Introduction
Peritoneal carcinomatosis (PC) is a common form of
metastatic dissemination into the peritoneal cavity, frequently
from cancers of the stomach, colon, ovary or pancreas (1,2). Our
previous studies demonstrated that the survival of PC patients has
significantly improved since the introduction of cytoreductive
surgery (CRS) plus hyperthermic intraperitoneal chemotherapy
(HIPEC) and modern systemic therapies (3–6). To ensure
that patients optimally benefit from this multimodality treatment,
patient selection must be restricted to those with limited
peritoneal disease, in whom a complete CRS may be achieved
(7,8).
Modern medical imaging technologies play an
important role in this regard. Contrast-enhanced multidetector-row
computed tomography (CT) is the modality of choice in the
preoperative evaluation of PC patients (9–13).
However, although modern CT technology has significantly
contributed to the determination of the PC score, it is a
relatively static technology, unable to accurately observe the
bowel movement and dynamic distribution of the small intestines.
Therefore, there is an urgent clinical demand for dynamic imaging
technologies for real-time observation of the changes of the small
intestine, in order to accurately assess the severity of the impact
of PC on bowel function.
There are currently several techniques for the
observation of the bowel movement under X-ray screen, such as
barium sulfate swallowing and air-barium sulfate double-contrast
studies. However, these studies are not suitable for PC patients,
as these patients usually have intestinal obstruction and barium
sulfate swallow may exacerbate the clinical symptoms of PC.
Therefore, a suitable alternative is required. For this purpose,
water-soluble contrast media are promising options.
This study aimed to prospectively investigate the
clinical utility of oral gastrografin radiography (OGR) for the
real-time dynamic study of the functional impacts of PC on the
gastrointestinal system, to enable the selection of patients
suitable for CRS+HIPEC treatment.
Patients and methods
Patients
A total of 105 patients with PC were included in
this study, including 54 cases (51.5%) with PC from gastric cancer,
22 (21.0%) from colorectal cancer, 9 (8.7%) from ovarian cancer, 6
(5.7%) from primary peritoneal carcinoma, 6 (5.7%) from appendiceal
mucinous adenocarcinoma, 2 (1.9%) from gallbladder carcinoma, 2
(1.9%) from lung cancer, 1 (0.9%) from breast cancer, 1 (0.9%) from
splenic adenocarcinoma, 1 (0.9%) from malignant mesothelioma and 1
(0.9%) from squamous cell carcinoma of the uterine cervix. The
patients included 43 men (41.0%) and 62 women (59.0%), with an age
range of 22–76 years (median, 55 years).
The study protocol was approved by the Institutional
Review Board of the Zhongnan Hospital of Wuhan University (Wuhan,
China) and conformed to the ethical standards of the World Medical
Association Declaration of Helsinki. Written informed consent was
obtained from the patients prior to conducting this
examination.
OGR study
Preparation
In patients with PC or suspected PC, the
gastrointestinal motility is often slower than normal (14). Therefore, proper preparation is
crucial, including 4 h of fasting and water deprivation prior to
the exanimation, to ensure the upper digestive tract is empty. For
patients with intestinal obstruction, gastrointestinal
decompression must be performed prior to the examination, to reduce
the retention of excessive gastrointestinal fluid.
OGR study at the standing position
After receiving detailed instructions on the entire
examination procedure, each patient stood on the digital
gastrointestinal machine for a brief observation of the chest and
the abdomen. If considered suitable for such an examination, the
patient was instructed to swallow 80 ml of the hyperosmolar
water-soluble contrast medium gastrografin (76% compound meglumine
diatrizoate injection, 20 ml/ampule, containing 15.2 g meglumine
diatrizoate and sodium diatrizoate; Shanghai Xudong Haipu
Pharmaceutical Co., Ltd., Shanghai, China), and directly observed
under the Philips OMEN type digital gastrointestinal machine
(OmniDiagnost Eleva Release DI 1.1; Philips, Amsterdam, The
Netherlands). The flow trace of gastrografin was recorded (15).
OGR study at shifting positions
In patients fulfilling the required conditions, when
the contrast medium was observed to have reached the stomach, the
patient was placed in the supine position. The outline and motility
of the stomach and duodenum were first observed while the patient
changed positions on the examination bed. Once the contrast medium
was observed to have reached the proximal jejunum, the patient
shifted to the standing position and the flow trace of the contrast
agent was recorded at regular time intervals (15 min) to reflect
the movements and distributions of the small intestine, until the
contrast agent reached the cecum.
