Introduction
Aging societies are becoming a major global problem
(1). The most important change in
the body with age is the loss of skeletal muscle. Rosenberg found
that the degree of sarcopenia, which represents a loss of skeletal
muscle, is correlated with aging. However, there is still no
explicit consensus regarding the cut-off point of skeletal muscle
loss in patients with sarcopenia (2). The detailed determination and
classification of sarcopenia was suggested by the European Working
Group on Sarcopenia in Older People (EWGSOP) (1). Regarding the narrow definition of
sarcopenia, skeletal muscle loss is the most important factor to
consider when determining sarcopenia (2).
We examined the usefulness of skeletal muscle loss
as a predictive factor for the length of admission among patients
who underwent radical nephro-ureterectomy.
Patients and methods
Patients
A total of 60 patients (male, n=44; female, n=16)
underwent nephro-ureterectomy for upper urothelial carcinoma in
Yokohama City University Medical Center (Table I). The institutional review board of
Yokohama City University Medical Center (Yokohama, Japan) approved
this study, and written consent was obtained from the patients. The
patients were followed up every three months for two years and
every six months thereafter with cystectomy and computed tomography
(CT). The psoas muscle volume was calculated using axial CT images
at the level of the umbilicus obtained prior to
nephro-ureterectomy. The psoas muscle index (PMI) was calculated by
the following formula: (right side psoas muscle area at the level
of the umbilicus mm2)/(body height m)2.
 | Table I.Baseline patient characteristics. |
Table I.
Baseline patient characteristics.
| Variables | Number (%) or (mean,
median) |
|---|
| Number of
patients | 44 (100.0) |
| Age (mean,
median) | 68.0, 71 |
| Side |
|
| Left | 33 (75) |
|
Right | 11 (25) |
| T stage |
|
| is | 3 (6.8) |
| a | 6 (13.6) |
| 1 | 14 (31.8) |
| 2 | 5 (11.4) |
| 3 | 16 (36.4) |
|
Unknown | 0 |
| Pathological grade
(low vs. high) |
|
| Low | 13 (29.5) |
| High | 22 (50) |
|
Unknown | 9(20.5) |
| Pathological grade
(G1, G2, G3) |
|
|
Grade1 | 8 (18.2) |
|
Grade2 | 20 (45.5) |
|
Grade3 | 15 (34.1) |
|
Unknown | 1 (2.3) |
| Recurrence | 24 (54.5) |
Statistical analyses
The patients' characteristics and preoperative
factors were analyzed by the Mann-Whitney U test and the
chi-squared test. The Kaplan-Meier product limit estimator was used
to estimate the progression-free survival (PFS) and overall
survival (OS). The duration of the survival was defined as the time
between radical cystectomy and tumor progression or death. The
log-rank test was performed for the statistical comparisons.
P-values of <0.05 were considered to indicate statistical
significance.
Results
The median and mean [± standard deviation (SD)] ages
of the 44 patients were 71 and 68.0 years (± 12.2 years),
respectively. The median and mean (± SD) post-operative
hospitalization periods were 12 and 14.5 days (± 6.5 days),
respectively. The median and mean (± SD) follow-up periods were
1,086 and 1,121.0 days (± 768.6 days), respectively. The
clinicopathological data are summarized in Table I. The survival duration was defined
as the time between nephro-ureterectomy and tumor recurrence or
death. The median and mean (± SD) areas of the psoas at the level
of the umbilicus were 1,022.5 and 1,010.1 mm2 (± 302.9).
The median and mean PMI were 397.1 and 411.6 (± 98.4),
respectively.
