Introduction
Intrahepatic cholangiocarcinoma (ICC) is the second
most common type of primary liver malignancy, accounting for 5–10%
of all malignant liver cancer cases (1,2). Patients
with ICC often have a poor prognosis due to a difficult early
diagnosis, a high degree of malignancy and a poor therapeutic
efficacy. Surgical resection is currently the only potential
curative therapy for ICC, but the majority of patients often
present at an advanced stage and are therefore not amenable to
surgical resection. A previous study reported that even when
patients received radical surgery, the 1-, 3- and 5-year survival
rates were 35–86, 20–52 and 20–40%, respectively (3–5). A widely
used conventional treatment for patients with advanced ICC is
chemotherapy. However, the response rates to numerous
chemotherapeutic agents are poor or non-existent given the fact
that ICC is a highly aggressive tumor that often displays
resistance to chemotherapy (3,6). The
efficacy of cytotoxic drugs, including 5-fluoropyrimidines,
gemcitabine, cisplatin/oxaliplatin, mitomycin C, doxorubicin,
docetaxel and irinotecan, have been investigated, with low response
rates of 0–36% and a median survival times of between 4.5 and 14.8
months (7–12). Previous studies have indicated that
combined chemotherapy can increase the response rate and survival
time, but typically, the response rate remains low with a higher
toxicity incidence (13,14). Thus, the development of more effective
therapies for patients with advanced ICC is warranted.
Sorafenib (Nexavar/Bay43-9006; Bayer AG, Leverkusen,
Germany) is a multi-targeted small molecule that inhibits the
activity of vascular endothelial growth factor receptor (VEGFR) 2
and 3, platelet-derived growth factor receptor (PDGFR), fibroblast
growth factor and RAF proto-oncogene, serine/threonine kinase, thus
inhibiting tumor proliferation and angiogenesis (15). Sorafenib has demonstrated safety and
efficacy against a wide variety of cancer types in numerous
preclinical and clinical studies, and has been approved for the
treatment of renal cell and hepatocellular carcinoma (16). However, limited data are available on
the use of sorafenib in patients with advanced ICC. In the current
study, the efficacy and tolerability of sorafenib in patients with
advanced ICC was evaluated.
Materials and methods
Eligibility criteria
Patients eligible for the present study had a
cytologically or pathologically confirmed diagnosis of ICC that was
surgically unresectable or metastatic, and excluded combined
hepatocellular carcinoma and cholangiocarcinoma. Measurable disease
was required with no prior therapy. Previous chemotherapy,
radiation therapy, transcatheter arterial chemoembolization or
other local treatments were permitted only when the size of the
measurable lesions had increased by >25%, and it must have been
completed ≥4 weeks prior to enrollment. Patients were >18 years
old, had an expected lifespan of >12 weeks and an Eastern
Cooperative Oncology Group (ECOG) (17) performance status of 0–2. In addition,
patients had adequate liver and renal function tests with a total
bilirubin level ≤2 times the upper limit of the normal level, AST
or ALT levels ≤2 times the upper limit of the normal level, a serum
creatinine level of <2 mg/dl and a creatinine clearance rate of
≥60 ml/min. Requirements also included adequate bone marrow
function, as indicated by an absolute neutrophil count of
≥1,500/mm3, a platelet count of ≥60×109/l, a
hemoglobin level of ≥8.0 g/dl, an International Normalized Ratio of
≤2.3 or a prothrombin time prolonged by ≤6 sec.
The present study was approved by the Human Research
Ethics Committee of Anhui Medical University (Hefei, China) and
written informed consent was obtained from all patients.
Study design
The present study was a single-arm open-label
exploratory study whose primary aim was the evaluation of
single-agent sorafenib activity, defined as the control rate at 12
weeks, in patients with advanced ICC. The disease control rate
(DCR) was defined as the percentage of patients that exhibited no
disease progression [complete response (CR), partial response (PR)
and stable disease (SD)] but who remained under treatment at 12
weeks. Secondary endpoints included time to progression (TTP),
progression-free survival (PFS), overall survival (OS), duration of
treatment (DOT) and the adverse event profile. TTP was defined as
the time between the first day of administration of sorafenib and
confirmed disease progression upon imaging. PFS was defined as the
time between the first day of administration of sorafenib and
confirmed disease progression upon imaging or mortality due to any
cause. OS was defined as the time between the first day of
sorafenib administration and mortality or last contact.
Treatment plan
Sorafenib (Nexavar/Bay43-9006; Bayer AG, Leverkusen,
Germany) was administered at a fixed dose of 400 mg twice a day
continuously in a 3-week cycle until disease progression,
intolerant drug-associated toxicity, the necessity for cessation of
the medication or withdrawal of patient consent occurred.
Doses were delayed or reduced in cases of possible
associated hematological or non-hematological toxicity graded
according to the National Cancer Institute Common Terminology
Criteria for Adverse Events (NCI CTCAE; version 4.0) (18). Sorafenib was taken orally at the
following predefined dose levels: Level-1, 400 mg every 12 h;
level-2, 400 mg every day; and level-3, 400 mg every other day. In
the case of G1-G2 hematological and non-hematological toxicity, no
dose modification or delay was planned. For G3 hematological
toxicity, treatment was continued with a dose reduction of one dose
level. For G4 hematological and G3 nonhematological toxicity,
treatment was delayed until toxicity resolution to G1-G2, and a
dose reduction of one level was planned. In the case of G4
non-hematological toxicity, treatment was terminated. Patients
requiring treatment interruption for >1 month or requiring a
reduction of >2 dose levels were removed from treatment unless
it was considered clinically beneficial.
