Introduction
Triple-negative breast cancer (TNBC) is defined as a
breast carcinoma without estrogen receptor (ER) and progesterone
receptor (PR) immunoexpression, and with a lack of amplification of
human epidermal growth factor receptor-2 (HER2). The disease
accounts for ~15% of all breast carcinomas (1–3). TNBC
shows biological aggressiveness and a higher recurrence rate, with
no benefit from endocrine or HER2-targeted therapies (1–3). A number
of studies have previously been performed to identify additional
prognostic markers to better classify TNBC and stratify it into
subgroups with different clinical courses (3–8).
Lactoferrin (LF), an iron binding 78- to 80-kDa
glycoprotein usually present in mammalian milk, has been
immunohistochemically revealed in numerous human neoplastic
conditions of different sites (9–22). An
immunopositive LF rate with a large variability, ranging from 7.5
to 42% of cases, has previously been identified in breast carcinoma
(23–27); however, LF was more often observed in
low-grade ER/PR-positive ductal carcinomas, confirming a decrease
in LF immunostaining in less differentiated and more aggressive
breast carcinomas (25–27). Moreover, it has been hypothesized that
increased LF levels LF may be associated with reduced ERα and PR
expression, and possibly reduced HER2 expression, and could
therefore contribute to TNBC phenotype development (24). Consequently, taking into consideration
the downregulation of ER, PR and HER2 at post-transcriptional
levels in TNBC cell lines (24), the
present study analyzed the immunohistochemical distribution of LF
in a cohort of human surgical TNBC patients.
Patients and methods
Patient cohort
The present study retrospectively investigated LF
immunoexpression in a cohort of 65 TNBC cases that were surgically
treated by breast-conserving surgery (lumpectomy, quadrantectomy,
partial mastectomy or segmental mastectomy), at the polyclinic ‘G.
Martino’ of Messina, as well as at the Humanitas Oncology Center of
Catania, between January 2001 and June 2015, and were not
previously subjected to any neoadjuvant treatment. All female
patients (mean age, 59.9 years; range, 38–82 years) were diagnosed
with TNBC, as 0% ER and PR cell staining was recorded upon
immunohistochemical analysis, as well as a HER2 staining score of
0% upon immunohistochemical analysis or a score of 1+ and 2+ with
no gene amplification, as verified by fluorescence in situ
hybridization (6). For all cases,
clinicopathological parameters, including age, grading and tumor
stage, were recorded according to international guidelines. Data on
the follow-up, including the recurrence of the disease, were
available for all patients, with the exception of 3 who were lost
to follow-up. The study was conducted in accordance with Good
Clinical Practice guidelines and the Declaration of Helsinki, and
was approved by the Local Ethics Committees of Polyclinic ‘G.
Martino’ (Messina, Italy) and Humanitas Oncology Center (Catania,
Italy).
Immunohistochemical methods
All surgical samples were fixed in 10% neutral
formalin for 24–36 h at room temperature, and then embedded in
paraffin at 56°C. From each tissue block, 4-µm sections were
stained with hematoxylin and eosin (H&E) for microscopic
examination. Parallel sections were cut and mounted on
silane-coated glasses, then dewaxed in xylene and rehydrated in
graded ethanols. Antigen retrieval was performed prior to the
addition of the primary antibody lactoferrin [clone 1A1; dilution,
1:75; catalog no., K99172B; Biodesign International, Inc., Saco,
ME, USA] by heating slides placed in 0.01 M citrate buffer at pH
6.0 in a microwave oven (750 W) for 3 cycles of 5 min each.
Immunohistochemical procedures, and positive and
negative controls of LF staining were performed as previously
described (18,19).
Immunohistochemical
quantification
The analysis of immunostained sections was estimated
by light microscopy using 20X and 40X objective lenses, and a ×10
eyepiece. Two pathologists used a double-headed microscope to
perform the assessment of LF-immunostained sections on a consensus
basis. The percentage of stained neoplastic cells [area of staining
positivity (ASP)] was graded as follows: 0) no staining; i) >0
to 5% staining; ii) >5 to 50% staining; and iii) >50%
staining. In addition, the intensity of staining (IS) (1, weak; 2,
moderate; and 3, strong) was also taken into consideration.
Successively, a LF intensity distribution (ID) score was calculated
for each case by multiplying the ASP and IS values, as previously
described (28,29); using this method, only cases showing
an ID score of >2 were considered as positive for LF.
Moreover, data concerning the Ki-67 labeling index
(LI) status were also available and had been evaluated by counting
the percentage of positive nuclei per 1,000 malignant cells in up
to 10 fields representative of the whole neoplastic portions. The
median MIB-1 staining score value (20%) was utilized as a cut-off
point to determine low and high Ki-67 expression, as described
previously (30); this mean value
corresponded to the value indicated by the majority of the St.
Gallen Breast Cancer Panel (31).
Statistical analysis
The statistical association between LF
immunoexpression and the various clinicopathological parameters was
investigated using the χ2 test or Fisher's exact test,
as appropriate.
Disease-free survival (DFS) and cancer-specific
survival (CSS) were assessed by the Kaplan-Meier method, with the
date of primary surgery as the entry data. The end point for the
DFS analysis was disease progression. CSS was characterized as the
length of survival to mortality due to TNBC or to the last
follow-up date. Patients who succumbed as a result of diseases
independent from TNBC were censored. The Mantel-Cox log-rank test
was applied to assess the strength of the association between DFS
or CSS and each of the parameters [age, histological grade,
pathological tumor (pT) stage, pathological node (pN) stage
(6)], Ki-67 LI and LF
immunoexpression) as a single variable. Successively, a
multivariate analysis (Cox regression model) with stepwise method
was utilized to determine the independent effect of each variable
on survival.
P<0.05 was considered to indicate a statistically
significant difference. Data were analyzed using the SPSS package
version 6.1.3 (SPSS, Inc., Chicago, IL, USA).
Results
The routinely stained H&E sections exhibited
good morphology, confirming the histopathological diagnosis of
ductal invasive breast carcinoma (BC) in all cases. The
immunoistochemical confirmed the diagnosis of TNBC.
Clinicopathological and immunohistochemical data for
LF for the 65 available TNBC cases analyzed are shown in Table I. The follow-up time ranged from 3 to
112 months (mean, 54.5 months).
 | Table I.Associations between
clinicopathological characteristics and LF expression. |
Table I.
Associations between
clinicopathological characteristics and LF expression.
|
| LF
immunoexpression |
|
|---|
|
|
|
|
|---|
| Parameter | Negative | Positive | P-value |
|---|
| Age |
|
| 1.000 |
| ≤70
years | 26 | 9 |
|
| >70
years | 25 | 8 |
|
| pT |
|
| 0.640 |
| 1 | 27 | 10 |
|
| 2 | 19 | 4 |
|
| 3 | 1 | 1 |
|
| 4 | 4 | 2 |
|
| pN |
| N0 | 30 | 8 |
|
| N+ | 21 | 9 |
|
| Histological
grade |
|
| 0.410 |
| 2 | 20 | 6 |
|
| 3 | 31 | 11 | 1.000 |
| Ki-67 LI |
|
| 0.040a |
| Low
(≤20%) | 20 | 12 |
|
| High
(>20%) | 31 | 5 |
|
| