Introduction
Small cell lung cancer (SCLC) is a highly malignant
neuroendocrine tumor with a 5-year survival rate of <5%. It
accounts for 10–15% of all lung cancers, with more than two-thirds
of cases classified as extensive-stage SCLC (ES-SCLC) (1). The brain is a common site of
metastasis in ES-SCLC; >50% of patients with ES-SCLC develop
brain metastases (BMs) within 2 years, and BMs are observed in up
to 80% of patients at autopsy (2).
Immunological drugs can prolong patient survival but
do not reduce the risk of BM (3).
Once BM occurs, it markedly impacts patient survival and quality of
life. As most chemotherapeutic drugs cannot cross the blood-brain
barrier, there are limited options for preventing BM (4). Therefore, the role of prophylactic
cranial irradiation (PCI) should not be overlooked.
Currently, there are controversies regarding the
benefits of PCI in patients with ES-SCLC: A European Organization
for Research and Treatment of Cancer study indicated that PCI is
effective in reducing the risk of BM and prolonging the 1-year
overall survival (OS) (5). However,
a previous phase III clinical trial of patients with ES-SCLC
without BMs used MRI to confirm PCI decreases the incidence of BM
but does not increase survival (6).
In addition, neurocognitive dysfunction associated with PCI may
affect quality of life (7–9). The hypothesis that PCI using
hippocampal avoidance decreases cognitive impairment is
controversial (10–12). Regular MRI monitoring of BM combined
with salvage stereotactic radiosurgery may replace PCI (6,13,14).
Therefore, it is essential to screen patients who
are at high risk of BM for PCI to avoid overtreatment, which may
lead to cognitive dysfunction and waste of medical resources
(6,7). The current National Comprehensive
Cancer Network guidelines recommend PCI for patients with ES-SCLC
who have an efficacy evaluations of partial/complete response
(PR/CR) following standard treatment, provided they are under MRI
surveillance (15). Nevertheless,
it remains unclear which patients are likely to benefit from PCI,
making the decision to perform this procedure challenging.
Previous studies (16,17)
have evaluated the risk factors for the development of BM in
patients with ES-SCLC; however, the enrollment population was all
patients with ES-SCLC, and, to the best of our knowledge, few
analyses (16–18) have been conducted separately for the
population with PR/CR evaluation. A retrospective study in 2011
reported that weight loss, response to chemotherapy were
independent predictors of BM in patients with ES-SCLC (16). Chung et al (17) demonstrated that extrathoracic
metastasis, fluorodeoxyglucose positron emission tomography bone or
splenic hypermetabolism and the neutrophil-to-lymphocyte ratio
(NLR) are associated with the risk of BM in patients with ES-SCLC.
However, neither of the aforementioned retrospective studies
analyzed the risk factors for BM in patients exhibiting good
efficacy.
The present study aimed to investigate the risk
factors for BM in patients with MRI-confirmed baseline absence of
BM in ES-SCLC, after achieving PR/CR as assessed by treatment
efficacy. Furthermore, the study aimed to establish a nomogram
model to facilitate decision-making for PCI.
Materials and methods
Study design and participants
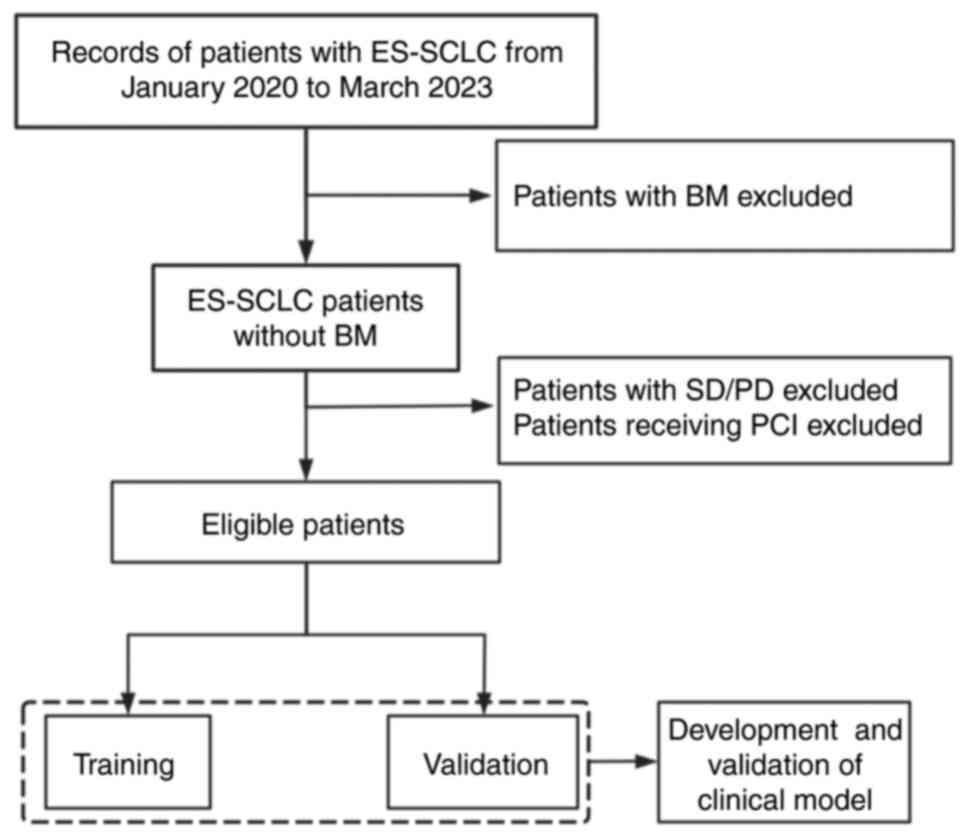
The present retrospective study included patients
newly diagnosed with ES-SCLC between January 2020 and February 2023
at Shandong Cancer Hospital (Jinan, China; Fig. 1). The inclusion criteria were as
follows: i) SCLC verified by pathology; ii) ES-SCLC confirmed by
imaging prior to treatment(MRI, ultrasound, Computed Tomography,
Positron Emission Tomography/Computed tomography and Emission
Computed Tomography), with no BM established by MRI; iii) receipt
of at least four cycles of standard first-line platinum-based
chemotherapy; and iv) CR or PR after 4–6 cycles. The exclusion
criteria were as follows: i) Patients who had received antitumor
therapy; ii) patients who had not undergone a brain MRI; iii)
patients who had received PCI therapy; iv) patients with follow-up
periods <9 months; and v) patients with a history of other
primary malignant tumors. The clinical stage was classified
according to the American Joint Committee on Cancer guidelines (8th
edition) (19), and responses were
evaluated using Response Evaluation Criteria in Solid Tumors
(version 1.1) (20). Overall, 156
of 727 patients with ES-SCLC met the criteria, with a median age of
63 years (IQR, 56–68 years) and were randomly divided into training
(n=109) and validation (n=47) cohorts in a 7:3 ratio using the
sample function in R software version 4.0.3(r-project.org/). A prediction model was constructed
for the training cohort, whereas the validation cohort was
internally validated using receiver operating characteristic,
calibration curves, and decision curve analysis. The requirement
for ethics approval and informed consent was waived by the Ethics
Committee of Shandong Cancer Hospital (Jinan, China).
Selection of potential predictors
Medical records of baseline clinical characteristics
were retrieved and reviewed using an electronic medical record
system. Patient demographics, including age, sex and smoking
history, were also documented. Medical records contained
information on hematological parameters, including carcinoembryonic
antigen, neuron-specific enolase (NSE), pro-gastrin-releasing
peptide, lactate dehydrogenase (LDH), NLR and platelet-lymphocyte
ratio (PLR). Clinical characteristics, such as T, N and metastasis
stage (19), were also extracted
from medical records. Baseline metastatic status, specific
parameters (NLR and PLR) and treatment status (mode of treatment,
chemotherapy cycle and thoracic radiation therapy) were considered,
and all unordered variables were transformed into categorical
variables. All indicators were extracted from the initial
diagnostic records.