Key considerations of the study
As the aim of this study was to evaluate the
functional impacts of PC on the gastrointestinal system, attention
was focused on the following aspects during the study: i) Stomach
filling and movements: Once the contrast agent reached the stomach,
the contour and movement of the stomach were observed. Any
disruptions of the mucosa, gastric wall recesses and/or irregular
movements were recorded. The time interval from the entry of the
contrast agent to the emptying of the stomach was also recorded.
ii) Small intestinal filling, movements and distribution: When the
contrast agent reached the duodenum, the contour, distribution,
mucosal characteristics and movements of the different parts of the
small intestine were observed, recording the following information:
Stenosis of the small bowel, stiffness of the intestinal wall,
deformation or mucosal damage, abnormal distribution of
peristalsis, site and severity of intestinal obstruction. iii)
Contracture of the small intestinal mesentery: As PC frequently
involves the small intestinal mesentery, leading to contracture and
hardening, a number of typical abnormal signs may appear during the
examination. In patients with partial mesenteric contracture, the
typical sign is the formation of small intestinal aggregates in one
or several segments of the small intestine, with reduced motility
of the involved part of the small intestine. In patients with more
severe mesenteric contracture, ball-like or petal-like aggregates
of small intestinal loops may appear, with significantly reduced
flow of the contrast agent through them. In patients with
generalized mesenteric contracture, the entire small intestine may
be pulled together to form a fixed ball in the central abdomen,
with stagnation of the contrast agent within the intestinal
loops.
Comparison of OGR signs with
clinicopathological findings
The patients underwent CRS+HIPEC, with the
designated operating team and standardized protocols established at
our institution (6). Briefly,
following induction of general anesthesia, a midline
xiphoid-to-pubic incision was performed and maximal CRS was
performed, with removal of the primary tumor with acceptable
margins, any involved adjacent tissues/organs and regional lymph
nodes, and peritonectomy. The completeness of cytoreduction was
evaluated prior to HIPEC (16). The
intraoperative findings were recorded and compared with the OGR
findings.
Statistical analysis
Data analyses were performed using the SPSS
software, version 17.0 (SPSS Inc., Chicago, IL, USA). The numerical
data were directly recorded and the categorical data were recorded
into different categories. The OGR characteristics of PC from
different cancers were compared and tested using analysis of
variance (Chi-squared test). The accordance rate between OGR and
operative findings was assessed with correlation studies. A
two-sided P-value of <0.05 was considered to indicate
statistically significant differences.
Results
Clinicopathological characteristics of
PC patients
A total of 105 patients were included in this study.
The major clinicopathological characteristics are summarized in
Table I.
 | Table I.Major clinicopathological
characteristics of the patients in this study (n=105). |
Table I.
Major clinicopathological
characteristics of the patients in this study (n=105).
| Variables | Patient no. (%) |
|---|
| Median age, years
(range) | 55 (22–76) |
| Gender,
male/female | 43/62
(41.0/59.0) |
| Primary tumor |
|
| Gastric
cancer | 54 (51.4) |
|
Colorectal cancer | 28 (26.7) |
|
Gynecological cancer | 9 (8.6) |
| Primary
peritoneal carcinoma | 6 (5.7) |
|
Othersa | 8 (7.6) |
| Histopathology |
|
|
Adenocarcinoma |
|
|
Well/moderately
differentiated | 17 (16.2) |
|
Poorly
differentiated/undifferentiated | 36 (34.3) |
| Signet
ring cell carcinoma | 11 (10.5) |
| Mucinous
adenocarcinoma | 29 (27.6) |
| Serous
papillary adenocarcinoma | 4 (3.8) |
|
Othersa | 8 (7.6) |
| Degree of small
intestinal mesenteric contracture |
|
|
Normal | 39 (37.1) |
|
Mild | 51 (48.6) |
|
Intermediate | 10 (9.5) |
|
Severe | 5 (4.8) |
Technical considerations of OGR
All the patients completed the OGR (103 patients by
direct oral swallow and 2 patients by nasogastric tube infusion).
