Introduction
Epithelial ovarian cancer (EOC) is one of the three
most common malignant tumors of the female reproductive system
(1). Owing to the lack of early
diagnosis modalities and effective treatment measures, >70% of
the patients are diagnosed at an advanced disease stage, and this
is associated with high rates of morbidity and mortality (2). At present, the standard therapy for
advanced ovarian cancer usually includes primary surgical
cytoreduction and chemotherapy (3,4). The
two-drug combination of paclitaxel and carboplatin (CBP) is
considered the standard first-line chemotherapy for patients with
EOC (5). Although this standard
chemotherapy initially yields a high response rate (>80%),
>70% of women with advanced-stage EOC experience recurrence
within 5 years and develop drug resistance (2,6). This
regimen has been associated with serious adverse effects including
myelosuppression, alopecia, neurotoxicity and fatigue, which affect
the tolerance of patients to the therapy, and their quality of
life. Therefore, it is necessary to search for chemotherapy
regimens with superior safety and efficacy for the treatment of
EOC.
Nedaplatin, namely 254-S, NDP (cisplatin analogue),
is a second-generation platinum derivative developed by Shionogi
& Co., Ltd. (Osaka, Japan). Experiments in vitro
demonstrated that NDP inhibited tumor cell proliferation in human
cervical and ovarian cancer (7,8). In
vivo, NDP exhibited an antitumor effect in tumor-bearing
animals (9,10). Results of phase II studies in Japan
revealed that NDP exerted pronounced antitumor activity against
various solid tumors, including lung, esophageal, head and neck,
testicular, and cervical cancer, and ovarian carcinoma (11–16).
Response rates of at least 25% have been achieved with 100
mg/m2 NDP monotherapy in a range of different types of
cancer (17). The response rate to
NDP monotherapy was 38 and 34–46% in ovarian and cervical cancer,
respectively (11,13). Furthermore, NDP has been reported to
exhibit higher antitumor activity in cervical cancer compared with
CBP (18,19).
On the basis of the above results, a multi-center,
randomized, open-label phase III trial was designed to compare the
clinical outcomes of NDP plus paclitaxel and CBP plus paclitaxel in
the treatment of epithelial ovarian cancer. The trial was designed
to test whether the efficacy and tolerability of NDP was maintained
in combination with paclitaxel. The endpoints, including
progression-free survival (PFS), overall survival (OS), and
toxicity profiles, were compared between the two groups to provide
further evidence for the clinical application of NDP.
Patients and methods
Patients
A total of 182 patients with epithelial ovarian
cancer [International Federation of Gynecology and Obstetrics
(FIGO) stage II–IV] (20) were
enrolled between August 2010 and April 2012 at 14 centers (Cancer
Hospital of Guangxi Medical University, Nanning; Tongji Hospital,
Shanghai; West China Second University Hospital, Chengdu; Shanghai
General Hospital, Shanghai; Peking University First Hospital,
Beijing; Women's Hospital School of Medicine Zhejiang University,
Hangzhou; Qilu Hospital of Shandong University, Jinan; Daping
Hospital, Research Institute of Surgery Third Military Medical
University, Chongqing; Jiangsu Cancer Hospital, Nanjing; The First
Affiliated Hospital of Haerbin Medical University, Haerbin;
Chongqing Cancer Hospital, Chongqing; Cancer Hospital Chinese
Academy of Medical Science, Beijing; The Second Affiliated Hospital
of Tsinghua University, Beijing; Peking University People's
Hospital, Beijing), in China. Clinicopathological characteristics
are presented in Table I. A
computer-based minimization procedure was used to randomly allocate
participants at a 1:1 ratio to either the standard schedule of CBP
plus paclitaxel or the experimental schedule of NDP plus
paclitaxel. The procedure of centralized randomization was
conducted by the Department of Biostatistics, Nanjing Medical
University (Nanjing, China). The ethics committee of each
participating center approved the study protocol. Written informed
consent was obtained from every participant prior to enrolment and
randomization. The main inclusion criteria were as follows: i)
Patients had pathologically or cytologically confirmed epithelial
ovarian cancer [The International Federation of Gynecology and
Obstetrics (FIGO) stage II–IV] followed by optimal cytoreductive
surgery; ii) patients were aged between 18 and 70 years old; and
iii) patients exhibited adequate hematological, renal, and hepatic
function. In addition, all included patients had no other serious
medical problems, and no intracranial or bone metastases. Good
adherence, regular follow-up and voluntary compliance with the
provisions of this research were required. Patients were excluded
it they failed to complete the planned cycles because of
progressive disease or any other reason. Patients who were pregnant
or lactating were also excluded from the present study. The trial
was registered with the Chinese Clinical Trial Registry (no.
