1. Introduction
The planet is choking on plastic. Plastic is one of
the most widely used products and since the 1970s, the rate of
production has grown rapidly as compared to other materials
(1). It is estimated that plastic
accounts for >80% of marine litter (2). By 2019, plastic accounting for
approximately nine and a half billion tonnes was generated
globally, which amounts to more than one tonne of plastic for every
person alive today (3).
The spread of COVID-19 was further boosted by the
use of single-use plastics, particularly personal protective
equipment (PPE). The extensive use of PPE can prevent the spread of
infection; however, it can add to the accumulation of plastic waste
(4).
Every piece of plastic ever produced, still exists
today and may accumulate in the natural environment and marine
bodies, and can persist for centuries (5). By the action of atmospheric agents,
such as waves, ultraviolet rays, photo-oxidation and bacteria,
pieces of plastic are broken down into larger particles known as
macroplastics and smaller particles (<5 ml) termed microplastics
(6). Macroplastics can persist for
decades in the shorelines, and may eventually come to a halt in
offshore locations (3).
Microplastics persist in the environment due to resistance to
degradation by microorganisms (7).
Microplastics sink into larger depths of oceans and can enter
living organisms, including mammals (8).
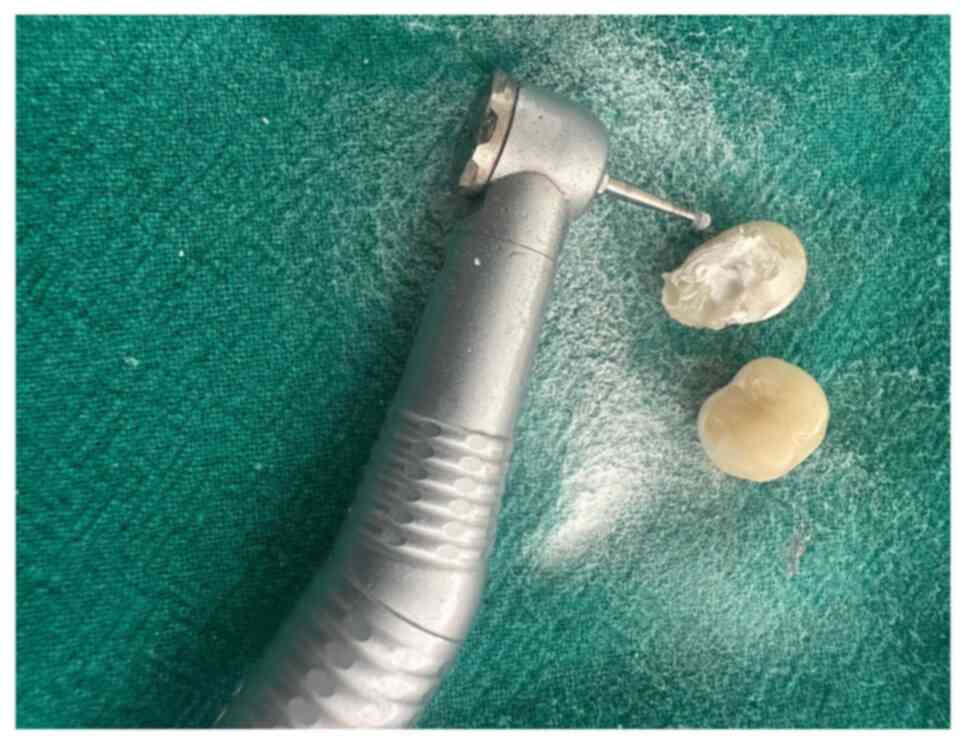
Plastics are not only ubiquitous in everyday lives,
but also form a core part of medical equipment. A vast amount of
medical equipment used in the general hospital environment is
either made from plastic or comes in plastic wrapping. Similarly,
dentistry is continuously evolving to incorporate newer
technologies and innovations, some of the dental materials still
used contain heavy metals and biochemical wastes (1) (Fig.
1).
Microplastics are currently considered an evolving
global issue that can harm marine and terrestrial life, including
humans and mammals (2). This may
lead to potential chronic effects include development of cancer, a
weakened reproductive activity, impaired immunity and developmental
malformations in animals and humans (3). Scientific reports by the World
Economic Forum in 2016 estimate that oceans will contain more
microplastics than fish by the year 2050(4). The impact of plastics (particularly
single-use plastics) on marine life must be emphasised and
strategies must be undertaken to mitigate the toxic effects
(5,6). The present review summarized the
dental procedures and dental materials that have a notable
detrimental effect on the environment and encourages measures to
mitigate these consequences.
2. Literature search methods
To identify articles that evaluated use of
microplastics in dentistry, a search was performed using the
electronic databases, PubMed, Web of Science, Scopus and Google
Scholar, including articles published up to April, 2024. The search
terms used were ‘Microplastics’, ‘Pollution’, ‘Plastics’,
‘Dentistry’, ‘Dental Materials’, ‘Environment’ and ‘COVID-19’.
These search terms were constructed with the aid of Boolean
operators with the use of English language filters. A manual search
was conducted of the articles obtained. Following the removal of
duplicate articles, 27 articles were obtained (6-32).
