Introduction
Lung cancer is the most common type of malignant
tumor, with a high incidence of ~2.1 million new cases and ~1.8
million deaths of lung cancer in 2018 worldwide (1–3).
Non-small cell lung cancer (NSCLC) accounts for 15% of all cases of
lung cancer with multiple toxin-associated mutations, including
epidermal growth factor, KRAS, PI3K subunit α (PIK3CA) and AKT1
mutations and PIK3CA amplification (4–6). Cancer
therapy has become increasingly personalized over the past decade
(7–9), and new effective diagnostic methods and
evaluation systems are urgently needed for imaging malignancies and
monitoring their therapeutic responses.
Imaging technologies allow non-invasive diagnosis of
cancers and provide dynamic information on the effectiveness of
therapies and on patient prognosis. Cancer diagnosis by
conventional radiological imaging methods, such as computed
tomography (CT) or magnetic resonance imaging (MRI) scanning, is
not fully straightforward in certain cases due to the relatively
non-specific nature of the clinical features and incomplete
validation of imaging findings (10). Molecular imaging has shown great
potential in the cancer field and has provided detailed information
about the uptake of target molecules by numerous types of tumor
lesions and their presence therein. The most common application to
date has been the imaging of overexpressed antigen-associated
tumors; the radiolabeled antibody of the human epidermal growth
factor receptors (HER1, HER2 and HER3) have been widely used in
breast cancer, gastric cancer and NSCLC (11,12).
Compared with traditional imaging techniques such as CT or MRI,
molecular imaging in nuclear medicine is a non-invasive whole-body
scanning modality, and is more suitable for the detection and
quantification of the expression levels of target molecules in
tumor tissue (13,14). Radioimmunoimaging, which involves the
use of a radionuclide in combination with highly specific
antibody-based imaging tracers (15), can provide a non-invasive way to
evaluate the expression and distribution of molecular targets in
vivo, thereby contributing to accurate disease diagnosis and
therapeutic and prognostic evaluations. Therefore, the search for
molecular markers that are highly specific to the various cancer
types is of great importance and urgently required for
radioimmunoimaging.
Angiogenesis is of fundamental importance for
growing tumors (16,17) since by switching to an angiogenic
phenotype, followed by the development of new vasculature, solid
tumors can reach a critical size of 1–2 mm3 (18,19).
Thus, angiogenesis is an attractive and novel target for tumor
diagnosis.
CD93, a transmembrane protein, acts as an adhesion
molecule to promote the adhesion and migration of inflammatory
cells to endothelial cells, the phagocytosis of apoptotic cells,
and the formation of new blood vessels (20). Previous studies have shown CD93 to be
a key regulator of tumor angiogenesis, regulating adhesion between
the cells and the cellular matrix. Decreased expression of CD93
could induce cytoskeletal reconstruction and adhesion loss, thereby
inhibiting endothelial cell adhesion and migration, as well as
abnormal angiogenesis in glioblastoma (21,22).
Additionally, CD93 has low expression in normal tissue, but
differential expression in metastatic and advanced primary glioma,
indicating its potential use in cancer diagnosis (23).
In the present study, a 125I-labeled
CD93-specific monoclonal antibody (125I-anti-CD93 mAb)
was prepared for the investigation of CD93 expression in mouse
xenograft models of two different types of NSCLC cell lines. We
postulated that 125I-anti-CD93 mAb radioimmunoimaging
could be used for monitoring NSCLC cells with CD93-positive
expression, and therefore may be useful in the future for
non-invasive clinical diagnosis of this disease.
Materials and methods
Ethics statement
All animal studies were conducted in accordance with
protocols approved by the Animal Care and Use Committee of Shandong
University.
Cell culture
The human lung adenocarcinoma (LUAD) A549 cell line
and the human lung squamous cell carcinoma (LUSC) SK-MES-1 cell
line (both human NSCLC cell lines) were obtained from the American
Type Culture Collection. Both cell lines were cultured in RPMI-1640
medium supplemented with 10% fetal bovine serum (Gibco; Thermo
Fisher Scientific, Inc.) and 1% penicillin/streptomycin (HyClone;
GE Healthcare Life Sciences) at 37°C in a humidified incubator with
5% CO2.
Flow cytometry analysis of CD93
expression in NSCLC cells
CD93 expression in A549 and SK-MES-1 cells was
determined using flow cytometry. In brief, the cells were digested
by trypsin, centrifuged (100 × g at 4°C for 5 min) and suspended in
ice-cold PBS (pH 7.4) at a concentration of 5×105
cells/100 µl. The cells were then incubated with PBS and
phycoerythrin (PE)-conjugated CD93 antibody (200 µg/ml, dissolved
in phosphate-buffered solution with 0.09% sodium azide and 0.2%
BSA, pH 7.2; BioLegend, Inc.) for 30 min at 4°C. After the
incubation, the cells were washed twice with ice-cold PBS and the
binding efficiency was analyzed using a MACSQuant flow cytometer
(Miltenyi Biotec GmbH). The mean fluorescence intensities were
quantified using FlowJo 7.6.1 software (Tree Star, Inc.).
Quantification of CD93 mRNA and
protein expression levels
The CD93 mRNA and protein expression levels were
evaluated using semi-quantitative reverse transcription (RT)-PCR
and western blot assays, respectively.
For the semi-quantitative RT-PCR analysis, cells at
~70% confluency were digested by trypsin and centrifuged (100 × g
at 4°C for 5 min), and the total RNA was extracted using
TRIzol® (Invitrogen; Thermo Fisher Scientific, Inc.)
according to the manufacturer's instructions. Total RNA was
resuspended in RNase-free water. Subsequently, the first-strand DNA
was generated using TransScript® One-Step gDNA Removal
and cDNA Synthesis kits (Beijing Transgen Biotech, Co., Ltd.). The
reactions were performed in a total volume of 20 µl, consisting of
1 µg total RNA, 1 µl anchored oligo(dT)18 (0.5 µg/µl), 10 µl 2X
TransScript reaction mix, 1 µl reverse transcription enzyme mix and
7 µl RNase-free water, and incubated at 42°C for 30 min and 85°C
for 5 min. According to the operation instruction of EasyTaq PCR
kit (Beijing Transgen Biotech, Co., Ltd.), 2 µl complementary DNA
was mixed with 0.5 µl specific primers (10 µM), 2 µl dNTP (2.5 mM),
0.25 µl EasyTaq DNA polymerase, 2.5 µl 10X EasyTaq buffer and 17.25
µl double-distilled water. The PCR primer sequences used are as
follows: CD93 forward, 5′-TGCCTGGACCCTAGTCTGC-3′ and reverse,
5′-GCTTGGAGATGCACGAGTTC-3′; and GAPDH forward,
5′-GGAGCGAGATCCCTCCAAAAT-3′ and reverse,
5′-GGCTGTTGTCATACTTCTCATGG-3′. GAPDH was used as the control. The
PCR conditions were as follows: Initial denaturation at 94°C for 3
min, followed by 35 cycles of 94°C for 30 sec, 56°C for 30 sec and
72°C for 1 min, with a final extension at 72°C for 10 min. The PCR
products were electrophoresed in 1.5% (w/v) agarose gels containing
0.5 µg/ml ethidium bromide to confirm the expected size of the
fragments and were visualized under UV light. Band density was
analyzed and quantified using Gel-Pro 3.1 software (Media
Cybernetics, Inc.).
For the western blot analysis, A549 and SK-MES-1
cells at ~70% confluency were harvested by scraping and the total
protein was extracted using RIPA lysis buffer containing 1%
phenylmethylsulfonyl fluoride (Boston BioProducts, Inc.). The
protein concentration was determined with a protein assay kit
(Beyotime Institute of Biotechnology). Then, 20 µg total protein
was loaded onto the corresponding wells of 4–12% SDS-PAGE (Bio-Rad
Laboratories, Inc.) together with the Chameleon Duo Pre-stained
Protein Ladder (SMOBIO Technology, Inc.). The electrophoresed
proteins were transferred onto a 0.45-µm PVDF membrane (EMD
Millipore) at 100 mV for 90 min at 4°C in transfer buffer (25 mM
Tris, 0.2 M glycine and 20% methanol). The membrane was blocked in
5% (w/v) skimmed milk blocking buffer for 1 h at 20°C with
agitation and then washed with TBS containing Tween-20 (TBS-T).
Rabbit anti-human CD93 antibody (dilution, 1:1,000; dissolved in
40% glycerol, 9.85% Tris glycine and 50% tissue culture
supernatant, pH 7.4; cat. no. ab134079; Abcam) was added and the
membrane was incubated overnight at 4°C. GAPDH polyclonal antibody
(dilution, 1:5,000; dissolved in phosphate-buffered solution with
0.02% sodium azide and 50% glycerol, pH 7.2; cat. no. AB0063;
Bioworld Technology, Inc.) was used as the loading control. Next,
the membrane was washed 3 times with TBS-T and then incubated with
horseradish peroxidase (HRP)-conjugated goat anti-rabbit IgG
(dilution 1:10,000; dissolved in phosphate-buffered solution with
0.09% sodium azide and 0.2% BSA, pH 7.2; cat. no. TA140003; OriGene
Technologies, Inc.) for 1 h at 20°C. After washing with TBS-T,
Immobilon Western HRP Substrate (EMD Millipore) was added. The
membrane was subsequently scanned and quantitatively analyzed using
a Tanon 4200 imaging system (Tanon Science & Technology Co.,
Ltd.) and ImageJ 1.8.0 software (National Institutes of
Health).
Preparation of the
125I-anti-CD93 mAb
Radioiodination of anti-CD93 mAb and rabbit isotype
IgG (dissolved in 0.01% sodium azide, 59% PBS, 40% glycerol and
0.05% BSA, pH 7.2; cat. nos. ab134079 and ab172730; Abcam) with
Na125I was performed according to the Iodogen
solid-phase labeling method, as previously described (24). In brief, 10 µg anti-CD93 mAb was
added to 100 µl phosphate buffer (PB; 0.05 M; pH 7.4), and then 12
megabecquerel (MBq; 12 MBq=300 mCi) Na125I was added.
The mixture was incubated for 20 min at 37°C, and the reaction was
subsequently terminated by adding 150 µl 0.05 M PB and incubating
the mixture for 10 min at 37°C. The labeling compound was purified
on a Sephadex G-25 gel filtration column (GE Healthcare Life
Sciences) as previously described (25) and the labeling efficiency was
calculated. A mixture of 0.9% saline and methanol at a volume ratio
of 1:2 was used as an unfolding agent. The stability of
125I-anti-CD93 mAb in vitro was determined in
0.05 M PBS (pH 7.4) or in human serum. The 125I-labeled
IgG isotype was used as a non-specific control tracer and was
prepared in a similar method as aforementioned.
Evaluation of
125I-anti-CD93 mAb
The binding affinity of 125I-anti-CD93
mAb to A549 and SK-MES-1 cells was determined. In brief, cells were
seeded into 96-well culture plates at 1×105 cells/well.
125I-anti-CD93 mAb in PBS solution (at concentrations
ranging from 3 to 100 nM) was added to the cells. After incubation
at room temperature for 2 h, the cells were washed twice with
ice-cold 1X PBS containing 0.1% BSA (Shanghai Lianshuo Biological
Technology Co., Ltd.), pyrolyzed with 1 mol/l NaOH and harvested,
and the activity was determined with a CRC 25R gamma counter
(Capintec, Inc.). For the competitive binding assay, 0.1–1,000 nM
anti-CD93 mAb and 15 nM 125I-anti-CD93 mAb were used,
with a final reaction volume of 500 µl. The maximum binding ability
(Bmax), dissociation constant (Kd) and receptor density on the
cells were determined using GraphPad Prism 5.0 software (GraphPad
Software, Inc.).
Animal studies
Subcutaneous xenograft tumors of the A549 or
SK-MES-1 cell lines were induced in 240 5-week-old (weight, 18±2 g)
female nude mice (BALB/c-nu; n=5/group; Beijing Vital River
Laboratory Animal Technology Co., Ltd.) by injecting
2×106 tumor cells (suspended in 200 µl PBS) into the
lower right flank of the animal. All mice were bred and maintained
under specific pathogen-free conditions in individually ventilated
(HEPA-filtered air) sterile cages (14 days; humidity, 50–60%). All
mice were maintained under a 12-h light/dark cycle with access to
standard mice chow and sterilized water ad libitum. The mice
and tumor size were monitored every 2 days for 2 weeks (Fig. S1). The volume of the tumor was
calculated as (long diameter × short diameter × short diameter)/2.
The animals were subjected to imaging and biodistribution studies
once the tumor size had reached 5–10 mm in diameter.
Dynamic whole-body phosphor
autoradiography
To block hormone synthesis by the thyroid gland, 10%
potassium iodide was added to the drinking water 2 days before
injection of the radiotracers. Tumor-bearing mice were then
intravenously injected with 0.55 MBq 125I-anti-CD93 mAb.
125I–IgG (0.55 MBq) was also injected into another group
of A549 tumor-bearing mice as the IgG isotype control for imaging.
Phosphor autoradiography scans were conducted at 24, 48 and 72 h
post injection. Dynamic whole-body phosphor autoradiography was
performed with a Cyclone Plus scanner (PerkinElmer, Inc.).
Anesthesia was induced and maintained with pentobarbital sodium (60
mg/kg) by intraperitoneal injection. Each anesthetized mouse was
placed on the storage phosphor screen plate, with its back to the
plate in low light, and exposed to the plate for 20 min. Upon
exposure, the plate was immediately scanned. Semi-quantitative
analysis was performed by manually drawing rectangular regions of
interest (n=5) within the target area at each time point. Digital
light units per square millimeter (DLU/mm2) measurements
were obtained using OptiQuant Image Analysis Software v5.0
(PerkinElmer, Inc.).
Biodistribution studies
125I-anti-CD93 mAb (0.37 MBq) was
injected into each mouse tumor model (n=5 per group).
125I–IgG (0.37 MBq) was also injected in another group
of A549 tumor-bearing mice to demonstrate the non-specific
distribution of the IgG isotype. The mice were sacrificed by
cervical dislocation at 24, 48 and 72 h post injection, and the
stopping of the heart and the limbs turning white indicated death.
The tumor, blood and major tissues/organs (heart, lung, liver,
kidney, spleen, small intestine and muscle) were harvested, washed
and weighed. The samples and primed standards used as the
radioactive background control were evaluated for radioactivity
with the gamma counter, and the measurements were corrected for
physical decay using a standard value. Tissue activity was
expressed as the percentage of injected dose per gram (% ID/g). The
target-to-non-target (T/NT) ratio was defined as the ratio of the
tumor to the muscle on the opposite side from the cell injection
site.
Statistical analysis
All experiments were repeated three times. All data
are denoted as the mean ± SD. The Student's t-test was used to
compare the expression of CD93 in A549 and SK-MES-1 cell lines.
Statistical comparisons of biodistribution data sets were analyzed
using a one-way factorial ANOVA. All analyses were performed with
GraphPad Prism v5.0 software (GraphPad Software, Inc.). P<0.05
was considered to indicate a statistically significant
difference.
Results
Flow cytometry analysis of CD93
expression in the NSCLC cell lines
The two NSCLC cell lines incubated with either
PE-conjugated CD93 antibody or negative control PBS were analyzed
for CD93 expression using flow cytometry (Fig. 1). The A549 cells displayed enhanced
fluorescence signals when incubated with the PE-conjugated CD93
antibody, which was indicative of elevated CD93 expression in this
cell line. By contrast, a lower fluorescence signal was detected in
the SK-MES-1 cell line.
Quantification of CD93 mRNA and
protein expression in the NSCLC cell lines
The relative expression levels of CD93 in the A549
and SK-MES-1 cell lines were determined using western blot
(Fig. 2A) and semi-quantitative
RT-PCR (Fig. 2B) analyses.
Semi-quantitative RT-PCR analysis revealed that CD93 mRNA
expression was high in A549 cells and low in the SK-MES-1 cells.
The ratio of CD93 to GAPDH was obtained by normalizing the band
intensities of CD93 to those of GAPDH at the protein level. The
protein band for A549 cells showed a high signal, indicative of a
high CD93 expression level (n=3), whereas the band for the SK-MES-1
cells showed a low signal, representing a low CD93 expression
level.
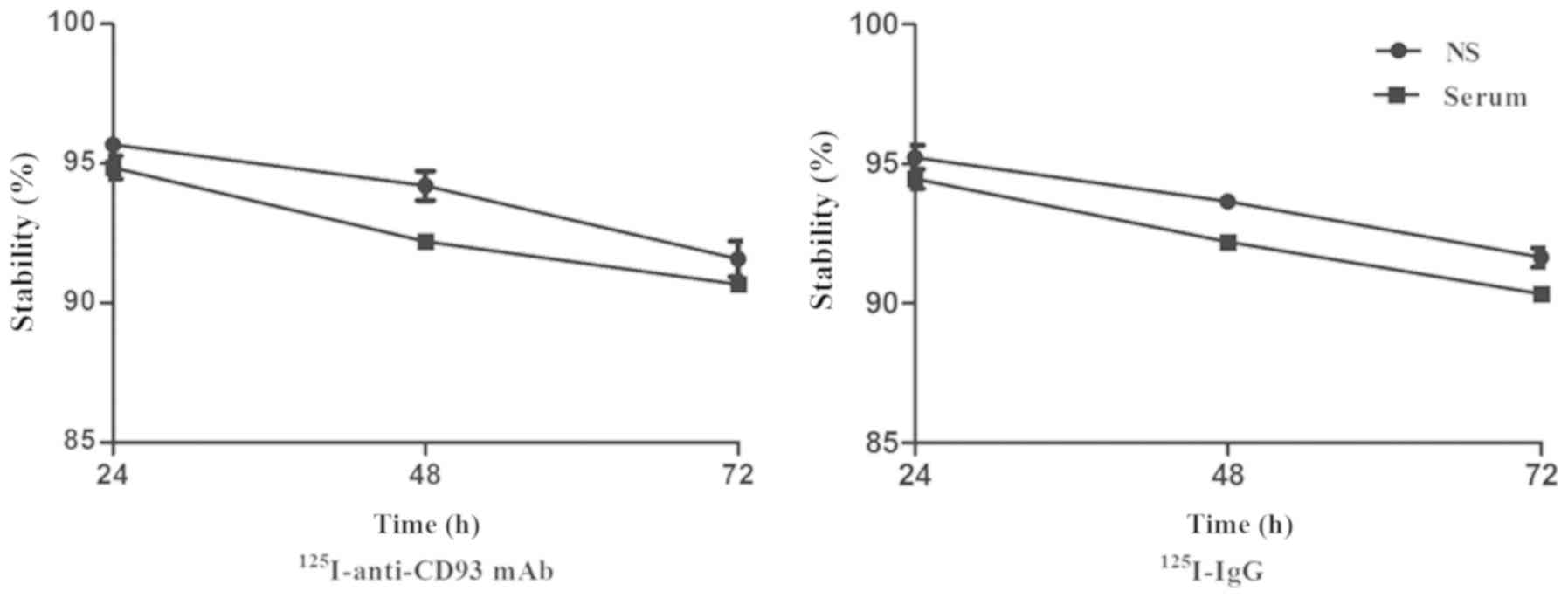
Radiochemical characteristics of the
125I-anti-CD93 mAb
Labeling of the anti-CD93 mAb with 125I
resulted in a labeling yield of 91.37±2.21%, whereas labeling of
the IgG yielded 90.24±1.58% 125I–IgG. The radiochemical
purity of both 125I-anti-CD93 mAb and
125I–IgG was >90%. The specific radioactivity of
125I-anti-CD93 mAb was 1,096.44 MBq/mg, whereas that of
125I–IgG was 1,082.88 MBq/mg. Both radiolabeled probes
were relatively stable in human serum and in normal saline, where
the radiochemical purity of these two probes was >90% for ≤72 h,
with no significant difference between them (Fig. 3).
