Introduction
Breast cancer is one of the most common cancers in
women, and the lung is one of the most prevalent sites of breast
cancer metastasis (1,2), which may recur after a long
disease-free period following locoregional treatment (1,2). We
herein present the cases of 2 breast cancer patients with pulmonary
metastasis that simulated primary lung adenocarcinoma. These
metastatic lesions were detected by mass screening 21 and 19 years
after surgical resection of the primary breast cancers. At first,
the nodules were considered as primary lung adenocarcinomas, as
they shared similar radiological findings, such as irregular
margins and a bronchus leading to the nodule (bronchus sign).
Metastatic breast cancer may exhibit the characteristic signs of
pulmonary lung adenocarcinoma. Although rare, pulmonary metastasis
from breast cancer should be considered even in the presence of
irregularly shaped nodule(s).
Case reports
Case 1
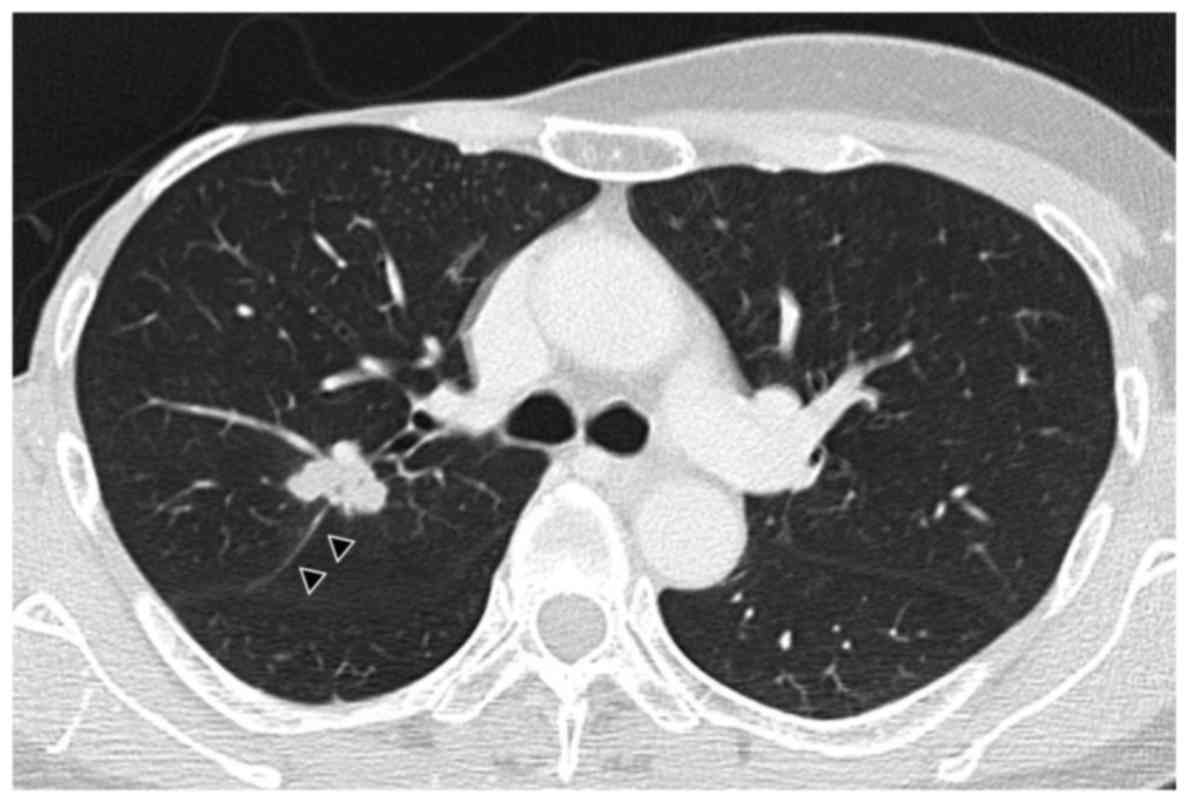
A 54-year-old woman was referred to our hospital in
January, 2016 due to a nodule identified on a chest radiograph
during a mass screening. The patient had undergone a right modified
radical mastectomy for breast cancer 21 years prior. The chest CT
scan revealed a nodule sized 20 mm with a well-defined, irregular
margin in S2 of the right lung (Fig.
1) without enlargement of the mediastinal lymph nodes. The
nodule exhibited notching, lobulation, spicular formation, pleural
indentation, and the bronchus sign. The lesion was suspected to be
either primary lung adenocarcinoma or metastatic tumor and, thus,
transbronchial biopsy was performed. As the pathological results
suggested that the nodule was metastatic, thoracoscopic surgery was
performed. At final histology, the tumor was found to be a
metastasis from breast cancer, and immunohistochemical
investigation revealed that it was positive for estrogen receptor.
The histopathological findings were compared with those in the
surgically resected specimen 21 years prior and were found to be
the same. Thereafter, the patient received systemic chemotherapy
with the aromatase inhibitor letrozole, and is currently alive with
stable disease.
