Spandidos Publications style
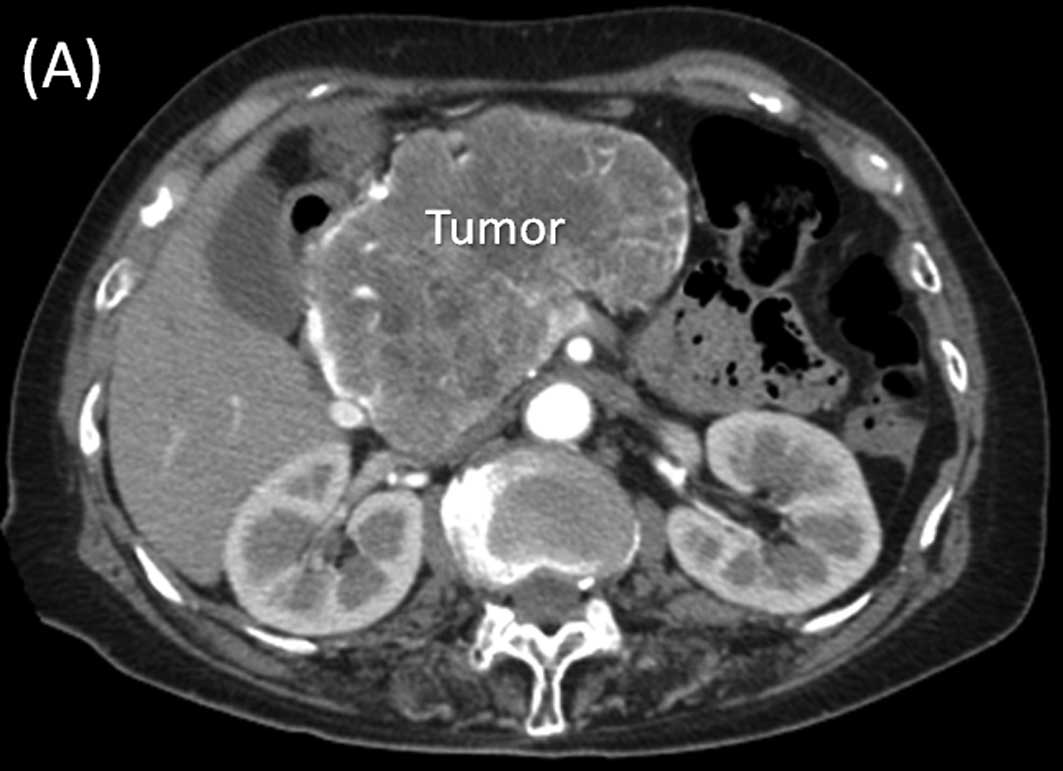
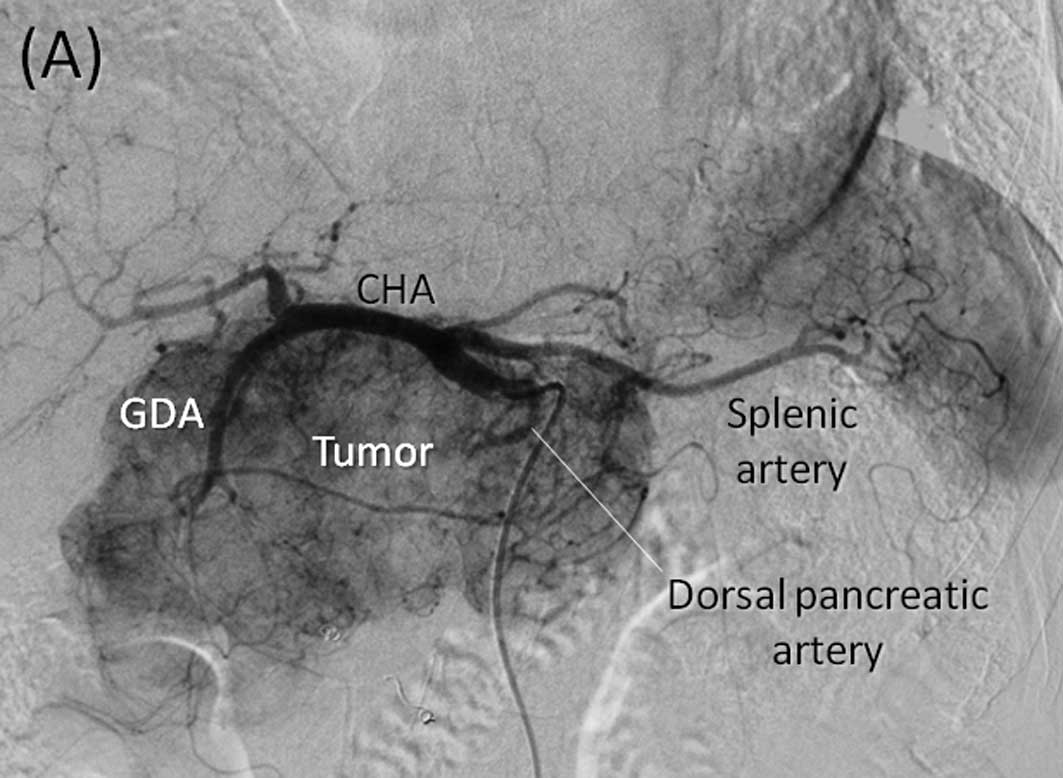
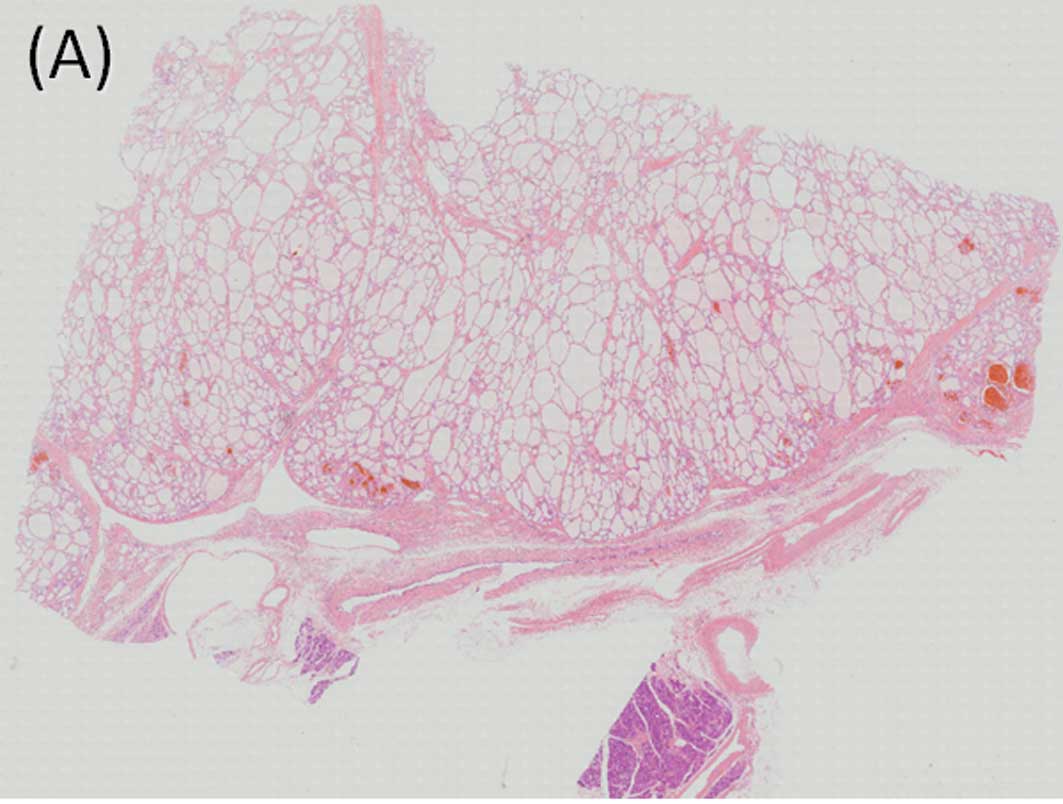
Tajima H, Ohta T, Kitagawa H, Shinbashi H, Hirose A, Sakai S, Makino I, Hayashi H, Nakagawara H, Onishi I, Onishi I, et al: Giant serous microcystic adenoma of the pancreas safely resected after preoperative arterial embolization
. Oncol Lett 1: 841-844, 2010.
APA
Tajima, H., Ohta, T., Kitagawa, H., Shinbashi, H., Hirose, A., Sakai, S. ... Matsui, O. (2010). Giant serous microcystic adenoma of the pancreas safely resected after preoperative arterial embolization
. Oncology Letters, 1, 841-844. https://doi.org/10.3892/ol_00000148
MLA
Tajima, H., Ohta, T., Kitagawa, H., Shinbashi, H., Hirose, A., Sakai, S., Makino, I., Hayashi, H., Nakagawara, H., Onishi, I., Takamura, H., Ninomiya, I., Fushida, S., Tani, T., Fujimura, T., Kayahara, M., Koda, W., Matsui, O."Giant serous microcystic adenoma of the pancreas safely resected after preoperative arterial embolization
". Oncology Letters 1.5 (2010): 841-844.
Chicago
Tajima, H., Ohta, T., Kitagawa, H., Shinbashi, H., Hirose, A., Sakai, S., Makino, I., Hayashi, H., Nakagawara, H., Onishi, I., Takamura, H., Ninomiya, I., Fushida, S., Tani, T., Fujimura, T., Kayahara, M., Koda, W., Matsui, O."Giant serous microcystic adenoma of the pancreas safely resected after preoperative arterial embolization
". Oncology Letters 1, no. 5 (2010): 841-844. https://doi.org/10.3892/ol_00000148