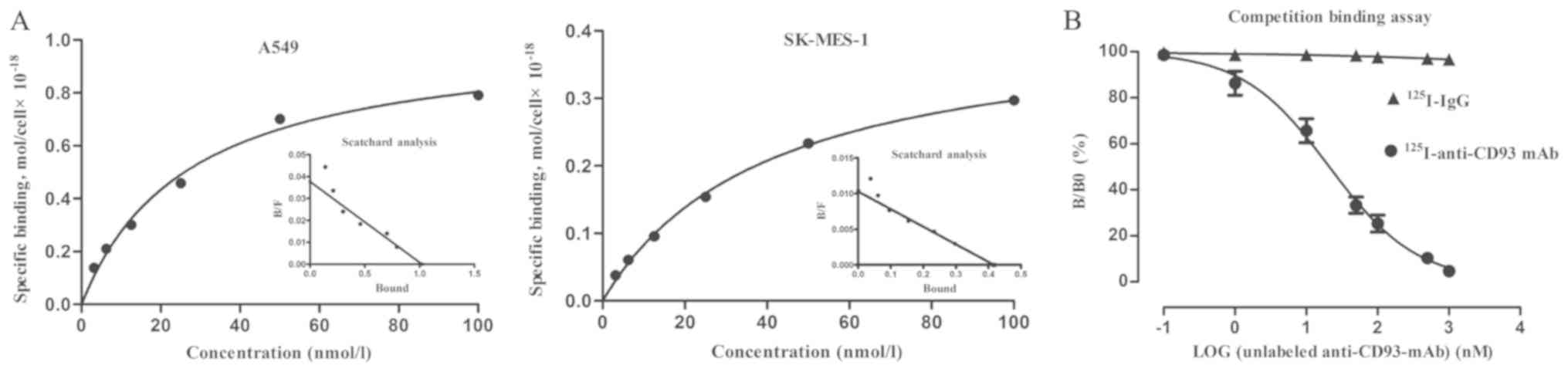
Cell-binding affinity of the
125I-anti-CD93 mAb
The cell-binding studies indicated that the Kd of
125I-anti-CD93 mAb was ~27.09±1.81 nM for A549 cells and
40.31±3.55 nM for SK-MES-1 cells (Fig.
4A), demonstrating that 125I-anti-CD93 mAb had a
higher binding affinity for A549 cells than for SK-MES-1 cells. In
the competitive binding analysis (Fig.
4B), the excess unlabeled anti-CD93 mAb could almost completely
block the binding of 125I-anti-CD93 mAb, which was
comparable with the 3–8% non-specific binding observed for
125I–IgG.
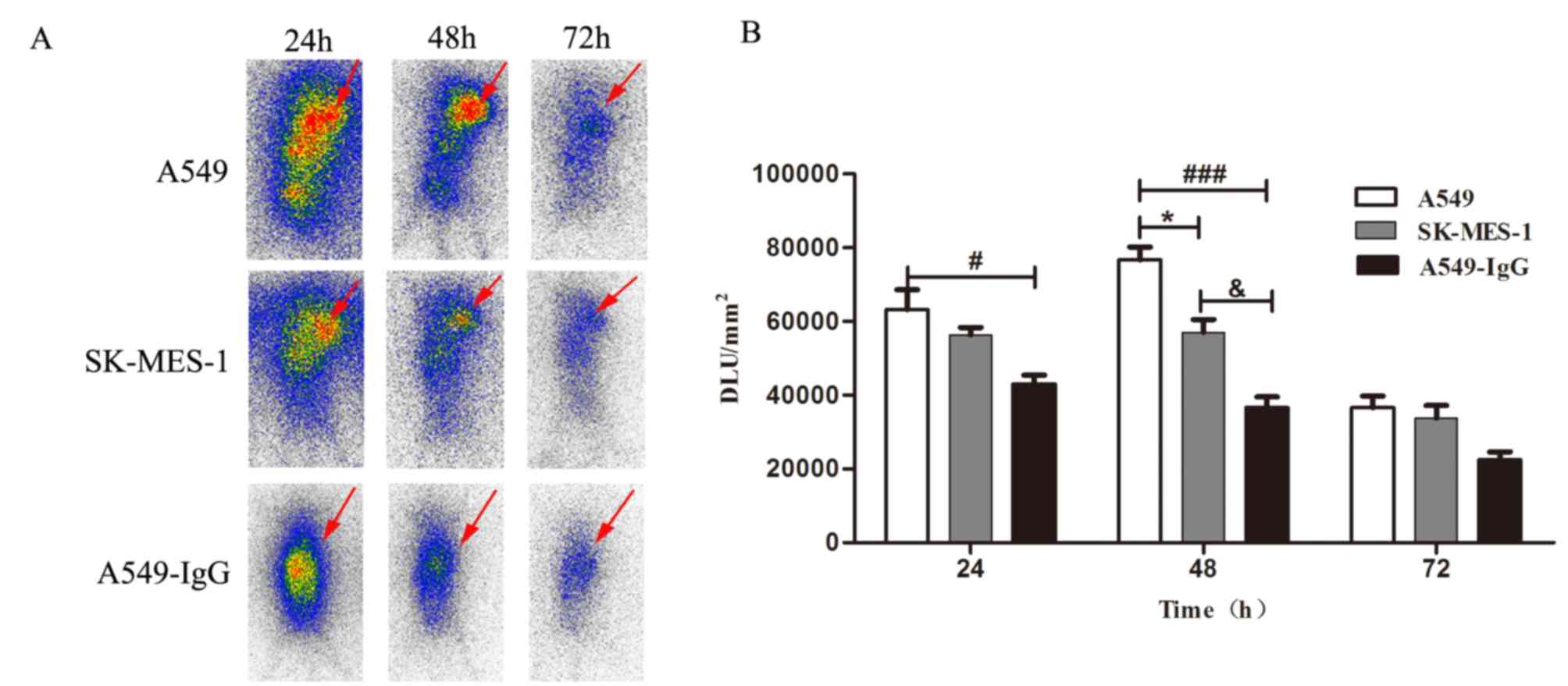
Dynamic whole-body phosphor
autoradiography
Whole-body phosphor autoradiography was performed at
24, 48 and 72 h after injection of the 125I-anti-CD93
mAb into the A549 and SK-MES-1 tumor-bearing mice. The uptake of
125I-anti-CD93 mAb in A549 tumor bearing mice increased
from 24 h and declined at 72 h (Fig.
5; Table SI), with the highest
uptake occurring at 48 h post-injection. At all times after
injection, A549 tumors displayed a higher uptake of radioactivity
compared with that of SK-MES-1 tumors. The radioactivity in the
tumor area showed a substantial increase from 63,210±5,419 to
76,740±3,430 DLU/mm2 for the A549 model, whereas there
was only an increase from 56,410±1991 to 57,060±3,495
DLU/mm2 for the SK-MES-1 model. There was no obvious
radioactivity concentration in 125I–IgG group (i.e.
A549-IgG group). 125I–IgG could not delineate the tumor
sites at any time point (Fig. 5),
suggesting that there was a specific accumulation of
125I-anti-CD93 mAb in the CD93-positive tumors only.
