Introduction
Paclitaxel serves an important role in the treatment
of advanced non-small cell lung cancer (NSCLC) (1). Use of this drug, however, is greatly
limited by its solvent-based formulation with respect to Cremophor
EL® (BASF, Ludwigshafen am Rhein, Germany), which
produces serious and dose limiting toxicities. Administration of
solvent-based paclitaxel routinely requires long infusion sets
(tubing and in-line filters), premedication with steroids and
antihistamines to prevent hypersensitivity reactions. Nanoparticle
albumin-bound paclitaxel (Nab-PTX) is an albumin-bound formulation
of paclitaxel that is readily soluble in saline. This formulation
allows the administration of paclitaxel without the use of
lipid-based solvents or the need for corticosteroid and
antihistamine pre-medication (2).
When administered as In the first-line therapy for
patients with NSCLC, nab-PTX, in combination with other platinum
reagents, showed has exhibited significant efficacy in improving
prognosis as well as in reducing toxicity profiles (3–5). Thus,
platinum-based doublet regimens have been widely applied in the
first-line treatment of patients with advanced NSCLC.
However, little is currently known regarding the
effect of single-agent nab-PTX targeting advanced NSCLC. The phase
I/II study of weekly single-agent nab-PTX administered to patients
with advanced NSCLC as an initial chemotherapy revealed that the
overall response rate (ORR) was 30%, the median progression free
survival (PFS) time was 5 months and the median overall survival
(OS) time was 11 months (6).
Concerning subsequent treatments, to date, there are only a small
number of clinical trials of single-agent nab-PTX.
Hu et al (7)
conducted a phase II clinical trial and reported an ORR of 16.1%, a
median PFS of 3.5 months and a median OS of 6.8 months.
Furthermore, Sakata et al (8)
reported an ORR of 31.7%, a median PFS of 4.9 months and a median
OS of 13.0 months. However, as these studies are relatively recent
(2015–2016) with limited sample sizes, further clinical data are
required in order to determine the optimal treatment strategy for
the application of single-agent nab-PTX in patients with
platinum-resistant NSCLC.
The aim of the current retrospective study was to
investigate the efficacy and toxicity of weekly administration of
single-agent nab-PTX in patients with platinum-resistant NSCLC.
Patients and methods
A retrospective study was performed of patients with
platinum-resistant NSCLC who were treated with single-agent nab-PTX
between August 2013 and December 2015 at the Kansai Medical
University Hospital (Osaka, Japan). Eligible patients had a
diagnosis of platinum-resistant NSCLC. Exclusion criteria included
patients who had not received prior treatment or had been treated
with combination chemotherapy. Patients were assessed with respect
to their clinical stage at the time of diagnosis, according to 7th
lung cancer TNM classification (9).
This retrospective clinical study was conducted in accordance with
the Declaration of Helsinki and the requirements of the local
institutional review board of Kansai Medical University Hospital,
and received approval from the Ethics Committee of Kansai Medical
University.
Treatment
Patients received nab-PTX at a dose of 100
mg/m2 on days 1, 8 and 15 of a 21-day cycle. The drug
was administered as an intravenous infusion over 30 min without
corticosteroid or antihistamine pre-medication. The treatment was
repeated every four weeks until disease progression was observed or
unacceptable toxicity happened.
Study assessments
Patient treatment response was evaluated according
to the Response Evaluation Criteria In Solid Tumors (10) via whole-body computerized tomography
scans performed every 8–12 weeks until treatment cessation.
Toxicity evaluation was based on the Common Toxicity Criteria for
Adverse Events version 4.0 (CTCAE v4.0) (http://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm#ctc_40).
