Introduction
Follicular thyroid carcinoma (FTC) is an uncommon
well-differentiated malignant tumor accounting for 10% of all
thyroid malignancies (1,2). It has been reported to be more common
in African American populations than in Asians or Caucasians, with
a female predominance (3). Insular
thyroid carcinoma (ITC) is another thyroid malignancy that is even
rarer, poorly differentiated and accounts for only 0.1 to 6.2% of
all thyroid malignancies (4).
Although ITC is rare, it represents the main cause of mortality
from non-anaplastic follicular cell-derived thyroid cancer, and 20%
of patients with ITC present with distant metastasis at the time of
diagnosis (5). The observation of
ITC arising within the background of FTC is an exceedingly unique
occurrence (6).
The present study reports a case of ITC arising
within the background of FTC, with a brief review of the
literature.
Case report
Patient information
A 52-year-old housewife presented to Smart Health
Tower (Sulaimani, Iraq) with anterior neck swelling for a duration
of 6 months. She had a negative previous medical, surgical and drug
history but a positive family history of thyroid diseases.
Clinical findings and diagnostic
assessment
The patient had a grade 2 thyroid enlargement with a
hard consistency. The hematological test results of the patient
were normal. An ultrasound (US) examination (images not available)
revealed a well-defined solid nodule measuring ~58x37x28 mm in the
mid-lower third of the right thyroid lobe without micro or macro
calcification, and with a TI-RADS 4 according to the Thyroid
Imaging Reporting and Data System (TIRADS). Furthermore, two small
nodules of <3 mm in size were also observed in the left thyroid
lobe. Fine needle aspiration cytology of the lesion led to the
suspicion of a follicular neoplasm, that fell into the Bethesda IV
category.
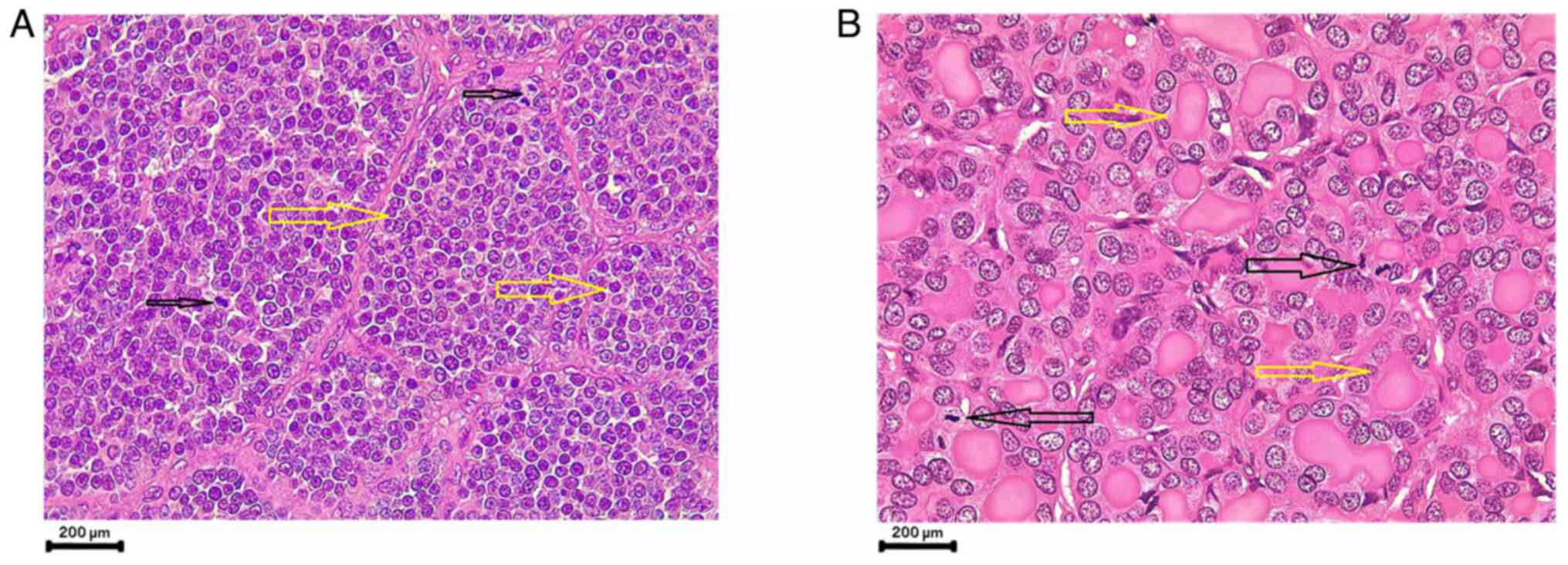
Therapeutic intervention
Following a right thyroid lobectomy, the
histopathological examination led to the diagnosis of ITC arising
within follicular carcinoma (Fig.
