Introduction
Breast cancer is a highly histological heterogeneous
disease comprised of several biologically different phenotypes
(1). One of these subtypes,
triple-negative breast cancer (TNBC), is defined by the lack of
expression of estrogen receptor (ER), progesterone receptor (PR)
and human epidermal growth factor receptor 2 (HER2) in the tumor
specimen, and comprises 10–20% of all diagnosed breast cancer cases
(2,3).
Patients diagnosed with TNBC normally have a younger age, higher
grade and higher rate of cellular tumor antigen p53 (p53) mutation
when compared with those of other breast cancer subtypes (4). Furthermore, due to the lack of hormone
receptor and HER2 targets, patients with TNBC do not have access to
targeted therapy or adjuvant endocrine treatment. Thus, they have a
higher incidence of early local recurrence or distant organ
metastases (5). Therefore, novel
methods to improve the prognosis of TNBC are urgently required.
According to the cancer stem cell hypothesis
(6), cancer stem cells are considered
as the source of malignancy, invasion and metastasis. In
preclinical study, the cancer stem cell subpopulation is defined by
two key characteristics, namely, self-renewal and multi-directional
differentiation (7). A previous study
by Al-hajj et al demonstrated that as few as 100
epithelial-specific antigen (ESA+)/lineage
(Lin−)/cluster of differentiation
(CD)44+/CD24− breast cancer cells were able
to serially reproduce tumors when transplanted into immunodeficient
mice, whereas 200-fold more cells without these surface markers did
not possess tumorigenic potential; i.e., these breast cancer stem
cells had properties of self-renewal and longevity (8). In addition, the key cell surface markers
that can isolate the cancer stem cell subpopulation are
CD44+/CD24−, aldehyde dehydrogenase 1 (ALDH1)
(9), ESA+,
Lin−, bromodeoxyuridine (10) and side-population cell labeling
(11). More recently, breast cancer
stem cells have been isolated primarily by cell surface markers of
CD44+/CD24− and ALDH1+ (12).
Previous findings have shown that the cancer stem
cell markers CD44+/CD24− and
ALDH1+ are more enriched in TNBC tumor tissues compared
with those in other breast cancer subtypes, including luminal A,
luminal B and HER2-enriched (13,14).
However, the study of the role of cancer stem cells with regard to
the survival of patients with TNBC remains inadequate. In the
present study, the distribution of CD44/CD24 and ALDH1 expression
was detected using double-staining or single-staining
immunohistochemistry, and the clinical outcomes of different
CD44/CD24 phenotypes and ALDH1 expression, as well as other
clinical characteristics, were analyzed in patients with TNBC.
Patients and methods
Patients and tissue specimens
A cohort of 1,036 female patients with breast cancer
who received breast surgery between Feb 2004 and December 2008 in
the Cancer Hospital of Harbin Medical University (Harbin, China)
were studied, and 145 eligible patients with TNBC were identified.
Patients were aged between 28 and 76 years (median age, 50 years)
at enrollment. Immunohistochemistry (ER <1%, PR <1% and HER2
<10%) of breast tumors was not positive by re-staining. Patients
were excluded from this cohort if they had undergone radiotherapy,
chemotherapy, targeted therapy or adjuvant endocrine treatment
prior to surgery. Patients were also excluded if the histological
specimens could not be collected or if they had not undergone
active follow-up. In addition, the patients who had developed
distant organ metastases or T4 tumors prior to surgery were not
included in the present study. Consequently, the final study cohort
consisted of 145 patients with stage I-Шa TNBC. For pathological
staging, the Tumor-Node-Metastasis staging system in the seventh
edition of the American Joint Committee on Cancer was used
(15).
Detailed clinical data of patients were collected
from hospital registries and medical records. Information about age
at diagnosis (<40, 40–49, 50–59 and ≥60 years), menopausal
status (premenopausal or postmenopausal), tumor size (<2, 2–5
and >5 cm), the number of lymph nodes involved (0, 1–3 and ≥4),
pathology (intraductal carcinoma, invasive ductal carcinoma,
invasive lobular carcinoma and other types), radiotherapy (yes or
no), chemotherapy [no chemotherapy, derivative regimens of
cyclophosphamide, adriamycin and fluorouracil (CAF), such as CAF,
cyclophosphamide, epirubicin and fluorouracil (CEF),
cyclophosphamide, pirarubicin and fluorouracil (CTF), or
ifosfamide, epirubicin and fluorouracil (IEF), regimens including
taxanes, such as paclitaxel or docetaxel and epirubicin (TE),
docetaxel and cyclophosphamide (TC), or docetaxel, adriamycin and
cyclophosphamide (TAC), and other regimens], dates of recurrences
or metastases and dates of mortality were collected. Disease-free
survival (DFS) was defined as the duration from the date of
diagnosis to the appearance of a regional recurrence or distant
metastasis. Overall survival (OS) was defined as the time from the
date of diagnosis to the mortality of the patient. The current
study was approved by the Harbin Medical University Medical Ethics
Committee and has therefore been performed in accordance with the
ethical standards laid down in the 1964 Declaration of Helsinki and
its later amendments. All patients provided written informed
consent prior to inclusion in the study.
The suitable formalin-fixed, paraffin-embedded
tissues of invasive tumors were consecutively retrieved from the
Laboratory of Pathology, and 4-µm sections were cut and used for
immunohistochemical staining of Ki-67, p53, androgen receptor (AR),
vimentin, breast cancer susceptibility gene 1 (BRCA1),
cytokeratin5/6 (CK5/6), epidermal growth factor receptor (EGFR),
ALDH1, CD44 and CD24.
Immunohistochemical staining
Expression of Ki-67, p53, AR, vimentin, BRCA1,
CK5/6, EGFR and ALDH1 was measured by immunohistochemical staining
in formalin-fixed paraffin tissue sections using methods described
previously (16,17). Sections were dewaxed in xylene,
rehydrated through a graded ethanol series and rinsed in distilled
water. Antigen retrieval was achieved by placing the glass slides
in citrate (pH 6.0; Sigma-Aldrich; Merck KGaA, Darmstadt, Germany)
or EDTA buffer (pH 9.0; Sigma-Aldrich; Merck KGaA) for 2 min under
high pressure. Sections (4-µm) were stained with the following
antibodies obtained from Abcam (Cambridge, UK): anti-Ki-67 (rabbit;
polyclonal; catalog no., ab15580; dilution, 1:50), anti-p53
(rabbit; monoclonal; catalog no., ab179477; dilution, 1:400),
anti-AR (rabbit; polyclonal; catalog no., ab74272; dilution, 1:50),
anti-vimentin (mouse; monoclonal; catalog no., ab8978; dilution,
1:150), anti-BRCA1 (mouse; monoclonal; catalog no., ab16780;
dilution, 1:150), anti-CK5/6 (mouse; monoclonal; catalog no.,
ab17133; dilution, 1:200), anti-EGFR (rabbit; polyclonal; catalog
no., ab2430; dilution, 1:25) and anti-ALDH1 (rabbit; monoclonal;
catalog no. ab52492; dilution, 1:250). The positive and negative
controls were designed in each staining experiment.