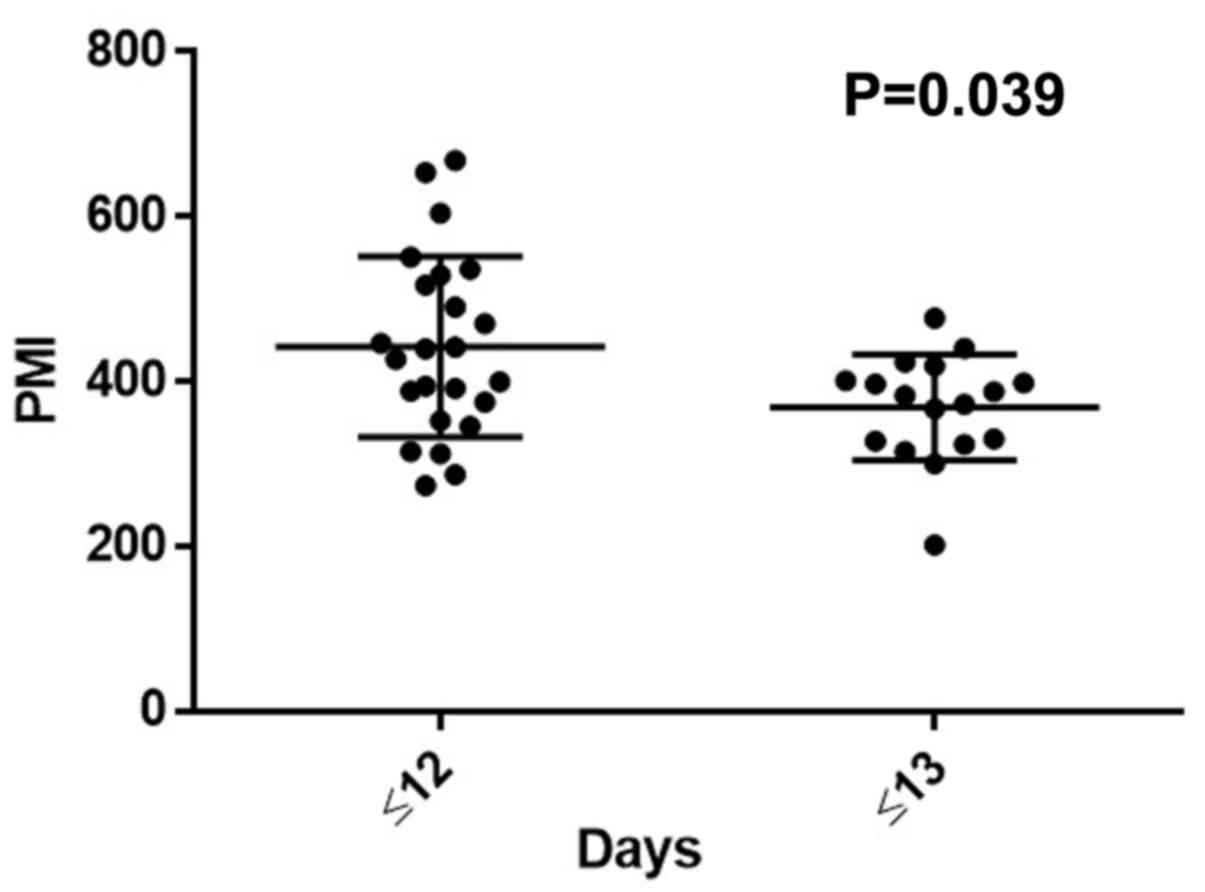
We divided the patients into two groups based on
their PMI (with even numbers of patients). In terms of the duration
of postoperative admission, the long-admission group (≥13 days)
showed significantly lower PMI than the short-admission group (≤12
days) (383.0 vs. 433.1, P=0.039) (Fig.
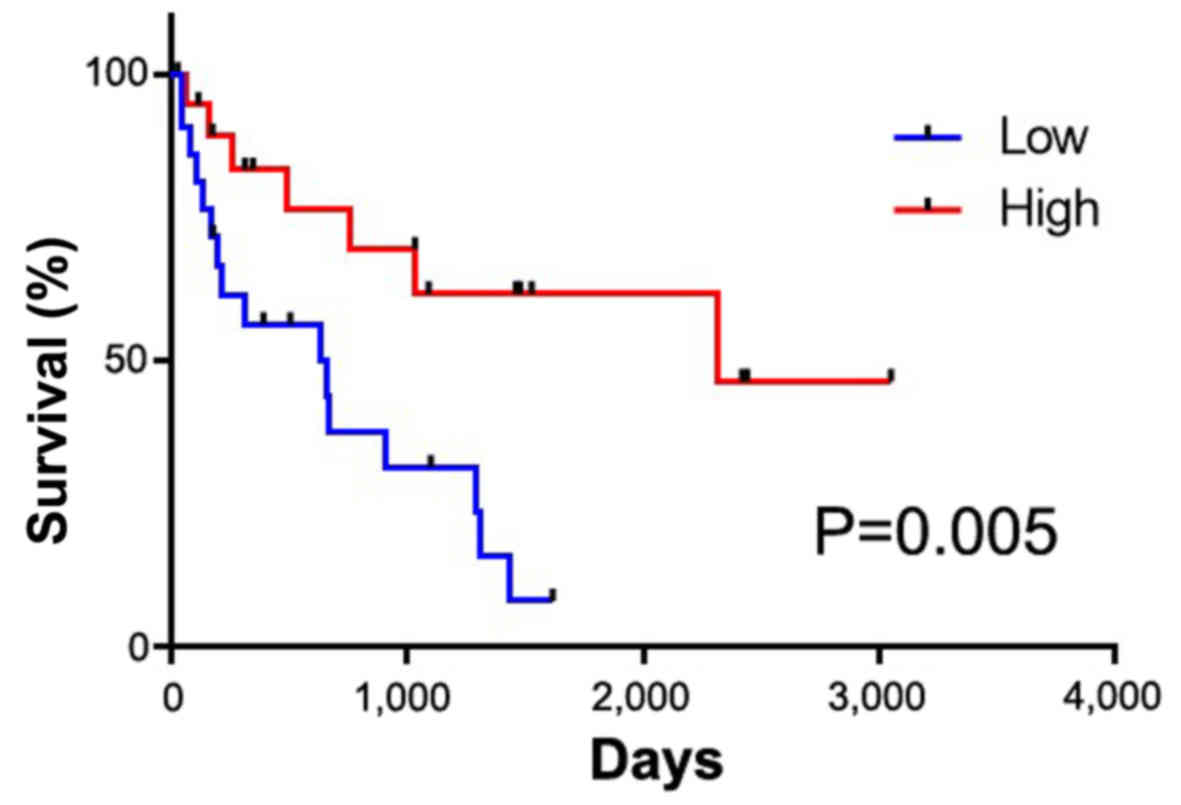
