therapeutic targets. However, the majority of these
reports regarding miRNA expression are based on findings from tumor
tissue specimens. Although tissue miRNA profiles may be useful for
distinguishing benign from malignant lesions, obtaining the tumor
tissue is not a suitable presurgical diagnosis. To date, a limited
number of reports have addressed the possibility of evaluating
circulating miR-222, miR-221 and miR-146b levels in patients with
PTC, and their conclusions remain controversial (29,33–35).
These considerations provided the basis for the
present study, which developed a novel screening approach that
specifically detects the diagnosis and recurrence of PTC. The
present study validated the expression of serum miR-222, miR-221
and miR-146b, which have previously been reported as miRNAs in
tumor tissues and cell lines that are able to differentiate PTCs
from BTN and controls. The present study focused on the dynamic
monitoring of miRNA profiles prior to and subsequent to surgery to
elucidate whether the abnormal expression of specific miRNAs is
associated with the diagnosis, prognosis and recurrence of PTC and
whether there are associated clinicopathological factors in
patients with PTC.
Materials and methods
Patients
A total of 106 PTC patient, of which 85 were newly
clinically diagnosed with PTC and 21 cases of PTC with newly
suspicious neck masses or lymph nodes subsequent to an initial
curative treatment. In addition 35 patients with BTN who had single
or multiple nodules and were undergoing a thyroidectomy. These
patients were enrolled from the Department of Thyroid Surgery of
the Second Affiliated Hospital of Harbin University (Heilongjiang,
China) between September 2013 and December 2015. In total, 40
control subjects were enrolled from the Physical Examination Center
of the Second Affiliated Hospital of Harbin University
(Heilongjiang, China) between September 2013 and December 2015. The
surgical procedure for patients with PTC was performed according to
the revised American Thyroid Association management guidelines for
pathway with thyroid nodules and differentiated thyroid cancer
(5). A more detailed explanation of
the procedures is provided below. For patients with thyroid cancer
tumors >1 cm, the initial surgical procedure must be a
near-total or total thyroidectomy. If surgery is selected for
patients with PTC with a tumor <1 cm without extrathyroidal
extension, the unifocal surgical procedure must be a
hemithyroidectomy (5). For patients
with BTN, the surgical procedure must be a hemithyroidectomy. The
40 control subjects were age- and gender-matched volunteers without
a current or previous history of any other types of cancer and were
confirmed to not have thyroid disease based on a neck US and
thyroid hormone measurements. The characteristics of the patients
with PTC in this study are presented in Table I. The clinical stage was classified
according to the American Joint Committee on Cancer (2010, 7th
edition) tumor node metastasis (TNM) classification system
(36). Patients were stratified into
low- and high-risk PTCs according to the age, metastasis, extension
and size risk-group classification (37). All pathological results for these
patients were verified by the Department of Pathology at the Second
Affiliated Hospital of Harbin Medical University. Tumor recurrence
was defined as new evidence of a pathologically proven recurrence
in a patient who initially met the criteria for remission. The
criteria for remission was no clinical or imaging evidence of
tumors.
 | Table I.Clinicopathological features of
patients and their associations with circulating levels of
miRNA. |
Table I.
Clinicopathological features of
patients and their associations with circulating levels of
miRNA.
|
Characteristics | No. of patients, n
(%) | miR-222 Median (IQ
range) | P-value | miR-221 Median (IQ
range) | P-value | miR-146b Median (IQ
range) | P-value |
|---|
| PTC (newly
diagnosed) | 85 | 1.95
(1.42–3.45) |
| 2.66
(1.63–4.98) |
| 2.46
(1.65–3.99) |
|
| Age, years |
|
| 0.124 |
| 0.132 |
| 0.143 |
|
<45 | 49 (57.6%) | 1.83
(1.36–2.65) |
| 2.38
(1.55–3.69) |
| 2.20
(1.45–3.63) |
|
|
≥45 | 36 (42.4%) | 2.88
(1.52–3.91) |
| 3.26
(1.79–5.56) |
| 2.64
(1.91–4.38) |
|
| Sex |
|
| 0.310 |
| 0.110 |
| 0.258 |
|
Male | 29 (34.1%) | 1.93
(1.26–3.12) |
| 3.23
(2.24–5.28) |
| 2.06
(1.32–3.52) |
|
|
Female | 56 (65.9%) | 1.97
(1.48–3.87) |
| 2.38
(1.57–4.03) |
| 2.47
(1.71–3.99) |
|
| Tumor size, cm |
|
| 0.024 |
| 0.081 |
| 0.378 |
|
≤2.0 | 64 (75.3%) | 1.87
(1.42–2.71) |
| 2.42
(1.57–3.88) |
| 2.44
(1.55–3.76) |
|
|
>2.0 | 21 (24.7%) | 3.71
(1.40–9.16) |
| 3.63
(2.25–5.49) |
| 2.51
(1.59–5.46) |
|
| Tumor location |
|
| 0.041 |
| 0.032 |
| 0.008 |
|
Unilateral | 46 (54.1%) | 1.83
(1.30–2.80) |
| 2.27
(1.56–3.63) |
| 2.01
(1.31–3.46) |
|
|
Bilateral | 39 (45.9%) | 2.60
(1.47–5,58) |
| 3.61
(1.13–5.86) |
| 2.62
(2.10–4.44) |
|
| Multifocal
tumor |
|
| 0.579 |
| 0.031 |
| 0.682 |
| No | 65 (76.5%) | 1.95
(1.32–3.62) |
| 2.38
(1.54–3.85) |
| 2.45
(1.58–3.88) |
|
|
Yes | 20 (23.5%) | 2.34
(1.49–3.30) |
| 3.67
(2.34–5.77) |
| 2.49
(1.55–64.30) |
|
| Extrathyroidal
invasion |
|
| <0.001 |
| 0.010 |
| 0.012 |
| No | 68 (80.0%) | 1.83
(1.35–2.67) |
| 2.42
(1.54–3.88) |
| 2.33
(1.35–3.65) |
|
|
Yes | 17 (20.0%) | 4.96
(2.94–9.51) |
| 3.71
(2.66–6.01) |
| 3.78
(2.18–6.79) |
|
| Metastatic lymph
node |
|
| 0.008 |
| 0.001 |
| 0.007 |
| No | 26 (30.6%) | 1.61
(1.20–2.02) |
| 1.73
(1.35–3.23) |
| 1.89
(1.26–2.81) |
|
|
Yes | 59 (69.4%) | 2.07
(1.49–3.73) |
| 3.01
(2.16–5.39) |
| 2.55
(1.85–4.20) |
|
| TNM stage
(AJCC) |
|
| <0.001 |
| <0.001 |
| 0.001 |
|
I/II | 56 (65.9%) | 1.80
(1.26–2.07) |
| 2.27
(1.50–3.18) |
| 2.04
(1.35–3.48) |
|
|
III/IV | 29 (34.1%) | 3.34
(1.93–5.84) |
| 4.96
(2.52–6.09) |
| 3.63
(2.37–5.26) |
|
| AMES |
|
| <0.001 |
| 0.002 |
| 0.001 |
| Low
risk | 72 (84.7%) | 1.83
(1.28–2.67) |
| 2.42
(1.55–3.76) |
| 2.31
(1.37–3.65) |
|
| High
risk | 13 (15.3%) | 8.11
(4.19–11.90) |
| 4.96
(3.56–6.66) |
| 3.89
(2.50–7.62) |
|
| Benign thyroid
nodule |
|
|
|
|
|
|
|
| Age, years |
|
| 0.620 |
| 0.124 |
| 0.506 |
|
<45 | 13 (37.1%) | 1.57
(0.62–3.12) |
| 1.60
(0.48–3.00) |
| 1.03
(0.63–1.87) |
|
|
≥45 | 22 (62.9%) | 1.64
(0.69–3.82) |
| 2.35
(1.57–4.25) |
| 1.62
(0.66–3.18) |
|
| Sex |
|
| 0.956 |
| 0.913 |
| 0.742 |
|
Male | 10 (28.6%) | 1.56
(0.72–3.87) |
| 2.28
(0.72–3.51) |
| 1.42
(0.53–2.23) |
|
|
Female | 25 (71.4%) | 1.60
(0.62–3.04) |
| 2.13
(1.45–3.55) |
| 1.57
(0.67–3.56) |
|
| Features of
nodules |
|
| 0.537 |
| 0.405 |
| 0.309 |
|
Solitary goiter | 10 (28.6%) | 1.56
(0.53–2.68) |
| 2.64
(1.13–4.99) |
| 1.59
(0.68–4.03) |
|
| Multinodular
goiters | 25 (71.4%) | 1.64
(0.79–3.82) |
| 1.91
(1.39–3.23) |
| 1.07
(0.58–2.01) |
|
| Control
subjects | 40 | 1.09
(0.99–1.26) |
| 1.03
(0.66–1.96) |
| 0.99
(0.63–1.40) |
|
| Age, years |
|
| 0.244 |
| 0.797 |
| 0.636 |
|
<45 | 21 (52.5%) | 1.09
(0.90–1.24) |
| 1.03
(0.88–1.43) |
| 0.92
(0.62–1.72) |
|
|
≥45 | 19 (47.5%) | 1.13
(0.99–1.37) |
| 1.15
(0.88–1.53) |
| 1.15
(0.88–1.53) |
|
| Sex |
|
| 0.467 |
| 0.296 |
| 0.575 |
|
Male | 11 (27.50%) | 1.12
(0.28–2.31) |
| 1.06
(0.30–1.85) |
| 0.93
(0.60–1.80) |
|
|
Female | 29 (72.5%) | 1.27
(0.91–2.74) |
| 1.29
(0.78–2.04) |
| 1.33
(0.61–1.92) |
|
The present study was approved by the Institutional
Review Board of Harbin Medical University. Written informed consent
was obtained from all participants involved in the present
study.
Serum samples and RNA extraction
Fasting peripheral blood samples were collected in
vacuum-sealed blood collection tubes from all control subjects and
patients with PTC and BTN on the day of surgery. Samples from prior
to and subsequent to surgery were separated into serum and cellular
components within 1 h of collection by centrifugation at 1,900 × g
for 15 min at 4°C. The supernatant was carefully transferred into
an RNase-free tube and centrifuged at 12,000 × g for 10 min at 4°C
to remove additional cellular debris and to minimize the
contamination of cell-free nucleic acid by DNA and RNA derived from
damaged blood cells. The serum samples were stored at −80°C until
RNA extraction.
