Introduction
Nasopharyngeal carcinoma (NPC) is a malignant tumor
type that arises from the epithelial surface of the nasopharynx,
and has the highest incidence of all types of head and neck cancer
in China. Men are most frequently affected by NPC, typically at an
age of 40–50 years. Causative factors for NPC include heredity,
Epstein-Barr virus (EBV) and environmental factors (1). Primary NPC lesions are differentiated
or undifferentiated non-keratinizing carcinomas, which are
sensitive to radiotherapy. As the radiotherapy response rate is
85%, it is the preferred treatment for NPC (2). However, due to the variable clinical
manifestations of NPC, misdiagnosis and missed diagnosis occur
frequently. The majority of patients are diagnosed in the late
stages of the disease, when the tumor has invaded the surrounding
tissues; the higher local recurrence rates and distant metastasis
rates associated with late-stage NPC lead to decreased overall
survival (3). Therefore, a novel and
effective method for the clinical diagnosis of NPC is urgently
required.
The occurrence of NPC is associated with EBV
infection, and immune function serves an important role in the
development of NPC. The expression of programmed death ligand 1
(PD-L1) has been reported as a reliable prognostic factor for
various types of malignancy. However, the association between the
expression of PD-L1 and the clinicopathological factors and
prognosis of NPC patients remain to be fully elucidated.
PD-L1 is a member of the B7 family and the protein
consists of 290 amino acids (4). The
extracellular domain of PD-L1 binds to programmed cell death
protein 1 (PD-1), which is expressed on the surface of activated T
lymphocytes. The PD-1/PD-L1 pathway mediates negative
co-stimulatory signals to effectively inhibit T-cell function and
proliferation, and decrease the secretion of cytokines, including
interleukin (IL)-2, IL-10 and interferon (IFN)-γ. The pathway
serves an important role in the immunomodulation of various
diseases and pathological processes, including tumor immunity,
transplantation immunity, viral infection and autoimmunity
(5,6). The abnormal expression of PD-L1 in
numerous types of malignant tumor, including melanoma, lung cancer,
esophageal cancer, colorectal cancer, breast cancer and glioma, is
associated with tumor invasion and metastasis, decreased tumor
infiltration by T lymphocytes, poor prognosis and reduced survival
time (7).
NPC is characterized by prevailing EBV infection and
the presence of immune cell infiltration around the cancer lesions
(8). EBV-DNA exists as cell-free
fragments in the serum of infected patients. Lo et al
(9) identified that EBV-DNA was
detectable in the plasma of 96% of the NPC patients assessed, and
observed that serum EBV-DNA levels in patients with advanced-stage
disease were significantly higher than that in patients with
early-stage disease, suggesting that serum EBV-DNA levels may be
positively correlated with the tumor burden. EBV early antigen
(EA)-immunoglobulin (Ig)A and EBV viral capsid antigen (VCA)-IgA
are markers of viral infection that are commonly used in the
clinical screening and auxiliary diagnosis of NPC, and indicate the
risk of NPC development. It has been identified that NPC patients
display aberrations in peripheral blood lymphocyte subsets
(10); this abnormal immune status
may be due to the abnormal cellular immune response in NPC and may
be associated with the immune response to EBV infection. However,
the possible underlying association between PD-L1 and alterations
in the immune components in the peripheral blood of NPC patients
has remained to be determined.
In the present study, the expression of PD-L1 was
examined in NPC tissues of patients from northern China, and the
association between PD-L1 expression levels and the
clinicopathological parameters was assessed. In addition, the
lymphocyte subsets, EBV-DNA and EBV antibodies in peripheral blood
were assessed in order to provide potential markers for the
diagnosis and treatment of NPC.
Materials and methods
Patients and clinical data
Tissue specimens and peripheral blood were collected
from 96 NPC patients, including 72 males (median age, 48 years;
range, 13–82 years) and 24 females (median age, 41.5 years; range,
11–67 years). Patients were recruited at the National Cancer
Center/Cancer Hospital, Chinese Academy of Medical Sciences
(Beijing, China). The patients were enrolled according to the
following criteria: i) Radiotherapy was received; ii) complete
clinical data were available; and iii) no other malignant diseases,
active hepatitis or diabetes were diagnosed. The retrospective
study was approved by the Institutional Review Board of the Cancer
Hospital, Chinese Academy of Medical Sciences (Beijing, China. The
trial registration number was NCC2016YJC-10). Written, informed
consent was provided by all patients prior to enrollment in the
study.
Immunohistochemical analysis
The paraffin-embedded tissues were cut into 4-µm
sections, dewaxed and then rehydrated with a graded ethanol series.