1). The lower PMI group showed a significantly poorer
recurrence-free survival than the higher PMI group (634 vs. 2,317
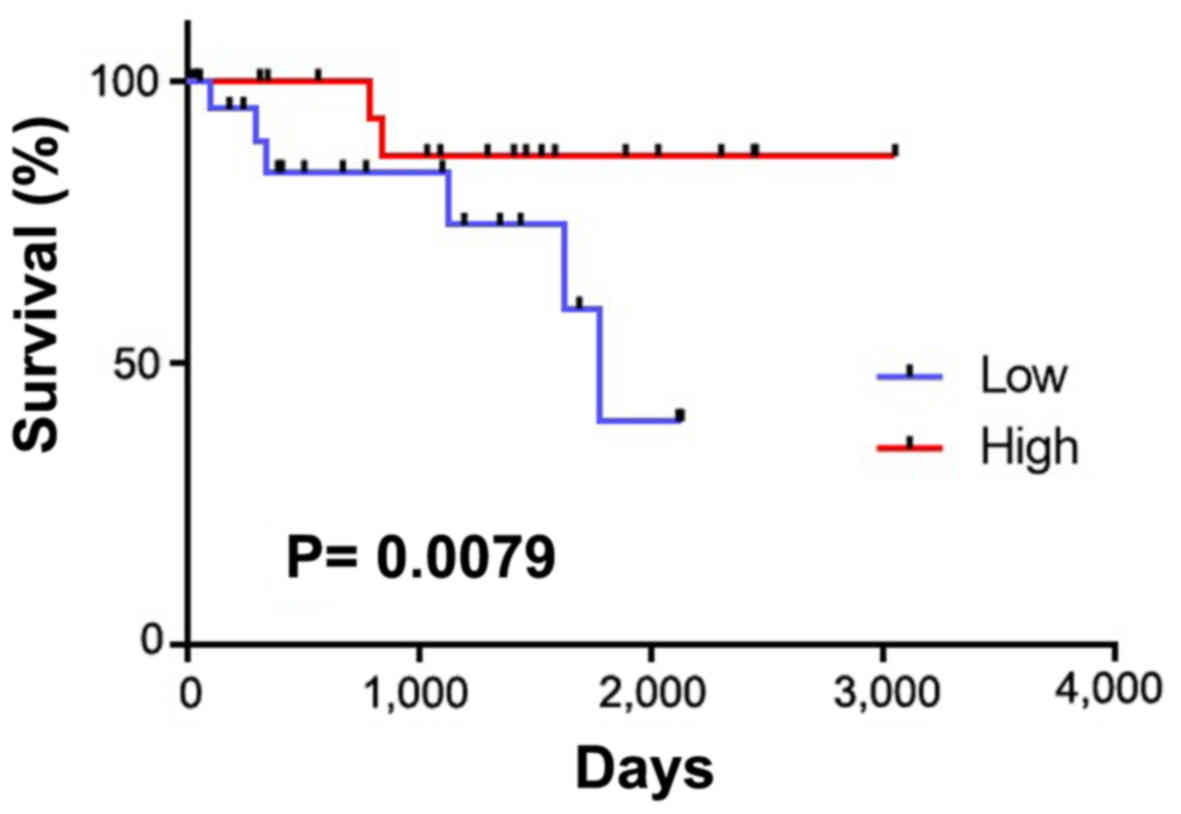
days, P=0.005) (Fig. 2). There were
no significant differences in the overall survival between the two
groups; however, the lower PMI group tended to have a shorter
survival than the higher PMI group (P=0.080) (Fig. 3).