Double-staining immunohistochemistry with antibodies
for CD44 and CD24 was performed on all cases. The antibodies used
were anti-CD24 mouse antibody (monoclonal; catalog no., ab31622;
dilution, 1:500; Abcam) and anti-CD44 rabbit antibody (monoclonal;
catalog no., ab51037; dilution, 1:100; Abcam). Antigen retrieval
was performed under high pressure, and endogenous peroxidase
vitality was blocked by incubating the glass slides according to
the manufacturer's protocol. Following primary antibody
application, the slides were incubated with MultiVision Polymer
Cocktail (anti-rabbit/alkaline phosphatase and
anti-mouse/horseradish peroxidase; Zhongshan Golden Bridge
Biotechnology Co., Ltd., Beijing, China). CD44 was detected with
Nitro-Blue-Tetrazolium working solutions and visualized as a brown
stain, whereas CD24 was detected with 3-amino-9-ethylcarbozole and
identified as a red stain. Sections were counterstained with
hematoxylin, followed by mounting with aqueous ClearMount. A
negative control of the primary antibody replaced by Tris
phosphate-buffered saline and a positive control of a known
CD24+/CD44+ tissue slice were used in each
staining experiment.
Evaluation of staining
Staining results were assessed by two pathologists
to determine the immunohistochemistry score independently. An
average was used for any discrepant staining between cores from the
same patient. Cytoplasmic staining for ALDH1 was graded as 0 if
≤10% of the cells were stained, 1+ when 10–25% of the cells were
stained, 2+ when 26–50% of the cells were stained and 3+ when
>50% of the cells were stained. Staining sections were
visualized using an Axiophot microscope (Carl Zeiss AG, Oberkochen,
Germany; magnification, ×400). Five fields of view were randomly
selected for immunohistochemical scoring. The expression of Ki-67,
p53, AR, vimentin, BRCA1, CK5/6 and EGFR were evaluated as
previously described (17–21). CD44 was identified as brown mainly in
the membranous staining and CD24 was identified as red mainly in
the cytoplasmic and membranous staining. The frequencies of
CD44+/CD24− tumor cells were determined as
the percentage of cells with brown color staining without much
interference from red coloration, whereas
CD44−/CD24+ tumor cells were characterized as
the cells with intense red staining with absence of brown
coloration. CD44+/CD24+ cells were cells with
brown membranous staining and red cytoplasmic staining.
CD44−/CD24− cells exhibited no staining. A
tumor was categorized with the CD44+/CD24−
phenotype only when the proportion of
CD44+/CD24− cells was >10%, and the
CD44−/CD24+ and
CD44+/CD24+ phenotypes were categorized in
the same way. Tumors were defined as exhibiting the
CD44−/CD24− phenotype when none of the three
types of positive cells (CD44+/CD24−,
CD44−/CD24+ and
CD44+/CD24+ cells) reached a proportion of
>10%. In addition, if two (12.4%) or three (6.9%) cell types
reached a proportion of >10% in one field of view, they were
categorized in accordance with the predominant cell type.
Statistical analysis
Associations between CD44/CD24 status and clinical
characteristics were assessed using Fisher's exact test and the
χ2 test for categorical variables. The Kaplan-Meier
method was used to calculate DFS and OS curves, and the log-rank
test was performed to assess changes in the relative risk of events
according to prognostic factors in univariate analysis. In
addition, the Cox proportional hazards regression model was used
for multivariate analyses to estimate prognostic value [hazard
ratios (HRs) and 95% confidence intervals (CIs)] for the two main
study outcomes, DFS and OS. All tests were two-sided and P<0.05
was considered to indicate a statistically significant difference.
Statistical analyses were performed using SPSS version 19.0 (IBM
SPSS, Armonk, NY, USA).
Results
Baseline clinical characteristics
A total of 145 patients were enrolled in the present
study with a median follow-up time of 76 months, and their baseline
clinical characteristics are listed in Table I. The median times for DFS and OS were
67 and 71 months, respectively. A total of 39 patients (26.9%) had
suffered recurrence or metastasis and 35 patients (24.1%) had
succumbed by the end of follow-up. Overall, lymph node metastasis
was recorded in 51.7% of cases, of which 23.4% had 1–3 lymph nodes
involved and 28.3% had ≥4 lymph nodes involved. The predominant
chemotherapy regimens included derivative regimens of CAF, such as
CAF, CEF, CTF or IEF (n=53), and regimens including taxanes, such
as TE, TC or TAC (n=43), which accounted for 96 (80.7%) of the 119
patients who underwent adjuvant chemotherapy.
 | Table I.Baseline clinical characteristics of
triple-negative breast cancer. |
Table I.
Baseline clinical characteristics of
triple-negative breast cancer.