To quench endogenous peroxidase activity, the sections were
incubated with 3% H2O2 at room temperature
for 20 min. For antigen retrieval, the sections were heated in
ethylene diamine tetraacetic acid buffer (pH, 8.0) for 2 min using
a pressure cooker. The slides were blocked with normal goat serum
(Ready-to-use; cat. no. ZLI-9022; OriGene Technologies, Beijing,
China) at 37°C for 20 min. Samples were incubated with
rabbit-monoclonal anti-PD-L1 antibody (dilution, 1:200; cat. no.
ab205921; Abcam, Cambridge, UK) and mouse monoclonal anti-P16
antibody (Ready-to-use; cat. no. 705-4713; Ventana Medical Systems,
Inc., Tucson, AZ, USA) overnight at 4°C. Incubation with secondary
antibody and staining was performed using an immunohistochemical
staining kit (cat. no. PV-9000; OriGene Technologies) according to
the manufacturer's protocol. The immunoreaction was visualized with
diaminobenzidine staining, followed by counterstaining with
hematoxylin. The primary antibody was replaced with PBS to prepare
the negative control sample, and PD-L1-positive slides incubated
with the antibodies were used as a positive control.
Percentages of PD-L1-positive tumor cells and
staining intensity were independently evaluated by two experienced
pathologists who were blinded to the clinical information. They
assessed 20 sequential high-power fields (0.54 mm diameter per
field) using Aperio ImageScope software version 12.3.0 (Leica
Biosystems, Wetzlar, Germany) to quantify the staining in the
images captured. A proportion of stained cells of >10% was
considered to indicate a positive expression status, with >25%
considered as high expression and 10–25% as low expression.
Lymphocyte subset detection
Venous blood samples were collected from patients
prior to radiotherapy and stored with K3EDTA anti-coagulant. The
samples were analyzed by flow cytometry using the BD Multitest™ IMK
kit (cat. no. 340503; BD Biosciences, Franklin Lakes, NJ, USA). The
CD4/CD8/CD3/CD45 trichromatic fluorescent monoclonal antibodies in
the kit were diluted 1:10 and incubated with the samples for 15 min
at room temperature. FACSCanto version 6.1.3 (BD Biosciences) was
used to analyze T-lymphocyte subsets, including total T lymphocytes
(CD3+T), the T auxiliary/induced cell subset
(CD3+CD4+T), the T suppressor/cytotoxic cell
subset (CD3+CD8+T), the ratio of T auxiliary
to suppressor cells
(CD3+CD4+/CD3+CD8+),
natural killer (NK) cells (CD3−CD56+) and B
lymphocytes (CD3−CD19+).
Detection of EBV infection
ELISA diagnostic kits (Euroimmun, Lübeck, Germany)
were applied to detect serum EBV EA-IgA (cat. no. EI 2795-9601 A)
and VCA-IgA (cat. no. EI 2791-9601 A) antibodies. The kits were
used according to the manufacturer's protocol, and the antibody
concentrations were determined with a standard curve. EBV-DNA was
detected using the Epstein-Barr Virus (EBV) Polymerase Chain
Reaction (PCR) Fluorescence Detection kit (cat. no. DA-D065; DaAn
Gene Co., Ltd., Guangzhou, China) according to the manufacturer's
protocol, with a Roche LightCycler® 480II (Roche
Diagnostics, Basel, Switzerland).
Follow-up
Following the completion of radiotherapy and
chemotherapy, the NPC patients were followed up every 3 months,
which included thoracic and abdominal computed tomography scans,
and nasopharyngeal and cervical magnetic resonance imaging (MRI).
When a nasopharyngeal mass was identified on MRI,
electro-epipharyngoscopy and biopsy were performed. Fine-needle
aspiration cytology was applied when cervical lymph node
enlargement was identified. Follow-up continued until June 1, 2017;
the last time-point for the patient with the latest enrolment.
Distant metastasis-free survival (DMFS) was defined as the time
from the beginning of radiotherapy to the identification of
metastasis, or until the last follow-up. The distant metastases
were all detected after 1 year's follow-up.
Statistical analysis
SPSS version 22.0 software (IBM Corp., Armonk, NY,
USA) was used for statistical analysis. Discrete variables were
compared using Fisher's exact test, χ2 test and Wilcoxon
W test, continuous variables were compared using Student's t-test,
Mann-Whitney U and Kruskal-Wallis H test. Survival data were
analyzed using the Log-rank test. P<0.05 was considered to
indicate a statistically significant difference.