Total RNA was isolated from 200 µl of serum
according to the manufacturer's protocol using a miRNeasy
serum/plasma kit (Qiagen GmbH, Hilden, Germany). Briefly, 1,000 µl
of QIAzol lysis reagent and 3.5 µl of the miRNeasy serum/plasma
spike-in control (C. elegans miR-39 miRNA mimic,
1.6×108 copies/µl working solution) were added to 200 µl
of serum and incubated at room temperature for 5 min. The C.
elegans miR-39 miRNA mimic was used as an external reference to
validate whether miR-16 may be utilized as an endogenous reference.
An equal volume of chloroform was added to the starting sample, and
the samples were centrifuged for 15 min at 12,000 x g at 4°C until
there was complete phase separation.
The upper aqueous phase was quickly transferred to a
new collection tube, and 1.5 volumes of 100% ethanol were added to
the sample, which was mixed thoroughly. The sample was transferred
into an RNeasy MinElute spin column (Qiagen GmbH, Hilden, Germany)
in a 2 ml collection tube and centrifuged at 8,000 x g for 15 sec
at room temperature and the flow-through was discarded. The RNeasy
MinElute spin columns were washed with 700 µl of buffer RWT, 500 µl
of buffer RPE and 80% ethanol. The precipitated RNA was resuspended
in 14 µl of RNase-free water. The final elution volume was 12 µl.
The concentrations of all RNA samples were quantified using a
NanoDrop 1000 spectrophotometer (NanoDrop Technologies; Thermo
Fisher Scientific, Inc., Wilmington, DE, USA). The concentrations
of RNA extracted from plasma ranged between 15.9 and 24.7
ng/ml.
Selection and detection of miRNAs
The miRNA candidates to be tested were selected
based on the following process. Firstly, miRNAs that were enriched
in normal thyroid tissues and significantly unregulated in PTC
compared with normal thyroid tissues and BTN were selected
(29–31,38).
Published reports describing the analysis of circulating miRNAs in
plasma or serum were then examined (29,33). This
step was critical since miRNA expression levels in various tissues
do not generally correlate with their concentrations in plasma or
serum in patients with PTC (29,33,34), and
the serum or plasma levels of tissue-enriched miRNAs can be
significantly lower compared with levels of ubiquitous miRNAs.
Finally, miRNAs that were significantly associated with a poor
prognosis of PTC were selected (29,30,33,34,38,39).
Based on this selection procedure, 3 miRNAs (miR-222, miR-221 and
miR-146b) were selected as candidate targets for the serum miRNA
assay.
Reverse transcription-quantitative
polymerase chain reaction (RT-qPCR)
First-strand cDNA synthesis of miRNA was performed
using a miRcute miRNA first-strand cDNA synthesis kit (Tiangen
Biotech Co. Ltd., Beijing, China) according to the manufacturer's
protocol. Reverse transcription was conducted on a GeneAmp PCR
System 9700 (Applied Biosystems; Thermo Fisher Scientific, Inc.,
Waltham, MA, USA). Briefly, 5 µl of total RNA was extracted from
plasma, polyadenylated by poly (A)polymerase and reverse
transcribed to cDNA according to the manufacturer's protocol. The
cycle parameter for the reverse transcription reaction was 37°C for
60 min. cDNA was stored at 20°C prior to use.
RT-qPCR was performed in duplicate using the SYBR
Green PCR master mix (miRcute miRNA qPCR detection kit; Tiangen
Biotech Co., Ltd.) with the Stratagene Mx3000PTM real-time PCR
system (Applied Biosystems; Thermo Fisher Scientific, Inc.).
miRNA-specific primer sequences were designed based on the miRBase
database by Primer Premier 5.0 and are presented in Table II. Each reaction was performed in a
final volume of 20 µl containing 2 µl of the cDNA, 0.4 µl of each
primer and 10 µl of SYBR Green PCR Master mix (Tiangen Biotech Co.,
Ltd.). The amplification cycle was denaturation at 94°C for 2 min
followed by 45 cycles at 94°C for 20 sec and 60°C for 34 sec. All
real-time PCR reactions were performed in triplicate.
| Table II.miRNA-specific forward primer
sequences. |
Table II.
miRNA-specific forward primer
sequences.
| Gene name | Primer sequence
(5′-3′) |
|---|
| miR-222 |
GGGCTCAGTAGCCAGTGTAGATCC |
| miR-221 |
GGCGACCTGGCATACAATGTAGAT |
| miR-146b |
GGCTGAGAACTGAATTCCATAGGC |
| miR-16 |
GCTAGCAGCACGTAAATATTGGCG |
miR-16 has been used as an endogenous reference for
serum and plasma miRNA analysis in several studies (40–44). It is
highly expressed in plasma and serum and is relatively invariant
across large numbers of samples, as reported by Kroh et al
(40). Therefore, the present study
utilized miR-16 as the endogenous serum control. ΔCq was calculated
by subtracting the Cq value of miR-16 from the Cq value of the
miRNA of interest. ΔΔCq was then calculated by subtracting ΔCq of
the control group from ΔCq of the disease group. The fold-change in
the expression of each miRNA was determined by comparing the mean
2−ΔΔCq values of the PTC and BTN groups to the mean
2−ΔΔCq value of the control group (45).
Statistical analysis
Statistical analysis was performed using SPSS
version 17.0 (SPSS, Inc., Chicago, IL, USA). The Mann-Whitney U
test was used to determine the significance of the different levels
of miRNA expression. Fisher's exact test was used to measure the
characteristics in the PTC with recurrence (PTC-RC) and PTC without
recurrence (PTC-NR) groups. Receiver operating characteristic (ROC)
curves were used to analyze the diagnostic utility of
differentially expressed miRNAs. The optimal cutoff point was
selected as the value with the maximal sum of sensitivity and
specificity. The levels of miRNA in each group were defined by the
median and interquartile range (IQR). All P-values were two-sided.
P<0.05 was considered to indicate a statistically significant
difference.
Results
Analysis of circulating miR-16 in
serum
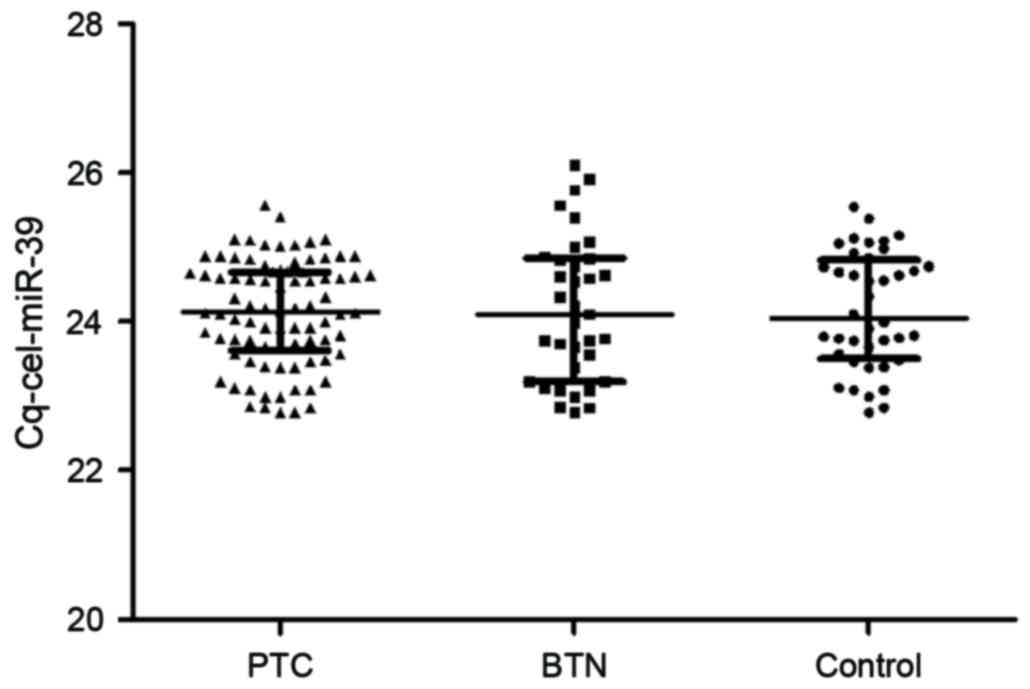
Initially, the presence of circulating miR-16 in
serum was analyzed. Cel-miR-39 expression levels in serum from
patients with PTC were similar to those observed in the BTN and
control groups. There was no significant difference among these 3
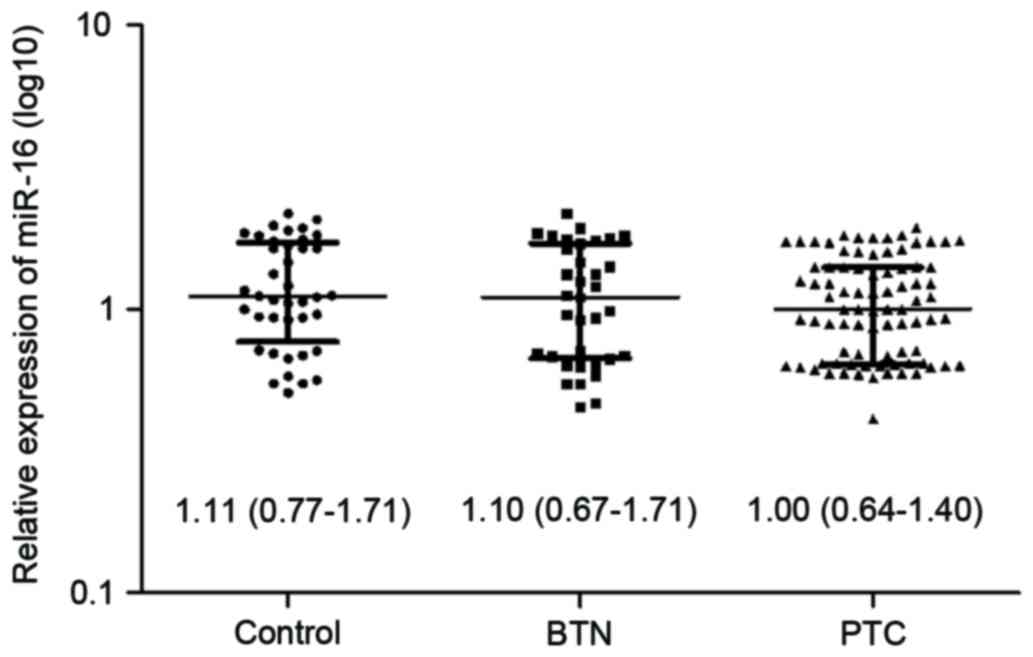
groups (P=0.808, P=0.828 and P=0.959, respectively; Fig. 1). To confirm that the present results
were not due to technical biases, miR-16 was normalized with spiked
cel-miR-39 and no significant differences were revealed in miR-16
values among PTC patients, BTN patients and controls (P=0.135,
P=0.432 and P=0.630; respectively; Fig.