The time interval between the administration of gastrografin to the
completion of the examination ranged from 30 to 360 min (median, 90
min; mean ± SD, 103±9.1 min). In 98 patients the contrast agent
successfully reached the cecum, while in 7 patients the contrast
agent failed to reach the cecum due to total pyloric obstruction
(n=2), total intestinal obstruction (n=3) and loss of intestinal
mobility (n=2).
Normal OGR findings in PC patients
without small intestinal function impairment
Of the 105 patients, 9 (8.6%) exhibited normal OGR
findings. The anatomical position, outlines, distribution and
motility of the stomach and small intestine were normal, with the
mucosa of the jejunum exhibiting feather-like or snowflake-like
characteristics and the mucosa of the ileum exhibiting strip-like
characteristics. The intestinal peristalsis was normal, with
gastrografin passing through the small intestine to the cecum in
60–90 min (Fig. 1).
Abnormal OGR findings in PC patients
with small intestinal function impairment
Of the 105 patients, 96 (91.4%) exhibited abnormal
OGR findings. A total of 29 cases (27.6%) exhibited limited
intestinal invasion, marginally stenotic small bowel and mucosal
deformities; 5 (4.8%) exhibited obvious mesenteric contracture,
ball-like changes, fixed position and disappearance of the
intestinal mucosa; 33 (31.4%) exhibited normal intestinal
peristalsis, mild intestinal aggregation and flattening of the
intestinal mucosa; 26 (24.8%) exhibited only mild mesenteric
contracture and mild slowing of the gastrointestinal peristalsis; 2
(1.9%) exhibited total pyloric obstruction and 1 (0.9%) exhibited
duodenal obstruction, with no contrast medium in the small
intestine.
In patients with limited intestinal invasion, the
involved small bowel loop became stenotic, with disordered mucosa
exhibiting serrated changes (Fig.
2A1, white arrows) and segmental intestinal dilation due to
incomplete obstruction (Fig. 2A2,
black arrows); however, the distribution of the bowels remained
normal. In cases with more severe small intestinal invasion,
incomplete intestinal obstruction with proximal bowel dilation was
observed (Fig. 2B2, black
arrows).
 | Figure 2.Oral gastrograffin radiography
findings in peritoneal carcinomatosis. (A) Limited intestinal
invasion, with signs of serrated changes of the mucosa in the
proximal jejunum (A1, white arrows) and segmental intestinal
dilation due to incomplete obstruction (A2, black arrows). (B) More
severe distal jejunum invasion, with dilation of the proximal
jejunum (B2, black arrows); the distribution and peristalsis of the
proximal jejunum were normal (B1, white arrows). (C) Intestinal
distribution, mild bowel aggregation and relatively fixed position
of the distal ileum at the right lower quadrant (C1, white arrow);
proximal jejunum at the left upper quadrant exhibiting a typical
stiff ‘3’ sign (C2, black arrows). (D) Intermediate mesenteric
contracture exhibiting the ‘cluster sign’ (D1, black ellipse); the
peristalsis and distribution were normal in the remaining intestine
(D2). (E) Asymmetric mucosa of the involved small bowel exhibiting
a half moon-shaped pressure recesses sign (E1, white arrow); the
involved small bowel exhibited a fixed position and fuzzy
intestinal mucosa (E2, black arrow). (F) The ascending colon
exhibited a distinct haustrum (F1, white arrows); ball-like sign of
mesenteric contracture with unclear boundary (F2, black arrows).
(G) Total obstruction of the distal intestine (G1, white arrows),
with petal-like mesenteric contracture (G2, black arrows). (H)
Significant stenosis of the terminal ileum and complete intestinal
obstruction (H1, black arrows). |
In patients with mild mesenteric contracture, the
small bowel loops became slightly aggregated and relatively fixed
(Fig. 2C1, white arrow), although the
distribution appeared normal. The wall of the involved intestines
appeared mildly stiff, with a typical stiff ‘3’ sign (Fig. 2C2, black arrows), although the small
bowel exhibited no stenosis and the intestinal mucosa was
relatively flat. The dynamic radiography revealed slow intestinal
peristalsis, with the contrast medium requiring >120 min to
reach the ileocecum.
In cases with intermediate mesenteric contracture,
the involved small intestines exhibited cluster buckling and
aggregation (Fig. 2D1, black
ellipse). The intestinal distribution appeared normal, without
expansion or stenosis. On dynamic radiographic observation, there
was slowing of the peristalsis of the involved intestine, whereas
the uninvolved intestinal loops appeared normal (Fig. 2D2).