Results
Expression of PD-L1 protein in NPC
patients
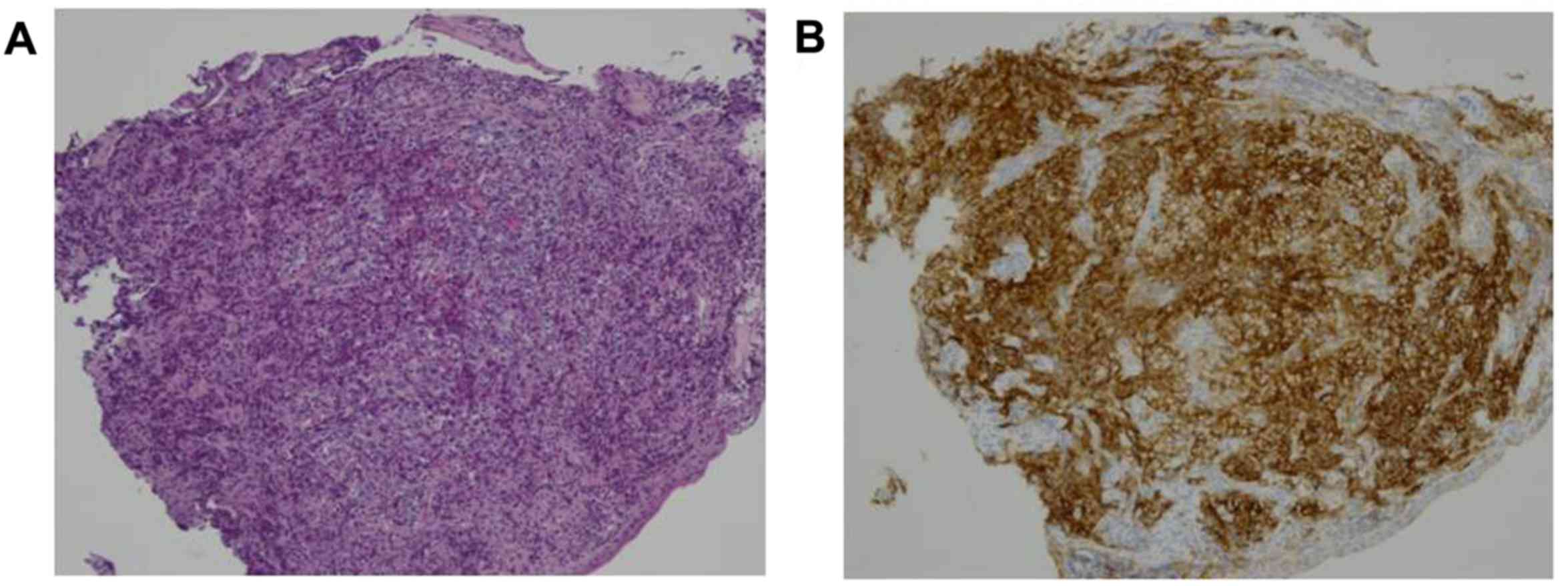
The expression of PD-L1 was analyzed in 96 NPC
specimens by immunohistochemical staining. The protein was
predominantly expressed on the cell membrane (Fig. 1). Immunohistochemical analysis
revealed that 28/96 NPC samples (29.2%) were positive for PD-L1
expression and 68 cases (70.8%) were negative.
PD-L1 expression and the
clinicopathological features of NPC patients
The association of PD-L1 expression with
clinicopathological parameters was assessed to clarify the function
of PD-L1 in NPC. No significant associations between PD-L1
expression status and sex, age or histotype classification were
identified. However, PD-L1 expression was significantly associated
with NPC 1-year distant metastasis (P=0.010) and the tumor
(T)-stage of the primary tumor (P=0.032). No significant
association between PD-L1 expression and the AJCC stage (2010) or
treatment modality (with or without chemotherapy or before or after
radiotherapy) was identified (Table
I).
 | Table I.Association between PD-L1 expression
and the clinicopathological features of nasopharyngeal carcinoma
patients. |
Table I.
Association between PD-L1 expression
and the clinicopathological features of nasopharyngeal carcinoma
patients.
| Characteristic | Cases (n) | PD-L1-negative
(%) | PD-L1-positive
(%) | χ2 | P-value |
|---|
| Sex |
|
|
| 0.269 | 0.604 |
| Male | 72 | 52 (72.2) | 20 (27.8) |
|
|
|
Female | 24 | 16 (66.7) | 8 (33.3) |
|
|
| Age (years) |
|
|
| 1.18 | 0.277 |
|
>46 | 46 | 35 (76.1) | 11 (23.9) |
|
|
| ≤46 | 50 | 33 (66.0) | 17 (34.0) |
|
|
| Histotype |
|
|
| 1.803 | 0.179 |
|
Undifferentiated
non-keratinizing carcinoma | 64 | 42 (65.6) | 22 (34.4) |
|
|
|