Informed consent regarding the publication of the
case details was obtained from the patient.
Case 2
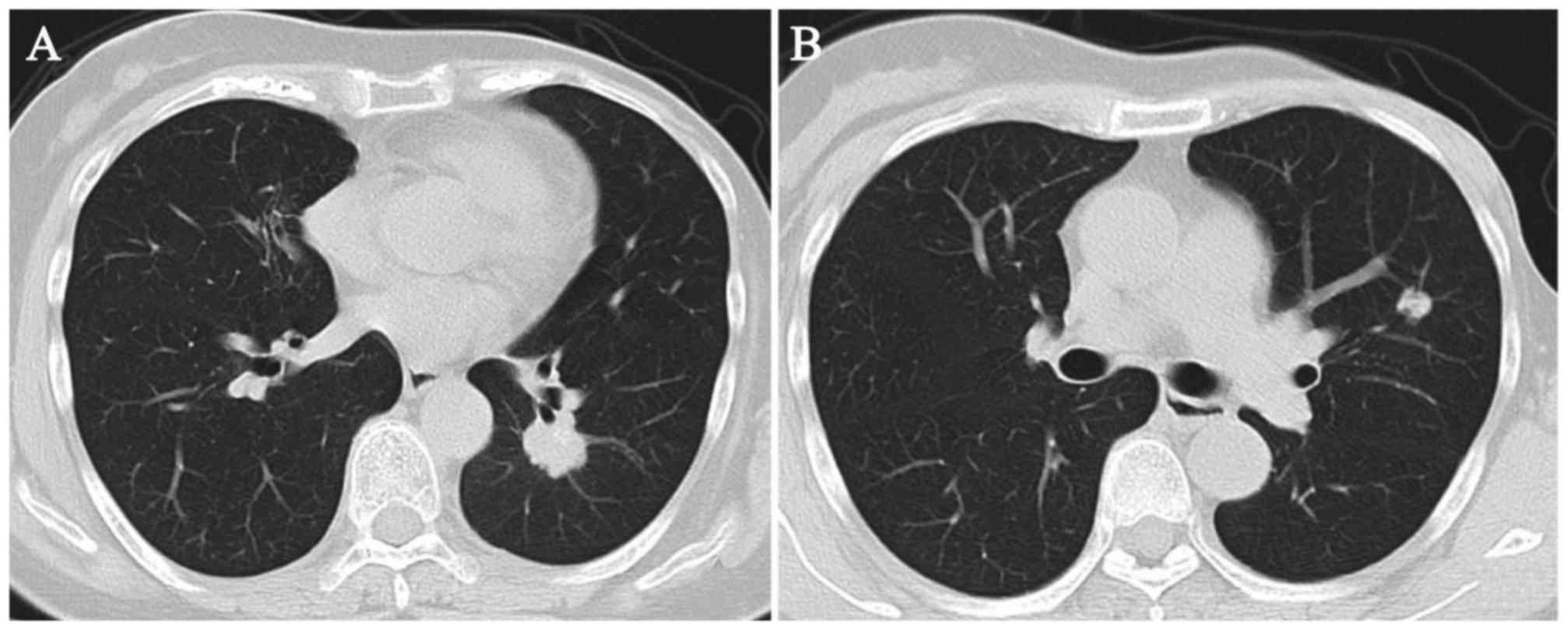
A 68-year-old woman was referred to our hospital in
November, 2015 due to three pulmonary nodules identified on a chest
radiograph taken during a mass screening. The patient had undergone
a left radical mastectomy for breast cancer 19 years prior. The
chest CT scan revealed a 28-mm nodule in the left lower lobe, a
21-mm nodule in the left upper lobe, and a 21-mm right lingular
nodule (Fig. 2), without enlargement
of the mediastinal lymph nodes. The nodules exhibited notching and
the bronchus sign. Primary lung adenocarcinoma or metastatic tumor
was suspected and, thus, transbronchial biopsy of the lingular
nodule was performed. At final histology, the lesion was found to
be a metastasis from breast cancer, and immunohistochemical
investigation revealed that the tumor was positive for estrogen and
progesterone receptors. Thereafter, the patient received systemic
chemotherapy with the aromatase inhibitor anastrozole, and is
currently alive with stable disease.
Informed consent regarding the publication of the
case details was obtained from the patient.
Discussion
Breast cancer is one of the most common cancers in
women and may be associated with various thoracic manifestations,
either from treatment, its complications, or tumor recurrence and
metastasis (3). Lymphangitic
metastasis, multiple nodules and a solitary nodule are the most
frequently observed patterns of pulmonary metastasis from breast
cancer (1–4). Lymphangitic lung metastasis of breast
cancer usually appears as reticular or reticulonodular interstitial
markings, or interlobar septal thickening (Kerley B lines) on
imaging (3). Other patterns of
pulmonary metastasis, such as a solitary or multiple pulmonary
nodules, occur by means of hematogenous spread. The presence of
lung metastasis is a major factor when considering treatment
options for breast cancer. Thus, the accurate diagnosis of thoracic
manifestations in patients with breast cancer is crucial.