Diagnosis of BM and definition of
intracranial progression-free survival (iPFS)
The occurrence of BM was the primary outcome of the
present study. iPFS was defined as the interval from the initial
pathological diagnosis (MRI was used to confirm lack of BM) to the
occurrence of BM or the date of the last follow-up examination. iP
was diagnosed based on imaging results (primarily brain MRI);
however, if BM symptoms manifested before the imaging, the time of
appearance was given precedence. Patients were instructed to
undergo brain MRI (preferred) or computed tomography every 3–4
months following the conclusion of chemotherapy. From the second
year onward, cranial imaging was performed every 6 months. The end
point follow-up was May 2024 and the median follow-up time was 18.7
months (range, 4.8–41 months).
Statistical analysis
SPSS 27.0 software (IBM Corp.) was used to analyze
the data. In the training cohort, univariate analysis was used to
explore the relationship between the potential predictors and iPFS.
The assessment of between-group differences was performed using
χ2 or Fisher's exact tests. Log-rank tests were used to
compare different groups for univariate analyses. Factors with a
P-value <0.05 were included in multivariate Cox regression
analysis to evaluate the independent risk factors influencing iPFS.
A nomogram was constructed based on risk factors identified through
multifactorial analysis by R software version 4.0.3 (r-project.org/). The total score was calculated for
all individuals in the training cohort, and the data were
quantitatively validated using the area under the receiver
operating characteristic, calibration curve and decision curve. The
Kaplan-Meier method was used to calculate OS. We performed
univariate and multivariate analysis using the Cox proportional
hazards models to identify possible predictors of prognosis. All
tests were two-sided. P<0.05 was considered to indicate a
statistically significant difference.
Results
Patient characteristics
A total of 156 patients were included in the present
study. Analysis of the baseline characteristics is shown in
Table I. Overall, 123 patients
(78.85%) were male and 33 (21.15%) were female. The median age was
63 years, with 63 (40.38%) patients aged >65 years and 93
(59.62%) aged ≤65 years. A total of 54 patients (34.62%) exhibited
non-oligometastatic status(extensive metastasis beyond
oligometastasis), defined as the presence of >3 metastatic
organs and >5 metastatic lesions. There was no significant
difference in risk factors between the training and validation sets
(all P>0.05). The median iPFS was 15.6 months (95% CI,
9.81–21.39 months), and the cumulative incidence of BM was 35% at 9
months, 44% at 12 months and 60% at 24 months. The median survival
and follow-up times were 20.70 months (95% CI, 17.58–23.82 months)
and 23.63 months (95% CI, 22.29–24.98 months), respectively (data
not shown).
 | Table I.Patient clinical and pathological
characteristics. |
Table I.
Patient clinical and pathological
characteristics.
| Variable | Total, n (%)
(n=156) | Training, n (%)
(n=109) | Validation, n (%)
(n=47) | χ2 | P-value |
|---|
| Sex |
|
|
| 0.00 | 0.980 |
|
Female | 33 (21.15) | 23 (21.10) | 10 (21.28) |
|
|
|
Male | 123 (78.85) | 86 (78.90) | 37 (78.72) |
|
|
| Age, years |
|
|
| 0.13 | 0.717 |
|
>65 | 63 (40.38) | 43 (39.45) | 20 (42.55) |
|
|
|
≤65 | 93 (59.62) | 66 (60.55) | 27 (57.45) |
|
|
| Smoking status |
|
|
| 0.10 | 0.755 |
| No | 66 (42.31) | 47 (43.12) | 19 (40.43) |
|
|
|
Yes | 90 (57.69) | 62 (56.88) | 28 (59.57) |
|
|
| T
classification |
|
|
| 0.00 | 0.975 |
| T1,
T2 | 70 (44.87) | 49 (44.95) | 21 (44.68) |
|
|
| T3,
T4 | 86 (55.13) | 60 (55.05) | 26 (55.32) |
|
|
| N
classification |
|
|
| 1.12 | 0.289 |
| N1,
N2 | 63 (40.38) | 47 (43.12) | 16 (34.04) |
|
|
| N3 | 93 (59.62) | 62 (56.88) | 31 (65.96) |
|
|
| CEA (ng/ml) |
|
|
| 0.31 | 0.575 |
|
<5 | 91 (58.33) | 62 (56.88) | 29 (61.70) |
|
|
| ≥5 | 65 (41.67) | 47 (43.12) | 18 (38.30) |
|
|
| NSE (ng/ml) |
|
|
| 1.04 | 0.308 |
|
<17.5 | 23 (14.74) | 14 (12.84) | 9 (19.15) |
|
|
|
≥17.5 | 133 (85.26) | 95 (87.16) | 38 (80.85) |
|
|
| Pro-GRP
(pg/ml) |
|
|
| 0.14 | 0.713 |
|
<50 | 13 (8.33) | 8 (7.34) | 5 (10.64) |
|
|
|
≥50 | 143 (91.67) | 101 (92.66) | 42 (89.36) |
|
|
| D-dimer (mg/l) |
|
|
| 2.31 | 0.129 |
|
<0.5 | 64 (41.03) | 49 (44.95) | 15 (31.91) |
|
|
|
≥0.5 | 92 (58.97) | 60 (55.05) | 32 (68.09) |
|
|
| LDH (U/l) |
|
|
| 0.96 | 0.328 |
|
<245 | 79 (50.64) | 58 (53.21) | 21 (44.68) |
|
|
|
≥245 | 77 (49.36) | 51 (46.79) | 26 (55.32) |
|
|
| NLR |
|
|
| 0.00 | >0.999 |
|
<1.37 | 11 (7.05) | 8 (7.34) | 3 (6.38) |
|
|
|
≥1.37 | 145 (92.95) | 101 (92.66) | 44 (93.62) |
|
|
| PLR |
|
|
| 0.01 | 0.920 |
|
<121 | 39 (25.00) | 27 (24.77) | 12 (25.53) |
|
|
|
≥121 | 117 (75.00) | 82 (75.23) | 35 (74.47) |
|
|
|
Oligometastasis |
|
|
| 0.07 | 0.789 |
| No | 54 (34.62) | 37 (33.94) | 17 (36.17) |
|
|
|
Yes | 102 (65.38) | 72 (66.06) | 30 (63.83) |
|
|
| Liver
metastasis |
|
|
| 0.01 | 0.921 |
| No | 102 (65.38) | 71 (65.14) | 31 (65.96) |
|
|
|
Yes | 54 (34.62) | 38 (34.86) | 16 (34.04) |
|
|
| Bone
metastasis |
|
|
| 0.00 | 0.963 |
| No | 100 (64.10) | 70 (64.22) | 30 (63.83) |
|
|
|
Yes | 56 (35.90) | 39 (35.78) | 17 (36.17) |
|
|
| Adrenal
metastasis |
|
|
| 0.43 | 0.514 |
| No | 128 (82.05) | 88 (80.73) | 40 (85.11) |
|
|
|
Yes | 28 (17.95) | 21 (19.27) | 7 (14.89) |
|
|
| Thoracic
radiotherapy |
|
|
| 0.66 | 0.418 |
| No | 92 (58.97) | 62 (56.88) | 30 (63.83) |
|
|
|
Yes | 64 (41.03) | 47 (43.12) | 17 (36.17) |
|
|
| Treatment mode |
|
|
| 0.25 | 0.614 |
|
ChT-alone | 39 (25.00) | 26 (23.85) | 13 (27.66) |
|
|
| IO +
ChT | 117 (75.00) | 83 (76.15) | 34 (72.34) |
|
|
| Chemotherapy
cycles |
|
|
| 0.74 | 0.389 |
| 4 | 18 (11.54) | 11 (10.09) | 7 (14.89) |
|
|
|
>4 | 138 (88.46) | 98 (89.91) | 40 (85.11) |
|
|
| Immunotherapy
cycles |
|
|
| 0.34 | 0.561 |
|
<6 | 108 (69.23) | 77 (70.64) | 31 (65.96) |
|
|
| ≥6 | 48 (30.77) | 32 (29.36) | 16 (34.04) |
|
|
| BM |
|
|
| 2.15 | 0.209 |
| No | 77 (49.36) | 58 (53.21) | 19 (40.43) |
|
|
|
Yes | 79 (50.64) | 51 (46.79) | 28 (59.57) |
|
|
Factors influencing BM
Univariate analysis of the training cohort
demonstrated that patients with non-oligometastases exhibited a
heightened risk of BM compared with those with oligometastases
[hazard ratio (HR), 0.35; 95% CI, 0.19–0.61; P<0.001; Table II]. Additionally, male patients had
a higher risk of BM compared with female patients (HR, 2.62; 95%
CI, 1.12–6.15; P=0.026). Furthermore, patients with liver
metastases at baseline exhibited a heightened risk of BM compared
with those without liver metastasis (HR, 1.98; 95% CI, 1.14–3.45;
P=0.016). Patients with adrenal metastases at baseline also had a
higher risk of BM compared with those without adrenal metastasis
(HR, 3.03; 95% CI, 1.67–5.48; P<0.001). Cox multivariate
analysis (Table III) demonstrated
that absence of oligometastasis (HR, 0.35; 95% CI, 0.14–0.85;
P=0.021), male sex (HR, 2.48; 95% CI, 1.05–5.85; P=0.038) and
baseline adrenal metastasis (HR, 2.85; 95% CI, 1.54–5.21;
P<0.001) were independent risk factors for BM.