2). These results indicate that miR-16 is an appropriate
endogenous normalizer.
Serum miRNA expression patterns in
patients with PTC or BTN and control subjects
The present study used RT-qPCR to measure the
expression levels of serum miR-222, miR-221 and miR-146b from all
enrolled subjects. No significant differences were identified in
terms of age or sex among the 3 groups (P=0.288 and P=0.940,
respectively). The serum levels of miR-222, miR-221 and miR-146b
were significantly higher in patients with newly diagnosed PTC
compared with those with BTN or in the control subjects (P<0.001
and P<0.001, respectively; Fig.
3). The fold-changes were 1.79, 2.58 and 2.48, respectively,
compared with the controls. In addition, miR-221 was overexpressed
in patients with BTN compared with control subjects (P<0.001),
with a fold-change of 1.98. However, no significant difference was
identified in the serum levels of miR-222 and miR-146b between
patients with BTN and control patients (P=0.983 and P=0.232,
respectively).
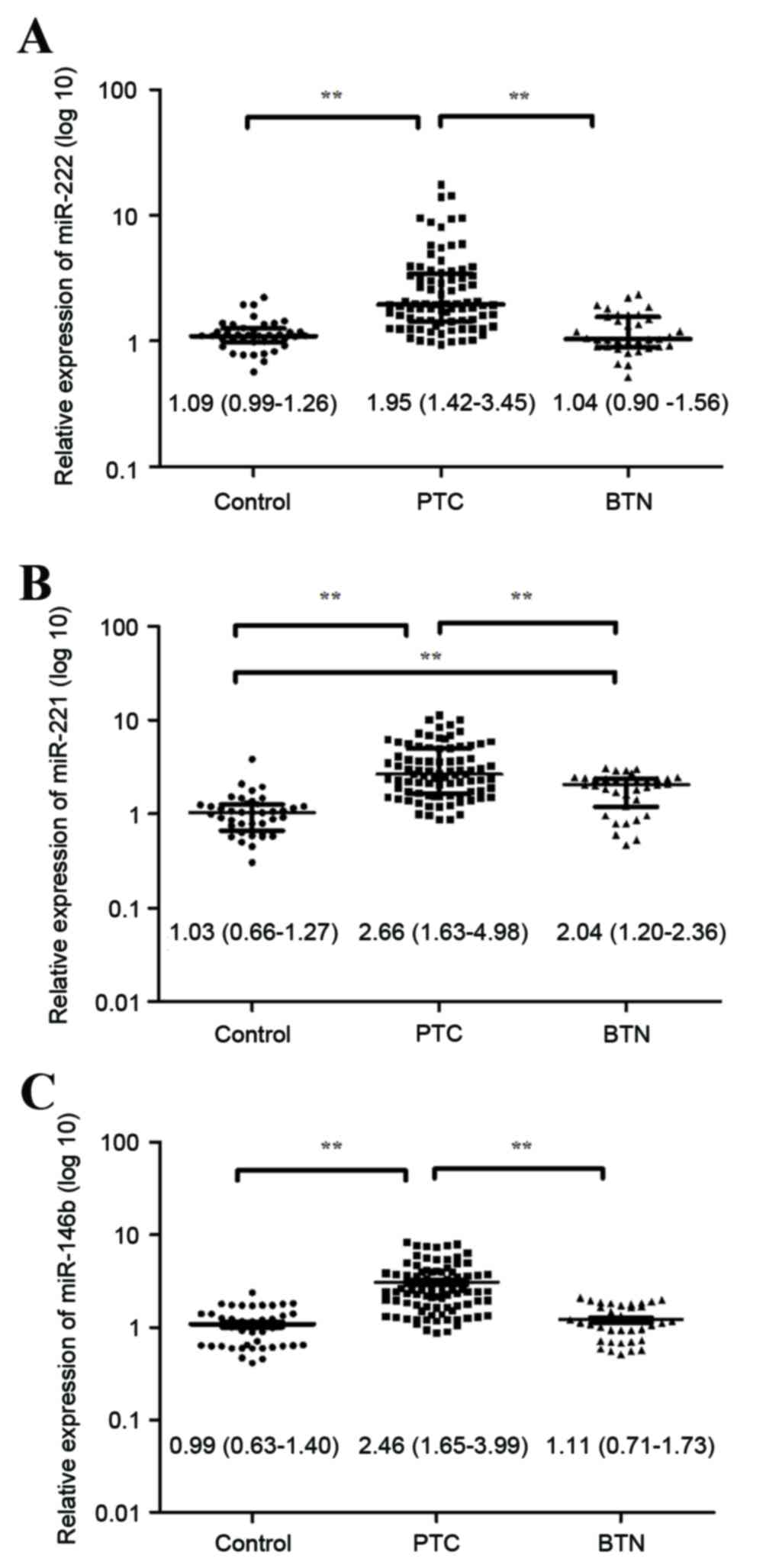 | Figure 3.Diagram of Mann-Whitney U test
results, demonstrating that the relative expression levels of (A)
miR-222, (B) miR-221 and (C) miR-146b in the PTC group (n=85;
median=1.95, 2.66 and 2.46; interquartile range=1.42–3.45,
1.63–4.98 and 1.65–3.99, respectively) were significantly increased
compared with in the control (n=40; median=1.09, 1.03 and 0.99;
interquartile range=0.99–1.26, 0.66–1.27 and 0.63–1.40,
respectively) and BTN (n=35; median=1.04, 2.04 and 1.11;
interquartile range=0.90–1.56, 1.20–2.36 and 0.71–1.73,
respectively) groups. For miR-222 and miR-146b, there was no
significant difference in expression between the BTN and control
groups (P=0.983 and P=0.232). For miR-221, there was a significant
difference in expression levels between the BTN and control groups
(**P<0.01). Relative miRNA expression is presented as the log 10
of target miRNA expression values. miR; microRNA; PTC, papillary
thyroid carcinoma; BTN, benign thyroid nodules. |
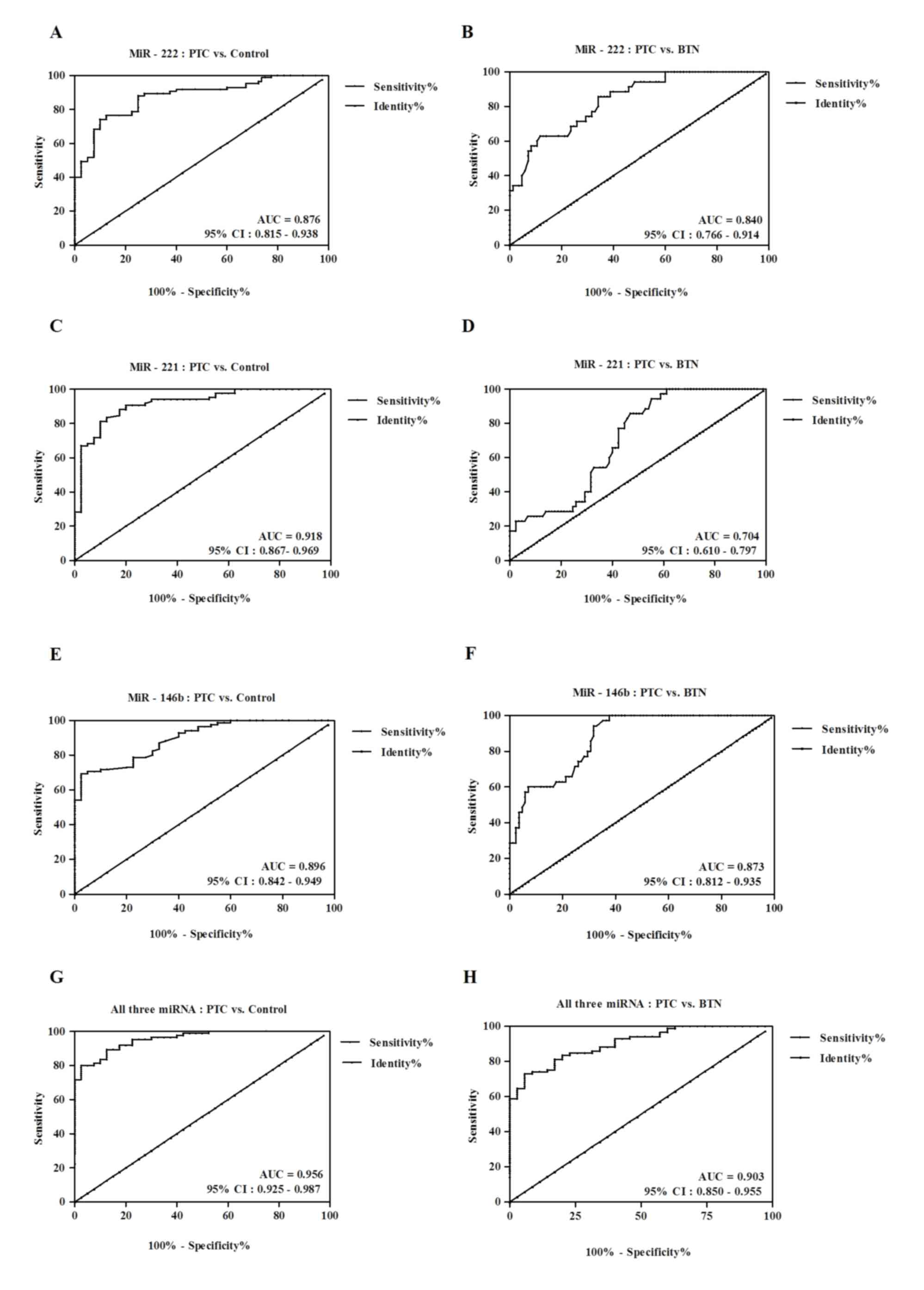
An ROC curve analysis was used to evaluate the
diagnostic value of serum miR-222, miR-221 and miR-146b levels for
PTC. A comparison of the PTC and control groups indicated that
using all 3 miRNAs produces an area under the curve (AUC) of 0.956
[95% confidence interval (CI), 0.925–0.987] with 72.94% sensitivity
and 94.29% specificity at the cutoff value of 0.73. Individually,
miR-222 had an AUC of 0.876 (95% CI, 0.815–0.938), miR-221 had an
AUC of 0.918 (95% CI, 0.867–0.969) and miR-146b had an AUC of 0.896
(95% CI, 0.842–0.949). At cutoff values of 1.46, 1.49 and 1.83 for
miR-222, miR-221 and miR-146b, respectively, the sensitivity and
specificity values were 74.12 and 90%, 83.53 and 87.50%, and 69.41
and 97.50%, respectively.