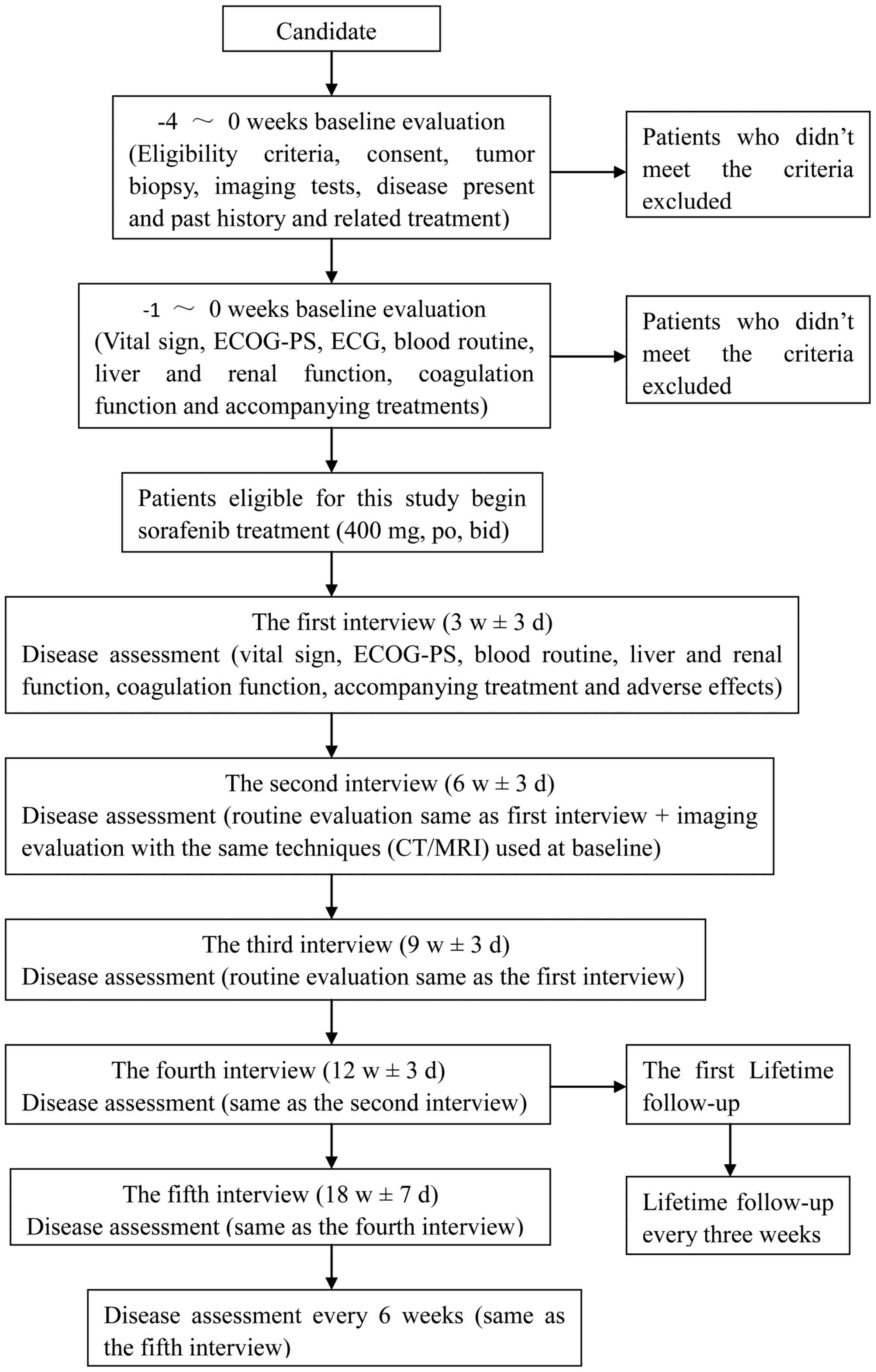
Disease assessment
Baseline evaluation included medical history,
physical examination, pathological ICC diagnosis and tumor
assessment using computed tomography (CT) or magnetic resonance
imaging (MRI) according to the Response Evaluation Criteria in
Solid Tumors (RECIST; version 1.1) (19) within 28 days of study entry.
Patients were contacted and interviewed every 3
weeks within the first 3 months after the start of treatment.
Disease assessment included determination of vital signs, ECOG
performance status, blood routine, liver and renal function,
coagulation function, accompanying treatment and adverse effects.
The interval between follow-ups could be prolonged to 6 weeks after
the first 3 months. Tumor response was evaluated every 6 weeks
using CT or MRI. Lifetime follow-up was to be conducted every 3
months and telephone follow-up was allowed (Fig. 1).
Toxicity assessment
Patients were evaluated for treatment-associated
toxicity in each cycle for the first 12 weeks and every two cycles
thereafter according to the NCI CTCAE.
Statistical analysis
The primary endpoint of the trial was taken as the
DCR (CR+PR+SD, according to the RECIST criteria) at 12 weeks.
Second endpoints included TTP, OS, DFS, DOT and safety. Survival
analysis was performed using the Kaplan-Meier method. All
statistical analyses were performed using SPSS software (version
17.0; SPSS Inc., Chicago, IL, USA).