1). Consequently, completion thyroidectomy was performed based
on this diagnosis. The immunostaining of thyroid transcription
factor 1 (TTF1) and PAX 8 were used to rule out medullary thyroid
carcinoma due to the presence of multiple foci of spinning and
large anaplastic cells, with bizarre giant cells. The patient was
later sent for radioiodine ablation. Of note, as the patient was an
outpatient, both the histological and immunohistochemistry
examinations were conducted by an external laboratory (Shorsh
Hospital Pathology Laboratory). For this reason, unfortunately, the
authors could not retrieve the exact methodology of the
aforementioned procedures.
Follow-up and outcome
The vital signs of the patient were stable, and
levothyroxine substitution therapy was prescribed, commencing at
150 mcg daily for 1 year post-operatively, followed by a
maintenance dose of 100 mcg daily. Following the definitive
diagnosis and the decision of the multidisciplinary team of Smart
Health Tower, the patient received two doses of radioactive iodine,
with a one-year interval between doses. Following three years of
follow-up, the patient was completely asymptomatic.
Discussion
The ITC is a rare and highly aggressive thyroid
malignancy that is morphologically and biologically considered an
intermediate between fully differentiated and
undifferentiated/anaplastic thyroid carcinomas (7). In 1984, Carcangiu et al
(8) described ITC for the first
time as a poorly differentiated carcinoma. It is termed as insular
as it is composed of well-defined nests. However, this pattern may
be less prominent, and tubercular or solid patterns are recognized
and co-exist (9).
The tumor has frequently been misdiagnosed and often
grouped with solid or moderately differentiated tumors, and it has
sometimes been mistaken for anaplastic carcinoma (10). In comparison to patients solely
with FTC, patients with ITC are older, more often male, have larger
tumor sizes, are more likely to experience metastasis, are less
likely to have a negative resection margin, and have a
significantly lower survival rate (11). Patients with ITC usually complain
of the presence of a rapidly growing neck swelling in association
with dyspnea, dysphagia and voice hoarseness (12). The case described in the present
study was a 52-year-old female with a hard neck mass and normal
vocal cords, with no other associated symptoms.
Histologically, ITC is characterized by small
uniform carcinoma cells, small follicles containing thyroglobulin
and necrotic foci, with a prospect of a peritheliomatous structure
formation (10). The
aforementioned characteristics were also observed in the
histopathological analysis of the case described herein. Necrosis
is another obvious finding, with both capsular and vascular
invasion (13). However, Harach
and Franssila (14) concluded in
their study that even though ITC has thyroglobulin secretion, among
5 cases, 2 cases were negative for thyroglobulin. The molecular
processes behind the unique insular structure found in thyroid
tumors pose a challenge, impeding the comprehension of the factors
contributing to their aggressive nature. Recently, research has
turned to molecular analysis techniques, such as polymerase chain
reaction-single-strand conformation polymorphism analysis, in hopes
of unraveling these mechanisms. These efforts have revealed a
spectrum of mutations associated with ITC (15). Notably, genetic alterations
affecting genes, such as the RAS family (N-ras gene) and p53 gene
have been documented (16).
Additionally, in poorly differentiated thyroid carcinoma, TERT
promoter mutations are frequently observed. Despite this, mutually
exclusive mutations in BRAF and RAS remain the prevailing driver
mutations in poorly differentiated thyroid carcinoma (17,18).