A comparison of the PTC and BTN groups indicated
that the use of all 3 miRNAs had an AUC of 0.903 (95% CI,
0.850–0.955) with 80% sensitivity and 97.50% specificity at the
cutoff value of 0.70. Individually, miR-222 had an AUC of 0.840
(95% CI, 0.766–0.914), miR-221 had an AUC of 0.704 (95% CI,
0.610–0.797) and miR-146b had an AUC of 0.873 (95% CI,
0.812–0.935). At cutoff values of 1.21, 2.51 and 1.94 for miR-222,
miR221 and miR-146b, respectively, the sensitivity and specificity
values were 62.86 and 88.24%, 85.71 and 52.94% and 94.29 and
68.24%, respectively (Fig. 4).
Correlation of miRNA levels and
clinicopathological characteristics of PTC
As the levels of miR-222, miR-221 and miR-146b were
significantly elevated in newly diagnosed patients with PTC, the
present study also assessed whether any of the clinicopathological
features of PTCs were associated with differential expression
levels of the 3 miRNAs. The results indicated that serum miR-222,
miR-221 and miR-146b levels were significantly higher in patients
with extrathyroid invasion (P<0.001, P=0.010 and P=0.012,
respectively); patients with advanced TNM stage (III/IV;
P<0.001, P<0.001 and P=0.001, respectively); high-risk
patients (P<0.001, P=0.002 and P=0.001, respectively); patients
with metastatic lymph nodes (P=0.008, P=0.001 and P=0.007,
respectively); patients with bilateral tumors (P=0.041, P=0.032 and
P=0.008, respectively). The present results also indicate that
serum miR-222 overexpression is clearly associated with tumor size
(>2 cm, P=0.024) and that serum miR-221 overexpression is
associated with multifocal lesions (P=0.031). The levels of these 3
miRNAs were not correlated with age or gender in any group
(P>0.05, Table I). In addition, no
significant differences were found between patients with solitary
or multifocal BTN (P=0.537, P=0.405 and P=0.309, respectively).
Dynamic monitoring of miRNAs in the
serum of PTC and BTN patients prior to and subsequent to
surgery
To additionally investigate whether levels of
specific circulating miRNAs may be used to monitor postoperative
progression, miR-222, miR-221 and miR-146b were evaluated via
subsequent RT-qPCR during varied postoperative periods in the same
patients (Fig. 5). The time points
included a preoperative sample and samples at 1, 3, 6 and 12 months
postoperatively in the PTC and BTN groups, including 28 patients
with PTC and 16 patients with BTN. miR-222, miR-221 and miR-146b
rapidly decreased 1 month following surgery compared with their
preoperative levels (P<0.001, P<0.001 and P<0.001,
respectively) in the PTC group. The fold-changes of miR-222,
miR-221 and miR-146b were 2.36, 2.69 and 5.39, respectively, in the
PTC group prior to surgery compared with 1 month subsequent to
surgery. In addition, the levels of miR-222, miR-221 and miR-146b
decreased between 1 and 12 months following surgery in the PTC
group. miR-222, miR-221 and miR-146b levels also decreased
gradually and had significant differences at 3 months compared with
6 months following surgery in the PTC group (P<0.001, P=0.003
and P=0.022, respectively). A similar pattern was observed for
miR-146b expression in the BTN group, with rapidly decreased
expression following surgery (P=0.010). The fold-change of miR-146b
was 2.88 in the BTN group prior to surgery compared with 1 month
subsequent to surgery. No change was identified between the miR-222
and miR-221 expression levels prior to surgery and 1, 3, 6 and 12
months following surgery in the BTN group (P>0.05). However,
miR-146b increased at 1 month following surgery compared with 3
months following surgery (P=0.001). There was also no observed
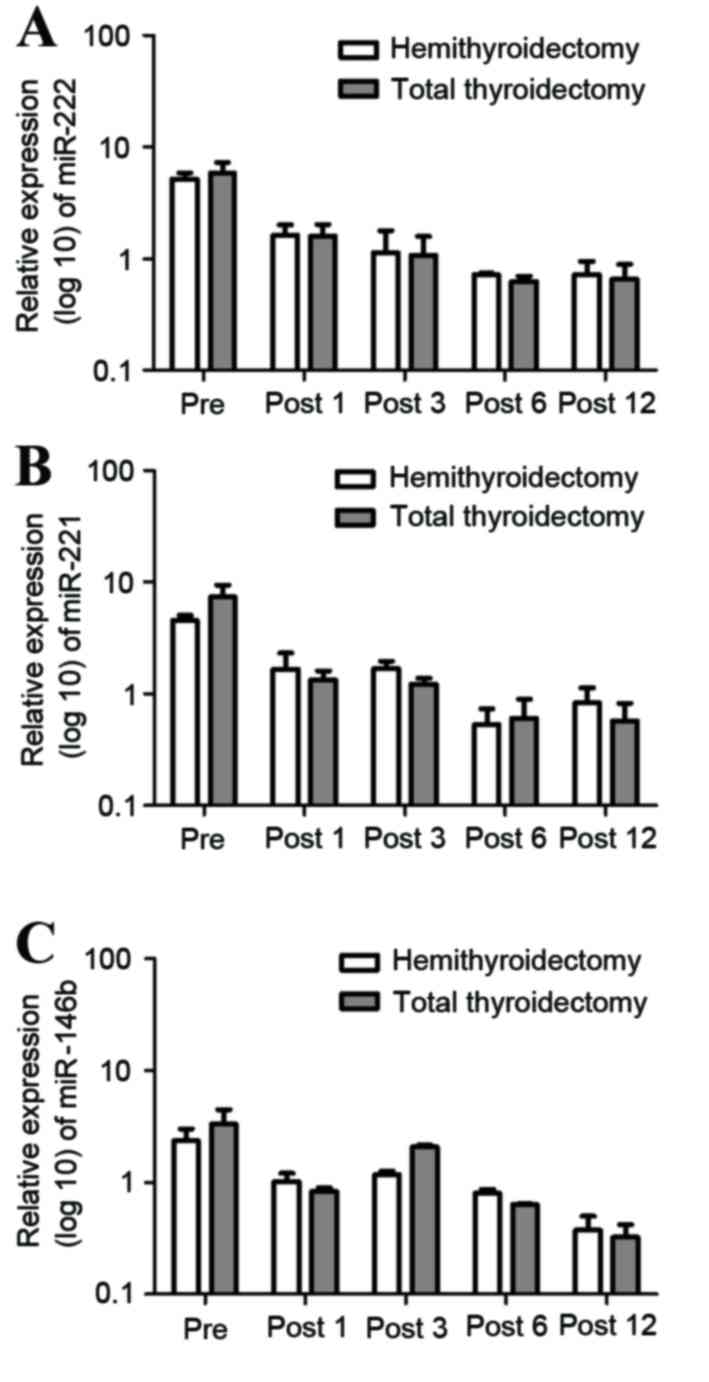
difference in the miR-222, miR-221 and miR-146b expression levels
for patients with PTC undergoing hemithyroidectomy or total
thyroidectomy prior to and subsequent to surgery (P>0.05,
Fig. 6).
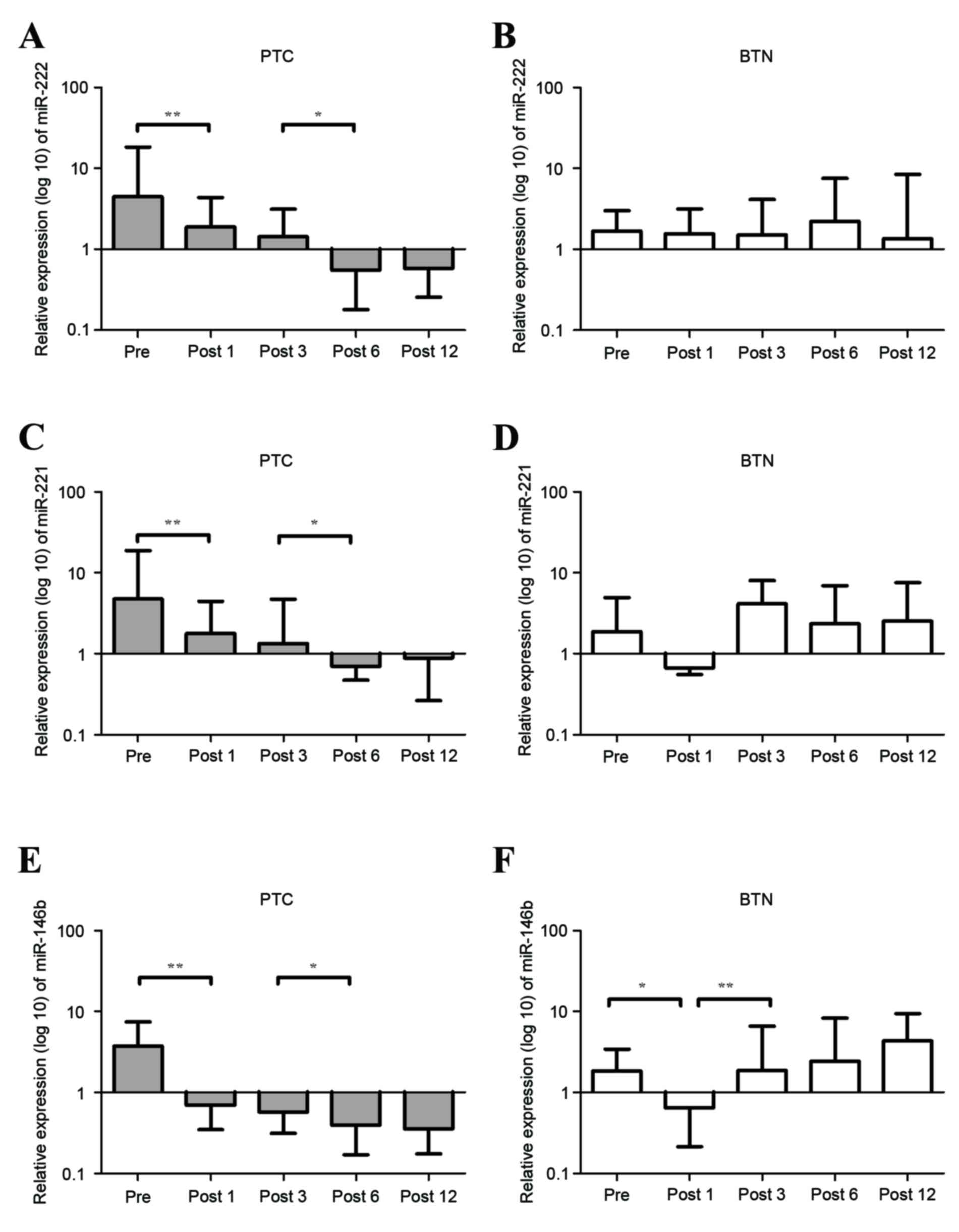 | Figure 5.The expression levels of miR-222,
miR-221 and miR-146b in patients with PTC (n=28) and BTN (n=16)
preoperatively, and at 1, 3, 6 and 12 months postoperatively.