ChiCTR-TRC-11001333).
 | Table I.Patient characteristics. |
Table I.
Patient characteristics.
| Characteristic | NDP group | CBP group | P-value |
|---|
| Age, years |
50.82±9.83a |
50.84±10.30a | 0.98 |
| FIGO stage, n
(%) |
|
|
|
| II | 28 (30.77) | 19 (21.11) | 0.66 |
|
III | 52 (57.14) | 67 (74.44) |
|
| IV | 12 (12.09) | 4 (4.44) |
|
| Treatment status, n
(%) |
|
|
|
| Initial
treatment | 86 (93.48) | 86 (95.56) | 0.75 |
|
Retreatment | 6 (6.52) | 4 (4.44) |
|
| Marital status, n
(%) |
|
|
|
|
Married | 91 (98.91) | 86 (95.56) | 0.21 |
|
Unmarried | 1 (1.09) | 4 (4.44) |
|
| Background disease,
n (%) |
|
|
|
| No | 76 (82.61) | 76 (84.44) | 0.84 |
|
Yes | 16 (17.39) | 14 (15.56) |
|
| Operation, n
(%) |
|
|
|
| No | 42 (45.65) | 42 (46.67) | 1.00 |
|
Yes | 50 (54.35) | 48 (53.33) |
|
| Radiotherapy, n
(%) |
|
|
|
| No | 92 (100.00) | 90 (100.00) | – |
|
Yes | 0 (0.00) | 0 (0.00) |
|
| Chemotherapy, n
(%) |
|
|
|
| No | 73 (79.35) | 71 (78.89) | 1.00 |
|
Yes | 19 (20.65) | 19 (21.11) |
|
| Biotherapy, n
(%) |
|
|
|
| No | 92 (100.00) | 90 (100.00) | – |
|
Yes | 0 (0.00) | 0 (0.00) |
|
| History of drug
allergy, n (%) |
|
|
|
| No | 85 (92.39) | 86 (95.56) | 0.54 |
|
Yes | 7 (7.61) | 4 (4.44) |
|
|
Pathological/cytological patterns, n
(%) |
|
|
|
| Serous
adenocarcinoma | 57 (62.64) | 58 (65.17) | 0.53 |
|
Mucinous adenocarcinoma | 7 (7.69) | 4 (4.49) |
|
|
Clear-cell carcinoma | 7 (7.69) | 3 (3.37) |
|
|
Endometrioid
adenocarcinoma | 7 (7.69) | 11 (12.36) |
|
|
Other | 14 (14.29) | 14 (14.61) |
|
| ECOG score, n
(%) |
|
|
|
| 0 | 69 (75.00) | 60 (66.67) | 0.19 |
| 1 | 23 (25.00) | 28 (31.11) |
|
| 2 | 0 (0.00) | 2 (2.22) |
|
| Treatment cycles, n
(%) |
|
|
|
| 1 | 8 (8.70) | 3 (3.33) | 0.07 |
| 2 | 5 (5.43) | 4 (4.44) |
|
| 3 | 0 (0.00) | 1 (1.11) |
|
| 4 | 10 (10.87) | 8 (8.89) |
|
| 5 | 10 (10.87) | 5 (5.56) |
|
| 6 | 59 (64.13) | 69 (76.67) |
|
Therapeutic regimens
All drugs were obtained from Jiangsu Aosaikang
Pharmaceutical Co., Ltd. (Nanjing, China). Patients assigned to the
experimental group (NDP group) received paclitaxel (175
mg/m2) plus NDP (80 mg/m2) whereas patients
in the control group (CBP group) received paclitaxel (175
mg/m2) plus CBP [area under the curve (AUC) 5 mg/ml per
min according to the Calvert formula] (21). Creatinine clearance was estimated
according to the Cockcroft-Gault formula (22). The treatment was administered once
every 3 weeks for a total of six cycles. NDP was dissolved in 500
ml of normal saline prior to use and infused over 2 h. To avoid
kidney damage, particularly in patients producing <1,500 ml
urine per 24-h, >1,000 ml intravenous infusion of paclitaxel (80
mg/m2) plus NDP (80 mg/m2) was administered
following administration of NDP. Paclitaxel was diluted in 500 ml
5% glucose diluted in hydrochloric acid water prior to intravenous
drip administration for at least 3 h. To prevent
paclitaxel-associated allergic reactions, the patients were orally
pre-medicated with 10 mg dexamethasone 12 h prior to paclitaxel
infusion and 30 min prior to paclitaxel infusion with 10 mg
dexamethasone by intravenous injection, 400 mg diphenhydramine by
intravenous infusion and 20 mg cimetidine by intramuscular
injection. CBP was infused intravenously in 500 ml 5% glucose
diluted in hydrochloric acid water over 2 h. To assess the risk of
acute toxic effects, hematological measurements were performed at
every administration of chemotherapy. An absolute neutrophil count