Discussion
Upper urothelial carcinoma accounts for ~5% of all
cases of urothelial carcinoma (3).
The likely incidence is higher among patients who are 70–80 years
of age; 60% of patients have invasion at the time of the diagnosis.
The bladder is the most common site of recurrence, with a
recurrence rate of 30–50% (4–6).
Recently, sarcopenia, which refers to the loss of
skeletal mass that occurs with aging, was found to be a prognostic
risk factor for the survival or postoperative complications.
Patients with sarcopenia show a worse swallowing ability and a
lower nutritional status than those without it. Furthermore, older
men (>65 years of age) with sarcopenia showed lower ADL values
than patients without sarcopenia (7,8).
We previously reported on the impact of sarcopenia
using PMI in bladder cancer patients who received systemic
chemotherapy and total cystectomy. There as well, a low PMI was
associated with a poorer oncological outcome than a high PMI
(9,10). Other recent studies have revealed
that sarcopenia is a risk factor for postoperative complications or
a poor survival in some solid cancers. For stage 2–3 gastric
cancer, patients with sarcopenia showed a higher rate of
postoperative complications and a poorer overall and
recurrence-free survival than those without sarcopenia (8,11).
Pancreatic cancer patients with sarcopenia who underwent
pancreatectomy also showed a poorer overall survival than the
patients without sarcopenia (12).
Although the detailed mechanisms underlying the
association between sarcopenia and postoperative complications are
still not fully understood, physical weakness reduces the
persistence of long admissions of due to the adverse health effects
of invasive surgery (10,13). Furthermore, sarcopenia is believed to
develop due to aging or malignancy.
In the present study, upper urothelial carcinoma
patients with longer admission durations showed lower PMI values
than those with shorter admission durations. Previous studies
reported a postoperative complication rate of 20.8% and a
postoperative mortality rate at 90 days after surgery of 4.4% in
similar populations (14,15).
Although several treatment options are available for
upper urothelial cancer, including nephron-ureterectomy,
conservative surgery, ureteroscopy, segmental resection,
percutaneous access, and the use of adjuvant topical agents, an
increased incidence of advanced-stage cases means that most
patients will require nephro-ureterectomy (4). Given that patients with upper
urothelial carcinoma tend to be older, surgeons should carefully
evaluate the risk of surgery. Due to the small number of patients
in the present study, further investigations will be needed to
confirm these findings.
In the present study, we showed that sarcopenia
predicts a longer hospitalization period and that sarcopenic
patients have a significantly worse prognosis than patients without
sarcopenia. The present findings suggest that sarcopenia is a
meaningful factor that should be considered when choosing therapy
for upper urothelial carcinoma.
Acknowledgements
We would like to thank Dr R. Shimizu, Dr Y.
Nakamkura and Dr T. Yamaki for their technical assistance. The
present study was supported by grants from KAKENHI grants
(16K20152) and from the Ministry of Education, Culture, Sports,
Science and Technology of Japan.
References
|
1
|
Cruz-Jentoft AJ, Baeyens JP, Bauer JM,
Boirie Y, Cederholm T, Landi F, Martin FC, Michel JP, Rolland Y,
Schneider SM, et al: European Working Group on Sarcopenia in Older
People: Sarcopenia: European consensus on definition and diagnosis:
Report of the European Working Group on Sarcopenia in older people.