miR-222 expression levels in (A) PTC and in (B) BTN. miR-221
expression levels in (C) PTC and in (D) BTN. miR-146b expression
levels in (E) PTC and in (F) BTN. miR-222, miR-221 and miR-146b
decreased significantly 1 month following surgery compared with the
preoperative level in patients with PTC (**P<0.01). miR-222,
miR-221 and miR-146b gradually decreased between 3 and 6 months
following surgery in the PTC group (*P<0.05). miR-146b decreased
significantly 1 month following surgery compared with the
preoperative level (*P<0.05) and increased significantly at 1
month compared with 3 months following surgery in the BTN group
(**P<0.01). Relative expression is presented as
2−∆∆Cq values. All P-values were determined using the
Mann-Whitney U test. miR, microRNA; PTC, papillary thyroid
carcinoma; BTN, benign thyroid nodules; pre, preoperative; post,
postoperative. |
Differentially expressed miRNAs in the
serum of PTC with and without recurrence following initial
surgery
In the present study, 21 patients with a history of
thyroidectomy due to PTC were recruited as they had newly emerged
lymph nodules or invasions in other locations that were suspicious
of recurrence and were detected by cervical ultrasonography and
medical examinations (Table III). A
total of 12 patients were confirmed to have recurrence, and the
remaining 9 patients were diagnosed with no recurrence by histology
following a second surgical procedure. Of the 12 patients with
recurrence, 7 developed a recurrence in the central neck lymph
nodes, 4 in the lateral neck lymph nodes and 1 in the perithyroid
soft tissues and lateral neck lymph nodes. The median time of
recurrence was 52 months (range, 10–124 months). It was
demonstrated that miR-222, miR-221 and miR-146b levels were
significantly elevated in the PTC-RC group of patients compared
with the PTC-NR group of patients (P<0.001) and controls
(P<0.001). The relative expression levels of miR-222, miR-221
and miR-146b in the PTC-RC group (n=12; median=7.53, 4.63 and 4.60;
range=3.38–9.53, 3.58–7.52 and 3.66–13.14, respectively; Fig. 7) were significantly increased compared
with the control (n=20; median=1.09, 1.14 and 1.23;
range=0.80–1.20, 0.81–1.49 and 0.70–1.71, respectively; Fig. 7) and PTC-NR groups (n=9; median=1.16,
1.53 and 2.25; range=0.96–1.53, 1.40–1.68 and 1.88–3.02,
respectively; Fig. 7). In addition,
miR-221 and miR-146b levels were significantly elevated in the
PTC-NR group of patients compared with controls (P=0.022 and
P=0.002, respectively; Fig. 7).
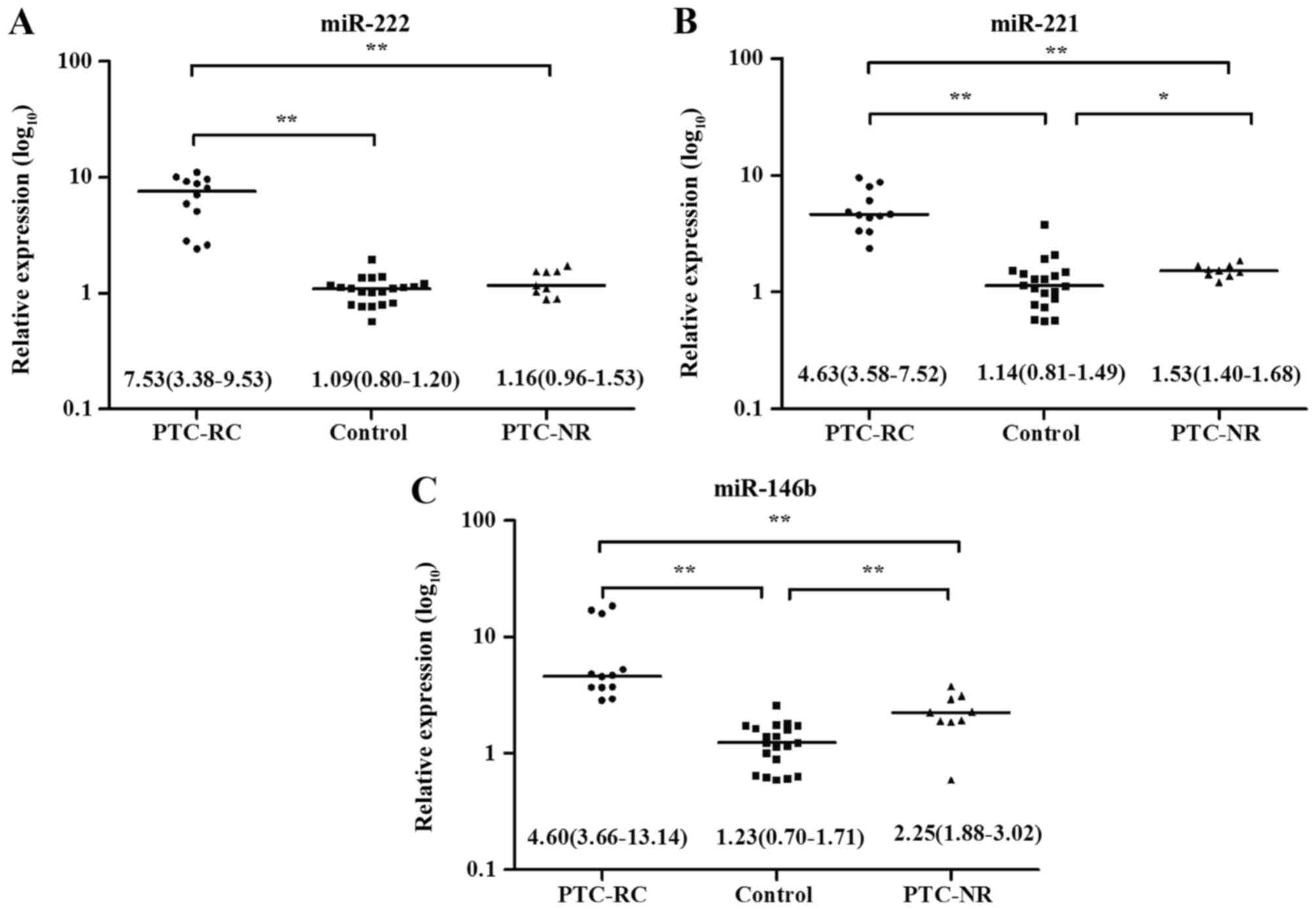 | Figure 7.The relative expression levels of (A)
miR-222, (B) miR-221 and (C) miR-146b in the PTC-RC group (n=12;
median=7.53,4.63 and 4.60; range=3.38–9.53, 3.58–7.52 and
3.66–13.14, respectively) were significantly increased compared
with the control (n=20; median=1.09, 1.14 and 1.23;
range=0.80–1.20, 0.81–1.49 and 0.70–1.71, respectively; *P<0.05
and **P<0.01) and PTC-NR groups (n=9; median=1.16, 1.53 and
2.25; range=0.96–1.53, 1.40–1.68 and 1.88–3.02, respectively;
**P<0.01). miR, microRNA; PTC-RC, papillary thyroid carcinoma
with recurrence; PTC-NR, papillary thyroid carcinoma without
recurrence. |
| Table III.Characteristics of patients with
recurrence and with no recurrence. |
Table III.
Characteristics of patients with
recurrence and with no recurrence.
|
Characteristics | PTC-RC, n=12 | PTC-NR, n=9 | P-value |
|---|
| Sex, n (%) |
|
Male | 5 (41.7) | 3 (33.3) | 1.00 |
|
Female | 7 (58.3) | 6 (66.7) |
|
| Age, year (mean ±
SD) | 49.73±15.60 | 47.75±10.81 | 0.76 |
| Tumor size, cm
(%) |
|
≤2.0 | 4 (33.3) | 5 (55.6) | 0.39 |
|
>2.0 | 8 (66.7) | 4 (44.4) |
|
| Tumor location, n
(%) |
|
Unilateral | 3 (25.0) | 3 (33.3) | 1.00 |
|
Bilateral | 9 (75.0) | 6 (66.7) |
|
| Multicentricity, n
(%) |
|
Yes | 6 (50.0) | 5 (55.6) | 1.00 |
| No | 6 (50.0) | 4 (44.4) |
|
| Extrathyroidal
invasion, n (%) |
|
Yes | 5 (41.7) | 2 (22.2) | 0.64 |
| No | 7 (58.3) | 7 (77.8) |
|
| Metastatic lymph
node, n (%) |
|
Yes | 11 (91.7) | 7 (77.8) | 0.55 |
| No | 1 (8.3) | 2 (22.2) |
|
| TNM stage, n
(%) |
|
I/II | 5 (41.7) | 4 (44.4) | 1.00 |
|
III/IV | 7 (58.3) | 5 (55.6) |
|
| AMES, n (%) |
| Low
risk | 9 (75.0) | 8 (88.9) | 0.60 |
| High
risk | 3 (25.0) | 1 (11.1) |
|
| DFS, median month
(range) | 52 (10–124) | 51.5 (16–108) | 0.90 |
| miR-222, RQ: Median
(IQR) | 7.53
(3.38–9.53) | 1.49
(1.06–1.53) | <0.001 |
| miR-221, RQ: Median
(IQR) | 4.63
(3.58–7.52) | 1.53
(1.40–1.68) | <0.001 |
| miR-146b, RQ:
Median (IQR) | 4.60
(3.66–13.14) | 2.25
(1.88–3.02) |
0.001 |
Discussion
Since miRNAs were first identified in
Caenorhabditis elegans in 1993 by Lee et al (46). To date, >1,000 human miRNAs have
been reported in the miRBase sequence database (47). The majority of previous studies have
examined miRNA expression in tumor cells and tissues from patients
with PTC (32,48–51).