Biodistribution studies
Ex vivo biodistribution studies were
performed to verify the results of the imaging studies and to
further quantify the 125I-anti-CD93 mAb uptake. As
presented in Table I,
125I-anti-CD93 mAb exhibited favorable blood clearance
efficiency in A549 tumor xenograft models, comparable with the
non-tumor-bearing mice (Table II).
The uptake of 125I-anti-CD93 mAb by A549 tumors was
7.81±0.80, 6.42±0.71 and 3.51±0.44% ID/g, with T/NT ratios of
2.42±0.14, 4.45±0.86 and 2.69±0.13 at 24, 48 and 72 h post
injection, respectively. By contrast, the T/NT ratios of
125I-anti-CD93 mAb in SK-MES-1 tumors were 1.67±0.27,
1.97±0.07 and 2.02±0.18 at 24, 48 and 72 h post injection,
respectively, which were significantly lower than those in A549
tumors (Fig. 6 and Table III). The uptake of
125I–IgG was only 1.71±0.24% ID/g at 48 h (Table IV), and the radioactive tracer
failed to target CD93 in the tumor-bearing mice, suggesting the
non-specific tumor binding of 125I–IgG. Statistical
comparisons of T/NT results (Table
SII) further demonstrated the specificity of
125I-anti-CD93 mAb in vivo. Bone, thyroid and
intestines displayed minimal or background levels of
125I-anti-CD93 mAb activity, in agreement with the
imaging data.
 | Table I.Biodistribution of
125I-antiCD93 monoclonal antibody in mice injected with
A549 tumor cells. |
Table I.
Biodistribution of
125I-antiCD93 monoclonal antibody in mice injected with
A549 tumor cells.
|
| Time, h |
|---|
|
|
|
|---|
| Tissue/organ, %
ID/ga,b | 24 | 48 | 72 |
|---|
| Blood | 3.37±0.74 | 1.95±0.38 | 0.96±0.99 |
| Bone | 2.20±0.55 | 1.79±0.52 | 0.76±0.36 |
| Kidney | 6.77±1.05 | 3.35±0.84 | 1.77±0.67 |
| Spleen | 6.06±0.83 | 3.87±0.74 | 2.58±0.32 |
| Thyroid | 2.30±0.48 | 1.61±0.20 | 1.17±0.21 |
| Liver | 4.82±1.07 | 3.70±0.90 | 1.44±0.58 |
| Intestines | 2.78±0.60 | 1.37±0.39 | 0.90±0.32 |
| Heart | 3.27±0.50 | 2.15±0.39 | 1.17±0.20 |
| Lung | 3.27±0.23 | 2.16±0.39 | 1.23±0.08 |
| Muscle | 3.30±0.55 | 1.54±0.34 | 1.31±0.16 |
| Tumor |
7.81±0.80c |
6.42±0.71c |
3.51±0.44c |
| Tumor-to-muscle
ratio | 2.42±0.14 | 4.45±0.86 | 2.69±0.13 |
| Table II.Biodistribution of
125I-antiCD93 monoclonal antibody in non-tumor-bearing
mice. |
Table II.
Biodistribution of
125I-antiCD93 monoclonal antibody in non-tumor-bearing
mice.
|
| Time, h |
|---|
|
|
|
|---|
| Tissue/organ, %
ID/ga,b | 24 | 48 | 72 |
|---|
| Blood | 3.57±0.22 | 1.89±0.20 | 0.97±0.87 |
| Bone | 2.35±0.41 | 1.74±0.48 | 0.81±0.29 |
| Kidney | 6.80±1.11 | 3.29±0.74 | 1.80±0.58 |
| Spleen | 6.02±0.47 | 3.95±0.63 | 2.49±0.32 |
| Thyroid | 2.22±0.35 | 1.70±0.11 | 1.10±0.20 |
| Liver | 4.77±1.01 | 3.81±0.84 | 1.39±0.55 |
| Intestines | 2.81±0.73 | 1.33±0.30 | 0.90±0.21 |
| Heart | 3.25±0.61 | 2.20±0.33 | 1.09±0.33 |
| Lung | 3.20±0.40 | 2.25±0.41 | 1.18±0.21 |
| Muscle | 3.24±0.47 | 1.50±0.40 | 1.25±0.18 |
| Table III.Biodistribution of
125I-antiCD93 monoclonal antibody in mice with SK-MES-1
tumor cells. |
Table III.
Biodistribution of
125I-antiCD93 monoclonal antibody in mice with SK-MES-1
tumor cells.
|
| Time, h |
|---|
|
|
|
|---|
| Tissue/organ, %
ID/ga,b | 24 | 48 | 72 |
|---|
| Blood | 3.40±0.67 | 2.01±0.40 | 1.04±0.06 |
| Bone | 2.27±0.42 | 1.70±0.51 | 0.70±0.21 |
| Kidney | 7.12±0.86 | 4.45±0.40 | 1.81±0.67 |
| Spleen | 6.25±0.59 | 3.89±0.27 | 2.74±0.45 |
| Thyroid | 2.62±0.19 | 1.66±0.53 | 1.18±0.13 |
| Liver | 5.03±1.17 | 4.31±0.75 | 1.50±0.41 |
| Intestines | 2.68±0.56 | 1.46±0.31 | 1.13±0.40 |
| Heart | 3.42±0.82 | 1.97±0.39 | 1.09±0.06 |
| Lung | 3.14±0.19 | 1.98±0.18 | 1.46±0.15 |
| Muscle | 3.06±0.47 | 1.67±0.21 | 1.31±0.14 |
| Tumor |
4.92±0.44c |
3.27±0.40c |
2.62±0.26c |
| Tumor-to-muscle
ratio | 1.67±0.27 | 1.97±0.07 | 2.02±0.18 |
| Table IV.Biodistribution of
125I–IgG isotype antibody in mice with A549 tumor
cells. |
Table IV.
Biodistribution of
125I–IgG isotype antibody in mice with A549 tumor
cells.
|
| Time, h |
|---|
|
|
|
|---|
| Tissue/organ, %
ID/ga,b | 24 | 48 | 72 |
|---|
| Blood | 3.45±0.70 | 1.82±0.14 | 1.09±0.11 |
| Bone | 2.71±0.30 | 1.91±0.19 | 1.13±0.15 |
| Kidney | 6.80±1.05 | 3.40±0.86 | 1.44±0.45 |
| Spleen | 4.42±0.87 | 3.23±0.35 | 1.68±0.37 |
| Thyroid | 2.70±0.43 | 1.65±0.28 | 0.85±0.13 |
| Liver | 6.05±0.84 | 3.29±0.73 | 1.40±0.29 |
| Intestines | 2.22±0.45 | 1.64±0.47 | 0.90±0.19 |
| Heart | 3.83±0.74 | 2.65±0.31 | 1.75±0.29 |
| Lung | 4.10±0.67 | 2.23±0.48 | 1.45±0.72 |
| Muscle | 3.13±0.23 | 1.54±0.43 | 0.90±0.06 |
| Tumor | 4.06±0.32 | 2.45±0.33 | 1.52±0.27 |
| Tumor-to-muscle
ratio | 1.30±0.02 | 1.71±0.24 | 1.68±0.25 |
Discussion
The identification of novel targeted molecules for
specific tumors would increase the accuracy of cancer diagnosis. In
recent years, radioimmunoimaging has emerged as a successful
imaging tool for detecting different types of cancer (26,27).