Solitary or multiple pulmonary nodules are generally
spherical or ovoid, vary in size, are sharply demarcated, and are
located mostly in the periphery of the lung (5–8). In
primary lung adenocarcinoma, notching and irregularity of the
nodule margins is commonly observed, whereas a smooth margin is a
sign of metastatic tumor, which results from hematogenous tumor
spread. Pleural indentation and the bronchus sign are also known to
be characteristic signs of primary lung adenocarcinoma on CT
scan.
Development of a solitary pulmonary nodule in
patients previously treated for breast cancer may represent
something other than recurrent disease. Casey et al
(9) found that 52% of breast cancer
patients presenting with a solitary pulmonary nodule had primary
lung cancer, 43% had metastatic breast cancer and 5% had benign
lesions. Histological confirmation is required for correct
diagnosis and treatment and lung biopsy is considered when there
are unexplained signs and symptoms with atypical radiographic
characteristics that are usually progressive or rapidly
deteriorating. According to Fujii et al, there are few
reported cases of cancer recurrence after >15 years of
disease-free survival following locoregional treatment of breast
cancer (10). That study reported a
case of lung metastasis from breast cancer after an 18-year
disease-free interval (10). Tomita
et al reported a case of pulmonary metastasis from breast
cancer following an 18-year disease-free interval that responded to
tamoxifen treatment (11). In our
cases, both patients presented with cancer recurrence after >15
years of disease-free survival following locoregional treatment of
breast cancer. Although very rare, development of a sole pulmonary
metastasis after a long-term interval from the diagnosis of breast
cancer is possible. The precise mechanism underlying cancer
recurrence after long-term disease-free survival has not been fully
elucidated.
Of note, in our patients, the metastatic lesions
were irregularly shaped nodules. These radiographic findings were
clearly different from those of pulmonary metastasis from breast
cancer, and similar to those of primary lung adenocarcinoma. To the
best of our knowledge, a similar case has not been reported in the
English medical literature to date. Based on the present study, we
recommend that metastatic lesion from breast cancer be considered
in the differential diagnosis of a solitary or multiple pulmonary
nodules with irregularly shaped margins and vascular convergence,
particularly in patients with breast cancer and those with a
history of breast cancer.
References
|
1
|
Kreisman H, Wolkove N, Finkelstein HS,
Cohen C, Margolese R and Frank H: Breast cancer and thoracic
metastases: Review of 119 patients. Thorax. 38:175–179. 1983.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kamby C, Vejborg I, Kristensen B, Olsen LO
and Mouridsen HT: Metastatic pattern in recurrent breast cancer.
Special reference to intrathoracic recurrences. Cancer.
62:2226–2233. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Jung JI, Kim HH, Park SH, Song SW, Chung
MH, Kim HS, Kim KJ, Ahn MI, Seo SB and Hahn ST: Thoracic
manifestations of breast cancer and its therapy. Radiographics.
24:1269–1285. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ohnishi H, Haruta Y, Yokoyama A, Nakashima
T, Hattori N and Kohno N: Metastatic breast cancer presenting as
air-space consolidation on chest computed tomography. Intern Med.
48:727–731. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Herold CJ, Banier AA and Fleischmann D:
Lung metastasis. Eur Radiol. 6:596–606. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Davis SD: CT evaluation for pulmonary
metastases in patients with extrathoracic malignancy. Radiology.
180:1–12. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Connolly JE Jr, Erasmus JJ and Patz EF Jr:
Thoracic manifestations of breast carcinoma: Metastatic disease and
complications of treatment. Clin Radiol. 54:487–494. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Seo JB, Im J, Goo JM, Chung MJ and Kim MY:
Atypical pulmonary metastases: Spectrum of radiologic findings.
Radiographics. 21:403–417. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Casey JJ, Stempel BG, Scanlon EF and Fry
WA: The solitary pulmonary nodule in the patient with breast
cancer. Surgery. 96:801–805. 1984.PubMed/NCBI
|
|
10
|
Fujii T, Yajima R, Yamaki E, Kohsaka T,
Yamaguchi S, Tsutsumi S, Mogi A, Asao T and Kuwano H: Pulmonary
metastasis from breast cancer with an 18-year disease-free
interval: Implication of the role of surgery. Int Surg. 97:281–284.
2012. View
Article : Google Scholar : PubMed/NCBI
|
|
11
|
Tomita M, Matsuzaki Y, Edagawa M, Maeda M,
Shimizu T, Hara M, Yamamoto A and Onitsuka T: A case of pulmonary
metastasis from breast cancer following an 18-year disease-free
interval that responded to tamoxifen treatment. Breast Cancer.
9:82–85. 2002. View Article : Google Scholar : PubMed/NCBI
|