Although tissue miRNA profiles are useful for distinguishing BTN
from PTC, obtaining tissue requires an invasive procedure, and
these profiles are not able to be used as biomarkers for
presurgical diagnoses. By contrast, serum sampling is minimally
invasive and easy to perform, making it attractive when exploring
potential biomarkers. There are several advantages to measuring
levels of circulating miRNAs. Firstly, as nucleotide non-coding
RNA, miRNA can be amplified and detected with high sensitivity and
specificity in serum, plasma and other bodily fluids. Secondly,
miRNA arrays and RT-qPCR methodologies allow the quantification of
numerous miRNAs in a single experiment. The combined analysis of
miRNAs and their co-expression patterns (miRNA networks) may
enhance their predictive power. miRNAs are also relatively stable
over time in the human blood and appear to be protected from
degradation through various mechanisms (44). The stability of miRNA in bodily fluids
and the numerous changes in expression in cancer suggest that
circulating miRNAs may possess a diagnostic value. Previous studies
have measured circulating miRNAs in serum and plasma as noninvasive
biomarkers for cancer, including lung, breast and colorectal cancer
(52–56).
To date, a limited number of studies have addressed
the use of circulating miRNA quantification in patients with PTC.
Yu et al (33) first reported
that miR-222, miR-151-5p and let-7e were significantly
overexpressed in patients with PTC compared with either patients
with benign nodule or controls (33).
Expression of these miRNAs correlated with certain
clinicopathological variables, including nodal status, tumor size,
multifocal lesion status and TNM stage, and the expression levels
decreased significantly following tumor excision in patients with
PTC (33). Another study performed in
Australia identified serum expression levels of miR-222, miR-221
and miR-146b that were much higher in patients with PTC compared
with in healthy controls and decreased significantly in
postoperative patients with PTC compared with the preoperative
levels (29). The same study also
revealed that the plasma levels of miR-222, miR-221 and miR-146b
were significantly overexpressed in preoperative patients with
multinodular goiters compared with healthy controls. However, no
significant difference was observed between the PTC and
multinodular goiter groups prior to surgery (29). In addition, the study also
demonstrated that miR-222 and miR-146b were overexpressed in tumor
tissue samples of patients with PTC-RC compared with patients with
PTC-NC (29). However, the expression
of miR-222 and miR-146b in serum was not detected (29). By contrast, Lee et al (35) reported that the expression levels of
miR-222 and miR-221 in the PTC group were increased compared with
those in the benign group; however, these differences were not
significant. Cantara et al (34) also identified miR-190 and miR-95 as
being overexpressed in the serum of patients with PTC compared with
patients with BTN and controls.
Although these studies have offered promising
evidence that identifying circulating miRNAs is useful and formed
the basis for our study, there remains controversy and ambiguity in
these findings. Firstly, the diagnostic value of miR-222 and
miR-146b were determined in patients with PTC compared with
patients with BTN and healthy controls. Secondly, it was unclear
whether the group with benign nodules in these studies had solitary
nodules, multinodular goiter, or solitary nodules and multinodular
goiter. In addition, these studies did not determine whether the
circulating miRNAs are able to distinguish between patients with
and without recurrence. Finally, the dynamic expression patterns of
circulating miRNA have not yet been clearly elucidated. Therefore,
additional studies are required to more comprehensively determine
whether the presence of circulating miRNAs is able to determine
diagnosis, prognosis and recurrence.
Therefore, the present study analyzed miRNA
expression in the serum from a cohort of patients with PTC,
patients with BTN and controls and reported 4 significant
observations. Firstly, it was revealed that miR-222, miR-221 and
miR-146b in patients with PTC were overexpressed in serum compared
with patients with BTN and control subjects, as detected using
RT-qPCR. The diagnostic value of these three miRNAs was also
investigated using an ROC curve analysis, and the present study
demonstrated that these three miRNAs may represent promising
biomarkers and serve as an accurate diagnostic tool for the
preoperative diagnosis of PTC. Secondly, the present study also
reported the association between the expression levels of the three
miRNAs and various clinicopathological features of patients with
PTC. The analysis indicated that all three elevated miRNAs were
associated with lymph node metastasis, extrathyroid invasion,
advanced TNM stage, bilateral thyroid lesions and high risk
patients. In addition, miR-222 was significantly associated with
tumor size (>2 cm), and miR-221 was significantly associated
with multifocal lesions.
The present study dynamically monitored these miRNAs
at 1, 3, 6 and 12 months following surgery and revealed that their
expression levels decreased rapidly in serum following surgery in
the PTC group. Additionally, the expression levels of miR-222,
miR-221 and miR-146b gradually decreased between 3 and 6 months
following surgery in the PTC group. A similar pattern was observed
with miR-146b expression in the BTN group prior to and subsequent
to surgery. However, the miR-222 and miR-221 levels were stable and
did not change significantly following surgery in the BTN group.
The miR-146b level increased at 1 month following surgery compared
with 3 months subsequent to surgery. The present study also
confirmed that the miR-222, miR-221 and miR-146b expression levels
in patients with PTC-RC were significantly increased compared with
patients with PTC-NR or controls.
Several studies have reported the function and
mechanism of upregulated miR-146b in PTC. Yip et al
(57) and Wang et al (30) demonstrated that miR-146b and miR-222
are significantly overexpressed in aggressive PTC compared with
nonaggressive PTC. Among BRAF-positive tumors, overexpression of
miR-146b is associated with aggressive behavior, suggesting that it
may additionally refine the prognostic significance of BRAF
(58,59). Previous studies have revealed that the
overexpression of miR-146b was associated with PTC carcinogenesis
and was associated with extrathyroidal invasion, advanced stages,
BRAF mutations, large tumor sizes (>2 cm) and lower overall
survival rates in patients with PTC (38,57–59). These
results highlight the importance of miR-146b in determining the
aggression of PTC and may aid the identification of potential gene
targets associated with tumor aggression in PTC. The present study
demonstrated that serum miR-146b expression levels possess a poor
prognostic value when dynamically monitoring patients with PTC. The
target genes regulated by miR-146b remain largely unknown, and
little has been reported regarding the molecular mechanisms by
which miR-146b influences tumor aggression in PTC. Previously,
Geraldo et al (60)
demonstrated that miR-146b regulates the signal transduction
pathways of transforming growth factor-β (TGF-β) by repressing
SMAD4 in thyroid tumorigenesis. miR-146b overexpression in PCCL3
cells also significantly increases cellular proliferation in the
absence of TSH and confers resistance to TGF-β-mediated cell cycle
arrest (61).
Previous studies have indicated that the miR-222 and
miR-221 expression levels in the tumor tissues of patients with PTC
are significantly increased compared with in patients with BTN and
controls, and are closely associated with lymph node metastasis,
advanced TNM stage and extrathyroidal invasion in patients with PTC
(51,62–65).
Similar to previous studies, analysis in the present study
indicated that elevated serum miR-222 and miR-221 levels are
associated with lymph node metastasis, extrathyroidal invasion,
advanced TNM stage and high risk in PTC patients. The present study
initially identified that the overexpression of serum miR-222 is
clearly associated with tumor size (>2 cm), and the
overexpression of serum miR-221 is associated with bilateral tumor
location in patients with PTC. As the two miRNAs are clustered on
the X chromosome, they may be encoded by a single polycistronas
previously suggested (66,67). Previous studies (68–71) have
indicated that the target genes of miR-222 and miR-221 are p27, p57
and PUMA, and that these may perform essential roles in thyroid
oncogenesis (72).
The dynamic expression patterns of circulating
miRNAs have not yet been clearly and systematically reported for
various cancer types, including PTC. Lee et al (29) identified that the plasma levels of
miR-222, miR-221 and miR-146b decreased significantly in patients
subsequent to a total thyroidectomy with central lymph node
dissection between 2 and 6 weeks following surgery. To the best of
our knowledge, the present study is the first to dynamically
monitor 3 serum miRNAs at 1 year following surgery in patients with
PTC. To additionally investigate whether the levels of these 3
miRNAs may be used to monitor postoperative progression, 3 miRNAs
were used to perform the subsequent validation at different
postoperative time points, including 1, 3, 6 and 12 months, in
patients with PTC or BTN. The 3 miRNAs exhibited different
expression levels in postoperative patients with PTC 12 months
following surgery, and the expression levels steadily decreased at
1, 3, 6 and 12 months following surgery. It is speculated that
these serum miRNAs are released into the peripheral blood from
thyroid tissues and that they correlate closely with the
development of PTC.
At present, no conclusive evidence has identified
patients who are at higher risk of recurrence. Due to the
alterations of these miRNA levels following thyroidectomy, studies
with larger numbers of patients are required to confirm whether
these miRNAs can serve as biomarkers for monitoring tumor
recurrence and predicting prognosis. Lee et al (29) identified miR-222 and miR-146b as
molecular markers of recurrence in tumor tissues; however, they did
not measure serum expression in patients with PTC with recurrence.
The present study is the first to compare these miRNAs in serum
between patients with PTC with and without recurrence with either
newly emerged lymph nodules or suspicious new neck masses following
an initial thyroidectomy due to PTC. Recurrence was confirmed by
pathology. The present results indicate that serum miR-222, miR-221
and miR-146b increased significantly in patients with recurrence
compared with patients without recurrence and control subjects.
Serum miRNA levels may be tested periodically to
monitor patients with suspected PTC or recurrence, preferably at
clinically asymmetric stages. Based on the present results, a
screening test for the expression of miRNA in serum would have a
number of advantages. Firstly, since the test would be performed on
a large population, it should be minimally invasive or noninvasive.