In cases with mixed mesenteric contracture and
limited intestinal invasion, the involved small intestinal loops
became segmented and aggregated, leading to altered anatomical
positions. On dynamic observation, part of the involved small
intestine exhibited asymmetric stenosis, with a half moon-shaped
pressure recess sign in the mucosa (Fig.
2E1, white arrow); the aggregated intestines exhibited fixed
position and fuzzy intestinal mucosa (Fig. 2E2, black arrow).
In cases with severe mesenteric contracture, the
involved small intestinal loops became distinctly fixed and
aggregated, exhibiting ball-like or petal-like signs. The
intestinal mucosa was ill-defined and the jejunum and ileum could
not be easily defined. On dynamic observation, the intestinal
peristalsis was very slow, with the contrast agent mainly moving
due to gravity rather than through peristalsis. In certain cases
with more severe mesenteric invasion, the aggregated small
intestines exhibited a distinct ball-like change (Fig. 2F2, black arrows); other cases with
severe mesenteric invasion exhibited petal-like aggregates
(Fig. 2G2, black arrows), with total
obstruction of the distal intestine (Fig.
2G1, white arrows).
In cases of severe intestinal invasion, severe
stenosis or complete obstruction of the involved segment of the
small intestine was observed and the proximal bowel became markedly
expanded. On dynamic observation, there was enhanced reverse
peristalsis of the proximal intestine. There were also marked
intestinal cavity liquid gas planes (Fig.
2H).
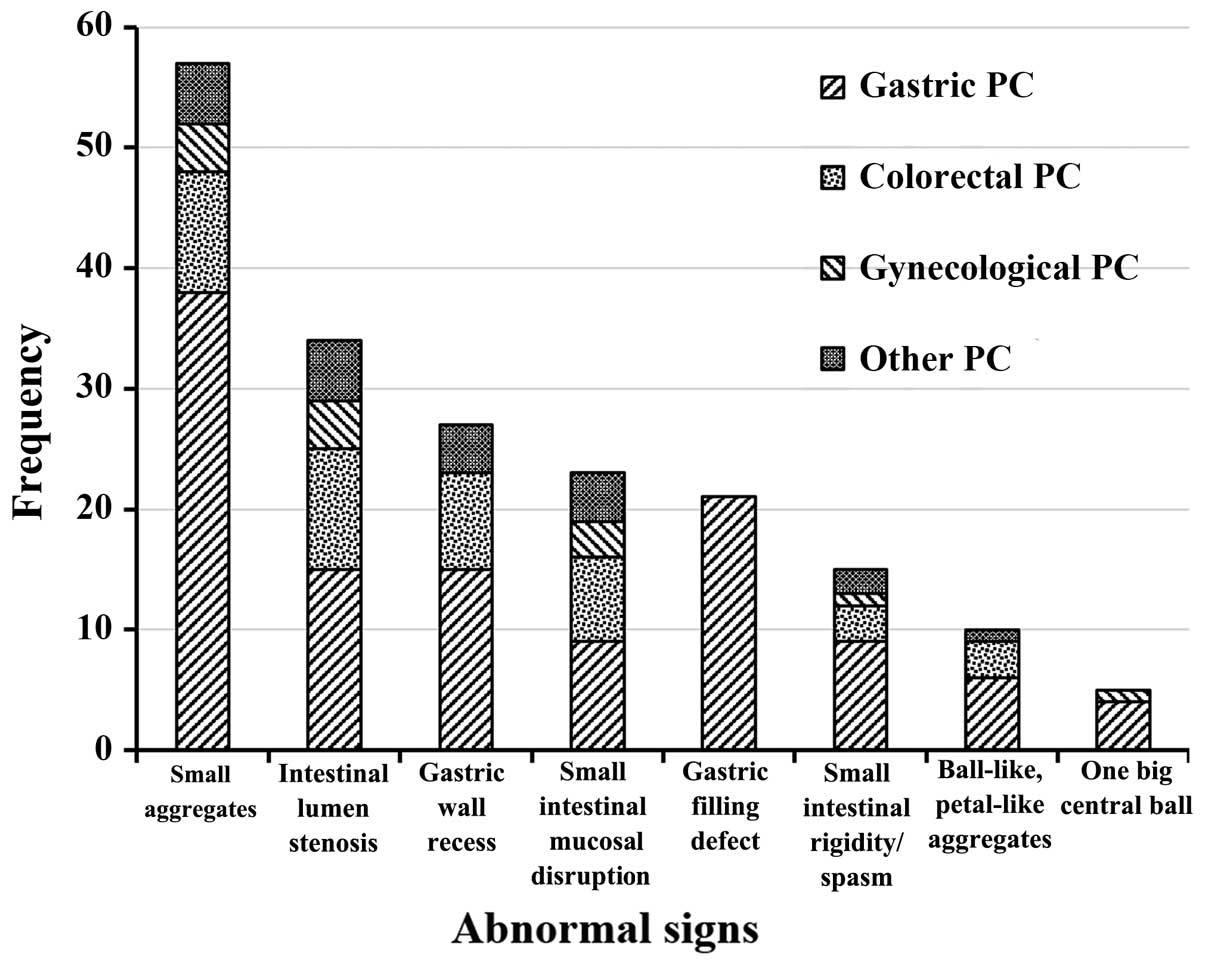
Statistical analysis of abnormal OGR
signs
Abnormal OGR signs were often composite, with a
total of 192 abnormal signs observed in this group. The frequency
of these OGR findings is presented in Fig. 3 and the detailed statistical analysis
is presented in Table II.
| Table II.Major abnormal findings on oral
gastrografin radiography in the 105 patients with peritoneal
carcinomatosis (PC). |
Table II.
Major abnormal findings on oral
gastrografin radiography in the 105 patients with peritoneal
carcinomatosis (PC).
| Abnormal findings,