| Table II.Univariate analysis predicting
intracranial progression-free survival in patients without
prophylactic cranial irradiation. |
Table II.
Univariate analysis predicting
intracranial progression-free survival in patients without
prophylactic cranial irradiation.
| Variable | P-value | HR (95% CI) |
|---|
| Sex |
|
|
|
Female |
| 1.00
(reference) |
|
Male | 0.026 | 2.62
(1.12–6.15) |
| Age, years |
|
|
|
>65 |
| 1.00
(reference) |
|
≤65 | 0.558 | 1.19
(0.67–2.10) |
| Smoking status |
|
|
| No |
| 1.00
(reference) |
|
Yes | 0.064 | 1.73
(0.97–3.08) |
| T
classification |
|
|
| T1,
T2 |
| 1.00
(reference) |
| T3,
T4 | 0.856 | 0.95
(0.55–1.64) |
| N
classification |
|
|
| N1,
N2 |
| 1.00
(reference) |
| N3 | 0.906 | 1.03
(0.60–1.78) |
| CEA (ng/ml) |
|
|
|
<5 |
| 1.00
(reference) |
| ≥5 | 0.856 | 0.95
(0.55–1.64) |
| NSE (ng/ml) |
|
|
|
<17.5 |
| 1.00
(reference) |
|
≥17.5 | 0.268 | 0.69
(0.35–1.34) |
| Pro-GRP
(pg/ml) |
|
|
|
<50 |
| 1.00
(reference) |
|
≥50 | 0.202 | 2.51
(0.61–10.32) |
| D-dimer (mg/l) |
|
|
|
<0.5 |
| 1.00
(reference) |
|
≥0.5 | 0.113 | 1.57
(0.90–2.73) |
| LDH (U/l) |
|
|
|
<245 |
| 1.00
(reference) |
|
≥245 | 0.173 | 1.46
(0.85–2.51) |
| NLR |
|
|
|
<1.37 |
| 1.00
(reference) |
|
≥1.37 | 0.224 | 2.40
(0.58–9.88) |
| PLR |
|
|
|
<121 |
| 1.00
(reference) |
|
≥121 | 0.222 | 1.54
(0.77–3.07) |
|
Oligometastasis |
|
|
| No |
| 1.00
(reference) |
|
Yes | <0.001 | 0.35
(0.19–0.61) |
| Liver
metastasis |
|
|
| No |
| 1.00
(reference) |
|
Yes | 0.016 | 1.98
(1.14–3.45) |
| Bone
metastasis |
|
|
| No |
| 1.00
(reference) |