Results
Patient characteristics and treatment
administration
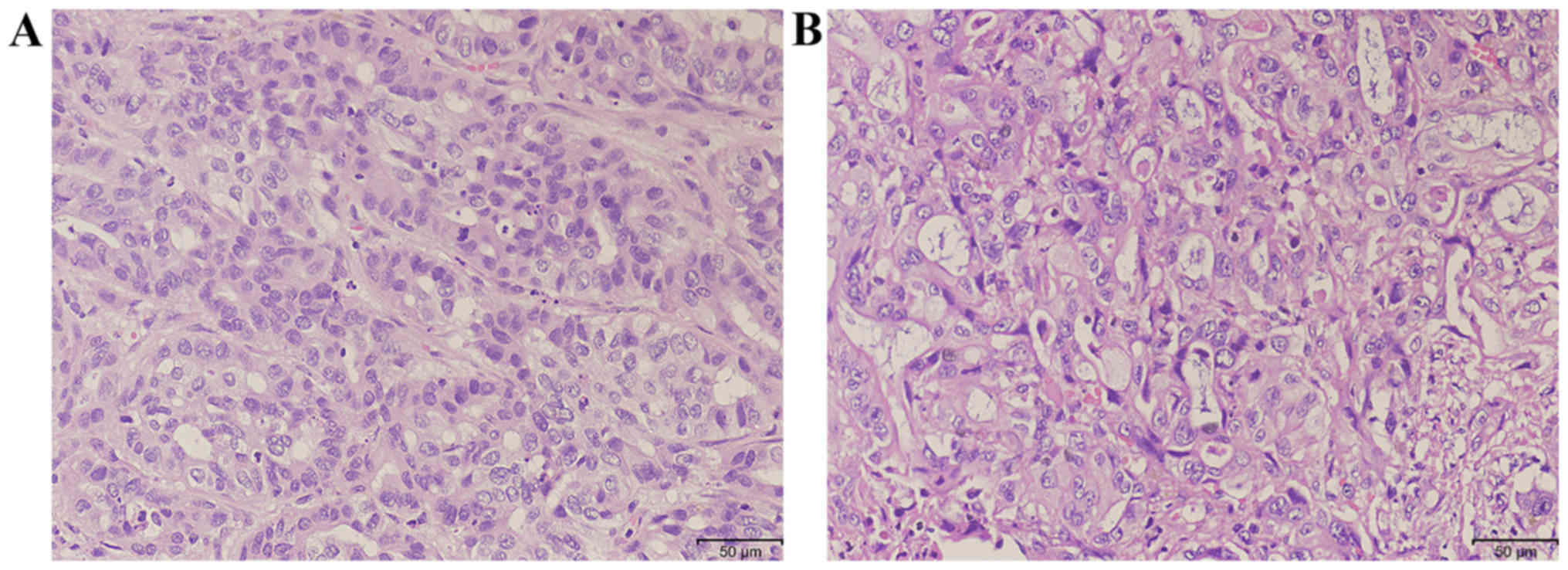
A total of 15 patients with pathologically confirmed
diagnosis of ICC were enrolled for the present study over a period
of 24 months (Fig. 2; Table I). The median age was 53 years (range,
39–65 years), with 8 males and 7 females. All patients had a good
ECOG performance status of 0–1 prior to sorafenib administration. A
total of 10 patients had received previous treatment; 4 had
received radical surgery (all with tumor recurrence following
surgery) and 6 had received palliative surgery or biopsy. Overall,
1 patient received radiotherapy and 1 received chemotherapy
following surgery.
 | Table I.Clinicopathological characteristics of
patients (n=15) with intrahepatic cholangiocarcinoma. |
Table I.
Clinicopathological characteristics of
patients (n=15) with intrahepatic cholangiocarcinoma.
| Clinicopathological
characteristic | Value |
|---|
| Age, years |
|
Median | 53 |
|
Range | 39–65 |
| Gender, n (%) |
| Male | 8
(53.3) |
|
Female | 7
(46.7) |
| ECOG performance
status, n (%) |
| 0 | 12 (80.0) |
| 1 | 3
(20.0) |
| Macrovascular
invasion, n (%) |
|
Present | 4
(26.7) |
|
Absent | 11 (73.3) |
| Extrahepatic tumor
metastasis, n (%) |
|
Present | 9
(60.0) |
|
Absent | 6
(40.0) |
| Extent of disease, n
(%) |
|
Liver | 15
(100.0) |
| Lymph
nodes | 9
(60.0) |
|
Lung | 1 (6.7) |
| Soft
tissue | 3
(20.0) |
| Previous treatment,
n (%) | 10 (66.7) |
|
Surgery | 10 (66.7) |
|
Radical | 4
(26.7) |
|
Palliative/biopsy | 6
(40.0) |
|
Radiotherapy after
surgery | 1 (6.7) |
|
Chemotherapy after
surgery | 1 (6.7) |
The median DOT was 3.2 months (range, 1.5–30
months). Sorafenib was discontinued in 14 patients due to tumor
progression in 4 patients (26.7%), intolerance to an adverse event
in 1 patient (6.7%), mortality in 2 patients (13.3%) and liver
failure in 7 patients (46.7%). By the time the follow-up of the
study ended (July 2014), only 1 patient (6.7%) remained on
sorafenib treatment.