Statistical analysis
OS was calculated as the duration between the
initiation of single-agent nab-PTX treatment and patient mortality
the date of the final follow-up, and PFS was calculated as the
duration from the initiation of treatment to the objective
progression of disease. Survival curves were created using the
Kaplan-Meier method, and differences between the groups were
evaluated using the log-rank test. All statistical tests were
two-sided, P<0.05 was considered to indicate a statistically
significant difference and 95% confidence intervals were
calculated. All statistical analyses were performed using EZR
(Saitama Medical Center, Jichi Medical University, Saitama, Japan),
which is a graphical user interface for R version 2.13.0 (The R
Foundation for Statistical Computing). More precisely, it is a
modified version of R Commander (version 1.6–3), designed to add
the statistical functions frequently used in biostatistics.
Results
Patients
The clinical characteristics of the patients
involved in this study are listed in Table I. A total of 67 patients were
enrolled, with a median age of 68 years (range, 44–85 years); 18%
were female and 82% were male. The percentage of patients with
adenocarcinoma was 58%, and with squamous carcinoma was 31%. The
remaining 11% of patients had an undetermined diagnosis of
adenocarcinoma or squamous carcinoma, or mixed characteristics of
each. The proportion of patients with stage III disease was 48%,
and of those with stage IV disease was 42%, at the stage of
diagnosis. EGFR mutation status was evaluated in all patients with
adenocarcinoma, 6% of whom were identified as having an exon 19
deletion, and 3% of whom had L858R in exon 21. Overall, 22% of
patients had received one prior regimen and 78% had received >2
regimens. Treatment was imitated once the diagnosis was confirmed;
platinum-based doublet therapy constituted the first-line therapy,