3. Materials and procedures in
dentistry
Dentistry is a field that is constantly evolving;
however, some materials and procedures that are still in use
include heavy metals and biomedical wastes, which pose a major
challenge to the environment (33).
The exploitation of single-use plastics and other
plastic equipment has amplified to maintain asepsis, reduce
contamination and prevent health challenges to the practitioner.
However, it remains to be determined if all this plastic is truly
degradable (34).
In the field of eco-friendly dentistry, two major
aspects must be recognized. One being at the level of the dental
office and the second including dental products that enhance oral
care.
Dental office
According to the Eco-Dentistry Association (35), waste generated from the dental
office includes 1.7 billion plastic sterilisation packets and
>680 million plastic barriers for dental chairs, covers for
light handles and drapes. Additionally, the use of items such as
personal protective equipment, plastic disposable dental trays and
plastic packaging of various dental products (syringes, polythene
or polyvinyl chloride foils and dental materials) further
exacerbate the existing burden (36).
Hence, evidence suggests that dentistry has a major
influence on the environment and contributes to the carbon
footprint; greater emphasis should be placed on changing these
practices towards an eco-friendly and sustainable environment.
Dental materials
Focus on the environmental impact of dentistry has
been limited, up until the past few decades. The majority of
materials used in dental practice have a high potential to
subsequently breakdown and become incorporated into the environment
as pollutants. A major part of the discussions regarding
environmental pollution in dentistry have been concentrated on
amalgam and its potential health effects due to mercury toxicity
(8).
Controversies surrounding amalgam have led to its
replacement with resin-based restorative materials, which are
considered inert or to have a reduced impact on the environment,
which is in accordance with the mandates in the Minamata Treaty
(37).
All the constituents of resin-based composites have
the potential to act as environmental pollutants upon degradation.
The environmental impact of these materials mainly originates from
their contribution to the carbon footprint during the process of
manufacturing, distribution, disposal, finishing and polishing and
removing old resin-based restorations (9).
Resin-based composites can be classified on the
basis of fabrication and use as follows: i) Direct placement in the
oral cavity and activation: The conversion of monomers to polymers
through this method is incomplete due to partial conversion. At
best, only 60-75% of the monomers convert to form polymers. These
levels can drop as low as 30% at the base of a restoration
(10). ii) Indirect placement:
This method involves the fabrication of appliances and restorations
outside the oral cavity, in dental laboratories through either heat
cure polymerisation or blocs/ingots for machined CAD/CAM.
Restorations fabricated in this method have relatively higher
degrees of conversion of monomers into polymers (38).
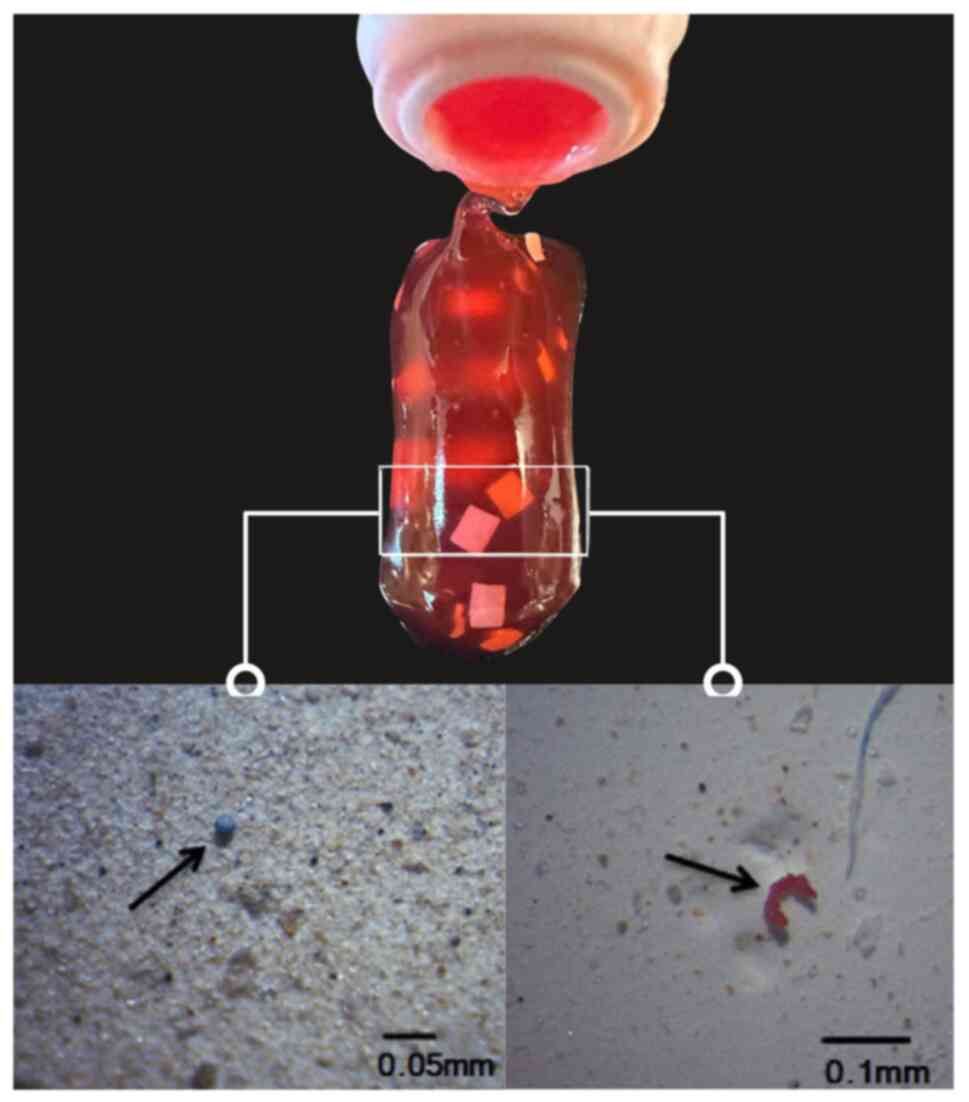
Resin-based composites have the potential to enter
the environment by either chemical means (dissolution and breakdown
of the material within the oral cavity), or physical means (through
the process of milling or grinding, finishing and polishing and
removing old/defective restorations). The illustrating in Fig. 2 depicts microparticulate waste
derived from resin-based composite materials. However, most
commonly, this release is a result of a combination of both
processes (7). According to the
U.S. Environmental Pollution Agency (USEPA) (39), potential contamination by dental
composites occurs through its accidental discharge during the
transportation of dental waste or any malfunction of landfills
which can cause potential environment contamination of dental
composites (11).
Polymethylmethacrylate-based denture
base materials
Denture base polymers can either be heat cured,