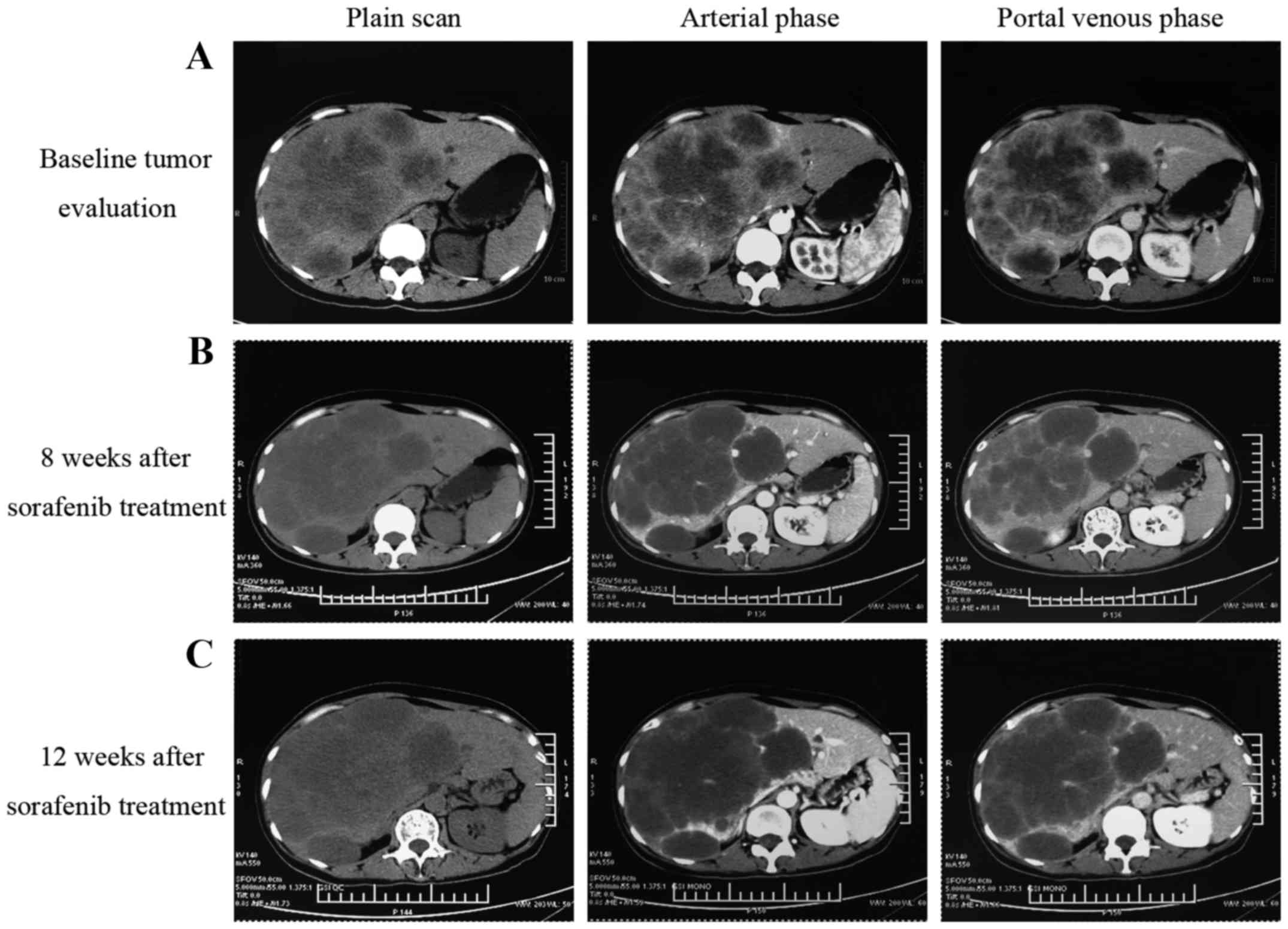
Efficacy
Following sorafenib monotherapy, 4 patients achieved
a partial response and 7 patients achieved a stable disease status,
with a DCR of 73.3% at 12 weeks (Table
II). Among the 4 patients who achieved a partial response, 1
patient succumbed with an inferior OS time of 4.2 months. As
illustrated in Fig. 3, the CT scan
image at 8 and 12 weeks post-sorafenib treatment demonstrated that
the tumor had developed liquefactive necrosis and was less viable.
The patient subsequently succumbed to liver failure induced by
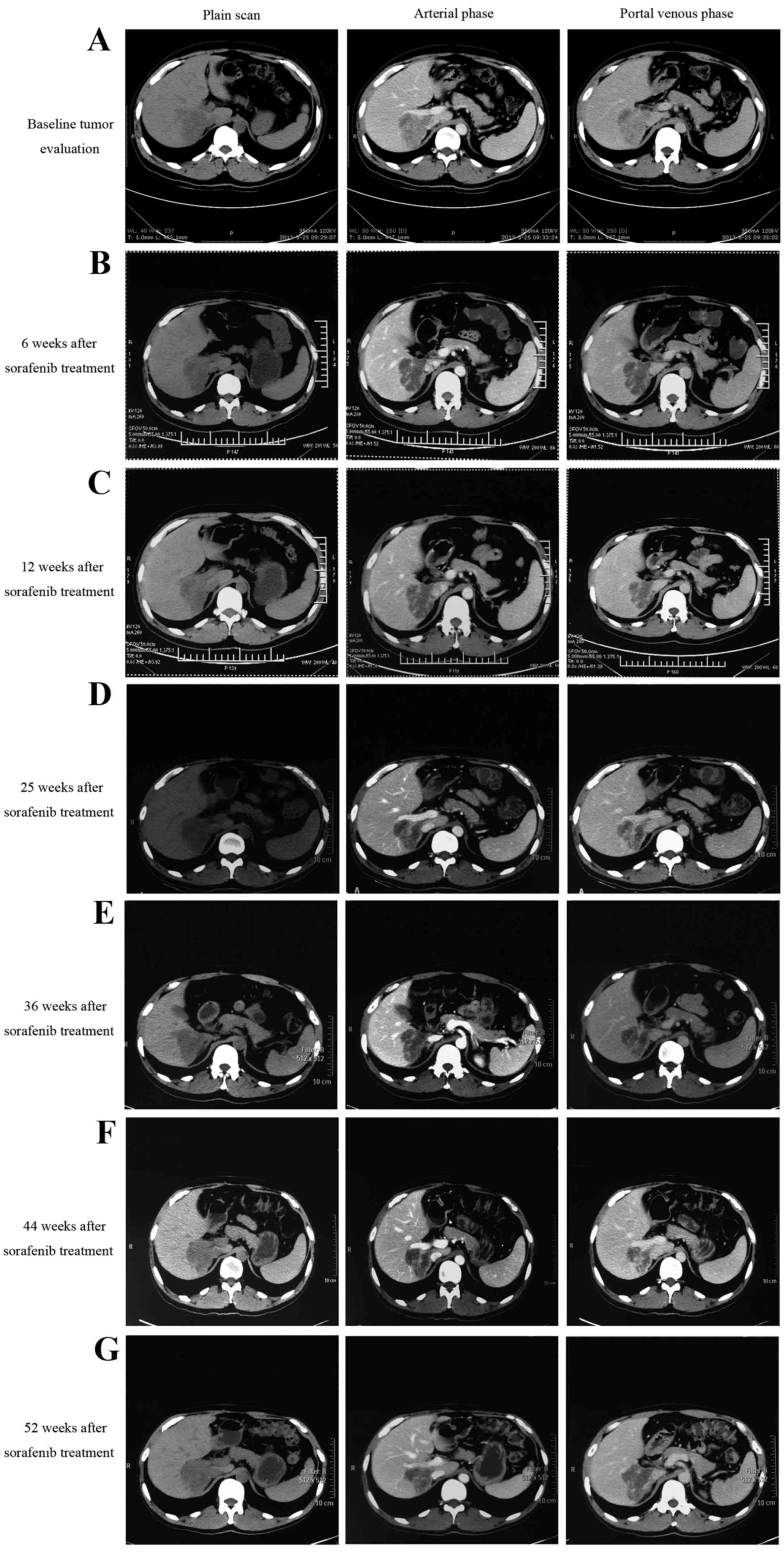
hepatic portal tumor compression. As illustrated in Fig. 4, another patient who presented with
unresectable ICC due to portal and inferior vena cava invasion
achieved a partial response following sorafenib treatment. The
patient had received sorafenib treatment for 15 months and remained
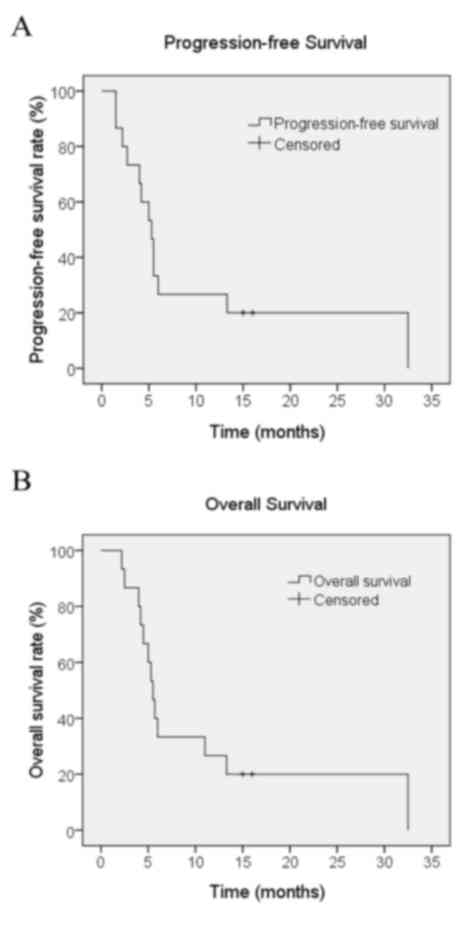
on sorafenib treatment. The median OS time for all patients was 5.7
months [range, 2.2–32.5 months; 95% confidence interval (CI),
5.0–6.4] and the median PFS time was 5.5 months (range, 1.5–32.5
months; 95% CI, 3.9–7.1), as illustrated in Fig. 5. The median TTP was 3.2 months (range,
1.5–29 months).
| Table II.Therapeutic efficacy of sorafenib inn
patients with intrahepatic cholangiocarcinoma. |
Table II.
Therapeutic efficacy of sorafenib inn
patients with intrahepatic cholangiocarcinoma.
| Response | Cases, n | Rate, % |
|---|
| Complete
response | 0 | 0.0 |
| Partial
response | 4 | 26.7 |
| Stable disease | 7 | 46.7 |
| Progressive
disease | 4 | 26.7 |
| Disease control
rate | 11 | 73.3 |
| Total | 15 | 100.0 |
Toxicity
All patients were assessed for toxicity. There were
no treatment-associated mortalities. As illustrated in Table III, the main adverse effects of
sorafenib included skin rashes, hand-foot syndrome, diarrhea,
nausea/vomiting, liver enzyme and bilirubin elevation, and fatigue.
G1-2 toxicity was observed in 8 patients (53.3%) while G3-4
toxicity was observed in 1 patient (6.7%). The most common toxicity
was a skin rash, which was present in 5 patients (33.3%). A single
patient exhibited G3 toxicity in the form of hand-foot syndrome
toxicity. Hematological toxicity was not identified in any
patients.
| Table III.Treatment-associated toxicities
following sorafenib treatment in patients with intrahepatic
cholangiocarcinoma. |
Table III.