of >1.5×109 cells/l, a white blood cell count of
>3.0×109 cells/l and a platelet count of
>100×109 cells/l at the beginning of treatment were
required for patients; otherwise, treatment was delayed until the
required hematological counts were achieved. Treatment delay was
permitted because pronounced toxic effects in patients require a
treatment discontinuation of 2 weeks or longer. In the two study
groups, the doses of all drugs were reduced by 20% if the
neutrophil count fell to <0.5×109 cells/l or platelet
count to <50×109 cells/l for 7 days or longer. The
drug doses were reduced by 25% if grade 2 neuropathy arose.
Chemotherapy was continued until unacceptable toxicity was
observed, or the patient refused further treatment.
Evaluation indicators and statistical
analysis
The primary objective of the present study was to
compare PFS and OS between the two treatment groups. Secondary
endpoints were toxicity profiles. PFS was defined as the interval
between the first day of randomization and date of first relapse,
progression or death (whichever occurred first) or the date of the
last follow-up for patients alive at the end of the study without
progression. Surviving patients or patients lost to follow-up were
censored at the date last known to be alive. Descriptive data were
presented as frequencies and percentages. Patient characteristics
in the two groups were compared using Pearson's χ2 test.
Differences in OS and PFS were calculated using Kaplan-Meier curves
and compared using the log-rank test. All P-values were two-tailed
and P<0.05 was considered to indicate a statistically
significant difference. All analyses were conducted by independent
third-party statisticians from the Department of Biostatistics,
Nanjing Medical University, using SPSS 19.0 software (IBM Corp,
Armonk, NY, USA).
Results
Characteristics of patients
The randomized, multi-center, open-label, phase III
trial analyzed 182 patients with EOC between August 2010 and April
2012. Of these patients, 92 received NDP plus paclitaxel regimens
and 90 received CBP plus paclitaxel regimens. The patient
characteristics are presented in Table
I. No statistical difference was observed between the two
groups with regard to age, FIGO stage, initial treatment or
retreatment, marital status, background disease or complications,
history of drug allergies, pathological patterns or Eastern
Cooperative Oncology Group score (23). All enrolled patients received between
1 and 6 cycles of chemotherapy. The chemotherapy duration was
5.02±1.63 [mean ± standard deviation (SD)] cycles in the NDP group
and 5.39±1.30 (mean ± SD) cycles in the CBP group (P=0.07; Table I). A number of patients received
surgery, radiotherapy, chemotherapy, biotherapy or other treatments
prior to the trial, but there was no statistical difference between
the two groups (Table I).
Response to treatment and
survival
In the present study, the date of last the follow-up
was May 20, 2015. A small proportion of the patients (35/182) were
lost to the follow-up due to loss of contact, and their data were
thus excluded from the survival analysis. There was no
statistically significant difference in censoring or lost-to-follow
up status between the two groups (data not shown). The median
follow-up times for the NDP group and CBP group were 44.63 months
[95% confidence interval (CI): 33.67–46.47 months] and 47.63 months
(95% CI: 45.13–49.07 months), respectively.