However, due to the lack of target molecules that can be uptaken in
high quantities by tumor cells, the clinical application of
radioimmunoimaging has been limited (28). Angiogenesis supplies all cellular
tissues with oxygen and nutrients, and plays a key role not only
during embryo development and physiological processes but also in
several diseases, such as diabetes, ischemic heart disease,
glomerular disease and cancer (29,30).
Tumor angiogenesis occurs through the regulation of genes,
including inhibitors of DNA binding-1, endothelial tyrosine kinase
and CD34, that orchestrate endothelial sprouting and vessel
maturation, including the deposition of a vessel-associated
extracellular matrix (31).
Angiogenic factors include activator and inhibitor molecules that
influence the angiogenic process (32).
CD93 has been recently reported as a novel
angiogenic activator (21,33). Known as the complement component C1q
receptor, CD93 is a transmembrane protein that is preferentially
expressed in the vascular endothelium (34). Langenkamp et al (22) reported that high expression of CD93
promoted angiogenesis and reduced survival of patients with
high-grade astrocytic gliomas. Moreover, it was reported that CD93
is highly expressed in nasopharyngeal carcinoma tissues and may
serve as a novel therapeutic target for the treatment of this
disease (35). Therefore, we
postulated that CD93 may be a suitable biomarker for NSCLC.
Despite the evaluation of CD93 in relation to tumors
would be of notable interest clinically, few studies on this topic
have been conducted to date. Recent research shows that anti-CD93
mAb is able to neutralize the formation of new vessels both in
vitro and in vivo (36),
suggesting that it may be a suitable target for antiangiogenic
therapy. The high blood clearance rate of anti-CD93 mAb
demonstrated a low background in the plasma (36). Therefore, radiolabeled anti-CD93 mAb
may provide an effective non-invasive method for visualizing CD93
expression in vivo. Similarly, in the present study, using a
mouse model of lung cancer, the blood uptake of the administered
125I-anti-CD93 mAb was lower compared with that of
125I–IgG (Tables I and
IV). Thus,
125I-anti-CD93 mAb could be used in these NSCLC models,
which is more clinically relevant compared with conventional tumor
imaging agents.
In the ex vivo biodistribution experiment in
the present study, low and uniform lung and cardiac uptakes also
allowed for a higher contrast of the qualitative read on tumors.
However, an unexpectedly high uptake (6.06±0.83% ID/g) in the
spleen was observed 24 h after 125I-anti-CD93 mAb
administration. This may be due to the spleen being blood-rich and
the biggest immune organ, which contained more CD93-positive
immunocytes, so 125I-anti-CD93 mAb in the blood may have
more chances of binding to these immunocytes, leading to the
relatively higher radioactivity retention. Considering that these
CD93-positive immunocytes dispersed in white pulp of the spleen,
the radioactive concentration was only slightly higher in the
spleen. This diffused radioactivity had little effect on the lung
cancer imaging. In addition, the radioactivity retention in the
spleen was found to be time dependent. The uptake in the spleen
decreased to 3.87±0.74% ID/g at 48 h post injection, while
6.42±0.71% ID/g retention was found in the tumors at the same time
point. Furthermore, there was no obvious radioactive accumulation
in the spleen during whole-body phosphor autoradiography at 48 and
72 h post injection. 125I–IgG was also evaluated in the
present study, and it failed to target CD93 in the tumor-bearing
mice, exhibiting non-specific retention in the tumors. These
cell-specific and favorable non-target clearance features of
125I-anti-CD93 mAb make it a promising radiotracer for
imaging NSCLC.
Two NSCLC cell lines of different histological
subtypes were selected for the present study: The human LUAD A549
cell line and the human LUSC SK-MES-1 cell line. Both LUSC and LUAD
are the NSCLC subtypes occurring with the highest prevalence,
accounting for 80–85% of all lung cancer cases (37,38). A
large-scale sequencing study has revealed the genomic differences
between LUAD and LUSC (39). These
two subtypes show a number of different pathological
characteristics, with LUAD growing more slowly than LUSC and
tending to metastasize extensively at an earlier stage (40). A previous study has shown that
patients with LUSC have a poorer prognosis compared with that of
patients with LUAD following surgical resection (41). In addition, 4,124 genes were
differentially expressed in LUAD and LUSC; a higher number of
pathways associated with immune response, cell signal transduction,
metabolism, cell division and cell proliferation were identified in
LUAD compared with LUSC (42).
Herein, the difference in CD93 expression between LUAD and LUSC has
been described, with the levels being higher in A549 cells compared
with those in SK-MES-1 cells. The specificity of a targeted probe
based on CD93 expression in the two different NSCLC xenograft
models was evaluated, and 125I-anti-CD93 mAb revealed a
higher rate of radiotracer retention in A549 tumors compared with
that in SK-MES-1 tumors at all time points. The imaging parameters
and their temporal changes may be essential for tissue
characterization, including histological subtypes of cancers.
Previous studies have demonstrated marked differences in positron
emission tomography-CT parameters according to the histological
subtype of resected NSCLC (43,44). In
addition, various CT perfusion parameters have been reported to
differ between lung cancer subtypes (45,46),
showing inconsistent results (47–52). The
results of the present study may be associated with the higher
angiogenic potential of LUAD, as demonstrated by the higher level
of CD93 expression in A549 cells compared with that in SK-MES-1
cells. These data indicated that CD93 may have the potential to be
used as a biomarker for improving the accurate diagnosis of
borderline lesions that lack specific characterizing features to
distinguish their histological subtype.
Radioimmunoimaging reveals the accumulation of the
target antibody in vivo, where the pharmacokinetic
characteristics of the radiotracers are based on the molecular
weight of the antibody (53). In the
present study, full antibodies with a long circulating half-life
were used. Fab fragments or genetically engineered antibodies may
be an optimal choice for improving the poor pharmacokinetic
characteristics of the radiotracers (54,55). In
addition, the molecular mechanism behind the regulation of CD93
expression in lung cancers of different histological subtype
remains to be further investigated.
In conclusion, 125I-anti-CD93 mAb could
be used for non-invasive radioimmunoimaging of NSCLC based on tumor
cell CD93 expression, particularly for histological subtype
identification. Our results indicate the potential clinical
application of this particular radiotracer for the diagnosis of
CD93-positive tumors.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
The present study was supported by grants from the
National Natural Science Foundation of China (grant no. 81000631),
the National Natural Science Foundation of China (grant no.
81371601) and the Natural Science Foundation of Shandong Province
(grant no. ZR2011HQ045).