Differentiated
non-keratinizing carcinoma | 27 | 22 (81.5) | 5 (18.5) |
|
|
| Poorly
differentiated non-keratinizing carcinoma | 5 | 4 (80) | 1 (20) |
|
|
| 1-year distant
metastasis |
|
|
| 6.619 | 0.010 |
| No | 88 | 66 (75) | 22 (25) |
|
|
| Yes | 8 | 2 (25) | 6 (75) |
|
|
| Locoregional
recurrence |
|
|
|
| 0.203 |
| No | 93 | 67 (72.0) | 26 (28.0) |
|
|
|
Yes | 3 | 1 (33.3) | 2 (66.7) |
|
|
| AJCC stage
(2010) |
|
|
|
3,079.5a | 0.051 |
| I | 4 | 4 (100.0) | 0 (0.0) |
|
|
| II | 7 | 5 (71.4) | 2 (28.6) |
|
|
|
III | 48 | 37 (77.1) | 11 (22.9) |
|
|
| IV | 37 | 22 (59.5) | 15 (40.5) |
|
|
| T-stage |
|
|
|
3,054.0a | 0.032 |
| 1 | 13 | 12 (92.3) | 1 (7.7) |
|
|
| 2 | 6 | 4 (66.7) | 2 (33.3) |
|
|
| 3 | 49 | 36 (73.5) | 13 (26.5) |
|
|
| 4 | 28 | 16 (57.1) | 12 (42.9) |
|
|
| N-stage |
|
|
|
3,295.5a | 0.983 |
| 0 | 7 | 5 (71.4) | 2 (28.6) |
|
|
| 1 | 27 | 18 (66.7) | 9 (33.3) |
|
|
| 2 | 46 | 35 (76.1) | 11 (23.9) |
|
|
| 3 | 16 | 10 (62.5) | 6 (37.5) |
|
|
| M-stage |
|
|
| 0.000 | 1.000 |
| 0 | 96 | 68 (70.8) | 28 (29.2) |
|
|
| 1 | 0 | 0 (0.0) | 0 (0.0) |
|
|
|
Chemotherapyb |
|
|
| 0.024 | 0.878 |
| No | 23 | 16 (69.6) | 7 (30.4) |
|
|
|
Yes | 73 | 52 (71.2) | 21 (28.8) |
|
|
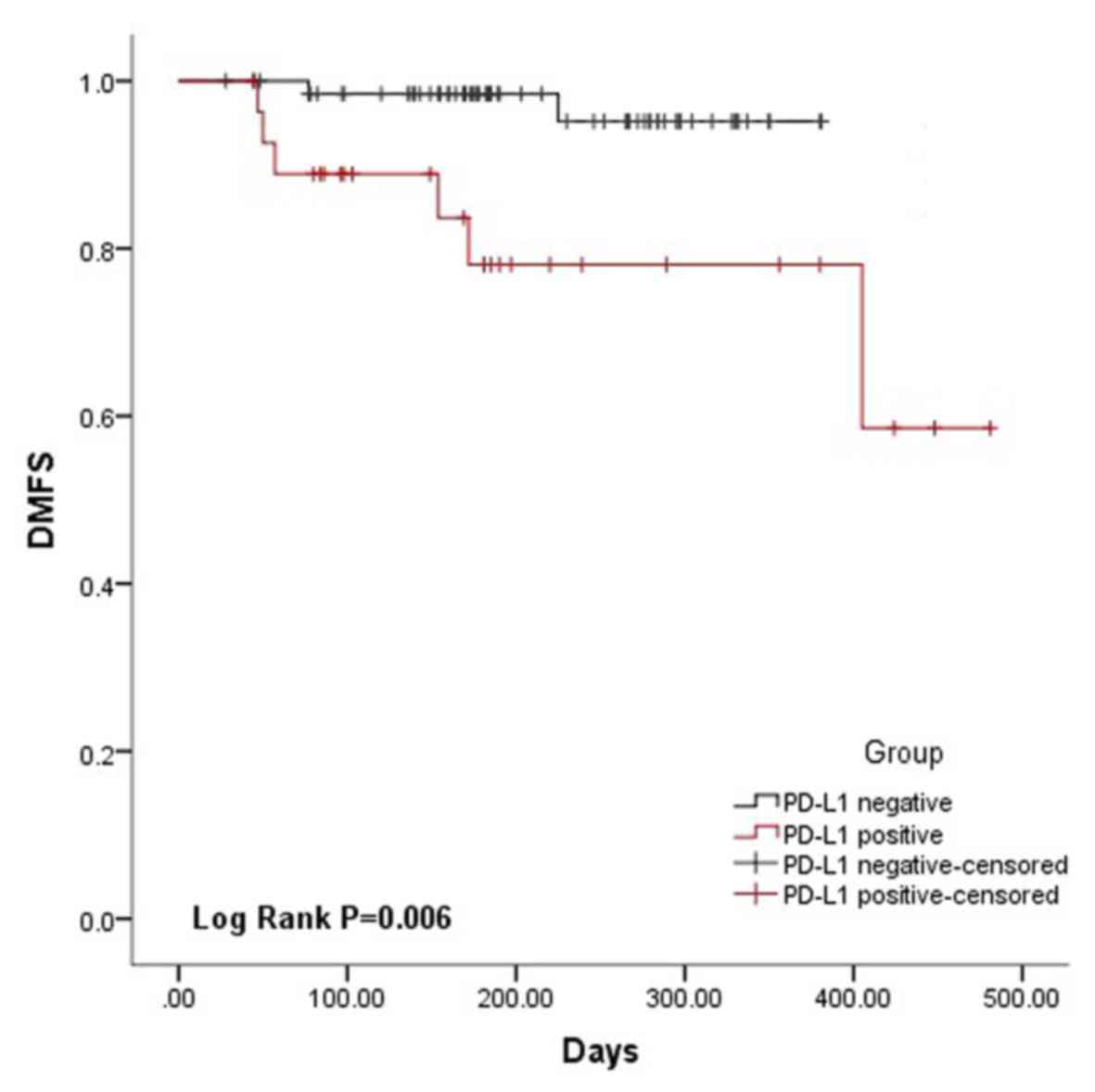
Expression of PD-L1 is associated with
the DMFS of NPC patients
The DMFS for the PD-L1-positive and -negative groups
is presented in Fig. 2. Patients
with a PD-L1-positive status had significantly poorer DMFS
(P=0.007) compared with that of patients with a PD-L1-negative
status. The 1-year distant metastasis rate was 2.9% for
PD-L1-negative patients and 21.4% for PD-L1-positive patients
(Table I). Thus, the patients with a
PD-L1-positive status were at a significantly higher risk of
developing metastasis.