|
Yes | 0.175 | 1.47
(0.84–2.56) |
| Adrenal
metastasis |
|
|
| No |
| 1.00
(reference) |
|
Yes | <0.001 | 3.03
(1.67–5.48) |
| Thoracic
radiotherapy |
|
|
| No |
| 1.00
(reference) |
|
Yes | 0.157 | 1.48
(0.86–2.55) |
| Treatment mode |
|
|
|
ChT-alone |
| 1.00
(reference) |
| IO +
ChT | 0.556 | 0.83
(0.45–1.53) |
| Chemotherapy
cycles |
|
|
|
>4 |
| 1.00
(reference) |
| ≤4 | 0.162 | 0.43
(0.14–1.40) |
| Immunotherapy
cycles |
|
|
|
<6 |
| 1.00
(reference) |
| ≥6 | 0.829 | 0.93
(0.50–1.73) |
| Table III.Multivariate analysis predicting
intracranial progression-free survival. |
Table III.
Multivariate analysis predicting
intracranial progression-free survival.
| Variable | HR (95% CI) | P-value |
|---|
| Sex |
|
|
|
Female | 1.00
(reference) |
|
|
Male | 2.48
(1.05–5.85) | 0.038 |
|
Oligometastases |
|
|
| No | 1.00
(reference) |
|
|
Yes | 0.35
(0.14–0.85) | 0.021 |
| Liver
metastasis |
|
|
| No | 1.00
(reference) |
|
|
Yes | 1.00
(0.42–2.38) | 0.997 |
| Adrenal
metastasis |
|
|
| No | 1.00
(reference) |
|
|
Yes | 2.85
(1.54–5.21) | <0.001 |
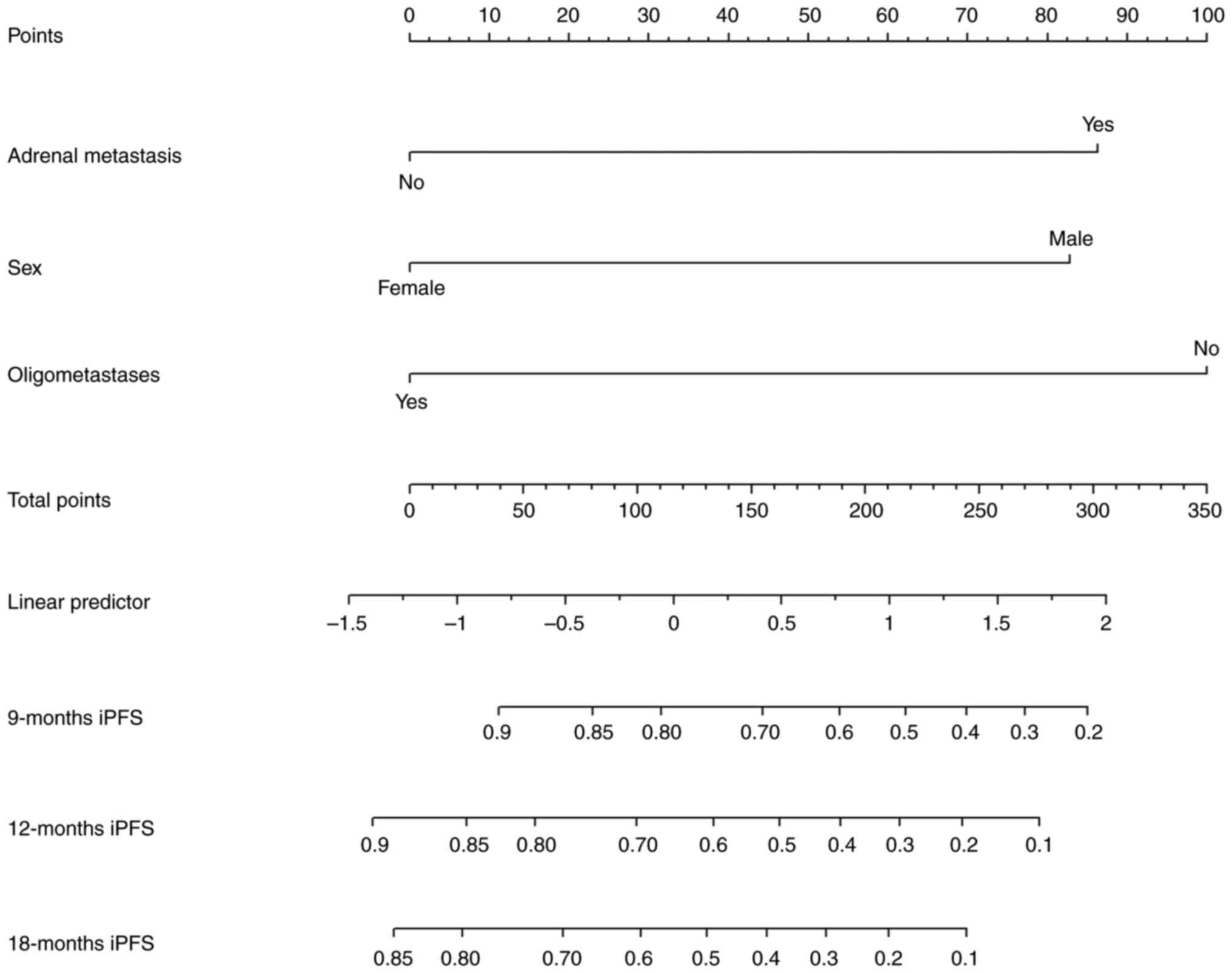
Establishment of the nomogram
A nomogram was constructed using the three risk
factors identified by Cox multifactorial analysis with P-values
<0.05. This nomogram was used to predict the probability of iPFS
at 9, 12 and 18 months in patients with baseline ES-SCLC without BM
who achieved PR/CR efficacy on standard treatment and did not
receive PCI. The risk associated with each factor was visualized in
the nomogram (Fig. 2). The