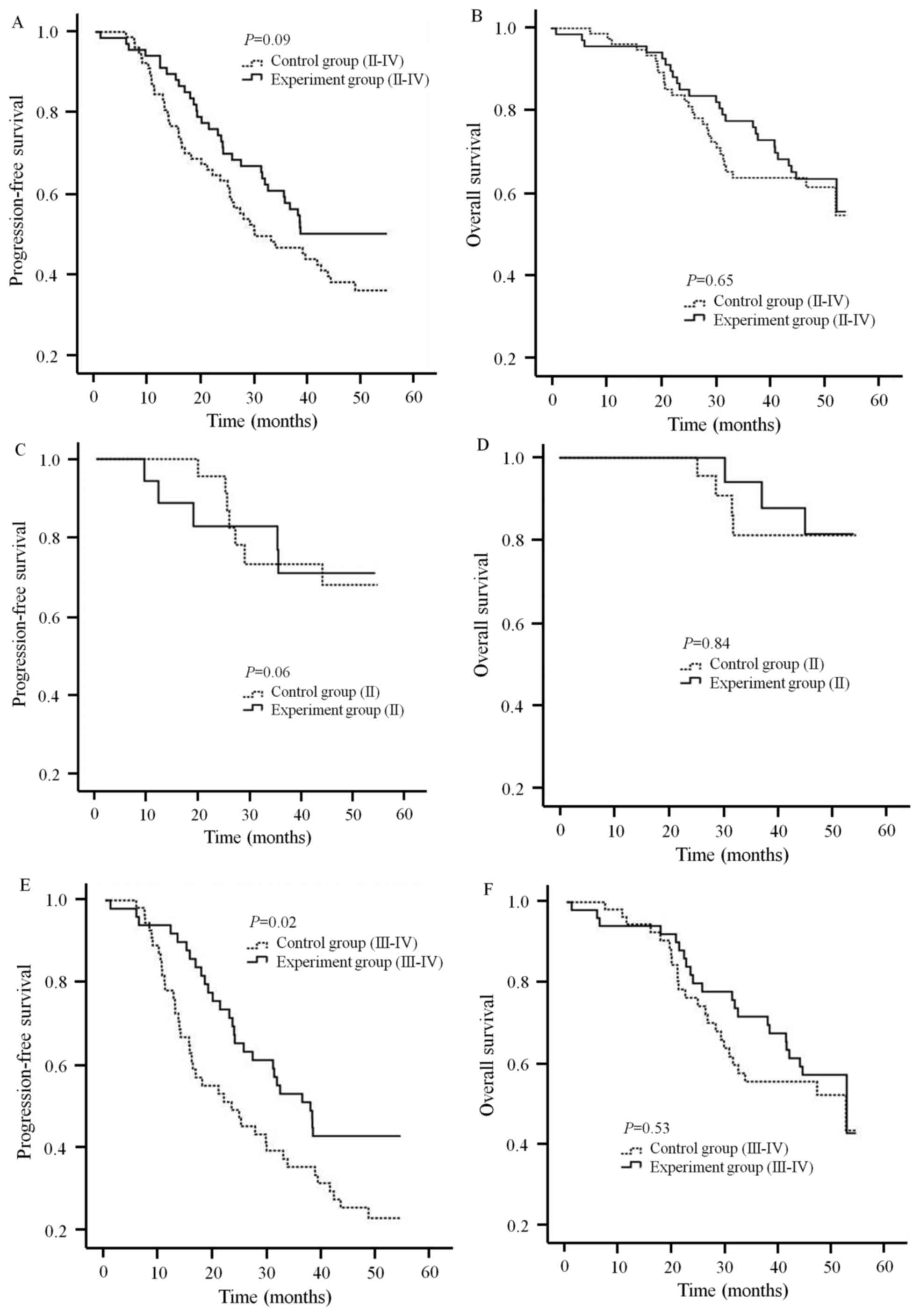
With respect to the primary endpoints, the
difference in the 5-year OS or PFS rate was not significant between
the NDP and the CBP groups. The PFS rate in the NDP group (50.20%)
was not statistically different from that of the CBP group (36.20%;
Fig. 1A; P=0.09), as revealed by
Kaplan-Meier analysis. Similarly, the 5-year OS rate was 63.5% in
the NDP group and 61.5% in the CBP group. Although the NDP group
exhibited a higher OS rate than the CBP group, no statistical
difference was observed between the two groups (Table II and Fig.
1B; P=0.65). Thus, the two treatment groups had the same effect
in terms of prolonging the lifespan of patients, and delaying the
progression of EOC.
| Table II.Comparison of adverse reactions
between the two groups. |
Table II.