Association of PD-L1 expression status
in NPC tissues with EBV-DNA and lymphocyte subsets in the
peripheral blood
PD-L1 is an immunosuppressive molecule associated
with an abnormal immune status in the body. ELISA and qPCR were
used to detect the levels of EBV antibodies and EBV-DNA, while
lymphocyte subsets were detected using flow cytometric analysis of
the peripheral blood of NPC patients. A statistically significant
association of PD-L1 expression with EBV VCA-IgA antibodies
(P=0.046) and with CD3−CD19+ cells was
identified (P=0.014; Table II).
| Table II.Correlation of various markers in the
serum with PD-L1 expression in tumor tissues. |
Table II.
Correlation of various markers in the
serum with PD-L1 expression in tumor tissues.
| A, EBV DNA levels
in plasma vs. PD-L1 expression |
|---|
|
|---|
| Group | PD-L1 negative | PD-L1 positive | χ2 | P-value |
|---|
| EBV
DNA− | 41 | 16 | 0.082 | 0.775 |
| EBV
DNA+ | 27 | 12 |
|
|
|
| B, EBV antibody
levels in serum vs. PD-L1 expression |
|
| Group | Cases
(n) | Median | Mann-whitney
U | P-value |
|
| EBV EA-IgA |
|
| 762.5 | 0.152 |
| PD-L1
negative | 67 | 1.019 |
|
|
| PD-L1
positive | 28 | 0.3405 |
|
|
| EBV VCA-IgA |
|
| 694.0 | 0.046 |
| PD-L1
negative | 67 | 2.067 |
|
|
| PD-L1
positive | 28 | 1.0155 |
|
|
|
| C, Lymphocyte
subset levels in plasma vs. PD-L1 expression |
|
| Cell
type | Cases
(n) | Value
(%) | t | P-value |
|
| CD3+ T
cells |
|
| 0.38 | 0.705 |
| PD-L1
negative | 65 | 67.4754±9.608 |
|
|
| PD-L1
positive | 26 | 66.6269±9.664 |
|
|
| CD3+
CD4+ T cells |
|
| 0.39 | 0.697 |
| PD-L1
negative | 65 | 31.0446±7.672 |
|
|
| PD-L1
positive | 26 | 30.3192±8.814 |
|
|
| CD3+
CD8+ T cells |
|
| 0.09 | 0.929 |
| PD-L1
negative | 65 | 31.8554±9.731 |
|
|
| PD-L1
positive | 26 | 31.6654±7.286 |
|
|
|
CD4+/CD8+ |
|
| 768.0a | 0.569 |
| PD-L1
negative | 64 | 0.965 (0.7575) |
|
|
| PD-L1
positive | 26 | 0.975 (0.52) |
|
|
| NK cells |
|
| −0.741 | 0.460 |
| PD-L1
negative | 64 |
23.5734±10.0917 |
|
|
| PD-L1
positive | 26 |
25.3731±11.2599 |
|
|
| CD3−
CD19+ cells |
|
| 8.532b | 0.014 |
| PD-L1
negative | 64 | 7.25 (5.95) |
|
|
| PD-L1
low expression | 19 | 8.1 (6.1) |
|
|
| PD-L1
high expression | 7 | 4.0 (2.9) |
|
|
Discussion
NPC is associated with EBV infection, poor tumor
cell differentiation and sensitivity to chemotherapy. In addition,
compared with other types of head and neck squamous cell carcinoma,
NPC has a unique geographical distribution, with a particularly
high incidence in southern China and Southeast Asia (11). After conventional treatment with
chemoradiotherapy, the majority of NPC tumor cells are eliminated.
The activation of immune cells, including tumor-infiltrating
lymphocytes (TILs), is important for the elimination of residual
tumor cells. However, a variety of immunosuppressive mechanisms act
to reduce the activity of TILs in the tumor microenvironment,
resulting in local recurrence and distant metastasis in a number of
patients after radiotherapy and chemotherapy (12,13).
Once this has occurred, effective treatment options are limited;
the majority of patients in this situation choose palliative
chemotherapy to prolong their survival period, but the effect is
limited. Therefore, identifying how the immune suppression index is
associated with the recurrence and metastasis of NPC may assist in
improving the prognosis of patients.