individual scores for the risk factors of each patient were summed
to obtain an overall score, which corresponded to the likelihood of
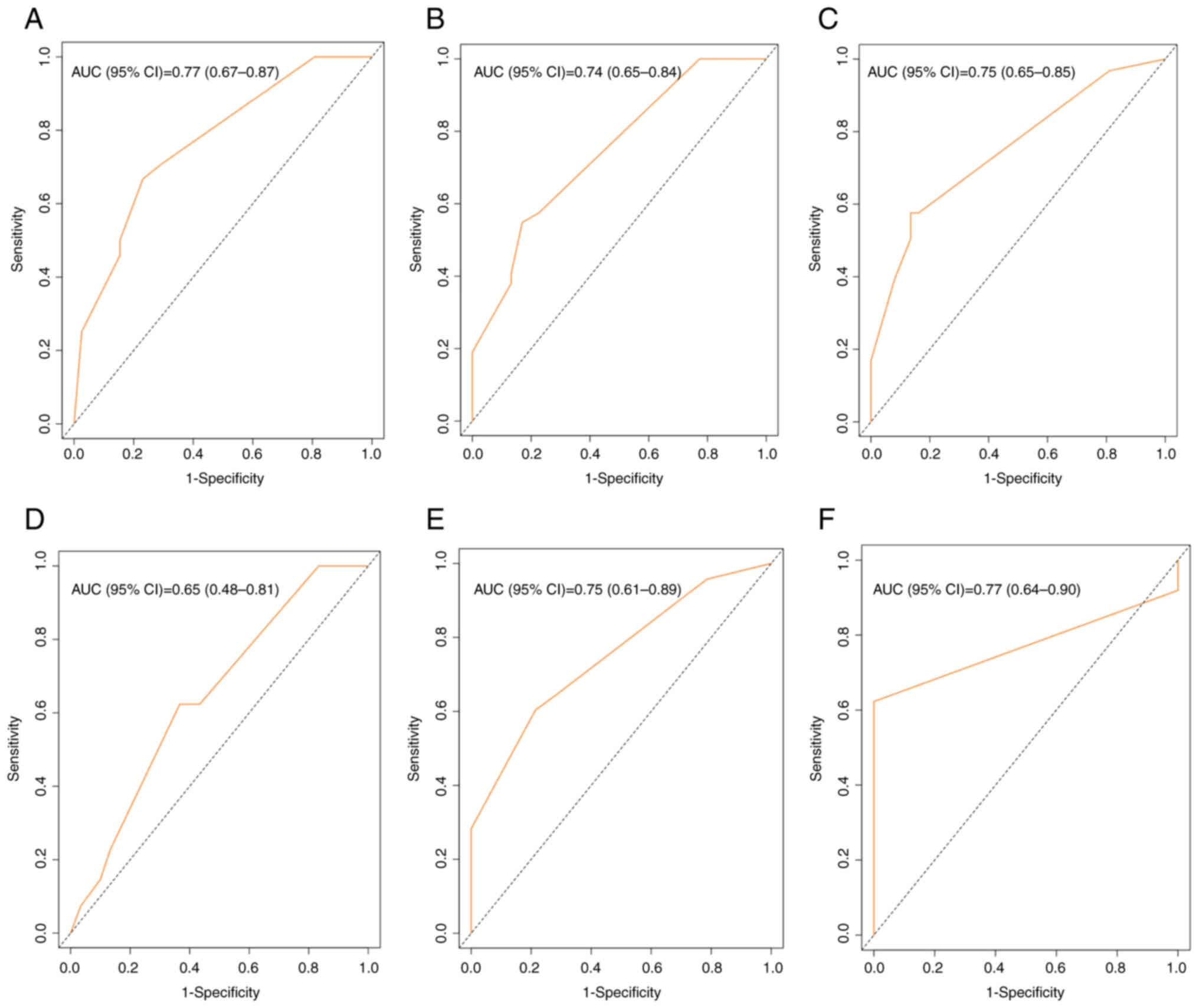
different iPFS outcomes. The areas under the receiver operating
characteristic curve for the 9-, 12- and 18-month iPFS in the
training cohort were 0.77 (95% CI, 0.67–0.87), 0.74 (95% CI,
0.65–0.84) and 0.75 (95% CI, 0.65–0.85), respectively (Fig. 3). Similarly, good results were
obtained in the validation cohort, with the areas under the curve
for the 9-, 12- and 18-month iPFS being 0.65 (95% CI, 0.48–0.81),
0.75 (95% CI, 0.61–0.89) and 0.77 (95% CI, 0.64–0.90), respectively
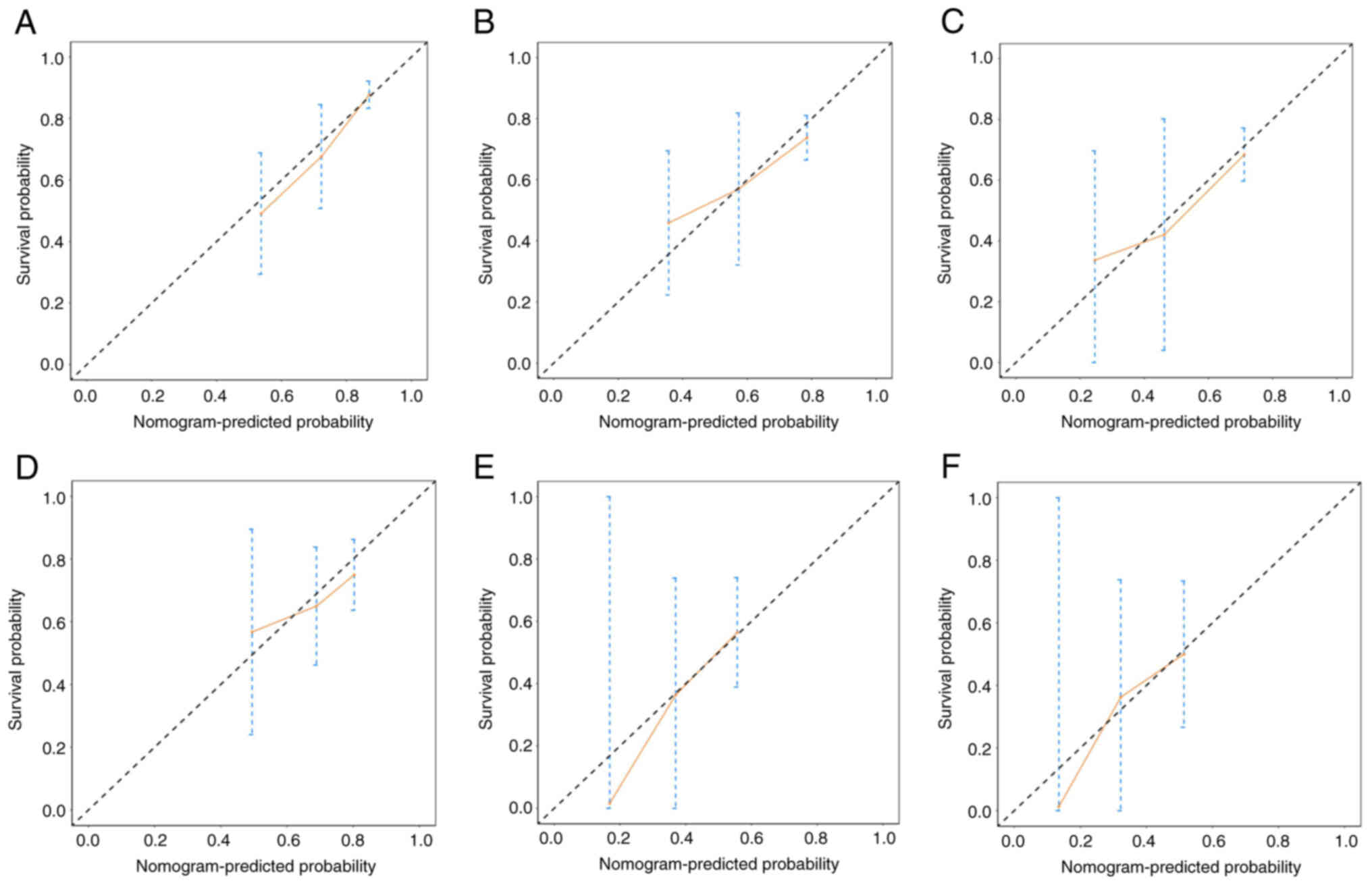
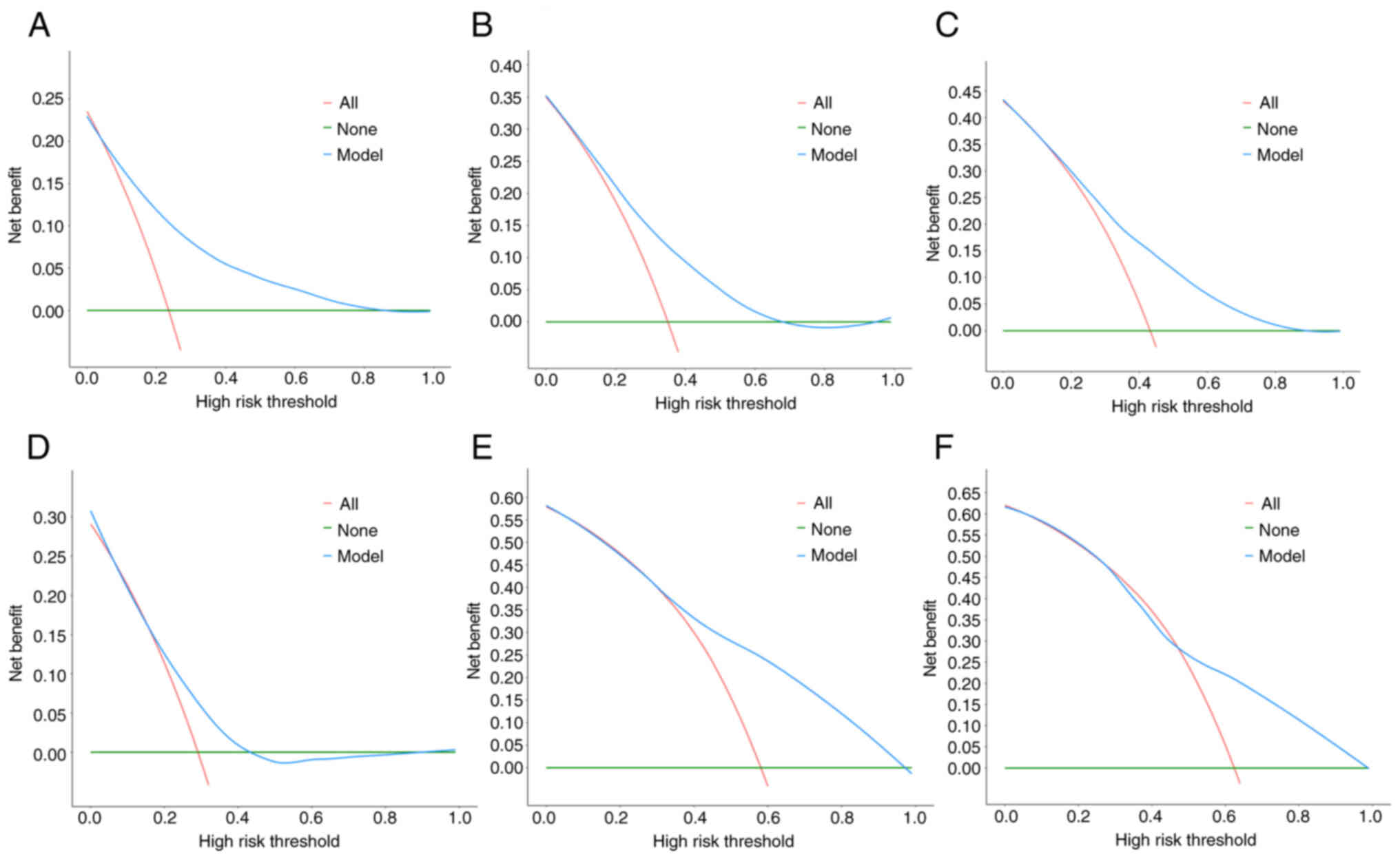
(Fig. 3). The calibration and
decision curves of this nomogram in the training and validation
cohorts demonstrated good agreement (Figs. 4 and 5).
Survival analysis
The univariate analysis revealed that age, N
classification, oligometastasis, NSE, D-dimer and LDH levels,
liver, bone and adrenal metastases, and thoracic radiotherapy, were
significantly associated with OS (Table IV). These factors were included in
the multivariate analysis, which demonstrated that oligometastasis
(HR, 0.38; 95% CI, 0.18–0.81; P=0.012) was a favorable prognostic
factor for OS. Conversely, higher N classification (HR, 2.08; 95%
CI, 1.27–3.40; P=0.003) and adrenal metastases (HR, 1.80; 95% CI,
1.08–3.02; P=0.025) were unfavorable prognostic factors for OS.
| Table IV.Multivariate analysis of factors
influencing overall survival of all patients. |
Table IV.