auto-polymerised self-cured, light-activated or thermoplastic resin
(40). However, this
polymerisation has been often incomplete and residual monomer
leaches out into the oral cavity, causing health hazards upon
entering the gastrointestinal tract and the inhalation of these
particles can cause asthma, anorexia, headache and drowsiness
(41).
Bisphenol A from orthodontic
appliances
Polymers are widely used in orthodontics in
elastomeric ligatures and chains, polycarbonates for esthetic
brackets and myofunctional appliances. The amount of bisphenol A
released is of minimal risk to humans; however, the effects of
long-term exposure need to be considered (13). Bisphenol A is known to be a toxic
chemical in the environment and recently, in animal models, it has
been shown to induce carcinogenesis and mutagenesis (13,42).
In orthodontics, the release of bisphenol A can
occur through three main ways: i) Through the peripheral margins of
orthodontic brackets (43); ii) in
bonded fixed retainers, a large surface to volume ration of the
adhesives is exposed in the oral cavity and it allows aging,
degradation and leaching of bisphenol A in an unpredictable manner
(15); iii) upon the completion of
orthodontic treatment, grinding and elimination of the adhesive
with instruments is done which releases the components into the
environment via aerosols (12).
Additionally, a recent in vitro study
highlighted the detachment of microplastics from commercial clear
aligners due to their mechanical friction. The majority of
microplastics have a diameter ≥20 µm, which can be excreted from
the gastrointestinal tract (17).
Bisphenol A from composite
restorations and pit and fissure sealants
During the finishing and polishing of dental
restorations, or when old, defective restorations are removed,
secondary microplastics are released into the oral environment
(18). These materials may contain
additives such as bisphenol A, phthalates, some brominated flame
retardants that give desirable properties in colour and
transparency and also counteract the breakdown from ozone,
bacteria, temperature and provide thermal and electrical resistance
(19). However, they have been
proven to be endocrine disruptors which alter the homeostasis of
endocrine system, inhibit the action of natural hormones and alter
its synthesis (44). The
superficial layers of pit and fissure sealants remain unpolymerized
on exposure to oxygen which causes leaching, particularly during
the initial few hours post-placement, which gradually decreases
(45).
Microparticulate waste generated from
the process of finishing, polishing and removal of old defective
restorations
Microparticulate waste is generated chairside when
resin-based composites undergo clinical grinding through the use of
high-speed rotary and abrasive burs and discs. This is usually
performed while removing defective and/or old restorations or while
shaping, finishing and polishing the restorations. These wastes can
also be generated from laboratory processes, such as the milling
and grinding of pre-polymerized resin blocks to design indirect
restorations such as crowns, inlays, onlays and implant abutments
(7). In comparison of the amount
of waste produced, it was noted that indirect restorations
generated significantly higher quantities of microparticulate
wastes (46). These wastes are
removed from the oral cavity by means of a suction tip or an
aspirator, which is released into the sewage wastewater, and
eventually, into the environment (21).
4. Oral hygiene practices
Toothbrushes
The American Dental Association recommends changing
a toothbrush every 3 to 4 months, or more often if the bristles are
visibly matted or frayed (47). In
the US market, approximately one billion toothbrushes are thrown
away each year and 50 million pounds of toothbrushes are added into
the landfills annually (36).
Considering the world's population of 7.53 billion individuals,
~29.4 billion toothbrushes are discarded each year. On average, a
plastic toothbrush weighs ~20 g; it can thus be calculated that the
whole of humanity produce 600 million kg of plastic toothbrush
waste in only 365 days (47).