no. (%) | Gastric PC
(n=54) | Colorectal PC
(n=28) | Gynecological PC
(n=9) | Other PC
(n=14) | P-value |
|---|
| Stomach |
|
|
|
|
|
| Filling
defect | 21 (38.9) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0.000 |
| Gastric
wall recess | 15 (27.8) | 8
(28.6) | 0 (0.0) | 4
(28.6) | 0.332 |
| Reduced
motility/stagnation | 38 (70.4) | 16 (57.1) | 3 (33.3) | 10 (71.4) | 0.138 |
| Small
intestine |
|
|
|
|
|
|
Intestinal wall
rigidity/spasm | 9
(16.7) | 3
(10.7) | 1 (11.1) | 2
(14.3) | 0.893 |
| Mucosal
disruption | 9
(16.7) | 7
(25.0) | 3 (33.3) | 4
(28.6) | 0.557 |
| Luminal
stenosis | 15 (27.8) | 10 (35.7) | 4 (44.4) | 5
(35.7) | 0.630 |
| Reduced
peristalsis/stagnation | 38 (70.4) | 19 (67.9) | 5 (55.6) | 12 (85.7) | 0.635 |
| Mesenteric
contracture |
|
|
|
|
|
| Small
aggregates | 38 (70.4) | 10 (35.7) | 4 (44.4) | 5
(55.6) | 0.008 |
|
Ball-like, petal-like
aggregates | 6
(11.1) | 3
(10.7) | 0 (0.0) | 1
(7.1) | 0.743 |
| One
large central ball | 4
(7.4) | 0 (0.0) | 1 (11.1) | 0
(0.0) | 0.292 |
Comparison between OGR and
clinicopathological findings
In the 96 cases with abnormal OGR findings, a total
of 192 typical abnormal signs were recorded. These abnormal signs
were further compared with the intraoperative findings. In 87 cases
(82.9%), the ORG findings were in accordance with the
intraoperative findings (κ=0.726, P<0.001) (Fig. 4). Among the 18 cases with discordant
findings, 17 (16.2%) were underestimated by OGR and turned out to
be more severe during surgery, whereas 1 case (0.9%) was
overestimated as severe mesenteric contracture on ORG and was found
to be intermediate mesenteric contracture during surgery. Among the
17 underestimated cases, 9 (8.6%) were upstaged from normal to mild
mesenteric contracture, 2 (1.9%) were upstaged from normal to
intermediate mesenteric contracture, 2 (1.9%) with mild intestinal
expansion and limited intestinal wall invasion were upstaged from
mild to intermediate mesenteric contracture, 2 (1.9%) were upstaged
from mild to severe mesenteric contracture and 2 (1.9%) were
upstaged from intermediate to severe mesenteric contracture.