Availability of data and materials
The datasets used and analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
WL wrote the manuscript. WL, CZ and DS performed the
experiments. TL and GH designed the study and drafted the
manuscript. WL, SZ and HC analyzed the data.
Ethics approval and consent to
participate
All animal studies were conducted in accordance with
protocols approved by the Animal Care and Use Committee of Shandong
University.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Molina-Pinelo S, Gutierrez G, Pastor MD,
Her-Gueta M, Moreno-Bueno G, Garcia-Carbonero R, Nogal A, Suarez R,
Salinas A, Pozo-Rodriguez F, et al: MicroRNA-dependent regulation
of transcription in non-small cell lung cancer. PLoS One.
9:e905242014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Schwander B, Ravera S, Giuliani G, Nuijten
M and Walzer S: Cost comparison of second-line treatment options
for late stage non-small-cell lung cancer: Cost analysis for Italy.
Clinicoecon Outcomes Res. 4:237–243. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Boch C, Kollmeier J, Roth A,
Stephan-Falkenau S, Misch D, Gruning W, Bauer TT and Mairinger T:
The frequency of EGFR and KRAS mutations in non-small cell lung
cancer (NSCLC): Routine screening data for central Europe from a
cohort study. BMJ Open. 3:e0025602013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Raji OY, Duffy SW, Agbaje OF, Baker SG,
Christiani DC, Cassidy A and Field JK: Predictive accuracy of the
Liverpool Lung Project risk model for stratifying patients for
computed tomography screening for lung cancer: A case-control and
cohort validation study. Ann Intern Med. 157:242–250. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Didkowska J, Wojciechowska U, Mańczuk M
and Łobaszewski J: Lung cancer epidemiology: Contemporary and
future challenges worldwide. Ann Transl Med. 4:1502016. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Sharp A, Bhosle J, Abdelraouf F, Popat S,
O'Brien M and Yap TA: Development of molecularly targeted agents
and immunotherapies in small cell lung cancer. Eur J Cancer.
60:26–39. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kumarakulasinghe NB, van Zanwijk N and Soo
RA: Molecular targeted therapy in the treatment of advanced stage
non-small cell lung cancer (NSCLC). Respirology. 20:370–378. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Spiegel ML, Goldman JW, Wolf BR, Nameth
DJ, Grogan TR, Lisberg AE, Wong DJL, Ledezma BA, Mendenhall MA,
Genshaft SJ, et al: Non-small cell lung cancer clinical trials
requiring biopsies with biomarker-specific results for enrollment
provide unique challenges. Cancer. 123:4800–4807. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Reck M: Pembrolizumab as first-line
therapy for metastatic non-small-cell lung cancer. Immunotherapy.
10:93–105. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Majumder S and Chari ST: Chronic
pancreatitis. Lancet. 387:1957–1966. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Knowles SM and Wu AM: Advances in
immuno-positron emission tomography: Antibodies for molecular
imaging in oncology. J Clin Oncol. 30:3884–3892. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Fu R, Carroll L, Yahioglu G, Aboagye EO
and Miller PW: Antibody fragment and affibody immunoPET imaging
agents: Radiolabelling strategies and applications. ChemMedChem.
13:2466–2478. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Li C, Wen B, Wang L, Feng H, Xia X, Ding
Z, Gao B, Zhang Y and Lan X: 99mTc-labeled single-domain
antibody EG2 in targeting epidermal growth factor receptor. Nucl
Med Commun. 36:452–460. 2015.PubMed/NCBI
|
|
14
|
Mishani E, Abourbeh G, Eiblmaier M and
Anderson CJ: Imaging of EGFR and EGFR tyrosine kinase
overexpression in tumors by nuclear medicine modalities. Curr Pharm
Des. 14:2983–2998. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Peña Y, Perera A and Batista JF:
Immunoscintigraphy and radioimmunotherapy in Cuba: Experiences with
labeled monoclonal antibodies for cancer diagnosis and treatment
(1993–2013). MEDICC Rev. 16:55–60. 2014.
|
|
16
|
Weidner N: Intratumor microvessel density
as a prognostic factor in cancer. Am J Pathol. 147:9–19.
1995.PubMed/NCBI
|
|
17
|
Folkman J: The role of angiogenesis in
tumor growth. Semin Cancer Biol. 3:65–71. 1992.PubMed/NCBI
|
|
18
|
Folkman J: Angiogenesis. Annu Rev Med.
57:1–18. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Ribatti D: History of research on
angiogenesis. Chem Immunol Allergy. 99:1–14. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Greenlee MC, Sullivan SA and Bohlson SS:
Detection and characterization of soluble CD93 released during
inflammation. Inflamm Res. 58:909–919. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Kao YC, Jiang SJ, Pan WA, Wang KC, Chen
PK, Wei HJ, Chen WS, Chang BI, Shi GY and Wu HL: The epidermal
growth factor-like domain of CD93 is a potent angiogenic factor.
PLoS One. 7:e516472012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Langenkamp E, Zhang L, Lugano R, Huang H,
Elhassan TE, Georganaki M, Bazzar W, Loof J, Trendelenburg G,
Essand M, et al: Elevated expression of the C-type lectin CD93 in
the glioblastoma vasculature regulates cytoskeletal rearrangements
that enhance vessel function and reduce host survival. Cancer Res.
75:4504–4516. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Lugano R, Vemuri K, Yu D, Bergqvist M,
Smits A, Essand M, Johansson S, Dejana E and Dimberg A: CD93
promotes β1 integrin activation and fibronectin fibrillogenesis
during tumor angiogenesis. J Clin Invest. 128:3280–3297. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Andersson H, Lindegren S, Bäck T,
Jacobsson L, Leser G and Horvath G: Biokinetics of the monoclonal
antibodies MOv 18, OV 185 and OV 197 labelled with 125I according
to the m-MeATE method or the Iodogen method in nude mice with
ovarian cancer xenografts. Acta Oncol. 38:323–328. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Sun H, Zhan Y, Liang T, Zhang C, Song J,
Han J and Hou G: In vivo Toll-like receptor5 (TLR5) imaging with
radiolabeled anti-TLR5 monoclonal antibody in rapamycin-treated
mouse allogeneic skin transplantation model. Transpl Infect Dis.
17:80–88. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
van Dongen GA, Visser GW, Lub-de Hooge MN,
de Vries EG and Perk LR: Immuno-PET: A navigator in monoclonal
antibody development and applications. Oncologist. 12:1379–1389.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Carmon KS and Azhdarinia A: Application of
immuno-PET in antibody-drug conjugate development. Mol Imaging.