Treatment-associated toxicities
following sorafenib treatment in patients with intrahepatic
cholangiocarcinoma.
| Toxicity | G1-G2, n (%) | G3-G4, n (%) | Total, n (%) |
|---|
| Bilirubin
elevation | 2 (13.3) | 0 (0.0) | 2 (13.3) |
| Skin rash | 5 (33.3) | 0 (0.0) | 5 (33.3) |
| Hand-foot
syndrome | 2 (13.3) | 1 (6.7) | 3 (20.0) |
| Diarrhea | 2 (13.3) | 0 (0.0) | 2 (13.3) |
|
Nausea/vomiting | 3 (20.0) | 0 (0.0) | 3 (20.0) |
| Liver enzyme
elevation | 2 (13.3) | 0 (0.0) | 2 (13.3) |
| Fatigue | 4 (26.7) | 0 (0.0) | 4 (26.7) |
| Total | 8 (53.3) | 1 (6.7) | 9 (60.0) |
Discussion
Few treatment options are available for ICC, and the
prognosis of affected patients is extremely poor. Advanced ICC
poses a significant therapeutic challenge for multiple reasons,
including a low radical resection rate, the limited efficacy of
cytotoxic chemotherapy and the rarity of the disease, leading to
difficulties in conducting large randomized studies (20–25). Novel
effective therapeutic approaches are required in order to improve
the treatment outcome of patients with ICC.
Sorafenib is an oral multikinase inhibitor with
existing approval for the treatment of metastatic renal cell and
advanced hepatocellular carcinoma. Furthermore, sorafenib has been
demonstrated to exhibit significant antitumor activity in various
cholangiocarcinoma cell lines and in xenograft ICC models (26–28). The
mechanism underlying the effects of sorafenib may involve the
ability to simultaneously inhibit tumor angiogenesis (via VEGF and
PDGF signaling pathways) and tumor cell survival (via
Ras/Raf/MEK/ERK1/mitogen activated protein kinase-2 kinase, and
signal transducer and activator of transcription 3-dependent
signaling pathways) (27,29). Owing to the molecular alterations
described in ICC, the present study aimed to investigate the
efficacy of sorafenib as a single agent in patients with advanced
ICC. The DCR at 12 weeks was defined as the primary endpoint, which
is considered a suitable endpoint in oncology when a non-cytotoxic
agent is used, and a low objective response and high SD rate is
expected (30).
At the intention-to-treat analysis, the response and
SD rates were 26.7, and 46.7%, respectively, with a DCR of 73.3%.
The median PFS and OS times were 5.5, and 5.7 months, respectively.
In a previous phase II study on sorafenib treatment as a single
agent in 46 patients with advanced biliary tract carcinoma, an
objective response rate of 2% and a DCR at 12 weeks of 32.6% were
reported. In addition, the median PFS and OS times were 2.3, and
4.4 months, respectively (31). One
possible explanation for the inferior survival outcomes reported in
this study is that 56% of patients had ≥1 prior lines of
chemotherapy prior to enrollment. In the present study, 1 patient
who received combined chemotherapy following surgery experienced
PFS and OS times of 6 months. Another patient who received
radiotherapy following surgery experienced worse PFS and OS times
of 2.2 months. A previous phase II study on gemcitabine and
cisplatin combined with sorafenib in patients with advanced biliary
adenocarcinomas demonstrated that the addition of sorafenib to
gemcitabine and cisplatin in biliary adenocarcinomas did not
improve efficacy compared with previous data, and showed that
toxicity was increased (32).
However, a previous comprehensive review summary stated that a
combination of sorafenib with cytotoxic agents is generally well
tolerated (33). In addition, several
phase I and II studies have demonstrated that the combination of
sorafenib with cytotoxic agents in several solid tumor types,
including hepatocellular carcinoma, melanoma, and gastric,
colorectal, breast and ovarian cancer, achieved promising results
(33). However, limited data are
available on the combination of sorafenib with chemotherapeutic
agents or radiotherapy in patients with ICC. Studies into the
effect of a combination of sorafenib with cytotoxic drugs therapy
or radiotherapy on advanced ICC are warranted.
A previous phase II trial that used sorafenib as a
first-line treatment for advanced cholangiocarcinoma and
gallbladder cancer failed to demonstrate a clinically significant
objective response (34). A confirmed
response rate of 0% and a DCR of 39% were reported. In addition,
the patients experienced a median PFS time of 3 months and a median
OS time of 9 months (34). It has
been noted that the response rate and survival outcomes appear to
be different among patients with gallbladder carcinoma vs.
intrahepatic cholangiocarcinoma vs. extrahepatic cholangiocarcinoma
(35); the limitation of this study
was the incorporation of all biliary cancer types into one group,
irrelevant of the site of origin. The molecular changes associated
with biliary tract adenocarcinoma development and progression was
poorly defined, and it is unclear whether suggested
location-associated differences in pathogenesis can influence
clinical behavior and patient prognosis. However, a study on 128
patients who underwent resection for biliary cancer indicated that
biliary tract cancer exhibits differential expression of cell cycle
regulatory proteins according to the tumor site of origin and
morphology, demonstrating different survival outcomes (36). Thus, the response rate and survival
outcomes may be different due to location-associated differences in
molecular changes. To the best of our knowledge, the present study
was the first to investigate the efficacy of sorafenib in patients
with ICC, and it achieved promising response rates.
The toxicity profile of sorafenib in the present
study was manageable. Toxicities observed were primarily grades 1
and 2. The most common toxicity was a skin rash in 5 patients
(33.3%). A previous study on the effects of sorafenib in patients
with hepatocellular carcinoma reported an improved response in
patients with early skin reactions (37). However, the same correlation was not
established in the current study. Grade 3 hand-foot syndrome was
observed in 1 atient (6.7%) and hematological toxicity was not
identified in any patients. The safety profile of sorafenib in the
present study is acceptable in comparison with that observed in
patients treated with chemotherapy. Several phase II clinical
trials on the effects of gemcitabine combined with cisplatin in
patients with advanced biliary tract carcinoma reported grade 3–4
toxicity in 33–75% of patients (13,38,39).