|
Characteristics | Patients, n
(%) |
|---|
| Age at diagnosis,
years |
|
|
<40 | 19 (13.1) |
|
40–49 | 53 (36.6) |
|
50–59 | 48 (33.1) |
|
≥60 | 25 (17.2) |
| Menopausal
status |
|
|
Premenopausal | 71 (49.0) |
|
Postmenopausal | 74 (51.0) |
| Tumor size, cm |
|
| ≤2 | 37 (25.5) |
|
2–5 | 96 (66.2) |
|
>5 | 12 (8.3) |
| Number of lymph
nodes involved |
|
| 0 | 70 (48.3) |
|
1–3 | 34 (23.4) |
| ≥4 | 41 (28.3) |
| Pathology |
|
|
Intraductal carcinoma | 4 (2.8) |
|
Invasive ductal carcinoma | 132 (91.0) |
|
Invasive lobular
carcinoma | 4 (2.8) |
| Other
types | 5 (3.4) |
| Radiotherapy |
|
| No | 125 (86.2) |
|
Yes | 20 (13.8) |
| Chemotherapy |
|
| No
chemotherapy | 26 (17.9) |
|
Derivative regimens of
CAF | 53 (36.6) |
| (CAF,
CEF, CTF or IEF) |
|
|
Regimens including
taxanes | 43 (29.7) |
| (TE, TC
or TAC) |
|
| Other
regimens | 23 (15.9) |
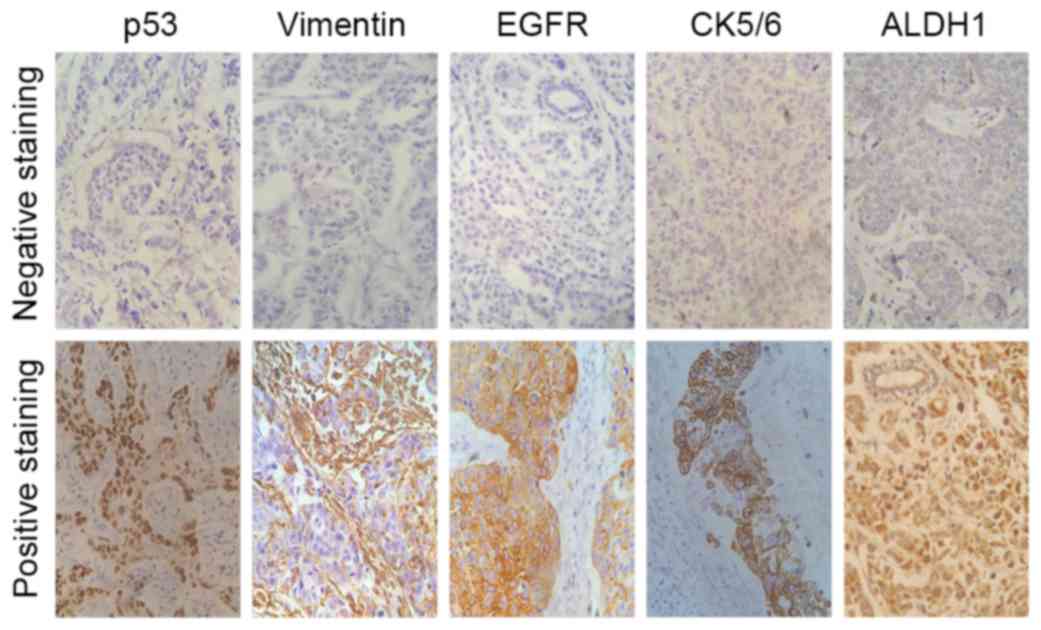
Immunohistochemical expression of the
biomarkers
As shown in Table II,
92.4% of cases exhibited a Ki-67 proliferative index >0%, of
which 26.9% exhibited an index of 1–10%, 24.8% an index of 11–50%
and 40.7% an index of 51–100%. The p53 and BRCA1 mutation carriers
accounted for 37.2 and 24.1%, respectively. Immunophenotyping
showed that AR was expressed in 11.7% (17/145) of the tumors, and
vimentin in 44.1% (64/145). In this group, EGFR and CK5/6
expression was observed in 15.2 and 31.7% of 145 TNBCs,
respectively. In addition, 57 tumors (39.3%) were classified as
basal-like subtype, and 52 tumors (35.9%) were grade 3+ for ALDH1
staining (Fig. 1).
| Table II.Overview of the biomarkers of
triple-negative breast cancer. |
Table II.
Overview of the biomarkers of
triple-negative breast cancer.
|
Characteristics | Patients, n
(%) |
|---|
| Ki-67 expression,
% |
|
| 0 | 11 (7.6) |
|
1–10 | 39 (26.9) |
|
11–50 | 36 (24.8) |
|
51–100 | 59 (40.7) |
| p53 |
|
|
Negative | 91 (62.8) |
|
Positive | 54 (37.2) |
| Androgen
receptor |
|
|
Negative | 128 (88.3) |
|
Positive | 17 (11.7) |
| Vimentin |
|
|
Negative | 81 (55.9) |
|
Positive | 64 (44.1) |
| Breast cancer
susceptibility gene 1 |
|
|
Negative | 110 (75.9) |
|
Positive | 35 (24.1) |
| EGFR |
|
|
Negative | 123 (84.8) |
|
Positive | 22 (15.2) |
| CK5/6 |
|
|
Negative | 99 (68.3) |
|
Positive | 46 (31.7) |
| Basal-like |
|
| EGFR
and CK5/6 negative | 88 (60.7) |
| EGFR or
CK5/6 positive | 57 (39.3) |
| Aldehyde
dehydrogenase 1 |
|
| Grade
0 | 45 (31.0) |
| Grade
1+ | 20 (13.8) |
| Grade
2+ | 28 (19.3) |
| Grade
3+ | 52 (35.9) |
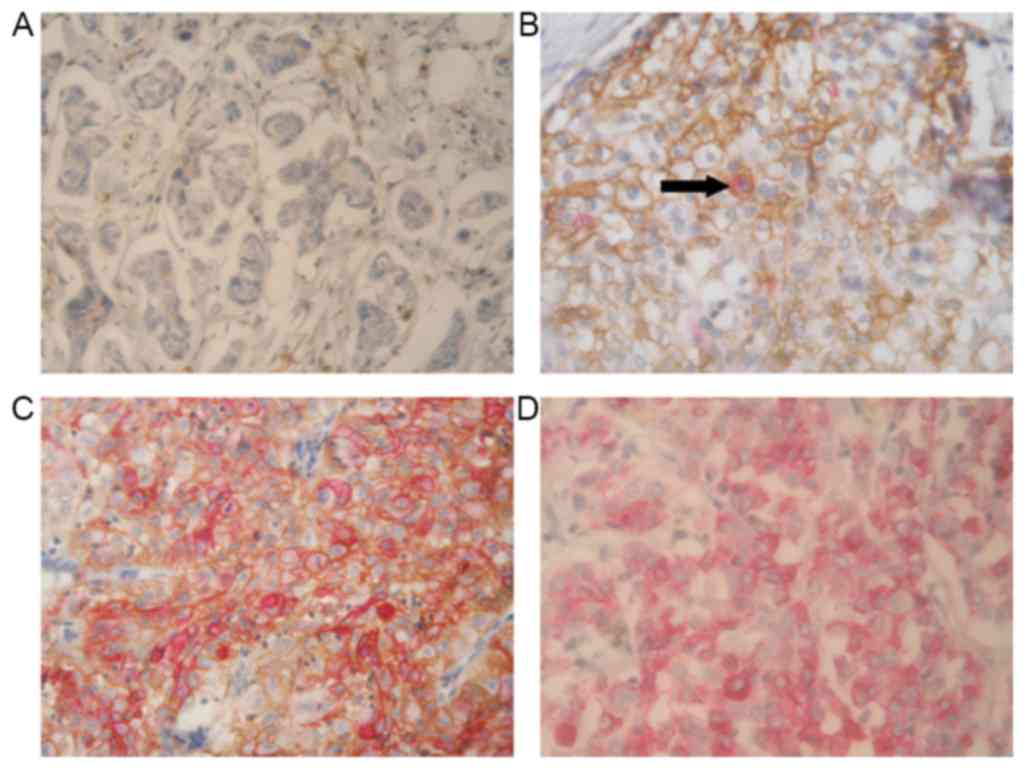
Immunohistochemical expression of CD44
and CD24
The presence of CD44 and CD24 antigens was analyzed
in human breast cancer tissues using double-staining
immunohistochemistry. The CD44 and CD24 expression was successfully
determined in 145 cases. Fig. 2 shows
representative staining patterns of various breast tumors. CD44 was
identified as brown mainly in the membranous staining and CD24 was
identified as red mainly in the cytoplasmic and membranous
staining. In addition, to investigate the association between
CD44/CD24 status and patient survival, tumors were classified
according to the percentage of cells with different CD44 and CD24
expression, which resulted in four phenotypic groups:
CD44−/CD24− (43.4%; 63/145),
CD44+/CD24− (30.3%; 44/145),
CD44+/CD24+ (3.4%; 5/145) and
CD44−/CD24+ (22.8%; 33/145) (Table III). According to the
classification, it was inferred that the
CD44−/CD24− and