17:15360121188012232018. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Ehlerding EB, England CG, Jiang D, Graves
SA, Kang L, Lacognata S, Barnhart TE and Cai W: CD38 as a PET
imaging target in lung cancer. Mol Pharm. 14:2400–2406. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Carmeliet P and Jain RK: Angiogenesis in
cancer and other diseases. Nature. 407:249–257. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Carmeliet P: Angiogenesis in health and
disease. Nat Med. 9:653–660. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Ribatti D: Judah Folkman, a pioneer in the
study of angiogenesis. Angiogenesis. 11:3–10. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Otrock ZK, Mahfouz RA, Makarem JA and
Shamseddine AI: Understanding the biology of angiogenesis: Review
of the most important molecular mechanisms. Blood Cells Mol Dis.
39:212–220. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Khan KA, Naylor AJ, Khan A, Noy PJ,
Mambretti M, Lodhia P, Athwal J, Korzystka A, Buckley CD, Willcox
BE, et al: Multimerin-2 is a ligand for group 14 family C-type
lectins CLEC14A, CD93 and CD248 spanning the endothelial pericyte
interface. Oncogene. 36:6097–6108. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Greenlee MC, Sullivan SA and Bohlson SS:
CD93 and related family members: Their role in innate immunity.
Curr Drug Targets. 9:130–138. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Bao L, Tang M, Zhang Q, You B, Shan Y, Shi
S, Li L, Hu S and You Y: Elevated expression of CD93 promotes
angiogenesis and tumor growth in nasopharyngeal carcinoma. Biochem
Biophys Res Commun. 476:467–474. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Orlandini M, Galvagni F, Bardelli M,
Rocchigiani M, Lentucci C, Anselmi F, Zippo A, Bini L and Oliviero
S: The characterization of a novel monoclonal antibody against CD93
unveils a new antiangiogenic target. Oncotarget. 5:2750–2760. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Cancer Genome Atlas Research Network, .
Comprehensive molecular profiling of lung adenocarcinoma. Nature.
511:543–550. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Cancer Genome Atlas Research Network, .
Comprehensive genomic characterization of squamous cell lung
cancers. Nature. 489:519–525. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Campbell JD, Alexandrov A, Kim J, Wala J,
Berger AH, Pedamallu CS, Shukla SA, Guo G, Brooks AN, Murray BA, et
al: Distinct patterns of somatic genome alterations in lung
adenocarcinomas and squamous cell carcinomas. Nat Genet.
48:607–616. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Hoda SA and Cheng E: Robbins basic
pathology. Am J Clin Pathol. 2017. View Article : Google Scholar
|
|
41
|
Kawase A, Yoshida J, Ishii G, Nakao M,
Aokage K, Hishida T, Nishimura M and Nagai K: Differences between
squamous cell carcinoma and adenocarcinoma of the lung: Are
adenocarcinoma and squamous cell carcinoma prognostically equal?
Jpn J Clin Oncol. 42:189–195. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Liu J, Yang XY and Shi WJ: Identifying
differentially expressed genes and pathways in two types of
non-small cell lung cancer: Adenocarcinoma and squamous cell
carcinoma. Genet Mol Res. 13:95–102. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Schuurbiers OC, Meijer TW, Kaanders JH,
Looigen-Salamon MG, de Geus-Oei LF, van der Drift MA, van der
Heijden EH, Oyen WJ, Visser EP, Span PN and Bussink J: Glucose
metabolism in NSCLC is histology-specific and diverges the
prognostic potential of 18FDG-PET for adenocarcinoma and
squamous cell carcinoma. J Thorac Oncol. 9:1485–1493. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Koh YW, Lee SJ and Park SY: Differential
expression and prognostic significance of GLUT1 according to
histologic type of non-small-cell lung cancer and its association
with volume-dependent parameters. Lung Cancer. 104:31–37. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Graves EE, Maity A and Le QT: The tumor
microenvironment in non-small-cell lung cancer. Semin Radiat Oncol.
20:156–163. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Shi J, Schmid-Bindert G, Fink C, Sadurski
S, Apfaltrer P, Poilz LR, Liu B, Haberland U, Klotz E, Zhou C, et
al: Dynamic volume perfusion CT in patients with lung cancer:
Baselineperfusion characteristics of different histological
subtypes. Eur J Radiol. 82:e894–e900. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Ma SH, Xu K, Xiao ZW, Wu M, Sun ZY, Wang
ZX, Hu ZG, Dai X, Han MJ and Li YG: Peripheral lung cancer:
Relationship between multi-slice spiral CT perfusion imaging and
tumor angiogenesis and cyclin D1 expression. Clin Imaging.
31:165–177. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Li Y, Yang ZG, Chen TW, Chen HJ, Sun JY
and Lu YR: Peripheral lung carcinoma: Correlation of angiogenesis
and first-pass perfusion parameters of 64-detector row CT. Lung
Cancer. 61:44–53. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Sauter AW, Winterstein S, Spira D, Hetzel
J, Schulze M, Mueller M, Pfannenberg C, Claussen CD, Klotz E, Hann
von Weyhern C and Horger MS: Multifunctional profiling of non-small
cell lung cancer using 18F-FDG PET/CT and volume
perfusion CT. J Nucl Med. 53:521–529. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
van Elmpt W, Zegers CML, Reymen B, Even
AJG, Dingemans AC, Oellers M, Wildberger JE, Mottaghy FM, Das M,
Troost EGC and Lambin P: Multiparametric imaging of patient and
tumor heterogeneity in non-small-cell lung cancer: Quantification
of tumor hypoxia, metabolism and perfusion. Eur J Nucl Med Mol
Imaging. 43:240–248. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Nakano S, Gibo J, Fukushima Y, Kaira K,
Sunaga N, Taketomi-Takahashi A, Tsushima Y and Mori M: Perfusion
evaluation of lung cancer: Assessment using dual-input perfusion
computed tomography. J Thorac Imaging. 28:253–262. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Spira D, Neumeister H, Spira SM, Hetzel J,
Spengler W, von Weyhern CH and Horger M: Assessment of tumor
vascularity in lung cancer using volume perfusion CT (VPCT) with
histopathologic comparison: A further step toward an individualized
tumor characterization. J Comput Assist Tomogr. 37:15–21. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Kang F, Wang Z, Li G, Wang S, Liu D, Zhang
M, Zhao M, Yang W and Wang J: Inter-heterogeneity and
intra-heterogeneity of αvβ3 in non-small cell lung cancer and small
cell lung cancer patients as revealed by 68Ga-RGD2 PET
imaging. Eur J Nucl Med Mol Imaging. 44:1520–1528. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Jing S, He Y, He Y, Wang L, Jia J, Shan X,
Liu S, Tang M, Peng Z and Liu X: Imaging potential evaluation of
fab derived from the anti-EGFRvIII monoclonal antibody 4G1. Radiat
Res. 190:194–203. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Shi S, Orbay H, Yang Y, Graves SA, Nayak
TR, Hong H, Hernandez R, Luo H, Goel S, Theuer CP, et al: PET
imaging of abdominal aortic aneurysm with 64Cu-labeled
anti-CD105 antibody fab fragment. J Nucl Med. 56:927–932. 2015.
View Article : Google Scholar : PubMed/NCBI
|