Discussion
The present study has developed a simple but useful
technique for evaluating the functional impacts of PC on the
gastrointestinal system, with the aim to optimize the selection of
candidate patients for CRS+HIPEC therapy. Dynamic OGR exhibited
several major abnormal radiological findings, including reduced
peristalsis/stagnation of the stomach and intestines, gastric wall
recess, small intestinal aggregates, luminal stenosis, mucosal
disruption and various degrees of mesenteric contracture. These
signs are not evenly distributed and are usually more prominent in
PC from gastric cancer. Patients with gastric PC exhibited a
significantly higher frequency of stomach filling defects (38.9%,
21/54) and small intestinal aggregates secondary to mesenteric
contracture (70.4%, 38/54) compared with those with PC from other
malignancies. This may reflect the different and more aggressive
biological behavior of gastric PC, as advanced gastric cancer may
result in early intraperitoneal dissemination and trigger
mesenteric contracture of the small intestine (17).
There are other non-invasive imaging techniques to
display the anatomical or functional abnormalities in the abdomen
caused by PC (18,19). Among these, CT-, magnetic resonance
imaging (MRI)- and positron emission tomography (PET)/CT-based
techniques are commonly used (20,21). CT is
the most commonly used technology in clinical practice due to its
advantages, such as superior spatial resolution, shorter imaging
times (22), wide availability and
clinical familiarity (18); its
disadvantages, however, are low sensitivity for small tumor nodules
and mesenteric deposits. Similarly, MRI has several technical
advantages, including superior contrast resolution, multiple
imaging types and manipulation of signal intensities; however, its
disadvantages include low sensitivity for small tumors, longer
imaging times, movement artifacts and lower spatial resolution
(23,24). As a functional imaging examination,
PET/CT exhibits higher sensitivity compared with MRI and CT, but is
associated with technical disadvantages, such as low specificity
and spatial resolution for small tumors, high cost and limited
availability (25,26). These technologies share one common
disadvantage, i.e., they are static technologies showing the sites
and severity of PC, but not the dynamic impacts of PC on
gastrointestinal function, as respiratory movements may produce
artifacts, compromising the image quality.
In comparison, OGR may help evaluate PC from another
perspective. This simple technique may be used to observe the
motility of the stomach and intestines, location, mucosal
manifestations and extent of tumor invasion under dynamic
conditions. Therefore, the OGR-based functional evaluation and the
CT- or MRI-based anatomical evaluation may complement each other,
making patient selection more reliable.
The practical advantages of OGR are evident. First,
the procedure is safe. Barium sulfate is currently a routinely used
clinical gastrointestinal contrast agent. This agent is not
dissolved in water and must be eliminated from the body. In PC
patients, barium sulfate may exacerbate small intestinal
obstruction. As this study focuses on patients with PC or suspected
PC with potential intestinal obstruction, barium sulfate should not
be used as a contrast agent. Instead, the water-soluble contrast
medium gastrografin is a safe, practical and useful alternative.
Second, gastrografin is easy to use. The patients undergo a simple
preparation, drink the medium and stand before the widely available
digital radiography machine for real-time observation of the
dynamic functions of the gastrointestinal tract. Other complex
procedures may be avoided. Third, the procedure is cost-effective.
As PC patients often have to undergo a series of complex
examinations and tests before a rational treatment decision can be
made, developing a low-cost and easy-to-use radiographic technology
meets the clinical priority. Fourth, gastrografin exerts a
potential therapeutic effect. Gastrografin is a conventional
hyperosmolar contrast medium with pharmacological effects when
administered orally. The osmotic pressure is ~1,900 mOsm/l in the
intestinal lumen (6 times more than the extracellular fluid osmotic
pressure) (27). Gastrografin may
cause drainage of the extracellular and intravascular fluid to the
intestine, diluting and increasing the intestinal contents, while
reducing local edema, increasing intestinal pressure gradients,
stimulating bowel peristalsis and relieving bowel obstruction
(28–30). Other effects include inhibition of
cholinesterase and release of histamine (31–33) to
improve bowel movement. In our experience, a proportion of the
patients experienced partial relief of their intestinal obstruction
following OGR. These advantages make ORG a practical and valuable
technology in the clinical setting.