Comparison of adverse reactions
between the two groups.
|
|
| Classification of
adverse reaction |
|
|
|
|
|---|
|
|
|
|
|
|
|
|
|---|
| Symptom | Group | 0 | I | II | III | IV | Total | Incidence (%) | P-value | Grade III–IV
incidence (%) | P-value |
|---|
| Leukocyte | NDP | 16 | 30 | 36 | 9 | 1 | 92 | 82.61 | 0.69 | 10.87 | 0.03 |
|
| CBP | 13 | 24 | 32 | 20 | 1 | 90 | 85.56 |
| 23.33 |
|
| Thrombocyte | NDP | 58 | 21 | 8 | 5 | 0 | 92 | 36.96 | 0.37 | 5.43 | 0.28 |
|
| CBP | 50 | 21 | 10 | 9 | 0 | 90 | 44.44 |
| 10.00 |
|
| Granulocyte | NDP | 22 | 25 | 22 | 16 | 7 | 92 | 76.09 | 0.47 | 25.00 | 0.08 |
|
| CBP | 17 | 11 | 28 | 19 | 15 | 90 | 81.11 |
| 37.78 |
|
| Hemoglobin | NDP | 14 | 27 | 43 | 8 | 0 | 92 | 84.78 | 1.00 | 8.70 | 0.63 |
|
| CBP | 14 | 29 | 37 | 8 | 2 | 90 | 84.44 |
| 11.11 |
|
| TBIL | NDP | 87 | 0 | 5 | 0 | 0 | 92 | 5.43 | 0.77 | 0 | 0.50 |
|
| CBP | 84 | 0 | 5 | 1 | 0 | 90 | 6.67 |
| 1.11 |
|
| Creatinine | NDP | 89 | 3 | 0 | 0 | 0 | 92 | 3.26 | 0.25 | 0 | – |
|
| CBP | 90 | 0 | 0 | 0 | 0 | 90 | 0 |
| 0 |
|
| ALT | NDP | 60 | 31 | 1 | 0 | 0 | 92 | 34.78 | 1.00 | 0 | – |
|
| CBP | 59 | 30 | 1 | 0 | 0 | 90 | 34.44 |
| 0 |
|
| AST | NDP | 67 | 25 | 0 | 0 | 0 | 92 | 27.17 | 0.39 | 0 | – |
|
| CBP | 71 | 19 | 0 | 0 | 0 | 90 | 21.11 |
| 0 |
|
|
Nausea/vomiting | NDP | 24 | 48 | 17 | 3 | 0 | 92 | 73.91 | 0.51 | 3.26 | 0.50 |
|
| CBP | 28 | 38 | 19 | 4 | 1 | 90 | 68.89 |
| 5.56 |
|
| Peripheral nervous
system | NDP | 71 | 17 | 4 | 0 | 0 | 92 | 22.83 | 1.00 | 0 | – |
|
| CBP | 69 | 19 | 2 | 0 | 0 | 90 | 23.33 |
| 0 |
|
Stratification analysis was further performed
according to FIGO stage. For patients with FIGO II stage EOC, the
PFS and OS were not statistically different between the NDP group
and the CBP group (P=0.06 for PFS, P=0.84 for OS; Fig. 1C and D). For the patients with FIGO
stage III–IV EOC, the OS rate in the two groups did not
significantly differ (Fig. 1F;
P=0.53). However, the PFS rate in the NDP group was significantly
higher than the CBP group (Fig. 1E;
P=0.02).
Toxicity profiles
With respect to the secondary endpoints, the
hematological and non-hematological toxicity profiles were
summarized in Table II. A
significant difference was observed in the white blood cell count
and occurrence of grade 3 or 4 leucopenia between the two groups.
The incidence of leucopenia was higher in the CBP group than the
NDP group (23.33 vs. 10.87%; P<0.05). The rate of granulopenia,
thrombocytopenia, hemoglobinemia and nausea/vomiting tended to be
lower in the NDP group when compared with the CBP group; however,
no statistical difference was observed between the two groups.
Furthermore, no grade 3 or 4 renal toxicity or neurotoxicity was
observed in the two groups.
Discussion
EOC is the most lethal gynecological malignancy and
is sensitive to chemotherapy. Survival is markedly improved when a
combination of paclitaxel and platinum-based chemotherapy is
administered as a first-line therapy. Even so, the rates of
recurrence and mortality remain high (24,25). Thus,
improved treatments for this disease are required. One option is to
substitute NDP for CBP, as has been done in the present study. The
present phase III trial intended to compare the clinical efficacy
of the experimental regimen of NDP plus paclitaxel and the control
regimen of CBP plus paclitaxel as first-line treatments for
patients with EOC.