PD-L1 is a member of the Ig superfamily with the
chromosomal location of 9p24.2, which encodes a 290-amino acid type
I transmembrane protein, including an extracellular portion with
IgV and IgC-like domains. Its IgV-like domain interacts with the
extracellular IgV domain of PD-1, and the immune tyrosine motif
region of the cytoplasmic tail of the PD-1 molecule serves an
important role in the negative regulation of the immune response
(14). Under normal physiological
conditions, PD-1 maintains the body's immune tolerance as a
negative regulator of T-cell proliferation; however, in tumors and
viral infection, the overexpressed PD-L1 and PD-L2 on the cell
surface interacts with PD-1 on the surface of T cells to inhibit
T-cell activation, proliferation and cytotoxicity to the tumor
(15). A number of studies have
demonstrated that the expression of PD-L1 is increased in numerous
types of cancer, including breast cancer (16), renal cell carcinoma (17), ovarian cancer (18) and non-small cell lung cancer
(19). The present study
investigated the expression of PD-L1 in 96 NPC tumors and
identified a PD-L1-positive rate of 29.2% (28/96). Previous Chinese
and international studies regarding PD-L1 expression and clinical
significance in NPC have reported conflicting results. Peng et
al (20) identified a
PD-L1-positive rate of 67.2% (43/64) in NPC tissue samples. This
discrepancy with the results of the present study may be due to
differences in the evaluation of PD-L1 staining, as in the present
study, staining in <10% of the cells was considered to indicate
a negative expression status. In addition, NPC has unique regional
characteristics. The patients in the present study were from
non-high incidence area (northern China) and there may be greater
heterogeneity outside high-incidence areas.
To date, a range of studies have confirmed that
PD-L1 expression is associated with the prognosis of cancer
patients. Shi et al (21)
identified that high expression of PD-L1 in colorectal carcinoma
was associated with the tumor-nodes-metastasis stage and prognosis.
Nomi et al (22) reported
that pancreatic cancer patients with PD-L1-positive tumors
exhibited a worse prognosis than those with PD-L1-negative tumors.
Frigola et al (17) indicated
that the expression of PD-L1 was associated with the tumor stage
and prognosis in patients with renal cell carcinoma. Li et
al (23) reported that high
tumor expression of PD-L1 was associated with significantly poorer
OS and DFS. Compared with other types of head and neck tumor, NPC
has a higher risk of metastasis. Therefore, it is critically
important to screen NPC patients who may have a high risk of
recurrence and distant metastasis subsequent to conventional
radiotherapy and chemotherapy. In the present study, it was
identified that the expression of PD-L1 was not associated with
sex, age, pathological type or lymph node metastasis, whereas it
differed significantly depending on the T-stage of the primary
tumor (P=0.032) and the 1-year distant metastasis status (P=0.01),
suggesting that PD-L1-positive patients may have a relatively poor
prognosis. The result that the association between the expression
of PD-L1 and the clinical stage was not statistically significant
(P=0.051) may be due to the small sample size. In addition, at the
1-year follow-up after radiotherapy, the survival analysis
demonstrated that the DMFS for patients with tumors with a
PD-L1-positive status was lower than that of the patients with
tumors with a negative status (P=0.006).
The occurrence of NPC is highly associated with EBV
infection; infection markers including EBV-DNA, as well as EBV
EA-IgA and EBV VCA-IgA, have been widely used in the clinical
diagnosis. In addition, the detection of T lymphocyte subsets in
the peripheral blood of patients with malignant tumors by flow
cytometry may be used to determine the immune status, which is a
valuable reference for clinical diagnosis and treatment. The
detection of EBV EA-IgA and EBV VCA-IgA antibodies is a common
method for the clinical screening for and diagnosis of NPC. The
presence of cell-free fragments of EBV-DNA in the serum has
recently been identified to be valuable in predicting the prognosis
and recurrence risk of NPC (24). In
the present study, it was observed that the concentration of EBV
VCA-IgA antibody in the serum of PD-L1-positive patients was
significantly lower than that of PD-L1-negative patients (P=0.046),
although the levels in each of the two groups were above the normal
levels. In addition, the number of B lymphocytes
(CD3−CD19+) in patients with PD-L1-positive
status was significantly lower than that in patients with
PD-L1-negative status. A possible explanation is that a PD-1/PD-L1
interaction mediated a negative regulation signal to produce
immunosuppression, including the reduced secretion of the cytokines
IL-2, IL-10 and IFN-γ (5), which may
influence the number of serum B lymphocytes and the ability of B
cells to produce antibodies subsequent to accepting a viral
antigen. However, the specific mechanisms require further study.
The present results suggest that the levels of EBV VCA-IgA and
CD3−CD19+ cells may be used to predict PD-L1
expression, particularly in cases when PD-L1 cannot be detected due
to a lack of a sufficient tissue sample.
In recent years, an increasing number of clinical
trials on PD-L1 antibodies have been performed, and clinical
remission has been achieved in certain patients with non-small cell
lung cancer and renal cell carcinoma (25–27).