and docetaxel or pemetrexed monotherapy followed as a second line
therapy. If patients had an EGFR gene mutation, they were treated
with an EGFR-TKI. The median treatment duration was 4.1 months
(range, 1.9–19.2 months). The median follow up duration was 8.7
months (range, 2.3–30.0 months).
 | Table I.Patients' characteristics. |
Table I.
Patients' characteristics.
| Categories | n, % |
|---|
| n | 67 |
| Median age, years
(range) | 68 (44–85) |
| Sex (%) |
|
| Male | 82 |
|
Female | 18 |
| ECOG PS (%) |
|
| 0–1 | 79 |
| 2 | 21 |
| Histology (%) |
|
|
Adenocarcinoma | 58 |
| Squamous
carcinoma | 31 |
|
Others | 11 |
| Stage (%) |
|
| I | 6 |
| II | 4 |
| III | 48 |
| IV | 42 |
| Postoperative
recurrence (%) | 13 |
| EGFR mutation status
(%) |
|
| Exon19
deletion | 6 |
| L858R in
exon21 | 3 |
| Smorking history
(%) |
|
|
Smorker | 84 |
|
Non-smorker | 16 |
| Number of prior
regimens (%) |
|
| 1 | 22 |
| ≤2 | 78 |
| Previous taxane
(%) |
|
| Yes | 16 |
| No | 84 |
| Median Treatment
durations, months (range) | 4.1 (1.0–19.2) |
| Median Treatment
cycles, n (range) | 3.6 (1.0–13.6) |
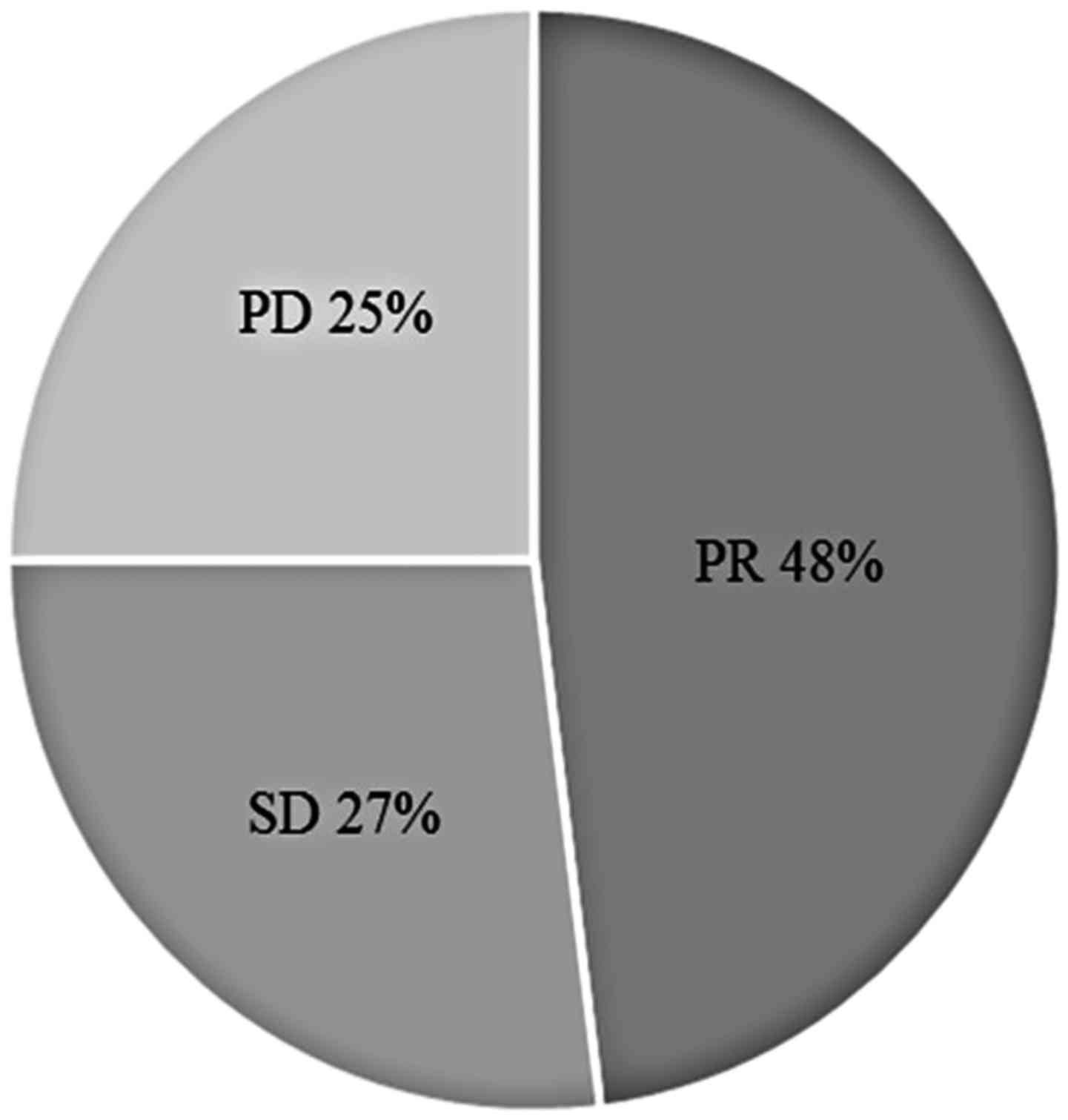
Response and survival
Treatment efficacy is summarized in Fig. 1. In total, 48% of patients manifested
a partial response (PR) but none exhibited a complete response
(CR); 27% of patients had stable disease (SD). The median PFS was
determined to be 4.8 months (range, 3.8–5.6 months; Fig. 2A), and the median OS was 18.2 months
(minimum, 10.4 months; Fig. 2B).
According to histological analysis, the median PFS was 5.1 months
for patients with non-squamous carcinoma (range, 4.0–6.7 months)
and 3.8 months for patients with squamous carcinoma (range, 3.4–5.6
months; P=0.546; Fig. 2C). The
median PFS was 4.0 months for nab-PTX administered as second-line
chemotherapy (range, 2.1–9.2 months) and 4.9 months as a third-line
or later treatment (range, 3.8–5.8 months; P=0.541; Fig. 2D).