One limitation of the present study was that it was
a single institute study with a small sample size. The results
indicate the requirement for a multiple center phase II or III
clinical trial with a large sample size.
In conclusion, the results of the present study have
provided the first evidence that sorafenib is generally well
tolerated and active in patients with advanced ICC. In order to
enhance the treatment efficacy of sorafenib, further trials focused
on the effects of sequential or combination therapy are warranted,
as patients eventually develop progressive disease when on
sorafenib or cannot tolerate the treatment. Correlative studies to
define predictive molecular markers for sorafenib are required.
Acknowledgements
The abstract was presented at the 8th Annual Meeting
of Chinese College of Surgeons and the 19th Annual Meeting of the
European Society of Surgery, May 15–17, 2015, in Beijing, China,
and was previously published in European Surgery, May 2015, Volume
47, Supplement 1, p1-281.
References
|
1
|
Casavilla FA, Marsh JW, Iwatsuki S, Todo
S, Lee RG, Madariaga JR, Pinna A, Dvorchik I, Fung JJ and Starzl
TE: Hepatic resection and transplantation for peripheral
cholangiocarcinoma. J Am Coll Surg. 185:429–436. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Jemal A, Bray F, Center MM, Ferlay J, Ward
E and Forman D: Global cancer statistics. CA Cancer J Clin.
61:69–90. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Morise Z, Sugioka A, Tokoro T, Tanahashi
Y, Okabe Y, Kagawa T and Takeura C: Surgery and chemotherapy for
intrahepatic cholangiocarcinoma. World J Hepatol. 2:58–64.
2010.PubMed/NCBI
|
|
4
|
Tan JC, Coburn NG, Baxter NN, Kiss A and
Law CH: Surgical management of intrahepatic cholangiocarcinoma-a
population-based study. Ann Surg Oncol. 15:600–608. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Paik KY, Jung JC, Heo JS, Choi SH, Choi DW
and Kim YI: What prognostic factors are important for resected
intrahepatic cholangiocarcinoma? J Gastroenterol Hepatol.
23:766–770. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Skipworth JR, Keane MG and Pereira SP:
Update on the management of cholangiocarcinoma. Dig Dis.
32:570–578. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Okusaka T, Ishii H, Funakoshi A, Yamao K,
Ohkawa S, Saito S, Saito H and Tsuyuguchi T: Phase II study of
single-agent gemcitabine in patients with advanced biliary tract
cancer. Cancer Chemother Pharmacol. 57:647–653. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Penz M, Kornek GV, Raderer M, Ulrich-Pur
H, Fiebiger W, Lenauer A, Depisch D, Krauss G, Schneeweiss B and
Scheithauer W: Phase II trial of two-weekly gemcitabine in patients
with advanced biliary tract cancer. Ann Oncol. 12:183–186. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Hezel AF and Zhu AX: Systemic therapy for
biliary tract cancers. Oncologist. 13:415–423. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ducreux M, Van Cutsem E, Van Laethem JL,
Gress TM, Jeziorski K, Rougier P, Wagener T, Anak O, Baron B and
Nordlinger B: EORTC Gastro Intestinal Tract Cancer Group: A
randomised phase II trial of weekly high-dose 5-fluorouracil with
and without folinic acid and cisplatin in patients with advanced
biliary tract carcinoma: Results of the 40955 EORTC trial. Eur J
Cancer. 41:398–403. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Eckel F and Schmid RM: Chemotherapy in
advanced biliary tract carcinoma: A pooled analysis of clinical
trials. Br J Cancer. 96:896–902. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Chen JS, Lin YC, Jan YY and Liau CT:
Mitomycin C with weekly 24-h infusion of high-dose 5-fluorouracil
and leucovorin in patients with biliary tract and periampullar
carcinomas. Anticancer Drugs. 12:339–343. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Valle J, Wasan H, Palmer DH, Cunningham D,
Anthoney A, Maraveyas A, Madhusudan S, Iveson T, Hughes S, Pereira
SP, et al: Cisplatin plus gemcitabine versus gemcitabine for
biliary tract cancer. N Engl J Med. 362:1273–1281. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Hsu C, Shen YC, Yang CH, Yeh KH, Lu YS,
Hsu CH, Liu HT, Li CC, Chen JS, Wu CY and Cheng AL: Weekly
gemcitabine plus 24-h infusion of high-dose
5-fluorouracil/leucovorin for locally advanced or metastatic
carcinoma of the biliary tract. Br J Cancer. 90:1715–1719.
2004.PubMed/NCBI
|
|
15
|
Wilhelm SM, Carter C, Tang L, Wilkie D,
McNabola A, Rong H, Chen C, Zhang X, Vincent P, McHugh M, et al:
BAY 43–9006 exhibits broad spectrum oral antitumor activity and
targets the RAF/MEK/ERK pathway and receptor tyrosine kinases
involved in tumor progression and angiogenesis. Cancer Res.
64:7099–7109. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Di Marco V, De Vita F, Koskinas J, Semela
D, Toniutto P and Verslype C: Sorafenib: From literature to
clinical practice. Ann Oncol. 24:(Suppl 2). ii30–ii37. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Oken MM, Creech RH, Tormey DC, Horton J,
Davis TE, McFadden ET and Carbone PP: Toxicity and response
criteria of the Eastern Cooperative Oncology Group. Am J Clin
Oncol. 5:649–655. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Basch E, Reeve BB, Mitchell SA, Clauser
SB, Minasian LM, Dueck AC, Mendoza TR, Hay J, Atkinson TM,
Abernethy AP, et al: Development of the national cancer institute's
patient-reported outcomes version of the common terminology
criteria for adverse events (PRO-CTCAE). J Natl Cancer Inst.