Secondly, the presence, stability and reliable detectability of
miRNA in serum make this sample easily obtained by minimally
invasive methods. In addition, the screen is a cost-efficient test
that can be performed using RT-qPCR. Finally, the expression levels
of serum miRNA are specific and sensitive for PTC and are a
potential tool for long-term surveillance. Therefore, this screen
may be particularly useful in patients for whom the measurement of
serum TG is not suitable, including patients with anti-TG
antibodies or whose tumors have lost TG expression.
Several limitations of the present study must be
noted. Firstly, this study is a randomized multicenter controlled
trial with a selection bias for patients with PTC and BTN.
Secondly, the miRNAs identified in the present study differed from
those reported in other studies. It is speculated that this
difference may be due to different genetic backgrounds and
clinicopathological features of patients with PTC and BTN. Thirdly,
the relatively small sample size and short-term follow-up resulted
in insufficient information regarding prognosis and recurrence.
Additional investigations with a larger cohort of samples and
long-term follow-up are required to validate the observations of
the present study.
In conclusion, the present study demonstrated that
miR-222, miR-221 and miR-146b were overexpressed in patients with
PTC compared with patients with BTN and controls, and their
expression was associated with certain poorer prognostic variables.
The present results also indicated that miR-222, miR-221 and
miR-146b may serve as indexes for dynamic monitoring in patients
with PTC, and these miRNAs are associated with PTC-RC. Therefore,
miR-222, miR-221 and miR-146b have the potential to be novel
non-invasive and effective diagnostic, prognostic and recurrent
biomarkers for patients with PTC prior to and subsequent to
surgery.
Acknowledgements
The present study was supported by grants from the
Natural Science foundation of China (grant nos 81473053 and
81673108) and the National Basic Research Program of China (973
Program; grant no SQ2013CB051164).
References
|
1
|
Bann DV, Goyal N, Camacho F and Goldenberg
D: Increasing incidence of thyroid cancer in the Commonwealth of
Pennsylvania. JAMA Otolaryngol Head Neck Surg. 140:1149–1156. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
N Howlader AMN and M Krapcho JG: SEER
Cancer Statistics Review, 1975–2011. Bethesda, MD: National Cancer
Institute; 2014
|
|
3
|
Leenhardt L, Grosclaude P and
Chérié-Challine L; Thyroid Cancer Committee, : Increased incidence
of thyroid carcinoma in France: A true epidemic or thyroid nodule
management effects? Report from the French Thyroid Cancer
Committee. Thyroid. 14:1056–1060. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Pacini F, Schlumberger M, Dralle H, Elisei
R, Smit JW and Wiersinga W; European Thyroid Cancer, : European
consensus for the management of patients with differentiated
thyroid carcinoma of the follicular epithelium. Eur J Endocrinol.
154:787–803. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
American Thyroid Association (ATA)
Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid
Cancer, ; Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL,
Mandel SJ, Mazzaferri EL, McIver B, Pacini F, et al: Revised
American thyroid association management guidelines for patients
with thyroid nodules and differentiated thyroid cancer. Thyroid.
19:1167–1214. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Cooper DS, Doherty GM, Haugen BR, Kloos
RT, Lee SL, Mandel SJ, Mazzaferri EL, McIver B, Sherman SI and
Tuttle RM: American Thyroid Association Guidelines Taskforce:
Management guidelines for patients with thyroid nodules and
differentiated thyroid cancer. Thyroid. 16:109–142. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Pusztaszeri MP, Bongiovanni M and Faquin
WC: Update on the cytologic and molecular features of medullary
thyroid carcinoma. Adv Anat Pathol. 21:26–35. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Zhao L, Gong Y, Wang J, Dawlett M, Huo L,
Caraway NP and Guo M: Ultrasound-guided fine-needle aspiration
biopsy of thyroid bed lesions from patients with thyroidectomy for
thyroid carcinomas. Cancer Cytopathol. 121:101–107. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lew JI, Snyder RA, Sanchez YM and
Solorzano CC: Fine needle aspiration of the thyroid: Correlation
with final histopathology in a surgical series of 797 patients. J
Am Coll Surg. 213:188–195. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Cibas ES and Ali SZ: The bethesda system
for reporting thyroid cytopathology. Thyroid. 19:1159–1165. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Gharib H, Papini E, Paschke R, Duick DS,
Valcavi R, Hegedüs L and Vitti P: AACE/AME/ETA Task Force on
Thyroid Nodules: American Association of Clinical Endocrinologists,
Associazione Medici Endocrinologi and European Thyroid Association
Medical guidelines for clinical practice for the diagnosis and
management of thyroid nodules: Executive summary of
recommendations. Endocr Pract. 16:468–475. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Leboulleux S, Rubino C, Baudin E, Caillou
B, Hartl DM, Bidart JM, Travagli JP and Schlumberger M: Prognostic
factors for persistent or recurrent disease of papillary thyroid
carcinoma with neck lymph node metastases and/or tumor extension
beyond the thyroid capsule at initial diagnosis. J Clin Endocrinol
Metab. 90:5723–5729. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Suh YJ, Kwon H, Kim SJ, Choi JY, Lee KE,
Park YJ, do J Park and Youn YK: Factors affecting the locoregional
recurrence of conventional papillary thyroid carcinoma after
surgery: A retrospective analysis of 3381 patients. Ann Surg Oncol.
22:3543–3549. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Spencer CA: Challenges of serum
thyroglobulin (Tg) measurement in the presence of Tg
autoantibodies. J Clin Endocrinol Metab. 89:3702–3704. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Woodmansee WW and Haugen BR: Uses for
recombinant human TSH in patients with thyroid cancer and nodular
goiter. Clin Endocrinol (Oxf). 61:163–173. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Castagna MG, Brilli L, Pilli T, Montanaro
A, Cipri C, Fioravanti C, Sestini F, Capezzone M and Pacini F:
Limited value of repeat recombinant human thyrotropin
(rhTSH)-stimulated thyroglobulin testing in differentiated thyroid
carcinoma patients with previous negative rhTSH-stimulated
thyroglobulin and undetectable basal serum thyroglobulin levels. J
Clin Endocrinol Metab. 93:76–81. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Snozek CL, Chambers EP, Reading CC, Sebo
TJ, Sistrunk JW, Singh RJ and Grebe SK: Serum thyroglobulin,
high-resolution ultrasound and lymph node thyroglobulin in
diagnosis of differentiated thyroid carcinoma nodal metastases. J
Clin Endocrinol Metab. 92:4278–4281. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Orlov S, Salari F, Kashat L, Freeman JL,
Vescan A, Witterick IJ and Walfish PG: Post-operative stimulated
thyroglobulin and neck ultrasound as personalized criteria for risk
stratification and radioactive iodine selection in low- and
intermediate-risk papillary thyroid cancer. Endocrine. 50:130–137.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Londero SC, Krogdahl A, Bastholt L,
Overgaard J, Pedersen HB, Hahn CH, Bentzen J, Schytte S,
Christiansen P, Gerke O, et al: Papillary thyroid carcinoma in
Denmark, 1996–2008: Outcome and evaluation of established
prognostic scoring systems in a prospective national cohort.
Thyroid. 25:78–84. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Lu J, Getz G, Miska EA, Alvarez-Saavedra
E, Lamb J, Peck D, Sweet-Cordero A, Ebert BL, Mak RH, Ferrando AA,
et al: MicroRNA expression profiles classify human cancers. Nature.
435:834–838. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Volinia S, Calin GA, Liu CG, Ambs S,
Cimmino A, Petrocca F, Visone R, Iorio M, Roldo C, Ferracin M, et
al: A microRNA expression signature of human solid tumors defines
cancer gene targets. Proc Natl Acad Sci USA. 103:pp. 2257–2261.
2006; View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Lawrie CH, Gal S, Dunlop HM, Pushkaran B,
Liggins AP, Pulford K, Banham AH, Pezzella F, Boultwood J,
Wainscoat JS, et al: Detection of elevated levels of
tumour-associated microRNAs in serum of patients with diffuse large
B-cell lymphoma. Br J Haematol. 141:672–675. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Kou CH, Zhou T, Han XL, Zhuang HJ and Qian
HX: Downregulation of mir-23b in plasma is associated with poor
prognosis in patients with colorectal cancer. Oncol Lett.
12:4838–4844. 2016.PubMed/NCBI
|
|
24
|
Hanke M, Hoefig K, Merz H, Feller AC,
Kausch I, Jocham D, Warnecke JM and Sczakiel G: A robust
methodology to study urine microRNA as tumor marker: microRNA-126
and microRNA-182 are related to urinary bladder cancer. Urol Oncol.
28:655–661. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Park NJ, Zhou H, Elashoff D, Henson BS,
Kastratovic DA, Abemayor E and Wong DT: Salivary microRNA:
Discovery, characterization, and clinical utility for oral cancer
detection. Clin Cancer Res. 15:5473–5477. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Faam B, Ghaffari MA, Ghadiri A and Azizi
F: Epigenetic modifications in human thyroid cancer. Biomed Rep.
3:3–8. 2015.PubMed/NCBI
|
|
27
|
Yang Z, Yuan Z, Fan Y, Deng X and Zheng Q:
Integrated analyses of microRNA and mRNA expression profiles in
aggressive papillary thyroid carcinoma. Mol Med Rep. 8:1353–1358.
2013.PubMed/NCBI
|
|
28
|
Peng Y, Li C, Luo DC, Ding JW, Zhang W and
Pan G: Expression profile and clinical significance of microRNAs in
papillary thyroid carcinoma. Molecules. 19:11586–11599. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Lee JC, Zhao JT, Clifton-Bligh RJ, Gill A,
Gundara JS, Ip JC, Glover A, Sywak MS, Delbridge LW, Robinson BG
and Sidhu SB: MicroRNA-222 and microRNA-146b are tissue and
circulating biomarkers of recurrent papillary thyroid cancer.