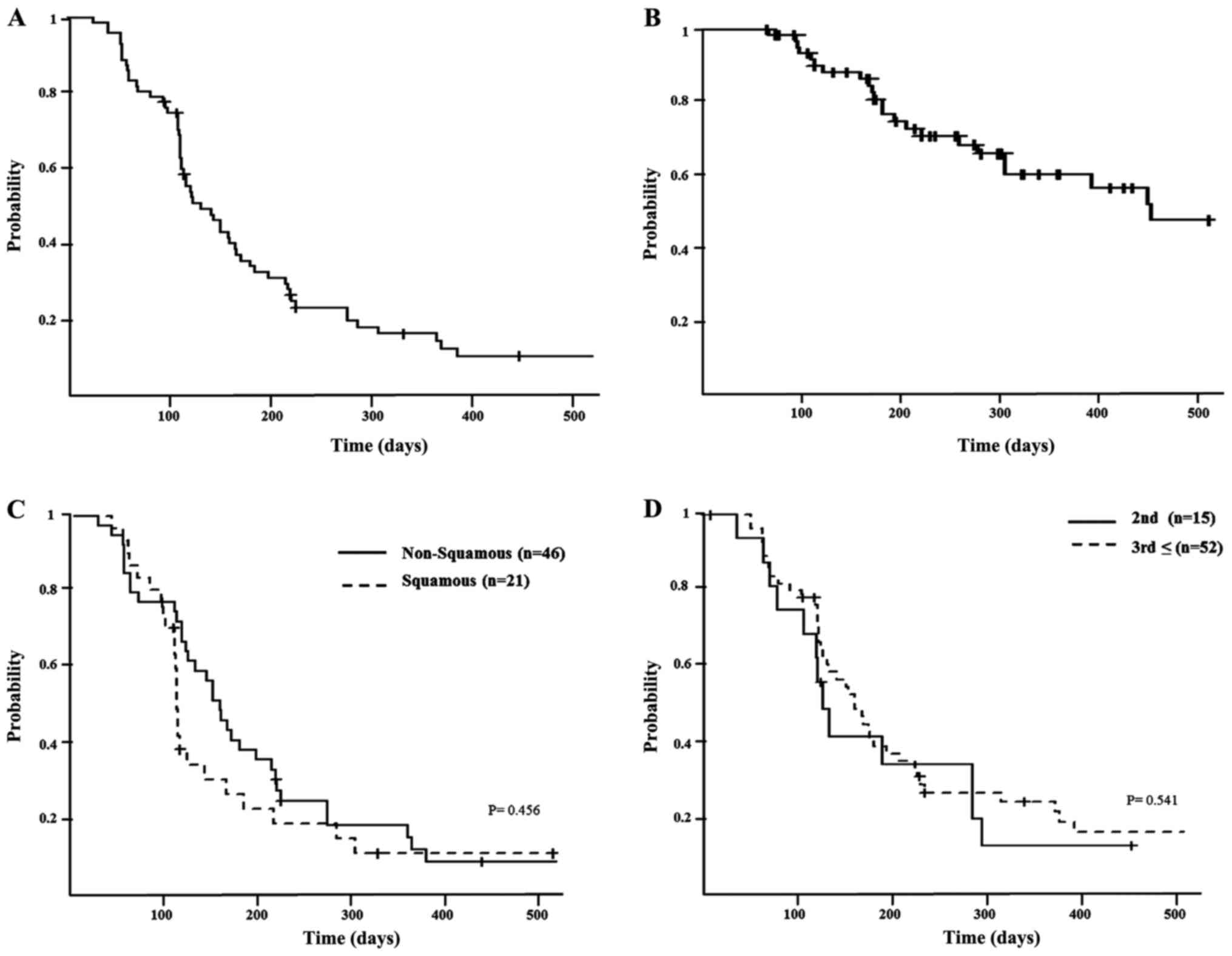 | Figure 2.(A) Kaplan-Meier graphs for PFS.
Median PFS was 4.8 months (range, 3.8–5.6 months). (B) Kaplan-Meier
graphs for OS. Median OS was 18.2 months (range, 10.4 months; data
not presented). (C) Kaplan-Meier graphs for the PFS of patients
with advanced non-squamous cell carcinoma and squamous carcinoma.