In conclusion, OGR provides dynamic information on
the functional impact of PC on the gastrointestinal system. To the
best of our knowledge, this is the first study to assess the
functional impacts of PC using a simple technique. However, further
studies are required to develop and validate this technology.
Acknowledgements
This study was supported by the Specialized Research
Fund of the Doctoral Program of Higher Education, Ministry of
Education of China (grant no. 20120141110042), the Science Fund for
Creative Research Groups of the Hubei Province Natural Science
Foundation of China (grant no. 2012FFB04314) and the Key Project of
the Fundamental Research Fund for the Central Universities (grant
no. 303274028).
References
|
1
|
Koppe MJ, Boerman OC, Oyen WJ and
Bleichrodt RP: Peritoneal carcinomatosis of colorectal origin:
incidence and current treatment strategies. Ann Surg. 243:212–222.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Huang B, Sun Z, Wang Z, et al: Factors
associated with peritoneal metastasis in non-serosa-invasive
gastric cancer: a retrospective study of a prospectively-collected
database. BMC Cancer. 13:572013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Yang XJ, Li Y and Yonemura Y:
Cytoreductive surgery plus hyperthermic intraperitoneal
chemotherapy to treat gastric cancer with ascites and/or peritoneal
carcinomatosis: Results from a Chinese center. J Surg Oncol.
101:457–464. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Yang XJ, Li Y, al-shammaa Hassan AH, et
al: Cytoreductive surgery plus hyperthermic intraperitoneal
chemotherapy improves survival in selected patients with peritoneal
carcinomatosis from abdominal and pelvic malignancies: results of
21 cases. Ann Surg Oncol. 16:345–351. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Huang CQ, Feng JP, Yang XJ and Li Y:
Cytoreductive surgery plus hyperthermic intraperitoneal
chemotherapy improves survival of patients with peritoneal
carcinomatosis from colorectal cancer: a case-control study from a
Chinese center. J Surg Oncol. 109:730–739. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Yang XJ, Huang CQ, Suo T, et al:
Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy
improves survival of patients with peritoneal carcinomatosis from
gastric cancer: final results of a phase III randomized clinical
trial. Ann Surg Oncol. 18:1575–1581. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Esquivel J, Elias D, Baratti D, Kusamura S
and Deraco M: Consensus statement on the loco regional treatment of
colorectal cancer with peritoneal dissemination. J Surg Oncol.
98:263–267. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Huang JY, Xu YY, Sun Z, et al: Comparison
different methods of intraoperative and intraperitoneal
chemotherapy for patients with gastric cancer: a meta-analysis.
Asian Pac J Cancer Prev. 13:4379–4385. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Pannu HK, Horton KM and Fishman EK: Thin
section dual-phase multidetector-row computed tomography detection
of peritoneal metastases in gynecologic cancers. J Comput Assist
Tomogr. 27:333–340. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Marin D, Catalano C, Baski M, et al:
64-Section multi-detector row CT in the preoperative diagnosis of
peritoneal carcinomatosis: correlation with histopathological
findings. Abdom Imaging. 35:694–700. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Franiel T, Diederichs G, Engelken F,
Elgeti T, Rost J and Rogalla P: Multi-detector CT in peritoneal
carcinomatosis: diagnostic role of thin slices and multiplanar
reconstructions. Abdom Imaging. 34:49–54. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
de Bree E, Koops W, Kroger R, van Ruth S,
Witkamp AJ and Zoetmulder FA: Peritoneal carcinomatosis from
colorectal or appendiceal origin: correlation of preoperative CT
with intraoperative findings and evaluation of interobserver
agreement. J Surg Oncol. 86:64–73. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Coakley FV, Choi PH, Gougoutas CA, et al:
Peritoneal metastases: detection with spiral CT in patients with
ovarian cancer. Radiology. 223:495–499. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Carmignani CP, Sugarbaker TA, Bromley CM
and Sugarbaker PH: Intraperitoneal cancer dissemination: mechanisms
of the patterns of spread. Cancer Metastasis Rev. 22:465–472. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kapoor S, Jain G, Sewkani A, Sharma S,
Patel K and Varshney S: Prospective evaluation of oral gastrografin
in postoperative small bowel obstruction. J Surg Res. 131:256–260.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Sugarbaker PH: Cytoreductive surgery and