Among the currently available toothbrushes,
including manual plastic and bamboo toothbrushes and electric
toothbrushes, the greatest contribution to the overall
environmental impact has been observed by traditional plastic
manual toothbrushes (23) as they
are made from polypropylene plastic and nylon, which are derived
from non-renewable fossil fuels (48). The manufacturing process of the
nylon bristles releases nitrous oxide (36). Nitrous oxide is a greenhouse gas,
which is 310-fold more potent than carbon dioxide (49). The toothbrush handles are
relatively larger, made of polypropylene plastic which is neither
biodegradable, nor recyclable (23). The amount of derived plastic waste
in landfills further increases over time.
Toothpastes
In the Indian scenario, the mean yearly release of
microplastics from toothpastes into the environment was gauged as
1.4 billion grams per year, which poses a significant environmental
threat (24). In order to
systematically assess the effects of toothpaste on the environment,
two main aspects must be considered:
i) Toothpaste packaging: The toothpaste tube is
primarily comprised of high-density polyethylene with the cap
comprised of polypropylene. Of note, ~4,000 empty tubes of plastic
need can become converted into one ton of plastic (24).
ii) Contents in toothpastes: Toothpastes are
open-use consumer products, which are intended to be washed off and
ultimately end up in the drains. Active contents of toothpastes are
remineralizing agents (50),
antibacterials (51) and lately,
also probiotics (52). Numerous
personal care and cosmetic products, such as toothpastes, soaps and
gels, include microplastics to enhance the scrubbing and cleansing
action (25). In toothpastes, they
can be added to improve the whitening properties and act as a
polishing aid (26). These
microplastics which eventually accumulate in marine bodies through
the drainage system and in turn within the tissues of aquatic life
as shown in Fig. 3. The
constituents include polyethylene (27), cellophane, polypropylene, polyvinyl
chloride and polyamide in varying concentrations (28). The most widely prevalent
microplastics are polyethylene and toothpastes contain up to 1.8%
of this component (29). A
previous study demonstrated various changes in marine organisms,
such as the complete or partial absence of contacts in the
filaments of gills, the presence of hemocytic infiltration in gills
or mutation of ciliated epithelium to squamous epithelium within
digestive organs and severe necrosis was noted in the gonads
(30).
Dental floss
On average, each individual uses approximately three
million miles of dental floss each year (53). Plastic forms a major component in
the preparation of dental floss and its packaging.
Dental floss contains plastic. Traditional dental
floss is comprised of non-recyclable and non-biodegradable
materials, such as synthetic waxed nylon and teflon that add on to
singe use plastic waste that pollutes marine bodies. Additionally,
it may be coated with pre- and polyfluoroalkyl substances to allow
passage between teeth; however, these chemicals are released while
decomposing, which is toxic to the environment. It is also
inadvertently consumed by marine life, which can cause starvation,
poisoning or suffocation. Corals, that form an essential part of
the marine ecosystem have floss entangled within them.
Dental floss with plastic packaging typically
comprised of polypropylene plastic have the worst carbon footprint
and highest environmental impact compared to other interdental
cleaning aids. The handle alone formed 49% of the overall carbon
footprint.
Mouthwashes
Mouthwashes contain antimicrobials, such as
triclosan [5-chloro-2-(2,4-dichlorophenoxy) phenol]. The use of
triclosan is not highly regulated due to its low acute toxicity and
safety. The continual exposure of on marine life to triclosan leads
to its accumulation within tissues and acute and chronic toxic
effects, such as increased catabolic activity within tissues.
Concentrations >34.5 nmol/l triclosan in river biofilms have
been shown to exert inhibitory effects on periphytic algae
(31).
5. Effects of COVID-19
Since the emergence of COVID-19 and its declaration
as a pandemic by the World Health Organization, stringent measures
to prevent the rapid spread were undertaken in all aspects of life
(54). Some of the measures
undertaken include the incorporation of protective equipment by the
general public and healthcare industry (55). PPE ranges from disposable masks,
head caps, protective eye wear, single use gloves, respirators and
‘splashproof’ protective clothing (56). The use of this protective equipment
shifted from being used almost exclusively in the healthcare
industry to widespread use by the general population against the
pandemic (32).
Additionally, the rate of plastic production
exhibited a notable surge due to two main reasons: One being the
temporary relaxation with the use of disposable plastics to combat
virus transmission; and second being the decrease in petroleum
prices due to the reduced demand in various countries. The decrease
in the oil rates translated into a decrease in the cost of plastic
production. Industries took advantage of this reduction in cost to
boost plastic production (20).
PPE
PPEs are prepared from various synthetic polymers,
including high- and low-dentistry polymers which are neither
recyclable, nor biodegradable. High-density polymers include
polyester, polyvinyl chloride and polyvinyl alcohol, which sink
into deep marine sediments (57).
On the other hand, low-density polymers, such as polyethylene,
expanded polystyrene and polypropylene float on sea water (58).