The median PFS for non-squamous was 5.1 months (range, 4.0–6.7
months), and for squamous it was 3.8 months (range, 3.4–5.6
months). There was no statistically significant difference
(P=0.456). (D) Kaplan-Meier graphs for the PFS of patients with
second-line and post-second-line therapy. The median PFS for
second-line was 4.0 months (range, 2.1–9.2 months), and for
post-second-line this was 4.9 months (range, 3.8–5.8 months). There
was no statistically significant difference (P=0.541). PFS,
progression-free survival; OS, overall survival. |
Frequency of adverse events
The frequencies of adverse events (AEs) are detailed
in Table II. In the patient cohort
studied, the most common nab-PTX-associated AE (grade ≤3) was
neutropenia (29.9%), followed by interstitial lung disease (6%),
infection (6%) and fatigue (6%). There was no fatal case recorded
in the present study that was associated with AEs. However, 39.4%
of patients were required to receive reduce doses or cease
treatment due to AEs.
| Table II.Toxicities of Nab-PTX presenting as
percentage of patients with adverse events. |
Table II.
Toxicities of Nab-PTX presenting as
percentage of patients with adverse events.
|
| NCI-CTC grade
(%) |
|---|
|
|
|
|---|
| Toxicity | Grade 1 | Grade 2 | Grade 3 | Grade 4 | Grade 5 |
|---|
| Neutropenia | 6.0 | 10.4 | 23.9 | 6.0 | 0 |
| Anemia | 9.0 | 30.0 | 0 | 0 | 0 |
| Thrombocytopenia | 3.0 | 1.5 | 1.5 | 0 | 0 |
| Febrile
neutropenia | – | – | 1.5 | 1.5 | 0 |
| Fatigue | 32.8 | 9.0 | 4.5 | 1.5 | 0 |
| Anorexia | 19.4 | 3.0 | 0 | 0 | 0 |
| Nausea | 11.9 | 0 | 1.5 | 0 | 0 |
| Constipation | 46.2 | 3.0 | 1.5 | 0 | 0 |
| Diarrhea | 1.5 | 0 | 0 | 0 | 0 |
|
Myalgia/arthralgia | 19.4 | 0 | 0 | 0 | 0 |
| Peripheral sensory
neuropathy | 31.3 | 16.4 | 1.5 | 0 | 0 |
| Dysgeusia | 13.4 | 0 | 0 | 0 | 0 |
| Infection | 3.0 | 3.0 | 1.5 | 4.5 | 0 |
| Interstitial lung
disease | 0 | 0 | 4.5 | 1.5 | 0 |
Discussion
This retrospective clinical study aimed to evaluate
the effect and toxicity of a single-agent nab-PTX in patients with
platinum-resistant NSCLC. The findings revealed that single agent
nab-PTX was associated with an acceptable toxicity and a favorable
response. In this study, 78% of patients were treated after
receiving second-line therapy, as single-agent nab-PTX regimen has
only recently been developed, thus was clinically available as a
second-line therapy only to 22% of the current patient cohort. A
comparison of our data with those of prior studies indicated that
ORR was marginally improved in the present study, although there
were more patients receiving subsequent therapies who were included
in the present study. There was no statistical difference in PFS
between those patients receiving second-line therapy and after a
second-line regimen. History of prior taxane treatment was not
associated with the PFS (data not presented). However, in the
current study cohort, the rate of prior taxane use was 16%, which
was relatively low. Therefore, the actual resistance to taxane
could be less, and the ORR may, therefore, be an improvement on
other previous studies. The PFS and OS in this study were similar
to those recorded in previous studies. According to histological
analysis, the PFS of patients with non-squamous carcinoma was
increased when compared with patients with squamous carcinoma;
although this was not a statistically significant difference, it
was consistent with the results of a previous study (8).
The optimal regimen for single-agent nab-PTX therapy
has not yet been established. A dose-finding study involving
patients with advanced NSCLC revealed that weekly nab-PTX (100
mg/m2) plus carboplatin administered at an area under
the curve (AUC) of 6 every three weeks provided the greatest
clinical benefit-risk ratio among the various weekly and
three-weekly regimens examined (11). Furthermore, a multicenter phase III
study evaluated the safety and efficacy of 100 mg/m2
nab-PTX followed by carboplatin AUC 6 mg/ml/min (3). Therefore, in Kansai Medical University
Hospital, a schedule of single-agent nab-PTX 100 mg/m2
on day 1, 8 and 15 of a 21-day cycle was adopted.