CD44+/CD24− phenotypes accounted for the
majority of TNBC cases. In the survival analyses, patients with the
CD44+/CD24− phenotype had a significantly
worse prognosis (P=0.005).
| Table III.Number and percentage of the
different CD44/CD24 phenotypes. |
Table III.
Number and percentage of the
different CD44/CD24 phenotypes.
|
Characteristics | Patients, n
(%) |
|---|
| CD44/CD24
status |
|
|
CD44−/CD24− | 63 (43.4) |
|
CD44+/CD24− | 44 (30.3) |
|
CD44+/CD24+ | 5 (3.4) |
|
CD44−/CD24+ | 33 (22.8) |
Association between CD44/CD24
phenotypes and other clinical characteristics
The distribution of different CD44/CD24 phenotypes
(CD44−/CD24−,
CD44+/CD24−,
CD44+/CD24+ and
CD44−/CD24+) was calculated in Table IV. The χ2 test identified
the following factors to be associated with CD44/CD24 status:
Pathology, AR status and vimentin. All four phenotypes appeared to
be mainly invasive ductal carcinoma. In addition, the
CD44−/CD24− phenotype contained a comparable
amount of invasive lobular carcinoma (P=0.011). The
CD44+/CD24− phenotype exhibited increased AR
expression (25%) compared with the other three groups (P=0.022).
CD44−/CD24+ tumors mostly expressed vimentin
protein (75.8%; P<0.0001). In addition,
CD44+/CD24− cases were more commonly scored
as ALDH1 staining grade 3+ tumors when compared with
CD44−/CD24+ cases, however, this difference
was not statistically significant (50.0 vs. 30.3%, respectively;
P=0.378).
| Table IV.Correlation of CD44/CD24 status with
pathology, androgen receptor and vimentin. |
Table IV.
Correlation of CD44/CD24 status with
pathology, androgen receptor and vimentin.
|
| CD44/CD24 status, n
(%) |
|
|---|
|
|
|
|
|---|
|
Characteristics |
CD44−/CD24− |
CD44+/CD24− |
CD44+/CD24+ |
CD44−/CD24+ | P-value |
|---|
| Pathology |
|
|
|
| 0.011 |
|
Intraductal carcinoma | 0 (0.0) | 4 (9.1) | 0 (0.0) | 0 (0.0) |
|
|
Invasive ductal carcinoma | 61 (96.8) | 37 (84.1) | 4 (80.0) | 30 (90.9) |
|
|
Invasive lobular
carcinoma | 2 (3.2) | 1 (2.3) | 1 (20.0) | 0 (0.0) |
|
| Other
types | 0 (0.0) | 2 (4.5) | 0 (0.0) | 3 (9.1) |
|
| Androgen
receptor |
|
|
|
| 0.022 |
|
Negative | 59 (93.7) | 33 (75.0) | 5 (100.0) | 31 (93.9) |
|
|
Positive | 4 (6.3) | 11 (25.0) | 0 (0.0) | 2 (6.1) |
|
| Vimentin |
|
|
|
| 0.000 |
|
Negative | 38 (60.3) | 32 (72.7) | 3 (60.0) | 8 (24.2) |
|
|
Positive | 25 (39.7) | 12 (27.3) | 2 (40.0) | 25 (75.8) |
|
| Aldehyde
dehydrogenase 1 |
|
|
|
| 0.378 |
| Grade
0 | 23 (36.5) | 8 (18.2) | 2 (40.0) | 12 (36.4) |
|
| Grade
1+ | 7 (11.1) | 6 (13.6) | 1 (20.0) | 6 (18.2) |
|
| Grade
2+ | 14 (22.2) | 8 (18.2) | 1 (20.0) | 5 (15.2) |
|
| Grade
3+ | 19 (30.2) | 22 (50.0) | 1 (20.0) | 10 (30.3) |
|
DFS analysis
For the prognostic evaluations, adjusted
multivariable Cox regression analyses were performed and listed in
Table V. In the analysis of CD44/CD24
status, patients with the CD44+/CD24− subtype
possessed a slightly increased risk of recurrence or metastasis
compared with patients with CD44−/CD24−
phenotype, adjusting for confounders. The estimated HR for
CD44+/CD24− subtype in CD44/CD24 status was
2.38 (95% CI, 0.90–6.33; P=0.081). No association was observed
between the CD44+/CD24+ phenotype and DFS,
nor between CD44−/CD24+ status and DFS, with
estimated HRs being 0.38 (95% CI, 0.03–4.44; P=0.438) and 0.59 (95%
CI, 0.18–1.98; P=0.393), respectively.
| Table V.Multivariate cox-regression analyses
of prognosis factors with DFS and OS. |
Table V.