Disposable masks comprise of three layers where the
inner layer is made up of hydrophilic soft fibers, the middle layer
is made of melt-blown filter and the outer layer is made of
non-woven hydrophobic fibers. The main filtering layer is the
middle layer, which is manufactured by the entanglement of micro-
and nanofibers (59).
Gloves were mostly made up of polyvinyl chloride,
latex and nitrile. Face shields are made using a wide variety of
materials, including polyethylene terephthalate glycol, acetate,
polyvinyl chloride and polycarbonate (60). The fate of these microplastics
ranges from either floating along the ocean currents, or sinking
into the sediments and becoming a part of the geological record
(61).
6. Mitigation strategies and challenges of
implementation
General considerations for the dental
office
Various practices can be adopted by the dental team
to make environmentally friendly choices. To begin with, further
attention should be directed towards purchasing products with
minimal plastic packaging and the use of reusable plastic
containers should be encouraged. Non-critical and semi-critical
items, such as paper towels, cotton rolls or wool rolls made from
recycled or partially recycled materials can be used. Containers or
packaging with polyvinyl chloride should be avoided, whenever
practical. Digital platforms for the maintenance of records and the
use of both sides of pages with single spacing can reduce the
amount of paper used in the office.
The use of biodegradable bags made out of vegetable
starch should replace plastic bags as natural materials, such as
vegetables are degraded readily and completely and serve as natural
soil fertilizers, as compared to plastics. To disinfect the dental
operatory, the Occupational Safety and Health Administration (OSHA)
recommended reusable nitrile gloves should be used instead of
disposable examination gloves. Furthermore, the use of gloves
should be limited as per requirement, and injudicious use should be
restricted.
Instruments that require sterilization in an
autoclave should be packed in metal autoclave cassettes or reusable
cloth or fabric bags, instead of plastic backed paper. This
alternative is more cost-effective, protects practitioners and
patients and does not overburden the environment (14). Instead of using plastic suction
tips, metal or autoclavable suction tips can be used. Special
considerations should be made towards incorporating a container for
recyclable items and effort to ensure the correct disposable of
recyclable items to designated centers, rather than adding on to
landfills (7).
Dental materials
The concept of ‘green dentistry’ incorporates the
four R's: Reduce, reuse, recycle and rethink. The use of trays for
the application of fluoride should be substituted by the use of
fluoride varnish. If the need for trays is mandated, such as for
the preparation of dental impressions, metal or reusable trays
should be used instead. Clinical recommendations should be followed
to avoid overbuilding resin-based composite restorations so as to
avoid further reduction and generation of microparticulate waste
(62). Consideration towards
repairing defective restorations, as compared to complete removal.
In the case that the removal of resin-based restorations is deemed
necessary, a water spray should be then used in conjunction to
reduce the generation of microplastics (9). The development of measures is
required to allow the complete conversion of monomers, such as
placing the curing light as close to the adhesive as clinically
possible during polymerization to allow the maximum direct
conversion of the monomer and reduce the amount of bisphenol A
released (14). Clinicians are
advised to perform a pumice prophylaxis after bonding to the
surface of these resin adhesives (43). Rinsing of the oral cavity is
recommended after bonding orthodontic brackets within the first
hour of placement to prevent the potential leaching of monomers
(14). Brackets comprised of
ceramic release lesser amounts of unpolymerized resin than
polycarbonate brackets (16). The
use of manual toothbrushes with replaceable heads and bamboo
toothbrushes have a marked positive environmental impact in terms
of their effect on climate change, resource use, ozone depletion
and accumulation in marine bodies (23). Additionally, they use >97% less
plastic than traditional plastic toothbrushes. However, the higher
purchase costs of bamboo toothbrushes may pose as a barrier for
consumer use (23). Alternatives
to dental floss include silk and candelilla wax floss, silk and
beeswax floss with packaging comprised of glass and aluminum
dispensers or in carbohydrate or bioplastic boxes (36). It is essential to advise patients
to not flush down used dental floss, as it can cause severe
clogging in the sewer systems by entangling with other debris, hair
or other particles.
The present review aimed to provide a comprehensive
overview of the environmental impacts of plastic use in dentistry,
from restorative practices to oral hygiene products, and their
contribution to microplastic waste. However, the present review has
certain limitations, such as a lack of quantitative data on the
specific contributions of dental practices to global plastic
pollution, limited focus on the regional variations and how local
regulations and practices may influence this generation and
management of plastic waste in dentistry.
7. Conclusion and future perspectives
While the present review provides valuable insight
into the environmental impacts of plastic use in dentistry, several
gaps in current knowledge warrant further investigation. Questions
such as the specific contribution of dental specialties to
microplastic pollution and the unique environmental impact of
dental wastes compared to medical or general wastes remain
unanswered. Additionally, evidence on the long-term impact of
biodegradable or alternative materials in dentistry is limited.
Future research is thus required to focus on
exploring emerging sustainable technologies and practices, as well
as to evaluate the effectiveness of current knowledge and policy
interventions in reducing plastic consumption. Such efforts could
facilitate the widespread adoption of sustainable practices in
dentistry.