For comparison with previous studies, the incidence
of neutropenia and severe interstitial lung disease (ILD) was
recorded as higher in the present study. A total of 78% of patients
received ≥2 therapeutic regimens; therefore, the recovery of bone
marrow must have been delayed. Thus, the incidence of infection was
also higher than previous studies. Although the safety of nab-PTX
for ILD is not yet clear, it is generally considered that nab-PTX
is as safe for ILD as is paclitaxel (3–4). In the
current study, there were four patients who developed severe ILD,
none of whom had a history of ILD. All patients who developed ILD
were male and a smoker, though these associations were not
statistically analyzed in the current study.
The National Comprehensive Cancer Network guidelines
(https://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf)
authorize the use of certain regimens for subsequent treatments:
Docetaxel (DTX), pemetrexed, erlotinib, gemcitabine, ramucirumab
plus DTX and nivolumab. Nab-PTX has not yet been listed. Among the
recommended treatments, DTX is part of the same taxane class as
nab-PTX, and has been previously used. Although the two agents have
not been directly compared, it appears that the survival rates
conferred by nab-PTX are comparable to those associated with DTX;
however, nab-PTX is less toxic and is associated with fewer AEs. In
the clinical trial of DTX as a monotherapy in patients with
platinum-resistant NSCLC (12),
67–86% of patients were noted to have developed grade 3/4
hematologic toxicities. Furthermore, 22.4% of patients developed
febrile neutropenia (FN). By contrast, in the phase II trial of
nab-PTX as a monotherapy (8), only
4.5–19.5% of patients developed grade 3/4 hematologic toxicities,
none of which were FN. The PR was determined to be 33.7% in the DTX
group and 31.7% in the nab-PTX group, respectively. In the separate
clinical trials of DTX and nab-PTX, the patients' ethnic and
demographical backgrounds were similar. Although each study was
independent and simple comparison is challenging, it is speculated
that nab-PTX may be less toxic. Furthermore, if ILD or edematous
tendencies are present, DTX is problematic to use. Nab-PTX is
considered to be relatively safe to use even in cases with ILD and
renal dysfunction (3,4,13,14). In
the present study, 22% of patients were treated with nab-PTX as a
second-line therapy. It was assumed that, if nab-PTX was selected
as a second-line therapy for those patients it meant those patients
may have experienced complications such as ILD or renal
dysfunction, thus they could not receive the agents that are
recommended for second-line regimens. Therefore, nab-PTX may be an
alternative to DTX in the future. Randomized phase III clinical
trials are required in order to compare the efficacy of nab-PTX and
DTX as a subsequent treatment.
The current study had certain limitations, including
that it was performed retrospectively, had a small sample size and
involved only a single treatment center in Japan.
In conclusion, the results of the present study
indicated a clinically equivalent efficacy and safety for
weekly-administered single-agent nab-PTX 100 mg/m2 on
days 1, 8 and 15 every 21 days in patients with platinum-resistant
NSCLC. However, the safety profile for ILD must be validated. To
assess the toxicity and efficacy of single agent nab-PTX in
advanced NSCLC, the results of an ongoing clinical trial are
expected.