Multivariate cox-regression analyses
of prognosis factors with DFS and OS.
|
| DFS | OS |
|---|
|
|
|
|
|---|
| Prognosis
factors | HR | 95% CI |
P-valuea | HR | 95% CI |
P-valuea |
|---|
| Number of lymph
nodes involved |
|
|
|
|
|
|
| 0 | 1.00 |
|
| 1.00 |
|
|
|
1–3 | 0.96 | 0.28–3.27 | 0.949 | 1.75 | 0.54–5.71 | 0.353 |
| ≥4 | 5.79 | 1.73–19.32 | 0.004 | 12.90 | 3.57–46.59 | 0.000 |
| Chemotherapy |
|
|
|
|
|
|
| No
chemotherapy | 1.00 |
|
| 1.00 |
|
|
|
Derivative regimens of
CAF | 6.00 | 1.26–28.46 | 0.024 | 1.36 | 0.31–5.92 | 0.681 |
| (CAF, CEF, CTF or
IEF) |
|
|
|
|
|
|
|
Regimens including
taxanes | 11.11 | 2.61–47.39 | 0.001 | 1.84 | 0.54–6.20 | 0.328 |
| (TE, TC or
TAC) |
|
|
|
|
|
|
| Other
regimens | 2.18 | 0.46–10.44 | 0.329 | 0.28 | 0.05–1.64 | 0.158 |
| Vimentin |
|
|
|
|
|
|
|
Negative | 1.00 |
|
| 1.00 |
|
|
|
Positive | 4.15 | 1.53–11.28 | 0.005 | 2.88 | 0.96–8.61 | 0.059 |
| Basal-like |
|
|
|
|
|
|
| EGFR
and CK5/6 negative | 1.00 |
|
| 1.00 |
|
|
| EGFR or
CK5/6 positive | 1.96 | 0.78–4.93 | 0.151 | 3.17 | 1.28–7.82 | 0.013 |
| Aldehyde
dehydrogenase 1 |
|
|
|
|
|
|
| Grade
0 | 1.00 |
|
| 1.00 |
|
|
| Grade
1+ | 0.61 | 0.14–2.58 | 0.605 | 0.57 | 0.11–2.87 | 0.492 |
| Grade
2+ | 0.33 | 0.09–1.23 | 0.329 | 0.44 | 0.10–1.94 | 0.279 |
| Grade
3+ | 1.30 | 0.42–4.06 | 1.298 | 1.40 | 0.44–4.43 | 0.571 |
| CD44/CD24
status |
|
|
|
|
|
|
|
CD44−/CD24− | 1.00 |
|
| 1.00 |
|
|
|
CD44+/CD24− | 2.38 | 0.90–6.33 | 0.081 | 4.38 | 1.57–12.18 | 0.005 |
|
CD44+/CD24+ | 0.38 | 0.03–4.44 | 0.438 | 0.89 | 0.09–8.99 | 0.920 |
|
CD44−/CD24+ | 0.59 | 0.18–1.98 | 0.393 | 1.24 | 0.38–4.01 | 0.722 |
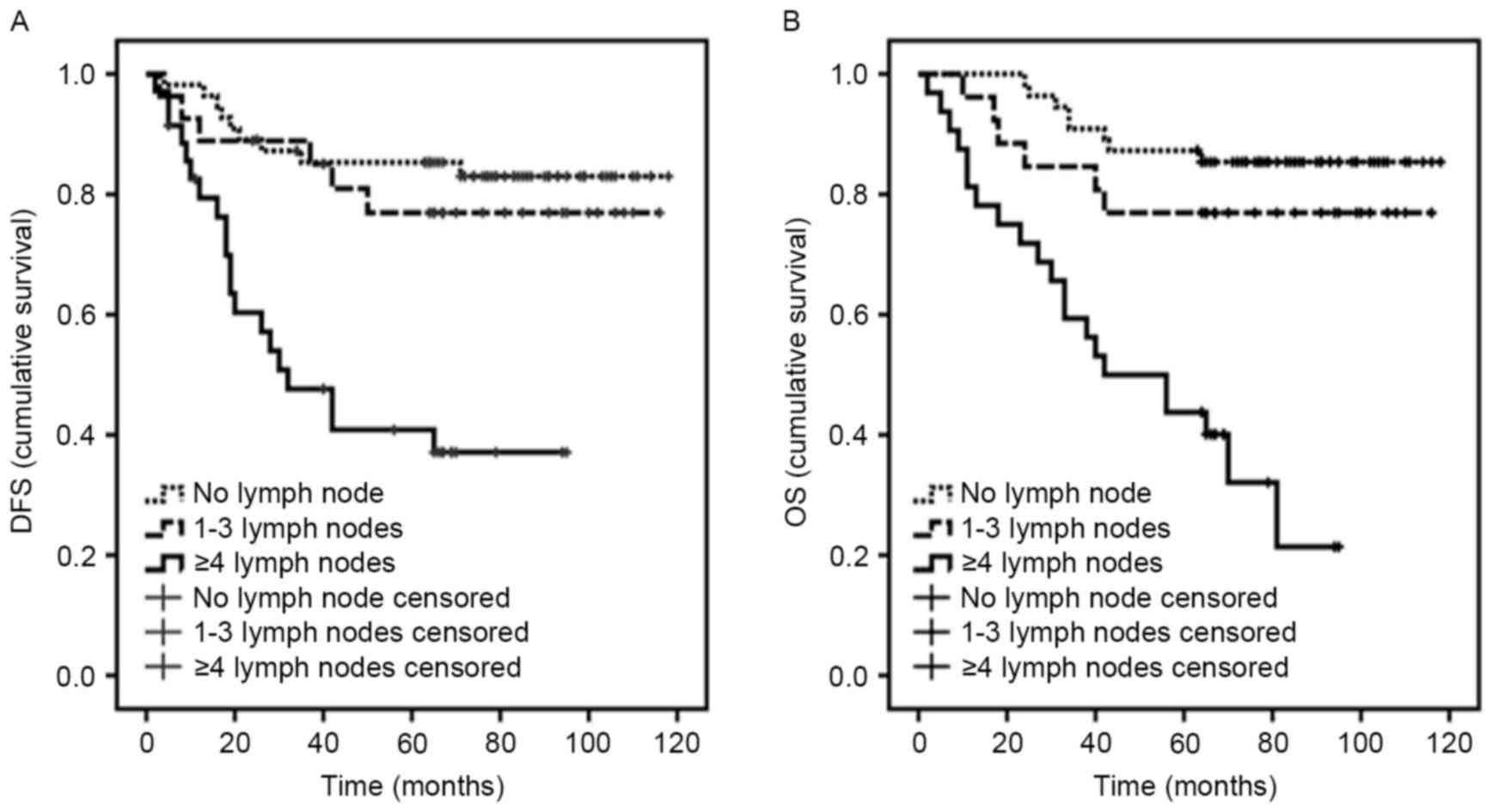
Notably, lymph node metastasis was associated with
DFS in multivariable analysis (P=0.004; Fig. 3A). In the cohort, it was observed that
patients with derivative regimens of CAF had a poor prognosis
(P=0.024), while regimens including taxanes were associated with a
shorter DFS time (P=0.001). Subsequently, additional analyses of
data revealed that the majority of patients with ≥4 lymph nodes
received regimens including taxanes. In addition, it was observed
that patients with vimentin-positive tumors had a poor prognosis
(P=0.005).