Multivariate analysis of factors
influencing overall survival of all patients.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Variable | χ2 | P-value | HR (95% CI) | P-value |
|---|
| Sex |
|
|
|
|
|
Female |
|
|
|
|
|
Male | 0.28 | 0.600 |
|
|
| Age, years |
|
|
|
|
|
>65 |
|
| 1.00
(reference) |
|
|
≤65 | 4.84 | 0.028 | 0.65
(0.41–1.03) | 0.066 |
| Smoking status |
|
|
|
|
| No |
|
|
|
|
|
Yes | 1.74 | 0.187 |
|
|
| T
classification |
|
|
|
|
| T1,
T2 |
|
|
|
|
| T3,
T4 | 2.67 | 0.102 |
|
|
| N
classification |
|
|
|
|
| N1,
N2 |
|
| 1.00
(reference) |
|
| N3 | 8.12 | 0.004 | 2.08
(1.27–3.40) | 0.003 |
|
Oligometastasis |
|
|
|
|
| No |
|
| 1.00
(reference) |
|
|
Yes | 30.03 | <0.001 | 0.38
(0.18–0.81) | 0.012 |
| CEA (ng/ml) |
|
|
|
|
|
<5 |
|
|
|
|
| ≥5 | 0.50 | 0.482 |
|
|
| NSE (ng/ml) |
|
|
|
|
|
<17.5 |
|
| 1.00
(reference) |
|
|
≥17.5 | 6.06 | 0.014 | 1.95
(0.86–4.42) | 0.108 |
| Pro-GRP
(pg/ml) |
|
|
|
|
|
<50 |
|
|
|
|
|
≥50 | 0.84 | 0.360 |
|
|
| D-dimer (mg/l) |
|
|
|
|
|
<0.5 |
|
| 1.00
(reference) |
|
|
≥0.5 | 6.77 | 0.009 | 1.44
(0.90–2.29) | 0.127 |
| LDH (U/l) |
|
|
|
|
|
<245 |
|
| 1.00
(reference) |
|
|
≥245 | 5.82 | 0.016 | 1.00
(0.62–1.60) | 0.999 |
| NLR |
|
|
|
|
|
<1.37 |
|
|
|
|
|
≥1.37 | 1.42 | 0.234 |
|
|
| PLR |
|
|
|
|
|
<121 |
|
|
|
|
|
≥121 | 0.00 | 0.992 |
|
|
| Liver
metastasis |
|
|
|
|
| No |
|
| 1.00
(reference) |
|
|
Yes | 8.44 | 0.004 | 1.02
(0.56–1.85) | 0.949 |
| Bone
metastasis |
|
|
|
|
| No |
|
| 1.00
(reference) |
|
|
Yes | 9.50 | 0.002 | 1.12
(0.62–2.03) | 0.711 |
| Adrenal
metastasis |
|
|
|
|
| No |
|
| 1.00
(reference) |
|
|
Yes | 5.63 | 0.018 | 1.80
(1.08–3.02) | 0.025 |
| Thoracic
radiotherapy |
|
|
|
|
| No |
|
| 1.00
(reference) |
|
|
Yes | 3.92 | 0.048 | 0.62
(0.38–1.00) | 0.051 |
| Treatment mode |
|
|
|
|
|
ChT-alone |
|
|
|
|
| IO +
ChT | 0.06 | 0.808 |
|
|
| Chemotherapy
cycles |
|
|
|
|
|
>4 |
|
|
|
|
| ≤4 | 0.15 | 0.701 |
|
|
| Immunotherapy
cycles |
|
|
|
|
|
<6 |
|
|
|
|
| ≥6 | 1.08 | 0.299 |
|
|
Discussion
SCLC is aggressive and progresses rapidly, with a
2-year BM incidence of 60–80% (21). BM poses a notable burden to the
patient and requires extensive care (22). Therefore, early intervention for BM
is necessary. The current National Comprehensive Cancer Network
guidelines recommend that only patients with good treatment
efficacy are considered for PCI (14). Therefore, only patients with good
efficacy ratings were included in the present study. However, the
selection of PCI has been approached with caution in clinical
practice; only 14 (4.7%) out of 297 patients with ES-SCLC without
prior BM at Shandong Cancer Hospital received PCI during the
present study period. An exploratory study by Ankolekar et
al (23) analyzed the shared
decision-making process among patients with ES-SCLC prepared to
undergo PCI and the physician perceptions of its benefits, the
results of the study revealed that most patients want better
information to help make PCI decisions. Although prior research has
addressed BM risk factors in SCLC, much focus has been on
limited-stage SCLC (LD-SCLC) (18,24–28).
Conversely, studies (15–16,27–29)
targeting the ES-SCLC population have not examined those who were
effectively treated and do not provide actionable guidance for
patients recommended for PCI by the current guidelines.
Consequently, the present study explored the BM risk factors in
this subgroup to offer more tailored decision-making
recommendations regarding PCI.
To the best of our knowledge, the present study was
the first to assess risk factors for BM in ES-SCLC in patients with
PR/CR following treatment and without PCI. Furthermore, a nomogram
visualization model was developed. Male sex, non-oligometastatic
status and baseline adrenal metastasis were independent risk
factors for BM. The nomogram validation results demonstrated good
concordance between the predicted and observed values, potentially
aiding clinicians in deciding on PCI for patients with ES-SCLC.
Patients with non-oligometastases were more susceptible to BM
compared with those with oligometastases. This disparity may stem
from the lower systemic tumor burden in oligometastatic patients,
which may result in reduced recurrence and metastasis
post-treatment, thereby diminishing the risk of BM (28). By contrast, patients with extensive
metastasis (non-oligometastatic), despite achieving a favorable
response to antitumor therapy (with treatment efficacy reaching
PR/CR), face a higher risk due to their inherent widespread
metastatic burden. Therefore, the likelihood of recurrence and
metastasis is higher in these patients (29). Chung et al (17) reached a similar conclusion,
suggesting that extensive systemic metastases are linked to
systemic inflammation and potentially associated with BM. A
retrospective study by Oliver et al (30) determined that the presence of ≥3
extrathoracic metastatic sites markedly increased the risk of
developing BM in patients with ES-SCLC. Furthermore, Bang et
al (29) identified
extrathoracic metastasis as an independent predictor of a shorter
iPFS. However, differing from the present study, the aforementioned
studies did not evaluate the number of metastatic sites to assess
oligometastatic status or vary the population selection, as both
included patients with stable/progressive disease for efficacy
assessment.
The present study demonstrated that the risk of BM
varied based on baseline metastatic status, a finding not reported
by previous studies (17,29–31).
Patients with adrenal metastases before initial treatment exhibited
a higher likelihood of developing BM compared with those without.
In the analysis by Oliver et al (30), patients with baseline adrenal
metastases had a non-significant tendency to develop BM in the Cox
multivariate analysis (P=0.12). Potential reasons for these
discrepancies include differing study populations, which could lead
to varied outcomes. Additionally, the aforementioned study recorded
only 10 cases (10.8%) of adrenal metastases before initial
treatment, whereas the present study included 28 cases (17.95%),
potentially influencing the results. Notably, in a study by
Megyesfalvi et al (32), a
higher co-occurrence of adrenal metastasis and BM was observed in
patients with SCLC. The mechanism underlying this phenomenon
remains poorly understood but may be associated with the
homogeneity of metastatic sites (33), Furlan et al (34) suggested that mature adrenal glands
have cells of nerve origin, the differentiation of peripheral glial
stem cells forms chromaffin cells in the adrenal medulla during
beginning of cell differentiation. Accordingly, it was hypothesized
that similar ‘metastatic hotbeds’ may exist within the central
nervous system alongside an abundant blood supply to the baseline
adrenal metastasis site, potentially facilitating BM. These
hypotheses require confirmation through further anatomical and
histological studies.
Sex was also demonstrated to be an independent risk
factor for the development of BM; Kim et al (35) noted that male sex was associated
with the risk of BM in LD-SCLC. A retrospective study by Reddy
et al (36) also identified
male sex as an independent risk factor for the development of
synchronous BM in patients with SCLC. Additionally, male sex was
included as a risk factor in the nomogram for BM risk in patients
with SCLC, developed by Li et al (18). This aligns with the present
findings; however, the reason for this phenomenon remains elusive.