Cancer. 119:4358–4365. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Wang Z, Zhang H, He L, Dong W, Li J, Shan
Z and Teng W: Association between the expression of four
upregulated miRNAs and extrathyroidal invasion in papillary thyroid
carcinoma. Onco Targets Ther. 6:281–287. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Dettmer M, Perren A, Moch H, Komminoth P,
Nikiforov YE and Nikiforova MN: Comprehensive MicroRNA expression
profiling identifies novel markers in follicular variant of
papillary thyroid carcinoma. Thyroid. 23:1383–1389. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
He H, Jazdzewski K, Li W, Liyanarachchi S,
Nagy R, Volinia S, Calin GA, Liu CG, Franssila K, Suster S, et al:
The role of microRNA genes in papillary thyroid carcinoma. Proc
Natl Acad Sci USA. 102:pp. 19075–19080. 2005; View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Yu S, Liu Y, Wang J, Guo Z, Zhang Q, Yu F,
Zhang Y, Huang K, Li Y, Song E, et al: Circulating microRNA
profiles as potential biomarkers for diagnosis of papillary thyroid
carcinoma. J Clin Endocrinol Metab. 97:2084–2092. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Cantara S, Pilli T, Sebastiani G, Cevenini
G, Busonero G, Cardinale S, Dotta F and Pacini F: Circulating
miRNA95 and miRNA190 are sensitive markers for the differential
diagnosis of thyroid nodules in a Caucasian population. J Clin
Endocrinol Metab. 99:4190–4198. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Lee YS, Lim YS, Lee JC, Wang SG, Park HY,
Kim SY and Lee BJ: Differential expression levels of plasma-derived
miR-146b and miR-155 in papillary thyroid cancer. Oral Oncol.
51:77–83. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Vrachimis A, Gerss J, Stoyke M, Wittekind
C, Maier T, Wenning C, Rahbar K, Schober O and Riemann B: No
significant difference in the prognostic value of the 5th and 7th
editions of AJCC staging for differentiated thyroid cancer. Clin
Endocrinol (Oxf). 80:911–917. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Cady B and Rossi R: An expanded view of
risk-group definition in differentiated thyroid carcinoma. Surgery.
104:947–953. 1988.PubMed/NCBI
|
|
38
|
Sun Y, Yu S, Liu Y, Wang F, Liu Y and Xiao
H: Expression of miRNAs in papillary thyroid carcinomas is
associated with BRAF mutation and clinicopathological features in
Chinese patients. Int J Endocrinol. 2013:1287352013. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Chou CK, Chen RF, Chou FF, Chang HW, Chen
YJ, Lee YF, Yang KD, Cheng JT, Huang CC and Liu RT: miR-146b is
highly expressed in adult papillary thyroid carcinomas with high
risk features including extrathyroidal invasion and the BRAF
(V600E) mutation. Thyroid. 20:489–494. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Kroh EM, Parkin RK, Mitchell PS and Tewari
M: Analysis of circulating microRNA biomarkers in plasma and serum
using quantitative reverse transcription-PCR (qRT-PCR). Methods.
50:298–301. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Toiyama Y, Tanaka K, Inoue Y, Mohri Y and
Kusunoki M: Circulating cell-free microRNAs as biomarkers for
colorectal cancer. Surg Today. 46:13–24. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Xiang M, Zeng Y, Yang R, Xu H, Chen Z,
Zhong J, Xie H, Xu Y and Zeng X: U6 is not a suitable endogenous
control for the quantification of circulating microRNAs. Biochem
Biophys Res Commun. 454:210–214. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
McDermott AM, Kerin MJ and Miller N:
Identification and validation of miRNAs as endogenous controls for
RQ-PCR in blood specimens for breast cancer studies. PLoS One.
8:e837182013. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Alegre E, Sanmamed MF, Rodriguez C,
Carranza O, Martin-Algarra S and Gonzalez A: Study of circulating
microRNA-125b levels in serum exosomes in advanced melanoma. Arch
Pathol Lab Med. 138:828–832. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(−Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Lee RC, Feinbaum RL and Ambros V: The C.
elegans heterochronic gene lin-4 encodes small RNAs with antisense
complementarity to lin-14. Cell. 75:843–854. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Griffiths-Jones S, Saini HK, van Dongen S
and Enright AJ: miRBase: Tools for microRNA genomics. Nucleic Acids
Res. 36(Database issue): D154–D158. 2008.PubMed/NCBI
|
|
48
|
Wang C, Lu S, Jiang J, Jia X, Dong X and
Bu P: Hsa-microRNA-101 suppresses migration and invasion by
targeting Rac1 in thyroid cancer cells. Oncol Lett. 8:1815–1821.
2014.PubMed/NCBI
|
|
49
|
Nikiforova MN, Tseng GC, Steward D, Diorio
D and Nikiforov YE: MicroRNA expression profiling of thyroid
tumors: Biological significance and diagnostic utility. J Clin
Endocrinol Metab. 93:1600–1608. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Zhu YZ, Zheng K, Zhang HH, Chen L, Wu KL,
Ren CH, Wang ZC, Kong LJ, Ruan WH and Chen XJ: Expression of
microRNA-155 in papillary thyroid carcinoma and its clinical
significance. Nan Fang Yi Ke Da Xue Xue Bao. 36:1364–1368. 2016.(In
Chinese). PubMed/NCBI
|
|
51
|
Xu J, Zhang D, Niu Q, Nan Y, Shi C, Zhao H
and Liang X: Value of distinguishing differentiated thyroid
carcinoma by miRNA. Oncol Lett. 12:79–82. 2016.PubMed/NCBI
|
|
52
|
Engelhardt S: Small RNA biomarkers come of
age. J Am Coll Cardiol. 60:300–303. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Markou A, Sourvinou I, Vorkas PA, Yousef
GM and Lianidou E: Clinical evaluation of microRNA expression
profiling in non small cell lung cancer. Lung Cancer. 81:388–396.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Eichelser C, Flesch-Janys D, Chang-Claude
J, Pantel K and Schwarzenbach H: Deregulated serum concentrations
of circulating cell-free microRNAs miR-17, miR-34a, miR-155, and
miR-373 in human breast cancer development and progression. Clin
Chem. 59:1489–1496. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Menendez P, Villarejo P, Padilla D,
Menéndez JM and Montes JA: Diagnostic and prognostic significance
of serum microRNAs in colorectal cancer. J Surg Oncol. 107:217–220.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Ng EK, Chong WW, Jin H, Lam EK, Shin VY,
Yu J, Poon TC, Ng SS and Sung JJ: Differential expression of
microRNAs in plasma of patients with colorectal cancer: A potential
marker for colorectal cancer screening. Gut. 58:1375–1381. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Yip L, Kelly L, Shuai Y, Armstrong MJ,
Nikiforov YE, Carty SE and Nikiforova MN: MicroRNA signature
distinguishes the degree of aggressiveness of papillary thyroid
carcinoma. Ann Surg Oncol. 18:2035–2041. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Chou CK, Yang KD, Chou FF, Huang CC, Lan
YW, Lee YF, Kang HY and Liu RT: Prognostic implications of miR-146b
expression and its functional role in papillary thyroid carcinoma.
J Clin Endocrinol Metab. 98:E196–E205. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Sun M, Fang S, Li W, Li C, Wang L, Wang F
and Wang Y: Associations of miR-146a and miR-146b expression and
clinical characteristics in papillary thyroid carcinoma. Cancer
Biomark. 15:33–40. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Geraldo MV, Yamashita AS and Kimura ET:
MicroRNA miR-146b-5p regulates signal transduction of TGF-β by
repressing SMAD4 in thyroid cancer. Oncogene. 31:1910–1922. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Lima CR, Geraldo MV, Fuziwara CS, Kimura
ET and Santos MF: MiRNA-146b-5p upregulates migration and invasion
of different papillary thyroid carcinoma cells. BMC Cancer.
16:1082016. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Cong D, He M, Chen S, Liu X, Liu X and Sun
H: Expression profiles of pivotal microRNAs and targets in thyroid
papillary carcinoma: an analysis of The Cancer Genome Atlas. Onco
Targets Ther. 8:2271–2277. 2015.PubMed/NCBI
|
|
63
|
Lee JC, Zhao JT, Gundara J, Serpell J,
Bach LA and Sidhu S: Papillary thyroid cancer-derived exosomes
contain miRNA-146b and miRNA-222. J Surg Res. 196:39–48. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Chen YT, Kitabayashi N, Zhou XK, Fahey TJ
III and Scognamiglio T: MicroRNA analysis as a potential diagnostic
tool for papillary thyroid carcinoma. Mod Pathol. 21:1139–1146.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Diao Y, Fu H and Wang Q: MiR-221
exacerbate cell proliferation and invasion by targeting TIMP3 in
papillary thyroid carcinoma. Am J Ther. Apr 12–2016.(Epub ahead of
print).
|
|
66
|
Zhang L, Wang T, Wright AF, Suri M,
Schwartz CE, Stevenson RE and Valle D: A microdeletion in Xp11.3
accounts for co-segregation of retinitis pigmentosa and mental
retardation in a large kindred. Am J Med Genet A. 140:349–357.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Yang QE, Racicot KE, Kaucher AV, Oatley MJ
and Oatley JM: MicroRNAs 221 and 222 regulate the undifferentiated
state in mammalian male germ cells. Development. 140:280–290. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Martins CS, Camargo RC, Saggioro FP, Neder
L, Machado HR, Moreira AC and de Castro M: P27/CDKN1B translational
regulators in pituitary tumorigenesis. Horm Metab Res. 48:840–846.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Castagnino P, Kothapalli D, Hawthorne EA,
Liu SL, Xu T, Rao S, Yung Y and Assoian RK: miR-221/222 compensates
for Skp2-mediated p27 degradation and is a primary target of cell
cycle regulation by prostacyclin and cAMP. PLoS One. 8:e561402013.
View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Kothapalli D, Castagnino P, Rader DJ,
Phillips MC, Lund-Katz S and Assoian RK: Apolipoprotein E-mediated
cell cycle arrest linked to p27 and the Cox2-dependent repression
of miR221/222. Atherosclerosis. 227:65–71. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Sun K, Wang W, Lei ST, Wu CT and Li GX:
MicroRNA-221 promotes colon carcinoma cell proliferation in vitro
by inhibiting CDKN1C/p57 expression. Nan Fang Yi Ke Da Xue Xue Bao.
31:1885–1889. 2011.(In Chinese). PubMed/NCBI
|
|
72
|
Visone R, Russo L, Pallante P, de Martino
I, Ferraro A, Leone V, Borbone E, Petrocca F, Alder H, Croce CM and
Fusco A: MicroRNAs (miR)-221 and miR-222, both overexpressed in
human thyroid papillary carcinomas, regulate p27Kip1 protein levels
and cell cycle. Endocr Relat Cancer. 14:791–798. 2007. View Article : Google Scholar : PubMed/NCBI
|