No significant associations were observed between
DFS and tumor size, pathology, radiotherapy, Ki-67, p53, AR, BRCA1,
basal-like or ALDH1.
OS analysis
The number of lymph nodes involved was strongly
associated with OS in multivariable analyses, with an estimated HR
for ≥4 lymph nodes of 12.90 (P<0.0001; Fig. 3B).
The roles of CD44/CD24 status and ALDH1 were
assessed using multivariable Cox regression analyses in OS
(Table V). Notably, for patients with
a CD44+/CD24− phenotype, risk of mortality
was statistically significantly increased compared with patients
with CD44−/CD24− phenotype (P=0.005; Fig. 4A). The estimated HR for
CD44+/CD24− subtype in CD44/CD24 status was
4.38 (95% CI, 1.57–12.18). Furthermore, no association was observed
between CD44+/CD24+ phenotype and OS, with
the estimated HR being 0.89 (95% CI, 0.09–8.99; P=0.920). Although
the HR was increased for the CD44−/CD24+
phenotype compared with the CD44−/CD24−
subtype, this difference was not statistically significant (HR,
1.24; 95% CI, 0.38–4.01; P=0.722). In this adjusted multivariable
analysis, no significant association was observed between ALDH1 and
OS in the TNBC cohort. However, the Kaplan-Meier curves of
different levels of ALDH1 did separate and the survival of patients
with ALDH1 grade 3+ was inferior to those of patients with grade 0,
1+ or 2+ (P=0.571; Fig. 4B). In
general, ALDH1 overexpression could be a disadvantage for the
survival of patients.
In addition, there was a trend toward an inferior OS
for patients with basal-like tumors vs. non-basal-like tumors
(P=0.013; Fig. 4C) (Table V). Similarly, no significant
difference was observed between OS and clinical characteristics,
including tumor size, pathology, radiotherapy, chemotherapy, Ki-67,
p53, AR, vimentin or BRCA1.
Discussion
Breast carcinoma is recognized as a heterogeneous
disease and presents with distinct histopathological features and
clinical behaviors, and a variety of outcomes (22). TNBC is a unique type of breast cancer
with a poor prognosis (2). Cancer
stem cells are more abundant in TNBC tumor tissues and perform
important roles in the recurrence and metastasis of TNBC (6,14).
Although several studies have shown that large percentages of
CD44+/CD24− cells or ALDH1+ cells
remain in TNBC (18,23–25), the
importance of the role of these cancer stem cell subpopulations
with regard to the prognosis of patients has not been clearly
understood. The present study investigated the association between
CD44/CD24 phenotypes and the ALDH1 expression and survival of
patients with TNBC following surgical therapy.
Previously, a number of studies (13,26)
demonstrated that the expression of TNBC antigens, including C-X-C
chemokine receptor type 4 and octamer-binding transcription factor
4, are most prevalent in CD44+/CD24− cells,
and may promote the epithelial-mesenchymal transition of the
CD44+/CD24− phenotype, facilitating breast
cancer recurrence or metastasis. In addition, breast cancer cell
lines with a prevalence of CD44+/CD24− cells
have a higher potential than others to invade Matrigel in
vitro and a high metastatic ability in vivo in the lymph
node microenvironment and in distant metastasis (27). Furthermore, in a cohort of 50 patients
with TNBC, Idowu et al (24)
reported that the tumor tissues with
CD44+/CD24− were more likely to have a high
Ki-67 proliferation index and be associated with a poor clinical
outcome. Other breast cancer specimens in which single staining
detected the expression of CD44 and CD24, it was clarified that the
tumor tissues with the CD44+/CD24− subtype
had a higher median vascular density compared with that in those
tissues with the CD44−/CD24− phenotype; OS
analysis of this study showed that patients with the
CD44+/CD24− phenotype may have an unfavorable
prognosis (23).
In the present study, the expression of CD24 and
CD44 was examined using immunohistochemical double-staining.
Results certified that the double-staining pattern did not
interfere with the accurate expression of CD44 and CD24, and it
could also locate cells with different expression profiles
individually. The percentages of four types of cancer cells
(CD44−/CD24−,
CD44+/CD24−,
CD44+/CD24+ and
CD44−/CD24+) in tumors were counted following
double-staining immunohistochemistry, and each tumor was defined by
the presence of the predominant cell type. No association was
observed between DFS and the CD44+/CD24−
phenotype, however, OS analysis showed that patients with the
CD44+/CD24− phenotype experienced a
significantly shorter survival time compared with patients with
other phenotypes. The CD44+/CD24− cell
population has been associated with a poor prognosis (28), although not in all relevant studies.
In a similar study (29), Ezrin and
CD44 protein co-expression, which was detected with
immunofluorescence double-staining, was shown to be associated with
a poor disease-specific survival time in 726 breast cancer
patients. In addition, according to the present data from
Kaplan-Meier curves of estimated DFS and OS, the
CD44−/CD24+ phenotype in TNBC may also be
associated with a trend for an increased risk of recurrence or
mortality when compared with the CD44−/CD24−
phenotype, although this did not reach statistical significance. A
previous study from Ahmed et al (30) demonstrated that the
CD44−/CD24+ phenotype was significantly
associated with shorter metastasis-free survival time and decreased
10-year breast cancer survival rate. In the study by Mylona et
al (31), the
CD44−/CD24+ phenotype emerged as a poor
prognostic indicator, at least within the group of grade 2
tumors.
Furthermore, ALDH1 is another key cell surface
marker isolating the cancer stem cell subpopulation.