However, no such trials have been performed on NPC, and targeted
immunotherapy of the PD-1/PD-L1 pathway has not been fully
evaluated in NPC. In the present study, it was observed that the
positive expression rate of PD-L1 in NPC tissues was 29.2%, which
was associated with distant metastasis and the T-stage of patients.
The DMFS of patients with positive PD-L1 expression status was
significantly reduced, suggesting a poor prognosis. Therefore, it
may be hypothesized that blocking the PD-1/PD-L1 pathway may be
effective as an immunotherapy for NPC. However, the present study
was of a retrospective nature and had a small sample size, a short
follow-up time and correspondingly a small number of recurrence and
metastasis cases. In the future, a prospective study with a larger
sample size, performed over a longer period, will be required, to
allow for in-depth exploration of the association between
PD-1/PD-L1 expression and groups of NPC patients with different
prognoses, and to provide a theoretical basis for immunotherapy via
the PD-1/PD-L1 pathway.
Funding
This work was supported by the Chinese Academy of
Medical Sciences Innovation Fund for Medical Sciences (grant nos.
2017-I2M-1-013 and 2017-I2M-3-005).
Availability of data and materials
The analyzed data sets generated during the study
are available from the corresponding author on reasonable
request.
Authors' contributions
YQ and DW performed the experiments. YQ and YC
analyzed and interpreted the patient data regarding NPC. LY and HL
performed the histological examination of NPC. DW and YC were major
contributors in writing the manuscript. YC and WC conceived and
designed the experiments. All authors read and approved the final
manuscript.
Ethical approval and consent to
participate
The present study was approved by the Institutional
Review Board of the Cancer Hospital of the Chinese Academy of
Medical Sciences (Beijing, China).
Consent for publication
Written informed consent was provided by all
patients prior to enrollment in the study. The consent was provided
by the guardians if they were under 18 years of age.
Competing interests
The authors declare no potential competing interests
regarding this manuscript.
References
|
1
|
Chang ET and Adami HO: The enigmatic
epidemiology of nasopharyngeal carcinoma. Cancer Epidemiol Biomark
Prev. 15:1765–1777. 2006. View Article : Google Scholar
|
|
2
|
Lee AW, Ma BB, Ng WT and Chan AT:
Management of nasopharyngeal carcinoma: Current practice and future
perspective. J Clin Oncol. 33:3356–3364. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Chua MLK, Wee JTS, Hui EP and Chan ATC:
Nasopharyngeal carcinoma. Lancet. 387:1012–1024. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Seliger B, Marincola FM, Ferrone S and
Abken H: The complex role of B7 molecules in tumor immunology.
Trends Mol Med. 14:550–559. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
del Rio ML, Buhler L, Gibbons C, Tian J
and Rodriguez-Barbosa JI: PD-1/PD-L1, PD-1/PD-L2, and other
co-inhibitory signaling pathways in transplantation. Transpl Int.
21:1015–1028. 2008.PubMed/NCBI
|
|
6
|
Day CL, Kaufmann DE, Kiepiela P, Brown JA,
Moodley ES, Reddy S, Mackey EW, Miller JD, Leslie AJ, DePierres C,
et al: PD-1 expression on HIV-specific T cells is associated with
T-cell exhaustion and disease progression. Nature. 443:350–354.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Balar AV and Weber JS: PD-1 and PD-L1
antibodies in cancer: Current status and future directions. Cancer
Immunol Immunother. 66:551–564. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Lin X, Gudgeon NH, Hui EP, Jia H, Qun X,
Taylor GS, Barnardo MC, Lin CK, Rickinson AB and Chan AT: CD4 and
CD8 T cell responses to tumour-associated Epstein-Barr virus
antigens in nasopharyngeal carcinoma patients. Cancer Immunol
Immunother. 57:963–975. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lo YM, Chan LY, Lo KW, Leung SF, Zhang J,
Chan AT, Lee JC, Hjelm NM, Johnson PJ and Huang DP: Quantitative
analysis of cell-free Epstein-Barr virus DNA in plasma of patients
with nasopharyngeal carcinoma. Cancer Res. 59:1188–1191.
1999.PubMed/NCBI
|
|
10
|
Li J, Huang ZF, Xiong G, Mo HY, Qiu F, Mai
HQ, Chen QY, He J, Chen SP, Zheng LM, et al: Distribution,
characterization, and induction of CD8+regulatory T
cells and IL-17-producing CD8+T cells in nasopharyngeal
carcinoma. J Transl Med. 9:1892011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Lin DC, Meng X, Hazawa M, Nagata Y, Varela
AM, Xu L, Sato Y, Liu LZ, Ding LW, Sharma A, et al: The genomic
landscape of nasopharyngeal carcinoma. Nat Genet. 46:866–871. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Apetoh L, Ghiringhelli F, Tesniere A,
Obeid M, Ortiz C, Criollo A, Mignot G, Maiuri MC, Ullrich E,
Saulnier P, et al: Toll-like receptor 4-dependent contribution of
the immune system to anticancer chemotherapy and radiotherapy. Nat
Med. 13:1050–1059. 2007. View
Article : Google Scholar : PubMed/NCBI
|
|
13
|
Chen L and Flies DB: Molecular mechanisms
of T cell co-stimulation and co-inhibition. Nat Rev Immunol.