In conclusion, the environmental impact of dentistry
should be considered and voluntary efforts should be taken to
reduce the production and discharge of plastics. The utilization of
plastics, particularly single-use plastics, should be carefully
monitored in the dental office and measures should be taken to curb
its use and encourage use of ecologically friendly measures.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
Not applicable.
Authors' contributions
DAT was involved in the conceptualization of the
study, in the literature search and in the screening of all
selected articles and in the removal of duplicates, in project
administration and visualization. DAT was also involved in the
writing of the original draft of the manuscript, and in the
writing, review and editing of the manuscript. SB was involved in
the screening of all selected articles and in the removal of
duplicates, study supervision, validation of the data obtained from
the literature for inclusion in the review, and in the writing,
review and editing of the manuscript. Both authors have read and
approved the final manuscript. Data authentication is not
applicable.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Bayne SC, Ferracane JL, Marshall GW,
Marshall SJ and van Noort R: The evolution of dental materials over
the past century: Silver and gold to tooth color and beyond. J Dent
Res. 98:257–265. 2019.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Rands MRW, Adams WM, Bennun L, Butchart
SH, Clements A, Coomes D, Entwistle A, Hodge I, Kapos V,
Scharlemann JP, et al: Biodiversity conservation: Challenges beyond
2010. Science. 329:1298–1303. 2010.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Auta HS, Emenike CU and Fauziah SH:
Distribution and importance of microplastics in the marine
environment: A review of the sources, fate, effects, and potential
solutions. Environ Int. 102:165–176. 2017.PubMed/NCBI View Article : Google Scholar
|
|
4
|
World Economic Forum: Annual Meeting.
2016, Mastering the fourth industrial revolution. World Economic
Forum, Davos-Klosters, 2016.
|
|
5
|
Shim WJ and Thomposon RC: Microplastics in
the ocean. Arch Environ Contam Toxicol. 69:265–268. 2015.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Anderson A, Andrady A, Arthur C, Baker J,
Bouwman H, Gall S, Hildalgo-Ruz V, Köhler A, Law KL, Leslie HA, et
al: Sources, fate and effects of microplastics in the environment:
A global assessment. GESAMP Reports and Studies Series, No. 90.
International Maritime Organization, 2015.
|
|
7
|
Mulligan S, Hatton PV and Martin N:
Resin-based composite materials: Elution and pollution. Br Dent J.
232:644–652. 2022.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Mulligan S, Kakonyi G, Moharamzadeh K,
Thornton SF and Martin N: The environmental impact of dental
amalgam and resin-based composite materials. Br Dent J.
224:542–548. 2018.
|
|
9
|
Mulligan S, Ojeda JJ, Kakonyi G, Thornton
SF, Moharamzadeh K and Martin N: Characterisation of microparticle
waste from dental resin-based composites. Materials (Basel).
14(4440)2021.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Sideridou ID and Achilias DS: Elution
study of unreacted Bis-GMA, TEGDMA, UDMA, and Bis-EMA from
light-cured dental resins and resin composites using HPLC. J Biomed
Mater Res B Appl Biomater. 74:617–626. 2005.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Erdal S and Orris P: Mercury in dental
amalgam and resin-based alternatives: A comparative health risk
evaluation. Health Care Res Collab. 10:2012.
|
|
12
|
Almeida MA: Analysis of aerodynamically
respirable dust generated from quartz-containing orthodontic and
dental composites utilizing air rotary abrasion. Am J Orthod
Dentofacial Orthop. 131(813)2007.
|
|
13
|
Ma Y, Liu H, Wu J, Yuan L, Wang Y, Du X,
Wang R, Marwa PW, Petlulu P, Chen X and Zhang H: The adverse health
effects of bisphenol A and related toxicity mechanisms. Environ
Res. 176(108575)2019.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Kloukos D and Eliades T: 13-Bisphenol A
and orthodontic materials. In: Orthodontic Applications of
Biomaterials. Elsevier, pp207-219, 2017.
|
|
15
|
Gioka C, Eliades T, Zinelis S, Pratsinis
H, Athanasiou AE, Eliades G and Kletsas D: Characterization and in
vitro estrogenicity of orthodontic adhesive particulates produced
by simulated debonding. Dent Mater. 25:376–382. 2009.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Kloukos D, Pandis N and Eliades T:
Bisphenol-A and residual monomer leaching from orthodontic adhesive
resins and polycarbonate brackets: A systematic review. Am J Orthod
Dentofacial Orthop. 143 (4 Suppl):S104–S112.e1-e2. 2013.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Quinzi V, Orilisi G, Vitiello F,
Notarstefano V, Marzo G and Orsini G: A spectroscopic study on
orthodontic aligners: First evidence of secondary microplastic
detachment after seven days of artificial saliva exposure. Sci
Total Environ. 866(161356)2023.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Van Landuyt KL, Nawrot T, Geebelen B, De
Munck J, Snauwaert J, Yoshihara K, Scheers H, Godderis L, Hoet P
and Van Meerbeek B: How much do resin-based dental materials
release? A meta-analytical approach. Dent Mater. 27:723–747.