According to previous studies, the median PFS time
was 16–21 months and the median OS time was 32–57 months in
patients with advanced EOC (26–30). In
the present study, the observed PFS time was longer (38.23 months
for the NDP group and 29.80 months for the CBP group), while the
observed OS time was similar to the value previously reported
(55.63 months for the NDP group and 55.10 months for the CBP
group). The results of the present study indicated that prolonged
PFS did not result in longer OS, a result also indicated in
previous studies (30,31).
Overall, there was no statistical difference in PFS
and OS between the two groups. However, stratified analysis
revealed that that the NDP treatment significantly extended PFS
time of patients with FIGO stage III–IV EOC (37.90 compared with
23.33 months; P=0.02). The observed survival benefits of NDP may be
explained by increased compliance and the greater number of
chemotherapy cycles that the patients received. Markman et
al (32) reported that the
incidence of hypersensitivity reactions (HSRs) against CBP
increased with repeated treatment. In the present study, the
patients who received NDP suffered less from leucopenia (Table II). It was also reported that NDP was
less renally toxic and had relatively lower rate of neurotoxicity
(33). Michikami et al
(34) revealed that the substitution
of NDP for CBP allowed for continued administration of platinum
agents, hence the patients who were treated with NDP may complete
more chemotherapy cycles than those treated with CBP.
In conclusion, the present multi-center, randomized,
open-label phase III trial indicated that NDP-based regimens may be
alternative platinum-based treatments for EOC. Compared with CBP
plus paclitaxel regimens, NDP plus paclitaxel regimens achieved
comparable survival outcomes and similar toxicity profiles.
However, patients with FIGO stage III–IV disease may experience
more clinical benefits, including prolonged PFS and a lower
incidence rate of leucopenia, from NDP plus paclitaxel
treatment.
Acknowledgements
The present study was supported by National Natural
Science Foundation of China (grant. no. 81672580). The authors
would like to thank the Department of Biostatistics, Nanjing
Medical University (Nanjing, China) for performing the centralized
randomization procedure.
References
|
1
|
Weiderpass E and Labrèche F: Malignant
tumors of the female reproductive system. Saf Health Work.
3:166–180. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Heintz AP, Odicino F, Maisonneuve P, Quinn
MA, Benedet JL, Creasman WT, Ngan HY, Pecorellu S and Beller U:
Carcinoma of the ovary. FIGO 26th Annual Report on the Results of
Treatment in Gynecological Cancer. Int J Gynecol Obstet. 95 Suppl
1:S161–S192. 2006. View Article : Google Scholar
|
|
3
|
Bookman MA, Brady MF, McGuire WP, Harper
PG, Alberts DS, Friedlander M, Colombo N, Fowler JM, Argenta PA, De
Geest K, et al: Evaluation of new platinum-based treatment regimens
in advanced-stage ovarian cancer: A phase III trial of the
Gynecologic Cancer Intergroup. J Clin Oncol. 27:1419–1425. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Bristow RE, Tomacruz RS, Armstrong DK,
Trimble EL and Montz FJ: Survival effect of maximal cytoreductive
surgery for advanced ovarian carcinoma during the platinum era: A
meta-analysis. J Clin Oncol. 20:1248–1259. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Thigpen T, duBois A, McAlpine J, DiSaia P,
Fujiwara K, Hoskins W, Kristensen G, Mannel R, Markman M, Pfisterer
J, et al: First-line therapy in ovarian cancer trials. Int J
Gynecol Cancer. 21:756–762. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Monk BJ and Coleman RL: Changing the
paradigm in the treatment of platinum-sensitive recurrent ovarian
cancer: From platinum doublets to nonplatinum doublets and adding
antiangiogenesis compounds. Int J Gynecol Cancer. 19 Suppl
2:S63–S67. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Monk BJ, Alberts DS, Burger RA, Fanta PT,
Hallum AV III, Hatch KD and Salmon SE: In vitro phase II comparison
of the cytotoxicity of a novel platinum analog, nedaplatin (254-S),
with that of cisplatin and carboplatin against fresh, human
cervical cancers. Gynecol Oncol. 71:308–312. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Alberts DS, Fanta PT, Running KL, Adair JL
Jr, Garcia DJ, Liu-Stevens R and Salmon SE: In vitro phase II
comparison of the cytotoxicity of a novel platinum analog,
nedaplatin (254-S), with that of cisplatin and carboplatin against
fresh, human ovarian cancers. Cancer Chemother Pharmacol.