106:pii: dju244. 2014. View Article : Google Scholar
|
|
19
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Patel T: Increasing incidence and
mortality of primary intrahepatic cholangiocarcinoma in the United
States. Hepatology. 33:1353–1357. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Altekruse SF, McGlynn KA and Reichman ME:
Hepatocellular carcinoma incidence, mortality, and survival trends
in the United States from 1975 to 2005. J Clin Oncol. 27:1485–1491.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Mosconi S, Beretta GD, Labianca R, Zampino
MG, Gatta G and Heinemann V: Cholangiocarcinoma. Crit Rev Oncol
Hematol. 69:259–270. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Anderson CD, Pinson CW, Berlin J and Chari
RS: Diagnosis and treatment of cholangiocarcinoma. Oncologist.
9:43–57. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Pattanathien P, Khuntikeo N, Promthet S
and Kamsa-Ard S: Survival rate of extrahepatic cholangiocarcinoma
patients after surgical treatment in Thailand. Asian Pac J Cancer
Prev. 14:321–324. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Jarnagin WR, Fong Y, DeMatteo RP, Gonen M,
Burke EC, Bodniewicz BSJ, Youssef BAM, Klimstra D and Blumgart LH:
Staging, resectability, and outcome in 225 patients with hilar
cholangiocarcinoma. Ann Surg. 234:517–519. 2001. View Article : Google Scholar
|
|
26
|
Kim DH, Jeong YI, Chung CW, Kim CH, Kwak
TW, Lee HM and Kang DH: Preclinical evaluation of sorafenib-eluting
stent for suppression of human cholangiocarcinomacells. Int J
Nanomedicine. 8:1697–1711. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Sugiyama H, Onuki K, Ishige K, Baba N,
Ueda T, Matsuda S, Takeuchi K, Onodera M, Nakanuma Y, Yamato M, et
al: Potent in vitro and in vivo antitumor activity of sorafenib
against human intrahepatic cholangiocarcinoma cells. J
Gastroenterol. 46:779–789. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Wang C, Maass T, Krupp M, Thieringer F,
Strand S, Wörns MA, Barreiros AP, Galle PR and Teufel A: A systems
biology perspective on cholangiocellular carcinoma development:
Focus on MAPK-signaling and the extracellular environment. J
Hepatol. 50:1122–1131. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Blechacz BR, Smoot RL, Bronk SF, Werneburg
NW, Sirica AE and Gores GJ: Sorafenib inhibits signal transducer
and activator of transcription-3 signaling in cholangiocarcinoma
cells by activating the phosphatase shatterproof 2. Hepatology.
50:1861–1870. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Adjei AA, Christian M and Ivy P: Novel
designs and end points for phase II clinical trials. Clin Cancer
Res. 15:1866–1872. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Bengala C, Bertolini F, Malavasi N, Boni
C, Aitini E, Dealis C, Zironi S, Depenni R, Fontana A, Del Giovane
C, et al: Sorafenib in patients with advanced biliary tract
carcinoma: A phase II trial. Br J Cancer. 102:68–72. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Lee JK, Capanu M, O'Reilly EM, Ma J, Chou
JF, Shia J, Katz SS, Gansukh B, Reidy-Lagunes D, Segal NH, et al: A
phase II study of gemcitabine and cisplatin plus sorafenib in
patients with advanced biliary adenocarcinomas. Br J Cance.
109:915–919. 2013. View Article : Google Scholar
|
|
33
|
Dal Lago L, D'Hondt V and Awada A:
Selected combination therapy with sorafenib: A review of clinical
data and perspectives in advanced solid tumors. Oncologist.
13:845–858. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
El-Khoueiry AB, Rankin CJ, Ben-Josef E,
Lenz HJ, Gold PJ, Hamilton RD, Govindarajan R, Eng C and Blanke CD:
SWOG 0514: A phase II study of sorafenib in patients with
unresectable or metastatic gallbladder carcinoma and
cholangiocarcinoma. Invest New Drugs. 30:1646–1651. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Nathan H, Pawlik TM, Wolfgang CL, Choti
MA, Cameron JL and Schulick RD: Trends in survival after surgery
for cholangiocarcinoma: A 30-year population-based SEER database
analysis. J Gastrointest Surg. 11:1488–1497. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Jarnagin WR, Klimstra DS, Hezel M, Gonen
M, Fong Y, Roggin K, Cymes K, DeMatteo RP, D'Angelica M, Blumgart
LH and Singh B: Differential cell cycle-regulatory protein
expression in biliary tract adenocarcinoma: Correlation with
anatomic site, pathologic variables, and clinical outcome. J Clin
Oncol. 24:1152–1160. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Vincenzi B, Santini D, Russo A, Addeo R,
Giuliani F, Montella L, Rizzo S, Venditti O, Frezza AM, Caraglia M,
et al: Early skin toxicity as a predictive factor for tumor control
in hepatocellular carcinoma patients treated with sorafenib.
Oncologist. 15:85–92. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Thongprasert S, Napapan S, Charoentum C
and Moonprakan S: Phase II study of gemcitabine and cisplatin as
first-line chemotherapy in inoperable biliary tract carcinoma. Ann
Onco. 16:279–281. 2005. View Article : Google Scholar
|
|
39
|
Weigt J and Malfertheiner P: Cisplatin
plus gemcitabine versus gemcitabine for biliary tract cancer.
Expert Rev Gastroenterol Hepatol. 4:395–397. 2010. View Article : Google Scholar : PubMed/NCBI
|