2011.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Hahladakis JN, Velis CA, Weber R,
Iacovidou E and Purnell P: An overview of chemical additives
present in plastics: Migration, release, fate and environmental
impact during their use, disposal and recycling. J Hazard Mater.
344:179–199. 2018.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Anderson A, Chandralingam R and
PraveenKumar TR: Impact of COVID-19 pandemic on plastic surge and
environmental effects. Energy Sources, Part A: Recovery,
Utilization, and Environmental Effects. Taylor & Francis,
pp1-7, 2021.
|
|
21
|
Lochhead RY: Chapter 13-The use of
polymers in cosmetic products. Cosmetic Science And Technology,
pp171-221, 2017.
|
|
22
|
Abed R, Ashley P, Duane B, Crotty J and
Lyne A: An environmental impact study of inter-dental cleaning
aids. J Clin Periodontol. 50:2–10. 2023.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Lyne A, Ashley P, Saget S, Porto Costa M,
Underwood B and Duane B: Combining evidence-based healthcare with
environmental sustainability: Using the toothbrush as a model. Br
Dent J. 229:303–309. 2020.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Malea A, Tzotzis A, Manavis A and Kyratsis
P: Innovative and sustainable toothpaste packaging design. J Graph
Eng Des. 11:19–30. 2020.
|
|
25
|
Leslie HA: Review of microplastics in
cosmetics. IVM Inst Environ Stud. 476:1–33. 2014.
|
|
26
|
Vaz VTP, Jubilato DP, de Oliveira MRM,
Bortolatto JF, Floros MC, Dantas AAR and Oliveira Junior OB:
Whitening toothpaste containing activated charcoal, blue covarine,
hydrogen peroxide or microbeads: Which one is the most effective? J
Appl Oral Sci. 27(e20180051)2019.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Ustabasi GS and Baysal A: Bacterial
interactions of microplastics extracted from toothpaste under
controlled conditions and the influence of seawater. Sci Total
Environ. 703(135024)2020.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Madhumitha CT, Karmegam N, Biruntha M,
Arun A, Al Kheraif AA, Kim W and Kumar P: Extraction,
identification, and environmental risk assessment of microplastics
in commercial toothpaste. Chemosphere. 296(133976)2022.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Lei K, Qiao F, Liu Q, Wei Z, Qi H, Cui S,
Yue X, Deng Y and An L: Microplastics releasing from personal care
and cosmetic products in China. Mar Pollut Bull. 123:122–126.
2017.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Bråte ILN, Blázquez M, Brooks SJ and
Thomas KV: Weathering impacts the uptake of polyethylene
microparticles from toothpaste in Mediterranean mussels (M.
galloprovincialis). Sci Total Environ. 626:1310–1318.
2018.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Johansson CH, Janmar L and Backhaus T:
Triclosan causes toxic effects to algae in marine biofilms, but
does not inhibit the metabolic activity of marine biofilm bacteria.
Mar Pollut Bull. 84:208–212. 2014.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Ammendolia J, Saturno J, Brooks AL, Jacobs
S and Jambeck JR: An emerging source of plastic pollution:
Environmental presence of plastic personal protective equipment
(PPE) debris related to COVID-19 in a metropolitan city. Environ
Pollut. 269(116160)2021.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Farahani A and Suchak M: Eco-friendly
dentistry, the environmentally responsible dental practice.
University of Waterloo, Ontario, Canada, 2007.
|
|
34
|
Patel B: Infection control in the
endodontic office. In: Patel B (ed). Endodontic Diagnosis,
Pathology, and Treatment Planning: Mastering Clinical Practice.
Switzerland: Springer International Publishing, pp87-101, 2015.
|
|
35
|
Epa U, of Resource Conservation O. EPA's
Guide for Industrial Waste Management: Introduction.
|
|
36
|
Mazur M, Ndokaj A, Jedlinski M, Maruotti
A, Stamegna C, Corridore D, Capocci M, Ottolenghi L and Guerra F:
How dentistry is impacting the environment. Senses Sci. 6:922–928.
2019.
|
|
37
|
United Nations Environment Programme
(UNEP): Minamata convention on mercury. United Nations Environment
Programme, Nairobi, Kenya. https://www.unep.org/globalmercurypartnership/our-work/mercury-products/phasing-down-the-use-of-dental-amalgam.
Accessed on April 24, 2024.
|
|
38
|
Nandini S: Indirect resin composites. J
Conserv Dent. 13:184–194. 2010.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Eco Dentistry Association (EDA): Infection
Control Waste (Internet). Eco Dentistry Association, Berkeley, CA.
https://ecodentistry.org/green-dental-professionals/dental-office-waste/infection-control-waste/.
Accessed on April 24, 2016.
|
|
40
|
Anusavice KJ, Shen C and Rawls HR:
Phillips' science of dental materials. Elsevier Health Sciences,
2012.
|
|
41
|
Jorge JH, Giampaolo ET, Machado AL and
Vergani CE: Cytotoxicity of denture base acrylic resins: A
literature review. J Prosthet Dent. 90:190–193. 2003.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Leung YK, Govindarajah V, Cheong A,
Veevers J, Song D, Gear R, Zhu X, Ying J, Kendler A, Medvedovic M,
et al: Gestational high-fat diet and bisphenol A exposure heightens
mammary cancer risk. Endocr Relat Cancer. 24:365–378.