13:227–242. 2013. View
Article : Google Scholar : PubMed/NCBI
|
|
14
|
Lim DY, Tanaka Y, Iwasaki M, Gittis AG, Su
HP, Mikami B, Okazaki T, Honjo T, Minato N and Garboczi DN: The
PD-1/PD-L1 complex resembles the antigen-binding Fv domains of
antibodies and T cell receptors. Proe Natl Acad Sci USA.
105:3011–3016. 2008. View Article : Google Scholar
|
|
15
|
Chang DY, Song SH, You S, Lee J, Kim J,
Racanelli V, Son H and Shin EC: Programmed death-1 (PD-1)-dependent
functional impairment of CD4(+T cells in recurrent
genital papilloma. Clin Exp Med. 14:305–313. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Muenst S, Schaerli AR, Gao F, Däster S,
Trella E, Droeser RA, Muraro MG, Zajac P, Zanetti R, Gillanders WE,
et al: Expression of programmed death ligand 1 (PD-L1) is
associated with poor prognosis in human breast cancer. Breast
Cancer Res Treat. 146:15–24. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Frigola X, Inman BA, Lohse CM, Krco CJ,
Cheville JC, Houston TR, Leibovich B, Blute ML, Dong H and Kwon ED:
Identification of a soluble form of B7-H1 that retains
immunosuppressive activity and is associated with aggressive renal
cell carcinoma. Clin Cancer Res. 17:1915–1923. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Maine CJ, Aziz NH, Chatterjee J, Hayford
C, Brewig N, Whilding L, George AJ and Ghaem-Maghami S: Programmed
death ligand-1 over-expression correlates with malignancy and
contributes to immune regulation in ovarian cancer. Cancer Immunol
Immunother. 63:215–224. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Azuma K, Ota K, Kawahara A, Hattori S,
Iwama E, Harada T, Matsumoto K, Takayama K, Takamori S, Kage M, et
al: Association of PD-L1 overexpression with activating EGFR
mutations in surgically resected nonsmall-cell lung cancer. Ann
Oncol. 25:1935–1940. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Peng H, Zhong BL, Li YM, Wang GM and Chen
YY: Expression and significance of costimulatory molecule PD-L1 in
nasopharyngeal carcinoma. J Trop Med. 12:1367–1368. 2012.
|
|
21
|
Shi SJ, Wang LJ, Wang GD, Guo ZY, Wei M,
Meng YL, Yang AG and Wen WH: B7-H1 expression is associated with
poor prognosis in colorectal carcinoma and regulates the
proliferation and invasion of HCT116 colorectal cancer cells. PLoS
One. 8:e760122013. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Nomi T, Sho M, Akahori T, Hamada K, Kubo
A, Kanehiro H, Nakamura S, Enomoto K, Yagita H, Azuma M and
Nakajima Y: Clinical significance and therapeutic potential of the
programmed death-1 ligand/programmed death-1 pathway in human
pancreatic cancer. Clin Cancer Res. 13:2151–2157. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Li YF, Ding JW, Liao LM, Zhang ZL, Liao
SS, Wu Y, Zhou DY, Liu AW and Huang L: Expression of programmed
death ligand-1 predicts poor outcome in nasopharyngeal carcinoma.
Mol Clin Oncol. 7:378–382. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Song Y, Xiao H, Yang Z, Geng M, Ma J, Ren
Y, Liu Y and Wang G: The predictive value of pre- and
post-induction chemotherapy plasma EBV DNA level and tumor volume
for the radiosensitivity of locally advanced nasopharyngeal
carcinoma. EXCLI J. 16:1268–1275. 2017.PubMed/NCBI
|
|
25
|
Topalian SL, Hodi FS, Brahmer JR,
Gettinger SN, Smith DC, McDermott DF, Powderly JD, Carvajal RD,
Sosman JA, Atkins MB, et al: Safety, activity, and immune
correlates of anti-PD-1 antibody in cancer. N Engl J Med.
366:2443–2454. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Hamid O, Robert C, Daud A, Hodi FS, Hwu
WJ, Kefford R, Wolchok JD, Hersey P, Joseph RW, Weber JS, et al:
Safety and tumor responses with lambrolizumab (anti-PD-1) in
melanoma. N Engl J Med. 369:134–144. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Brahmer JR, Tykodi SS, Chow LQ, Hwu WJ,
Topalian SL, Hwu P, Drake CG, Camacho LH, Kauh J, Odunsi K, et al:
Safety and activity of anti-PD-L1 antibody in patients with
advanced cancer. N Engl J Med. 366:2455–2465. 2012. View Article : Google Scholar : PubMed/NCBI
|