References
|
1
|
Strauss GM, Herndon JE II, Maddaus MA,
Johnstone DW, Johnson EA, Harpole DH, Gillenwater HH, Watson DM,
Sugarbaker DJ, Schilsky RL, et al: Adjuvant paclitaxel plus
carboplatin compared with observation in stage IB non-small-cell
lung cancer: CALGB 9633 with the Cancer and Leukemia Group B,
Radiation Therapy Oncology Group and North Central Cancer Treatment
Group Study Groups. J Clin Oncol. 26:5043–5051. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Gradishar WJ, Tjulandin S, Davidson N,
Shaw H, Desai N, Bhar P, Hawkins M and O'Shaughnessy J: Phase III
trial of nanoparticle albumin-bound paclitaxel compared with
polyethylated castor oil-based paclitaxel in women with breast
cancer. J Clin Oncol. 23:7794–7803. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Socinski MA, Bondarenko I, Karaseva NA,
Makhson AM, Vynnychenko I, Okamoto I, Hon JK, Hirsh V, Bhar P,
Zhang H, et al: Weekly nab-paclitaxel in combination with
carboplatin versus solvent-based paclitaxel plus carboplatin as
first-line therapy in patients with advanced non-small-cell lung
cancer: Final results of a phase III trial. J Clin Oncol.
30:2055–2062. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Socinski MA, Okamoto I, Hon JK, Hirsh V,
Dakhil SR, Page RD, Orsini J, Yamamoto N, Zhang H and Renschler MF:
Safety and efficacy analysis by histology of weekly nab-paclitaxel
in combination with carboplatin as first-line therapy in patients
with advanced non-small-cell lung cancer. Ann Oncol. 24:2390–2396.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Fang Y, Wang L, Xia GH and Shi MQ:
Clinical investigation of efficacy of albumin bound paclitaxel plus
platinum compounds as first-line chemotherapy for stage III/IV
squamous non-small cell lung cancer. Asian Pac J Cancer Prev.
15:7453–7. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Rizvi NA, Riely GJ, Azzoli CG, Miller VA,
Ng KK, Fiore J, Chia G, Brower M, Heelan R, Hawkins MJ and Kris MG:
Phase I/II trial of weekly intravenous 130-nm albumin-bound
paclitaxel as initial chemotherapy in patients with stage IV
non-small-cell lung cancer. J Clin Oncol. 26:639–643. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hu W and Zhang Z: A phase II clinical
study of using nab-paclitaxel as second-line chemotherapy for
Chinese patients with advanced non-small cell lung cancer. Med
Oncol. 32:4982015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Sakata S, Saeki S, Okamoto I, Otsubo K,
Komiya K, Morinaga R, Yoneshima Y, Koga Y, Enokizu A, Kishi H, et
al: Phase II trial of weekly nab-paclitaxel for previously treated
advanced non-small cell lung cancer: Kumamoto thoracic oncology
study group (KTOSG) trial 1301. Lung Cancer. 99:41–45. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
American Joint Committee on Cancer: Lung
cancer staging (7th). https://cancerstaging.org/references-tools/quickreferences/Documents/LungMedium.pdf#search=%27TNM+classification+7th+lung+canacer+AJCC%27Accessed.
August 19–2017.
|
|
10
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumors:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Socinski MA, Manikhas GM, Stroyakovsky DL,
Makhson AN, Cheporov SV, Orlov SV, Yablonsky PK, Bhar P and
Iglesias J: A dose finding study of weekly and every-3-week
nab-Paclitaxel followed by carboplatin as first-line therapy in
patients with advanced non-small cell lung cancer. J Thorac Oncol.
5:852–861. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Shepherd FA, Dancey J, Ramlau R, Mattson
K, Gralla R, O'Rourke M, Levitan N, Gressot L, Vincent M, Burkes R,
et al: Prospective randomized trial of docetaxel versus best
supportive care in patients with non-small-cell lung cancer
previously treated with platinum-based chemotherapy. J Clin Oncol.
18:2095–2103. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Yasuda K, Igishi T, Kawasaki Y, Yamamoto
M, Kato K, Matsumoto S, Kotani M, Sako T, Shigeoka Y, Sugitani A,
et al: Phase II trial of weekly paclitaxel in previously untreated
advanced non-small-cell lung cancer. Oncology. 65:224–228. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Khan A, McNally D, Tutschka PJ and
Bilgrami S: Paclitaxel-induced acute bilateral pneumonitis. Ann
Pharmacother. 31:1471–1474. 1997. View Article : Google Scholar : PubMed/NCBI
|