Due to limited resources, genetic tests were not conducted for the
case reported in the present study. Almost all stages of FTC are
treated with total or near-total thyroidectomy, iodine ablation and
thyroid hormone suppression therapy (19). Similarly, aggressive management is
recommended for patients with ITC, and the most appropriate
treatment is total thyroidectomy followed by radioiodine therapy
and close follow-up. These were also performed for the patient
described herein. According to the study by Pezzi et al
(11), the primary treatment for
almost all patients with ITC was surgery undertaken in ~98% of
cases, while this number was 95% in FTC cases. A total
thyroidectomy was performed for the majority of patients with ITC
(79.6%), with a positive margin being found in 32.7% of the
resected ITC cases (11). A
re-operation for these cases is usually associated with the risk of
nerve injury and post-operative hypocalcemia (20).
The ITC is highly aggressive with a high rate of
recurrence and distant metastasis, ranging from 36 to 92% (10). The prognosis of patients with FTC
is dependent on several factors, such as post-operative residual
gross, age, local or distant metastasis, size of the tumor and the
pathologic category (21). Even
though the effect of ITC on the biological behavior of masses with
follicular origin remains unknown (22), studies in the genuine literature
(23) still demonstrate that the
presence of ITC in fully differentiated FTC is associated with
distant metastasis (7,24). Moreover, it has been reported that
patients who have tumors with a minor insular component are not
evidenced to have a poor prognosis (7).
In conclusion, poorly differentiated ITC emerging
from the background of FTC is a very rare incidence that is more
aggressive than any other thyroid tumor, and it is usually
associated with distant metastasis. The management of choice for
these cases is direct total thyroidectomy, followed by radioiodine
therapy.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
AMS and ASM were major contributors to the
conception of the study, as well as to the literature search for
related studies. HOB, MNH and FHK were involved in the literature
review, in the writing of the manuscript, and in the design of the
study. AMA was the pathologist who performed the histopathological
diagnosis. GLO, IJH, ROM, SHH and HMD were involved in the
literature review, in the design of the study, in the critical
revision of the manuscript and in the processing of the images. FHK
and SHH confirm the authenticity of all the raw data. All authors
have read and approved the final manuscript.
Ethics approval and consent to
participate
Written informed consent was obtained from the
patient for her participation in the present study.
Patient consent for publication
Written informed consent was obtained from the
patient for the publication of the present case and any
accompanying images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Nicolson NG, Murtha TD, Dong W, Paulsson
JO, Choi J, Barbieri AL, Brown TC, Kunstman JW, Larsson C, Prasad
ML, et al: Comprehensive genetic analysis of follicular thyroid
carcinoma predicts prognosis independent of histology. J Clin
Endocrinol Metab. 103:2640–2650. 2018.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Mohemed FM, Fatih BN, Qadir AA, Abdalla SH
and Mahmood ZH: Cancer publications in one year (2022); a
cross-sectional study. Barw Med J. 1:18–26. 2023.
|
|
3
|
D'Avanzo A, Treseler P, Ituarte PH, Wong
M, Streja L, Greenspan FS, Siperstein AE, Duh QY and Clark OH:
Follicular thyroid carcinoma: Histology and prognosis. Cancer.
100:1123–1129. 2004.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Salih AM, Kakamad FH and Aube H:
Hyperfuctioning insular thyroid carcinoma: A rare case report. Int
J Surg Case Rep. 28:142–144. 2016.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Uçmak G and Demirel BB: The clinical
management of a patient with insular thyroid carcinoma. Thyroid and
Parathyroid Diseases. Springer, Cham, pp365-370, 2019.
|
|
6
|
Loh TL, Latis S, Ali RB and Patel H:
Insular carcinoma arising on a background of follicular carcinoma,
thyrolipomatosis and amyloid goitre. BMJ Case Rep.
2017(bcr2017219747)2017.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Pellegriti G, Giuffrida D, Scollo C,
Vigneri R, Regalbuto C, Squatrito S and Belfiore A: Long-term
outcome of patients with insular carcinoma of the thyroid: The
insular histotype is an independent predictor of poor prognosis.
Cancer. 95:2076–2085. 2002.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Carcangiu ML, Zampi G and Rosai J: Poorly
differentiated (‘insular’thyroid carcinoma. A reinterpretation of
Langhans' ‘wuchernde Struma’. Am J Surg Pathol. 8:655–668.