39:493–497. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Uchida N, Yoshida H, Yamada H, Wada T,
Daikatsu K, Ikeuchi I, Maekawa R, Sugita K and Yoshioka T:
Combination chemotherapy with nedaplatin and cyclophosphamide in
human ovarian cancer model. Jpn J Cancer Res. 90:887–894. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Uchida N, Yamada H, Maekawa R and Yoshioka
T: Combination chemotherapy of paclitaxel followed by nedaplatin
for human ovarian cancer. Gan To Kagaku Ryoho. 29:1943–1949.
2002.(In Japanese). PubMed/NCBI
|
|
11
|
Noda K, Ikeda M, Yakushiji M, Nishimura H,
Terashima Y, Sasaki H, Hata T, Kuramoto H, Tanaka K, Takahashi T,
et al: A phase II clinical study of cis-diammine glycolato
platinum, 254-S, for cervical cancer of the uterus. Gan To Kagaku
Ryoho. 19:885–892. 1992.(In Japanese). PubMed/NCBI
|
|
12
|
Inuyama Y, Miyake H, Horiuchi M, Hayasaki
K, Komiyama S and Ota K: A late phase II clinical study of
cis-diammine glycolato platinum, 254-S, for head and neck cancers.
Gan To Kagaku Ryoho. 19:871–877. 1992.(In Japanese). PubMed/NCBI
|
|
13
|
Kato T, Nishimura H, Yakushiji M, Noda K,
Terashima Y, Takeuchi S, Takamizawa H, Suzuki M, Arai M, Ota M, et
al: Phase II study of 254-S (cis-diammine glycolato platinum) for
gynecological cancer. Gan To Kagaku Ryoho. 19:695–701. 1992.(In
Japanese). PubMed/NCBI
|
|
14
|
Taguchi T, Wakui A, Nabeya K, Kurihara M,
Isono K, Kakegawa T and Ota K: A phase II clinical study of
cis-diammine glycolato platinum, 254-S, for gastrointestinal
cancers. 254-S Gastrointestinal Cancer Study Group. Gan To Kagaku
Ryoho. 19:483–488. 1992.(In Japanese).
|
|
15
|
Akaza H, Togashi M, Nishio Y, Miki T,
Kotake T, Matsumura Y, Yoshida O and Aso Y: Phase II study
ofcis-diammine(glycolato)platinum, 254-S, in patients with advanced
germ-cell testicular cancer, prostatic cancer, and
transitional-cell carcinoma of the urinary tract. 254-S Urological
Cancer Study Group. Cancer Chemother Pharmacol. 31:187–192. 1992.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Fukuda M, Shinkai T, Eguchi K, Sasaki Y,
Tamura T, Ohe Y, Kojima A, Oshita F, Hara K and Saijo N: Phase II
study of (glycolate-O,O,)diammineplatinum(II), a novel platinum
complex, in the treatment of non-small-cell lung cancer. Cancer
Chemother Pharmacol. 26:393–396. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Lebwohl D and Canetta R: Clinical
development of platinum complexes in cancer therapy: An historical
perspective and an update. Eur J Cancer. 34:1522–1534. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Hong WS, Min YI, Kim HT, Cho YB, Kim KH
and Kim DK: Antitumor activity of five new platinum complexes
having a glycolate leaving ligand. J Korean Med Sci. 10:269–274.
1995. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Weiss RB and Christian MC: New cisplatin
analogues in development. A review. Drugs. 46:360–377. 1993.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Paik ES, Lee YY, Lee EJ, Choi CH, Kim TJ,
Lee JW, Bae DS and Kim BG: Survival analysis of revised 2013 FIGO
staging classification of epithelial ovarian cancer and comparison
with previous FIGO staging classification. Obstet Gynecol Sci.