Age Ageing. 39:412–423. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Rosenberg IH: Sarcopenia: Origins and
clinical relevance. J Nutr. 127 Suppl 5:990S–991S. 1997.PubMed/NCBI
|
|
3
|
Raman JD, Messer J, Sielatycki JA and
Hollenbeak CS: Incidence and survival of patients with carcinoma of
the ureter and renal pelvis in the USA, 1973–2005. BJU Int.
107:1059–1064. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Rouprêt M, Zigeuner R, Palou J, Boehle A,
Kaasinen E, Sylvester R, Babjuk M and Oosterlinck W: European
Association of Urology Guideline Group for urothelial cell
carcinoma of the upper urinary tract: European guidelines for the
diagnosis and management of upper urinary tract urothelial cell
carcinomas: 2011 update. European Association of Urology Guideline
Group for urothelial cell carcinoma of the upper urinary tract.
Actas Urol Esp. 36:2–14. 2012.(In Spanish). View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Oya M and Kikuchi E: Committee for
establishment of clinical practice guideline for management of
upper tract urothelial carcinoma; japanese urological association:
Evidenced-based clinical practice guideline for upper tract
urothelial carcinoma (summary-Japanese Urological Association, 2014
edition). Int J Urol. 22:3–13. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Hara T, Fujimoto H, Sakura M, Inokuchi J,
Nishiyama H, Miyazaki J, Ohyama C, Koie T, Kikuchi E and Hinotsu S;
Cancer Registration Committee of the Japanese Urological
Association, : Prognostic factors of recurrent disease in upper
urinary tract urothelial cancer after radical nephroureterectomy:
Subanalysis of the multi-institutional national database of the
Japanese Urological Association. Int J Urol. 22:1013–1020. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Shiozu H, Higashijima M and Koga T:
Association of sarcopenia with swallowing problems, related to
nutrition and activities of daily living of elderly individuals. J
Phys Ther Sci. 27:393–396. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Tanimoto Y, Watanabe M, Sun W, Tanimoto K,
Shishikura K, Sugiura Y, Kusabiraki T and Kono K: Association of
sarcopenia with functional decline in community-dwelling elderly
subjects in Japan. Geriatr Gerontol Int. 13:958–963. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kasahara R, Kawahara T, Ohtake S, Saitoh
Y, Tsutsumi S, Teranishi JI, Miyoshi Y, Nakaigawa N, Yao M,
Kobayashi K and Uemura H: A Low psoas muscle index before treatment
can predict a poorer prognosis in advanced bladder cancer patients
who receive gemcitabine and nedaplatin therapy. Biomed Res Int.
2017:79815492017. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Saitoh-Maeda Y, Kawahara T, Miyoshi Y,
Tsutsumi S, Takamoto D, Shimokihara K, Hayashi Y, Mochizuki T,
Ohtaka M, Nakamura M, et al: A low psoas muscle volume correlates
with a longer hospitalization after radical cystectomy. BMC Urol.
17:872017. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Zhuang CL, Huang DD, Pang WY, Zhou CJ,
Wang SL, Lou N, Ma LL, Yu Z and Shen X: Sarcopenia is an
independent predictor of severe postoperative complications and
long-term survival after radical gastrectomy for gastric cancer:
Analysis from a large-scale cohort. Medicine (Baltimore).
95:e31642016. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Onesti JK, Wright GP, Kenning SE, Tierney
MT, Davis AT, Doherty MG and Chung MH: Sarcopenia and survival in
patients undergoing pancreatic resection. Pancreatology.
16:284–289. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Makary MA, Segev DL, Pronovost PJ, Syin D,
Bandeen-Roche K, Patel P, Takenaga R, Devgan L, Holzmueller CG,
Tian J and Fried LP: Frailty as a predictor of surgical outcomes in
older patients. J Am Coll Surg. 210:901–908. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Bastiampillai R, Lavallée LT, Cnossen S,
Witiuk K, Mallick R, Fergusson D, Schramm D, Morash C, Cagiannos I
and Breau RH: Laparoscopic nephroureterectomy is associated with
higher risk of adverse events compared to laparoscopic radical
nephrectomy. Can Urol Assoc J. 10:126–131. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Jeldres C, Sun M, Isbarn H, Lughezzani G,
Budäus L, Alasker A, Shariat SF, Lattouf JB, Widmer H, Pharand D,
et al: A population-based assessment of perioperative mortality
after nephroureterectomy for upper-tract urothelial carcinoma.
Urology. 75:315–320. 2010. View Article : Google Scholar : PubMed/NCBI
|