Due to limitations of retrospective studies, such as small
enrollment and single-center studies, a higher proportion of male
patients may reduce the credibility of the conclusions. However, in
the real world and clinical trials, the percentage of male patients
is also high. In a retrospective study in Korea, the proportion of
male patients among 9,994 patients with ES-SCLC was 86.4% (37). In the Chinese CAPSTONE-1 trial, the
proportion of male patients was 80% (38). This is consistent with the present
results. Therefore, it is necessary to expand the sample to
validate the conclusions.
Certain risk factors for BM in patients with SCLC
were not observed in the present study. A retrospective study
demonstrated that weight loss is an independent risk factor for the
development of BM (16); however,
this factor was excluded due to the retrospective nature of the
present study due to challenges in standardizing the timing of
weight recordings and difficulty in determining precise weights. In
patients with LD-SCLC, hematology-associated markers such as tumor
markers, LDH and NLR are associated with the occurrence of BM
(24,25,27);
however, this association was not demonstrated in the present
study. This may be attributed to the participants in the present
study being patients with ES-SCLC who had developed extensive
metastases (65% were oligometastatic) and having a high systemic
tumor burden. Therefore, LDH and associated tumor markers were not
risk factors for BM in patients with ES-SCLC.
Since the publication of phase III randomized
controlled trials, such as IMpower133 and CASPIAN (39,40),
immune checkpoint inhibitors combined with platinum-containing
chemotherapy have been established as the standard first-line
treatment for ES-SCLC, enhancing OS in patients with ES-SCLC
(39). However, previous studies
have not demonstrated that combination immunotherapy extends iPFS
(3), and this observation has been
reported only in patients with non-SCLC (41). The findings of the present study
align with the aforementioned results, indicating that combination
immunotherapy did not significantly increase iPFS compared with
chemotherapy alone.
In the survival analysis of high-risk factors
associated with BM, adrenal metastasis at baseline and
non-oligometastasis were unfavorable factors for survival. More
aggressive application of PCI may be more favorable for the
prognosis of the patient.
The present study had limitations. Firstly, it was a
single-center retrospective study with a limited sample size and
not a randomized controlled trial, which may limit the
generalizability of the data. Additionally, the nomogram
established in the present study could only be validated through
randomized internal validation and not with external data.
Therefore, further large-scale, multicenter, prospective studies
are required to confirm the validity of the present findings.
In conclusion, non-oligometastasis, baseline adrenal
metastasis and male sex were significant risk factors for BM in
patients with ES-SCLC who responded to standard treatment.
Furthermore, the developed nomogram offered a personalized risk
assessment for BM in patients with ES-SCLC who were free of BM at
baseline and responded to standard treatment, thereby assisting
clinicians in making informed decisions regarding PCI.
Acknowledgements
Not applicable.
Funding
The present study was supported by National Natural Science
Foundation of China (grant no. 82103632) and Natural Science
Foundation of Shandong Province (grant no. ZR2021QH245).
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
HL, FC, YJ and HZ conceived and designed the study.
QX, HL, SL, JN, XZ and ZS analyzed data. YT, SL, YJ, ZS, JZ and JN
interpreted data. Acquisition of funding by YT and HZ. HL, HZ, YT,
JZ and SL revised the manuscript critically for important
intellectual content. YT, YJ and HZ supervised the study. HL and FC
wrote the manuscript. HL and HZ confirm the authenticity of all the
raw data. All authors have read and approved the final
manuscript.
Ethics approval and consent to
participate
The present study did not require ethics approval as
it was waived by the Ethical Review Committee of the Affiliated
Cancer Hospital of Shandong First Medical University. Due to the
retrospective nature of the present study, the requirement for
informed consent to participate was waived.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Gazdar AF, Bunn PA and Minna JD:
Small-cell lung cancer: What we know, what we need to know and the
path forward. Nat Rev Cancer. 17:725–737. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Manapov F, Kasmann L, Roengvoraphoj O,
Dantes M, Schmidt-Hegemann NS, Belka C and Eze C: Prophylactic
cranial irradiation in small-cell lung cancer: Update on patient
selection, efficacy and outcomes. Lung Cancer (Auckl). 9:49–55.
2018.PubMed/NCBI
|
|
3
|
Lu S, Guo X, Li Y, Liu H, Zhang Y and Zhu
H: Antiprogrammed death ligand 1 therapy failed to reduce the risk
of developing brain metastases in patients with extensive-stage
small cell lung cancer: A retrospective analysis. Cancer.
130:18–30. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Upton DH, Ung C, George SM, Tsoli M,
Kavallaris M and Ziegler DS: Challenges and opportunities to
penetrate the blood-brain barrier for brain cancer therapy.
Theranostics. 12:4734–4752. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Slotman B, Faivre-Finn C, Kramer G, Rankin
E, Snee M, Hatton M, Postmus P, Collette L, Musat E and Senan S;
EORTC Radiation Oncology Group and Lung Cancer Group, :
Prophylactic cranial irradiation in extensive small-cell lung
cancer. N Engl J Med. 357:664–672. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Takahashi T, Yamanaka T, Seto T, Harada H,
Nokihara H, Saka H, Nishio M, Kaneda H, Takayama K, Ishimoto O, et
al: Prophylactic cranial irradiation versus observation in patients
with extensive-disease small-cell lung cancer: A multicentre,
randomised, open-label, phase 3 trial. Lancet Oncol. 18:663–671.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Slotman BJ, Mauer ME, Bottomley A,
Faivre-Finn C, Kramer GW, Rankin EM, Snee M, Hatton M, Postmus PE,
Collette L and Senan S: Prophylactic cranial irradiation in
extensive disease small-cell lung cancer: Short-term health-related
quality of life and patient reported symptoms: Results of an
international phase III randomized controlled trial by the EORTC
Radiation Oncology and Lung Cancer Groups. J Clin Oncol. 27:78–84.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Gondi V, Hermann BP, Mehta MP and Tome WA:
Hippocampal dosimetry predicts neurocognitive function impairment
after fractionated stereotactic radiotherapy for benign or
low-grade adult brain tumors. Int J Radiat Oncol Biol Phys.
85:348–354. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Gondi V, Paulus R, Bruner DW, Meyers CA,
Gore EM, Wolfson A, Werner-Wasik M, Sun AY, Choy H and Movsas B:
Decline in tested and self-reported cognitive functioning after
prophylactic cranial irradiation for lung cancer: Pooled secondary
analysis of Radiation Therapy Oncology Group randomized trials 0212
and 0214. Int J Radiat Oncol Biol Phys. 86:656–664. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Gondi V, Pugh SL, Tome WA, Caine C, Corn
B, Kanner A, Rowley H, Kundapur V, DeNittis A, Greenspoon JN, et
al: Preservation of memory with conformal avoidance of the
hippocampal neural stem-cell compartment during whole-brain
radiotherapy for brain metastases (RTOG 0933): A phase II
multi-institutional trial. J Clin Oncol. 32:3810–3816. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Brown PD, Gondi V, Pugh S, Tome WA, Wefel
JS, Armstrong TS, Bovi JA, Robinson C, Konski A, Khuntia D, et al:
Hippocampal avoidance during whole-brain radiotherapy plus
memantine for patients with brain metastases: Phase III trial NRG
oncology CC001. J Clin Oncol. 38:1019–1029. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Belderbos JSA, De Ruysscher DKM, De Jaeger
K, Koppe F, Lambrecht MLF, Lievens YN, Dieleman EMT, Jaspers JPM,
Van Meerbeeck JP, Ubbels F, et al: Phase 3 randomized trial of
prophylactic cranial irradiation with or without hippocampus
avoidance in SCLC (NCT01780675). J Thorac Oncol. 16:840–849. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Dingemans AC, Fruh M, Ardizzoni A, Besse
B, Faivre-Finn C, Hendriks LE, Lantuejoul S, Peters S, Reguart N,
Rudin CM, et al: Small-cell lung cancer: ESMO clinical practice
guidelines for diagnosis, treatment and follow-up✩. Ann
Oncol. 32:839–853. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Rusthoven CG and Kavanagh BD: Prophylactic
Cranial Irradiation (PCI) versus active MRI surveillance for small
cell lung cancer: The case for Equipoise. J Thorac Oncol.