58:124–134. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Calvert AH, Newell DR, Gumbrell LA,
O'Reilly S, Burnell M, Boxall FE, Siddik ZH, Judson IR, Gore ME and
Wiltshaw E: Carboplatin dosage: Prospective evaluation of a simple
formula based on renal function. J Clin Oncol. 7:1748–1756. 1989.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Cockcroft DW and Gault MH: Prediction of
creatinine clearance from serum creatinine. Nephron. 16:31–41.
1976. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Giantonio BJ, Catalano PJ, Meropol NJ,
O'Dwyer PJ, Mitchel EP, Alberts SR, Schwartz MA and Benson AB:
Bevacizumab in combination with oxaliplatin, fluorouracil, and
leucovorin (FOLFOX4) for previously treated metastatic colorectal
cancer: Result from the Eastern Cooperative Oncology Group Study
E3200. J Clin Oncol. 25:1539–1544. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Aghajanian C, Blank SV, Goff BA, Judson
PL, Teneriello MG, Husain A, Sovak MA, Yi J and Nycum LR: OCEANS: A
randomized, double-blinded, placebo-controlled phase III trial of
chemotherapy with or without bevacizumab in patients with
platinum-sensitive recurrent epithelial ovarian, primary
peritoneal, or fallopian tube cancer. J Clin Oncol. 30:2039–2045.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Jemal A, Murray T, Ward E, Samuels A,
Tiwari RC, Ghafoor A, Feuer EJ and Thun MJ: Cancer statistics,
2005. CA Cancer J Clin. 55:10–30. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Piccart MJ, Bertelsen K, Stuart G, Cassidy
J, Mangioni C, Simonsen E, James K, Kaye S, Vergote I, Blom R, et
al: Long-term follow-up confirms a survival advantage of the
paclitaxel-cisplatin regimen over the cyclophosphamide-cisplatin
combination in advanced ovarian cancer. Int J Gynecol Cancer. 13
Suppl 2:S144–S148. 2003. View Article : Google Scholar
|
|
27
|
Ozols RF, Bundy BN, Greer BE, Fowler JM,
Clarke-Pearson D, Burger RA, Mannel RS, DeGeest K, Hartenbach EM
and Baergen R; Gynecologic Oncology Group, : Phase III trial of
carboplatin and paclitaxel compared with cisplatin and paclitaxel
in patients with optimally resected stage III ovarian cancer: A
Gynecologic Oncology Group study. J Clin Oncol. 21:3194–3200. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
du Bois A, Lück HJ, Meier W, Adams HR,
Möbus V, Costa S, Bauknecht T, Richter B, Warm M, Schröder W, et
al: A randomized clinical trial of cisplatin/paclitaxel versus
carboplatin/paclitaxel as first-line treatment of ovarian cancer. J
Natl Cancer Inst. 95:1320–1329. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Neijt JP, Engelholm SA, Tuxen MK, Sorensen
PG, Hansen M, Sessa C, de Swart CA, Hirsch FR, Lund B and van
Houwelingen HC: Exploratory phase III study of paclitaxel and
cisplatin versus paclitaxel and carboplatin in advanced ovarian
cancer. J Clin Oncol. 18:3084–3092. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
McGuire WP, Hoskins WJ, Brady MF, Kucera
PR, Partridge EE, Look KY, Clarke-Pearson DL and Davidson M:
Cyclophosphamide and cisplatin compared with paclitaxel and
cisplatin in patients with stage III and stage IV ovarian cancer.
New Engl J Med. 334:1–6. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Li Y and Zhang Q: A Weibull multi-state
model for the dependence of progression-free survival and overall
survival. Stat Med. 34:2497–2513. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Markman M, Kennedy A, Webster K, Elson P,
Peterson G, Kulp B and Belinson J: Clinical features of
hypersensitivity reactions to carboplatin. J Clin Oncol.
17:11411999. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Sasaki Y, Shinkai T, Eguchi K, Tamura T,
Ohe Y, Ohmori T and Saijo N: Prediction of the antitumor activity
of new platinum analogs based on their ex vivo pharmacodynamics as
determined by bioassay. Cancer Chemother Pharmacol. 27:263–270.
1991. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Michikami H, Minaguchi T, Ochi H, Onuku M,
Okada S, Matsumoto K, Satoh T, Oki A and Yoshikawa H: Safety and
efficacy of substituting nedaplatin after carboplatin
hypersensitivity reactions in gynecologic malignancies. J Obstet
Gynaecol Res. 39:330–335. 2013. View Article : Google Scholar : PubMed/NCBI
|