Charafe-Jauffret et al (32)
found that the aggressive and metastatic behaviors of inflammatory
breast cancer are mediated by ALDH1+ breast cancer stem
cells in mouse xenograft models. In another study involving 577
breast carcinomas, the expression of ALDH1, as defined by
immunohistochemistry staining, was significantly associated with a
poor clinical outcome (9). In the
present study, DFS and OS analyses showed that the survival curve
of ALDH1 grade 3+ was inferior to those of grade 0, 1+ or 2+,
although the analysis did not reach statistical significance.
In our OS analyses, patients with a basal-like
subtype have been more likely to experience shorter OS times. The
basal-like breast cancer, which is mostly comprised of TNBCs, is
positive for CK5/6 and/or EGFR, and is particularly common in BRCA1
hereditary tumors (17). Moestue
et al (33) observed that
basal-like xenografts exhibited significantly higher
phosphatidylinositol 3-kinase pathway activity than luminal-like
xenografts in animal models of breast cancer; i.e., basal-like
tumors exhibited worse prognoses compared with luminal-like
tumors.
In the present cohort, the involvement of ≥4 lymph
nodes has been associated with an increased risk of recurrence and
mortality in patients with TNBC. In a cohort of 1,711 patients with
the TNBC subtype, Hernandez-Aya et al (16) found that when comparing node-negative
and node-positive patients, there was a significant difference in
relapse-free survival.
In summary, the present study reported that the
CD44/CD24 phenotype evaluated by double staining
immunohistochemistry constitutes an independent prognostic factor
for TNBC. Patients with TNBC with the
CD44+/CD24− phenotype exhibit a significantly
worse prognosis. Additional studies are required to investigate the
molecular mechanism of the aggressive behaviors of cancer stem
cells and guide clinical treatment for TNBC.
Acknowledgements
The authors are grateful for the excellent technical
assistance of the pathologists in the Cancer Hospital of Harbin
Medical University and for the assistance provided for the
collection of follow-up data by the staff in the Department of
Records. The study was supported by the National Natural Science
Foundation of China (grant no. 81270034), the Chunhui Program from
Chinese Ministry of Education (grant no. Z2012075) and the Yuweihan
Academician Prominent Youth Foundation from Harbin Medical
University (grant no. 2011-2013).
Glossary
Abbreviations
Abbreviations:
|
TNBC
|
triple-negative breast cancer
|
|
ER
|
estrogen receptor
|
|
PR
|
progesterone receptor
|
|
HER2
|
human epidermal growth factor receptor
2
|
|
ESA
|
epithelial-specific antigen
|
|
Lin
|
lineage
|
|
ALDH1
|
aldehyde dehydrogenase 1
|
|
CAF
|
cyclophosphamide, adriamycin and
fluorouracil
|
|
CEF
|
cyclophosphamide, epirubicin and
fluorouracil
|
|
CTF
|
cyclophosphamide, pirarubicin and
fluorouracil
|
|
IEF
|
ifosfamide, epirubicin and
fluorouracil
|
|
TE
|
paclitaxel or docetaxel and
epirubicin
|
|
TC
|
docetaxel and cyclophosphamide
|
|
TAC
|
docetaxel, adriamycin and
cyclophosphamide
|
|
DFS
|
disease-free survival
|
|
OS
|
overall survival
|
|
AR
|
androgen receptor
|
|
BRCA1
|
breast cancer susceptibility gene
1
|
|
CK5/6
|
cytokeratin5/6
|
|
EGFR
|
epidermal growth factor receptor
|
|
HR
|
hazard ratio
|
References
|
1
|
Sotiriou C and Pusztai L: Gene-expression
signatures in breast cancer. N Engl J Med. 360:790–800. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Bauer KR, Brown M, Cress RD, Parise CA and
Caggiano V: Descriptive analysis of estrogen receptor
(ER)-negative, progesterone receptor (PR)-negative, and
HER2-negative invasive breast cancer, the so-called triple-negative
phenotype: A population-based study from the California Cancer
Registry. Cancer. 109:1721–1728. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Reis-Filho JS and Tutt AN: Triple negative
tumours: A critical review. Histopathology. 52:108–118. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Anders C and Carey LA: Understanding and
treating triple-negative breast cancer. Oncology (Williston Park).
22:1233–1239. 2008.PubMed/NCBI
|
|
5
|
Lee E, McKean-Cowdin R, Ma H, Spicer DV,
Van Den Berg D, Bernstein L and Ursin G: Characteristics of
triple-negative breast cancer in patients with a BRCA1 mutation:
Results from a population-based study of young women. J Clin Oncol.
29:4373–4380. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Reya T, Morrison SJ, Clarke MF and
Weissman IL: Stem cells, cancer, and cancer stem cells. Nature.
414:105–111. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Clarke MF, Dick JE, Dirks PB, Eaves CJ,
Jamieson CH, Jones DL, Visvader J, Weissman IL and Wahl GM: Cancer
stem cells-perspectives on current status and future directions:
AACR workshop on cancer stem cells. Cancer Res. 66:9339–9344. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Al-Hajj M, Wicha MS, Benito-Hernandez A,
Morrison SJ and Clarke MF: Prospective identification of
tumorigenic breast cancer cells. Proc Natl Acad Sci USA.
100:3983–3988. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Ginestier C, Hur MH, Charafe-Jauffret E,
Monville F, Dutcher J, Brown M, Jacquemier J, Viens P, Kleer CG,
Liu S, et al: ALDH1 is a marker of normal and malignant human
mammary stem cells and a predictor of poor clinical outcome. Cell
Stem Cell. 1:555–567. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Zhang J, Niu C, Ye L, Huang H, He X, Tong
WG, Ross J, Haug J, Johnson T, Feng JQ, et al: Identification of
the haematopoietic stem cell niche and control of the niche size.
Nature. 425:836–841. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Patrawala L, Calhoun T,
Schneider-Broussard R, Zhou J, Claypool K and Tang DG: Side
population is enriched in tumorigenic, stem-like cancer cells,
whereas ABCG2+ and ABCG2− cancer cells are
similarly tumorigenic. Cancer Res. 65:6207–6219. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Lin L, Hutzen B, Lee HF, Peng Z, Wang W,
Zhao C, Lin HJ, Sun D, Li PK, Li C, et al: Evaluation of STAT3
signaling in ALDH+ and
ALDH+/CD44+/CD24− subpopulations
of breast cancer cells. PLoS One. 8:e828212013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Honeth G, Bendahl PO, Ringnér M, Saal LH,
Gruvberger-Saal SK, Lövgren K, Grabau D, Fernö M, Borg A and
Hegardt C: The CD44+/CD24− phenotype is
enriched in basal-like breast tumors. Breast Cancer Res.