12:1746–1754. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
NCCN Clinical Practice Guidelines in
Oncology (NCCN Guidelines), . Small Cell Lung Cancer Version
2.2024. November 21–2023
|
|
16
|
Greenspoon JN, Evans WK, Cai W and Wright
JR: Selecting patients with extensive-stage small cell lung cancer
for prophylactic cranial irradiation by predicting brain
metastases. J Thorac Oncol. 6:808–812. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Chung JH, Kang SY, Wu HG, Seo YS, Kim DW,
Kang KW, Kim HJ and Cheon GJ: Risk stratification of symptomatic
brain metastases by clinical and FDG PET parameters for selective
use of prophylactic cranial irradiation in patients with extensive
disease of small cell lung cancer. Radiother Oncol. 143:81–87.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Li W, Ding C, Sheng W, Wan Q, Cui Z, Qi G
and Liu Y: Development and validation of a nomogram for the
prediction of brain metastases in small cell lung cancer. Clin
Respir J. 17:456–467. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Detterbeck FC, Boffa DJ, Kim AW and Tanoue
LT: The eighth edition lung cancer stage classification. Chest.
151:193–203. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Murray N and Sheehan F: Limited stage
small cell lung cancer. Curr Treat Options Oncol. 2:63–70. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Lee JJ, Bekele BN, Zhou X, Cantor SB,
Komaki R and Lee JS: Decision analysis for prophylactic cranial
irradiation for patients with small-cell lung cancer. J Clin Oncol.
24:3597–3603. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Ankolekar A, De Ruysscher D, Reymen B,
Houben R, Dekker A, Roumen C and Fijten R: Shared decision-making
for prophylactic cranial irradiation in extensive-stage small-cell
lung cancer: An exploratory study. Transl Lung Cancer Res.
10:3120–3131. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
An N, Jing W, Wang H, Li J, Liu Y, Yu J
and Zhu H: Risk factors for brain metastases in patients with
non-small-cell lung cancer. Cancer Med. 7:6357–6364. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Liu J, Wu D, Shen B, Chen M, Zhou X, Zhang
P, Qiu G, Ji Y, Du X and Yang Y: A nomogram to predict the
cumulative risk for brain metastases in patients with limited-stage
small cell lung cancer without prophylactic cranial irradiation.
Strahlenther Onkol. 199:727–738. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Ueki K, Matsuo Y, Kishi N, Yoneyama M,
Yoshida H, Sakamori Y, Ozasa H, Hirai T and Mizowaki T: Usefulness
of pro-gastrin-releasing peptide as a predictor of the incidence of
brain metastasis and effect of prophylactic cranial irradiation in
patients with limited-stage small-cell lung cancer. J Radiat Res.
63:636–645. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Hou Q, Sun B, Yao N, Liang Y, Cao X, Wei L
and Cao J: Construction of brain metastasis prediction model and
optimization of prophylactic cranial irradiation selection for
limited-stage small-cell lung cancer. Cancers (Basel). 14:49062022.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Zhu H, Bi Y, Han A, Luo J, Li M, Shi F,
Kong L and Yu J: Risk factors for brain metastases in completely
resected small cell lung cancer: A retrospective study to identify
patients most likely to benefit from prophylactic cranial
irradiation. Radiat Oncol. 9:2162014. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Bang A, Kendal WS, Laurie SA, Cook G and
MacRae RM: Prophylactic Cranial Irradiation in extensive stage
small cell lung cancer: Outcomes at a comprehensive cancer centre.
Int J Radiat Oncol Biol Phys. 101:1133–1140. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Oliver DE, Donnelly OG, Grass GD, Naghavi
AO, Yang GQ, Dilling TJ and Perez BA: Extracranial metastatic
burden in extensive-stage small cell lung cancer: Implications for
prophylactic cranial irradiation. J Thorac Dis. 10:4321–4327. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Chen Y, Li J, Hu Y, Zhang Y, Lin Z, Zhao Z
and Jiao S: Prophylactic cranial irradiation could improve overall
survival in patients with extensive small cell lung cancer: A
retrospective study. Strahlenther Onkol. 192:905–912. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Megyesfalvi Z, Tallosy B, Pipek O,
Fillinger J, Lang C, Klikovits T, Schwendenwein A, Hoda MA,
Renyi-Vamos F, Laszlo V, et al: The landscape of small cell lung
cancer metastases: Organ specificity and timing. Thorac Cancer.
12:914–923. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Gao Y, Bado I, Wang H, Zhang W, Rosen JM
and Zhang XH: Metastasis Organotropism: Redefining the congenial
soil. Dev Cell. 49:375–391. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Furlan A, Dyachuk V, Kastriti ME,
Calvo-Enrique L, Abdo H, Hadjab S, Chontorotzea T, Akkuratova N,
Usoskin D, Kamenev D, et al: Multipotent peripheral glial cells
generate neuroendocrine cells of the adrenal medulla. Science.
357:eaal37532017. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Kim TG, Pyo H, Ahn YC, Noh JM and Oh D:
Role of prophylactic cranial irradiation for elderly patients with
limited-disease small-cell lung cancer: Inverse probability of
treatment weighting using propensity score. J Radiat Res.
60:630–638. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Reddy SP, Dowell JE and Pan E: Predictors
of prognosis of synchronous brain metastases in small-cell lung
cancer patients. Clin Exp Metastasis. 37:531–539. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Lee JS, Kim S, Sung SY, Kim YH, Lee HW,
Hong JH and Ko YH: Treatment outcomes of 9,994 patients with
extensive-disease small-cell lung cancer from a retrospective
nationwide population-based cohort in the Korean HIRA database.
Front Oncol. 11:5466722021. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Wang J, Zhou C, Yao W, Wang Q, Min X, Chen
G, Xu X, Li X, Xu F, Fang Y, et al: Adebrelimab or placebo plus
carboplatin and etoposide as first-line treatment for
extensive-stage small-cell lung cancer (CAPSTONE-1): A multicentre,
randomised, double-blind, placebo-controlled, phase 3 trial. Lancet
Oncol. 23:739–747. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Liu SV, Reck M, Mansfield AS, Mok T,
Scherpereel A, Reinmuth N, Garassino MC, De Castro Carpeno J,
Califano R, Nishio M, et al: Updated overall survival and PD-L1
subgroup analysis of patients with extensive-stage small-cell lung
cancer treated with Atezolizumab, Carboplatin, and Etoposide
(IMpower133). J Clin Oncol. 39:619–630. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Goldman JW, Dvorkin M, Chen Y, Reinmuth N,
Hotta K, TDDDrukhin D, Statsenko G, Hochmair MJ, Özgüroğlu M, Ji
JH, et al: Durvalumab, with or without tremelimumab, plus
platinum-etoposide versus platinum-etoposide alone in first-line
treatment of extensive-stage small-cell lung cancer (CASPIAN):
Updated results from a randomised, controlled, open-label, phase 3
trial. Lancet Oncol. 22:51–65. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Gadgeel SM, Lukas RV, Goldschmidt J,
Conkling P, Park K, Cortinovis D, de Marinis F, Rittmeyer A, Patel
JD, von Pawel J, et al: Atezolizumab in patients with advanced
non-small cell lung cancer and history of asymptomatic, treated
brain metastases: Exploratory analyses of the phase III OAK study.
Lung Cancer. 128:105–112. 2019. View Article : Google Scholar : PubMed/NCBI
|