1984.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Erkılıç S and Koçer NE: Insular carcinoma
of the thyroid with uncommon cytologic features: Anisokaryotic
cells and microfollicles containing dense colloid. Pathol Res
Pract. 202:389–393. 2006.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Agha A, Glockzin G, Woenckhaus M,
Dietmaier W, Iesalnieks I and Schlitt HJ: Insular carcinomas of the
thyroid exhibit poor prognosis and long-term survival in comparison
to follicular and papillary T4 carcinomas. Langenbecks Arch Surg.
392:671–677. 2007.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Pezzi TA, Sandulache VC, Pezzi CM,
Turkeltaub AE, Feng L, Cabanillas ME, Williams MD and Lai SY:
Treatment and survival of patients with insular thyroid carcinoma:
508 Cases from the national cancer data base. Head Neck.
38:906–612. 2016.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Rijhwani A and Satish GN: Insular
carcinoma of the thyroid in a 10-year-old child. J Pediatr Surg.
38:1083–1085. 2003.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Cornetta AJ, Burchard AE, Pribitkin EA,
O'Reilly RC, Palazzo JP and Keane WM: Insular carcinoma of the
thyroid. Ear Nose Throat J. 82:384–386, 388-389. 2003.PubMed/NCBI
|
|
14
|
Harach HR and Franssila KO: Thyroglobulin
immunostaining in follicular thyroid carcinoma: Relationship to the
degree of differentiation and cell type. Histopathology. 13:43–54.
1988.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Lam KY, Lo CY, Chan KW and Wan KY: Insular
and anaplastic carcinoma of the thyroid: A 45-year comparative
study at a single institution and a review of the significance of
p53 and p21. Ann Surg. 231:329–338. 2000.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Pilotti S, Collini P, Mariani L, Placucci
M, Bongarzone I, Vigneri P, Cipriani S, Falcetta F, Miceli R,
Pierotti MA and Rilke F: Insular carcinoma: A distinct de novo
entity among follicular carcinomas of the thyroid gland. Am J Surg
Pathol. 21:1466–1473. 1997.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Takeuchi Y, Daa T, Kashima K, Yokoyama S,
Nakayama I and Noguchi S: Mutations of p53 in thyroid carcinoma
with an insular component. Thyroid. 9:377–381. 1999.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Pozdeyev N, Gay LM, Sokol ES, Hartmaier R,
Deaver KE, Davis S, French JD, Borre PV, LaBarbera DV, Tan AC, et
al: Genetic analysis of 779 advanced differentiated and anaplastic
thyroid cancers. Clin Cancer Res. 24:3059–3068. 2018.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Choudhury MAM and Shaikh MAA: Management
of papillary and follicular (differentiated) thyroid carcinoma-an
update. Bangladesh J Otorhinolaryngol. 16:126–130. 2010.
|
|
20
|
Baba HO, Muhialdeen AS, Salih AM, Saeed
YA, Abdullah IY, Qaradakhy AJ, Salih KM, Tahir SH, Kakamad FH,
Abdullah HO, et al: Redo thyroidectomy modified technique to
eliminate complications: A cohort study. Barw Med J. 1:7–11.
2023.
|
|
21
|
Chao TC, Lin JD and Chen MF: Insular
carcinoma: Infrequent subtype of thyroid cancer with aggressive
clinical course. World J Surg. 28:393–396. 2004.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Ashfaq R, Vuitch F, Delgado R and
Albores-Saavedra J: Papillary and follicular thyroid carcinomas
with an insular component. Cancer. 73:416–423. 1994.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Muhialdeen AS, Ahmed JO, Baba HO, Abdullah
IY, Hassan HA, Najar KA, Mikael TM, Mustafa MQ, Mohammed DA, Omer
DA, et al: Kscien's list; a new strategy to discourage predatory
journals and publishers (second version). Barw Med J. 1:1–3.
2023.
|
|
24
|
Yamashita H, Noguchi Y, Noguchi S,
Yamashita H, Uchino S, Watanabe S, Ogawa T and Murakami T:
Significance of an insular component in follicular thyroid
carcinoma with distant metastasis at initial presentation. Endocr
Pathol. 16:41–48. 2005.PubMed/NCBI View Article : Google Scholar
|