10:R532008. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ricardo S, Vieira AF, Gerhard R, Leitão D,
Pinto R, Cameselle-Teijeiro JF, Milanezi F, Schmitt F and Paredes
J: Breast cancer stem cell markers CD44, CD24 and ALDH1: Expression
distribution within intrinsic molecular subtype. J Clin Pathol.
64:937–946. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Sinn HP, Helmchen B and Wittekind CH: TNM
classification of breast cancer: Changes and comments on the 7th
edition. Pathologe. 31:361–366. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Hernandez-Aya LF, Chavez-Macgregor M, Lei
X, Meric-Bernstam F, Buchholz TA, Hsu L, Sahin AA, Do KA, Valero V,
Hortobagyi GN and Gonzalez-Angulo AM: Nodal status and clinical
outcomes in a large cohort of patients with triple-negative breast
cancer. J Clin Oncol. 29:2628–2634. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Nielsen TO, Hsu FD, Jensen K, Cheang M,
Karaca G, Hu Z, Hernandez-Boussard T, Livasy C, Cowan D, Dressler
L, et al: Immunohistochemical and clinical characterization of the
basal-like subtype of invasive breast carcinoma. Clin Cancer Res.
10:5367–5374. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Resetkova E, Reis-Filho JS, Jain RK, Mehta
R, Thorat MA, Nakshatri H and Badve S: Prognostic impact of ALDH1
in breast cancer: A story of stem cells and tumor microenvironment.
Breast Cancer Res Treat. 123:97–108. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Abdel-Fatah TM, Arora A, Alsubhi N,
Agarwal D, Moseley PM, Perry C, Doherty R, Chan SY, Green AR, Rakha
E, et al: Clinicopathological significance of ATM-Chk2 expression
in sporadic breast cancers: A comprehensive analysis in large
cohorts. Neoplasia. 16:982–991. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Lee JG and Wu R: Erlotinib-cisplatin
combination inhibits growth and angiogenesis through c-MYC and
HIF-1α in EGFR-mutated lung cancer in vitro and in vivo. Neoplasia.
17:190–200. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Bane A, Viloria-Petit A, Pinnaduwage D,
Mulligan AM, O'Malley FP and Andrulis IL: Clinical-pathologic
significance of cancer stem cell marker expression in familial
breast cancers. Breast Cancer Res Treat. 140:195–205. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Jacquemier J, Ginestier C, Rougemont J,
Bardou VJ, Charafe-Jauffret E, Geneix J, Adélaïde J, Koki A,
Houvenaeghel G, Hassoun J, et al: Protein expression profiling
identifies subclasses of breast cancer and predicts prognosis.
Cancer Res. 65:767–779. 2005.PubMed/NCBI
|
|
23
|
Giatromanolaki A, Sivridis E, Fiska A and
Koukourakis MI: The CD44+/CD24− phenotype
relates to ‘triple-negative’ state and unfavorable prognosis in
breast cancer patients. Med Oncol. 28:745–752. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Idowu MO, Kmieciak M, Dumur C, Burton RS,
Grimes MM, Powers CN and Manjili MH: CD44(+)/CD24(−/low) cancer
stem/progenitor cells are more abundant in triple-negative invasive
breast carcinoma phenotype and are associated with poor outcome.
Hum Pathol. 43:364–373. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Nalwoga H, Arnes JB, Wabinga H and Akslen
LA: Expression of aldehyde dehydrogenase 1 (ALDH1) is associated
with basal-like markers and features of aggressive tumours in
African breast cancer. Br J Cancer. 102:369–375. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Wang D, Lu P, Zhang H, Luo M, Zhang X, Wei
X, Gao J, Zhao Z and Liu C: Oct-4 and Nanog promote the
epithelial-mesenchymal transition of breast cancer stem cells and
are associated with poor prognosis in breast cancer patients.
Oncotarget. 5:10803–10815. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Pandit TS, Kennette W, Mackenzie L, Zhang
G, Al-Katib W, Andrews J, Vantyghem SA, Ormond DG, Allan AL,
Rodenhiser DI, et al: Lymphatic metastasis of breast cancer cells
is associated with differential gene expression profiles that
predict cancer stem cell-like properties and the ability to
survive, establish and grow in a foreign environment. Int J Oncol.
35:297–308. 2009.PubMed/NCBI
|
|
28
|
Meyer MJ, Fleming JM, Ali MA, Pesesky MW,
Ginsburg E and Vonderhaar BK: Dynamic regulation of CD24 and the
invasive, CD44posCD24neg phenotype in breast cancer cell lines.
Breast Cancer Res. 11:R822009. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Ma L and Jiang T: Clinical implications of
Ezrin and CD44 co-expression in breast cancer. Oncol Rep.
30:1899–1905. 2013.PubMed/NCBI
|
|
30
|
Ahmed MA, Aleskandarany MA, Rakha EA,
Moustafa RZ, Benhasouna A, Nolan C, Green AR, Ilyas M and Ellis IO:
A CD44−/CD24+ phenotype is a poor prognostic
marker in early invasive breast cancer. Breast Cancer Res Treat.
133:979–995. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Mylona E, Giannopoulou I, Fasomytakis E,
Nomikos A, Magkou C, Bakarakos P and Nakopoulou L: The
clinicopathologic and prognostic significance of
CD44+/CD24 (−/low) and CD44−/CD24+
tumor cells in invasive breast carcinomas. Hum Pathol.
39:1096–1102. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Charafe-Jauffret E, Ginestier C, Iovino F,
Tarpin C, Diebel M, Esterni B, Houvenaeghel G, Extra JM, Bertucci
F, Jacquemier J, et al: Aldehyde dehydrogenase 1-positive cancer
stem cells mediate metastasis and poor clinical outcome in
inflammatory breast cancer. Clin Cancer Res. 16:45–55. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Moestue SA, Dam CG, Gorad SS, Kristian A,
Bofin A, Mælandsmo GM, Engebråten O, Gribbestad IS and Bjørkøy G:
Metabolic biomarkers for response to PI3K inhibition in basal-like
breast cancer. Breast Cancer Res. 15:R162013. View Article : Google Scholar : PubMed/NCBI
|