2017.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Eliades T, Viazis AD and Eliades G:
Bonding of ceramic brackets to enamel: Morphologic and structural
considerations. Am J Orthod Dentofacial Orthop. 99:369–375.
1991.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Cingotti N and Jensen GK: Health and
Environment Alliance (HEAL). Food contact materials and chemical
contamination. Health and Environment Alliance. Brussels, Belgium,
2019.
|
|
45
|
Chandran T, Vishnu U and Warrier AK:
Microplastics in dentistry-a review. In: Muthu SS (ed) Microplastic
Pollution. Sustainable Textiles: Production, Processing,
Manufacturing & Chemistry. Springer, Singapore, pp157-174,
2021.
|
|
46
|
Akhtar N, Tahir A, Qadir A, Masood R,
Gulzar Z and Arshad M: Profusion of microplastics in dental
healthcare units; morphological, polymer, and seasonal trends with
hazardous consequences for humans. J Hazard Mater.
479(135563)2024.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Niederman R: ADA Council on Scientific
Affairs; ADA Division of Science; Journal of the American Dental
Association. Manual versus powered toothbrushes: The Cochrane
review. J Am Dent Assoc. 134:1240–1244. 2003.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Zhu Y, Romain C and Williams CK:
Sustainable polymers from renewable resources. Nature. 540:354–362.
2016.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Wightman J: Production and mitigation of
greenhouse gases in agriculture. Cornell University Agricultural
Ecosystems Program Team, Ithaca, NY, 2006. Accessed on October 25,
2010.
|
|
50
|
Butera A, Gallo S, Pascadopoli M,
Montasser MA, Abd El Latief MH, Modica GG and Scribante A: Home
oral care with biomimetic hydroxyapatite vs conventional
fluoridated toothpaste for the remineralization and desensitizing
of white spot lesions: Randomized clinical trial. Int J Environ Res
Public Health. 19(8676)2022.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Reda B, Hollemeyer K, Trautmann S, Volmer
DA and Hannig M: First insights into chlorhexidine retention in the
oral cavity after application of different regimens. Clin Oral
Investig. 25:6109–6118. 2021.PubMed/NCBI View Article : Google Scholar
|
|
52
|
Butera A, Pascadopoli M, Nardi MG, Ogliari
C, Chiesa A, Preda C, Perego G and Scribante A: Clinical use of
paraprobiotics for pregnant women with periodontitis: Randomized
clinical trial. Dent J (Basel). 12(116)2024.PubMed/NCBI View Article : Google Scholar
|
|
53
|
Ainsworth S: Flossed for words:
Developments in oral care. Dent Nurs. 4:706–710. 2008.
|
|
54
|
McKay B, Calfas J and Ansari T:
Coronavirus declared pandemic by world health organization. Wall St
J. 8:15–23. 2020.
|
|
55
|
World Health Organization (WHO): Rational
use of personal protective equipment for coronavirus disease
(COVID-19) and considerations during severe shortages. WHO, Geneva,
2020.
|
|
56
|
Dharmaraj S, Ashokkumar V, Hariharan S,
Manibharathi A, Show PL, Chong CT and Ngamcharussrivichai C: The
COVID-19 pandemic face mask waste: A blooming threat to the marine
environment. Chemosphere. 272(129601)2021.PubMed/NCBI View Article : Google Scholar
|
|
57
|
Wright RJ, Erni-Cassola G, Zadjelovic V,
Latva M and Christie-Oleza JA: Marine plastic debris: A new surface
for microbial colonization. Environ Sci Technol. 54:11657–11672.
2020.PubMed/NCBI View Article : Google Scholar
|
|
58
|
Karim N, Afroj S, Lloyd K, Oaten LC,
Andreeva DV, Carr C, Farmery AD, Kim ID and Novoselov KS:
Sustainable personal protective clothing for healthcare
applications: A review. ACS Nano. 14:12313–12340. 2020.PubMed/NCBI View Article : Google Scholar
|
|
59
|
Esposito S, Principi N, Leung CC and
Migliori GB: Universal use of face masks for success against
COVID-19: Evidence and implications for prevention policies. Eur
Respir J. 55(2001260)2020.PubMed/NCBI View Article : Google Scholar
|
|
60
|
Roberge RJ: Face shields for infection
control: A review. J Occup Environ Hyg. 13:235–242. 2016.PubMed/NCBI View Article : Google Scholar
|
|
61
|
Torres FG and De-la-Torre GE: Historical
microplastic records in marine sediments: Current progress and
methodological evaluation. Reg Stud Mar Sci. 46(101868)2021.
|
|
62
|
Heintze SD, Ilie N, Hickel R, Reis A,
Loguercio A and Rousson V: Laboratory mechanical parameters of
composite resins and their relation to fractures and wear in
clinical trials-a systematic review. Dent Mater. 33:e101–e114.
2017.PubMed/NCBI View Article : Google Scholar
|