peri-operative intraperitoneal chemotherapy as a curative approach
to pseudomyxoma peritonei syndrome. Eur J Surg Oncol. 27:239–243.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Roviello F, Caruso S, Neri A and Marrelli
D: Treatment and prevention of peritoneal carcinomatosis from
gastric cancer by cytoreductive surgery and hyperthermic
intraperitoneal chemotherapy: overview and rationale. Eur J Surg
Oncol. 39:1309–1316. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Yan TD, Morris DL, Shigeki K, Dario B and
Marcello D: Preoperative investigations in the management of
peritoneal surface malignancy with cytoreductive surgery and
perioperative intraperitoneal chemotherapy: Expert consensus
statement. J Surg Oncol. 98:224–227. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Liu Y, Endo Y, Fujita T, et al:
Cytoreductive surgery under aminolevulinic acid-mediated
photodynamic diagnosis plus hyperthermic intraperitoneal
chemotherapy in patients with peritoneal carcinomatosis from
ovarian cancer and primary peritoneal carcinoma: Results of a phase
I trial. Ann Surg Oncol. 21:4256–4262. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Klumpp BD, Aschoff P, Schwenzer N, et al:
Peritoneal carcinomatosis: comparison of dynamic contrast-enhanced
magnetic resonance imaging with surgical and histopathologic
findings. Abdom Imaging. 37:834–842. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Dirisamer A, Schima W, Heinisch M, et al:
Detection of histologically proven peritoneal carcinomatosis with
fused 18F-FDG-PET/MDCT. Eur J Radiol. 69:536–541. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Funicelli L, Travaini LL, Landoni F,
Trifiro G, Bonello L and Bellomi M: Peritoneal carcinomatosis from
ovarian cancer: the role of CT and [18F] FDG-PET/CT.
Abdom Imaging. 35:701–707. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Bozkurt M, Doganay S, Kantarci M, et al:
Comparison of peritoneal tumor imaging using conventional MR
imaging and diffusion-weighted MR imaging with different b values.
Eur J Radiol. 80:224–228. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Wu Y, Yue X, Shen W, et al: Diagnostic
value of diffusion-weighted MR imaging in thyroid disease:
application in differentiating benign from malignant disease. BMC
Med Imaging. 13:232013. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Sanli Y, Turkmen C, Bakir B, et al:
Diagnostic value of PET/CT is similar to that of conventional MRI
and even better for detecting small peritoneal implants in patients
with recurrent ovarian cancer. Nucl Med Commun. 33:509–515. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kitajima K, Suenaga Y, Ueno Y, et al:
Value of fusion of PET and MRI in the detection of intra-pelvic
recurrence of gynecological tumor: comparison with
18F-FDG contrast-enhanced PET/CT and pelvic MRI. Ann
Nucl Med. 28:25–32. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Khasawneh MA, Ugarte ML, Srvantstian B,
Dozois EJ, Bannon MP and Zielinski MD: Role of gastrografin
challenge in early postoperative small bowel obstruction. J
Gastrointest Surg. 18:363–368. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Ha HK, Kim JS, Lee MS, et al:
Differentiation of simple and strangulated small-bowel
obstructions: usefulness of known CT criteria. Radiology.
204:507–512. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Fevang BT, Fevang J, Stangeland L, Soreide
O, Svanes K and Viste A: Complications and death after surgical
treatment of small bowel obstruction: A 35-year institutional
experience. Ann Surg. 231:529–537. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Rahmani N, Mohammadpour RA, Khoshnood P,
Ahmadi A and Assadpour S: Prospective evaluation of oral
gastrografin (R) in the management of postoperative adhesive small
bowel obstruction. Indian J Surg. 75:195–199. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Stordahl A, Laerum F, Gjolberg T and Enge
I: Water-soluble contrast media in radiography of small bowel
obstruction. Comparison of ionic and non-ionic contrast media. Acta
Radiol. 29:53–56. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Chen SC, Lin FY, Lee PH, Yu SC, Wang SM
and Chang KJ: Water-soluble contrast study predicts the need for
early surgery in adhesive small bowel obstruction. Br J Surg.
85:1692–1694. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Assalia A, Schein M, Kopelman D, Hirshberg
A and Hashmonai M: Therapeutic effect of oral gastrografin in
adhesive, partial small-bowel obstruction: a prospective randomized
trial. Surgery. 115:433–437. 1994.PubMed/NCBI
|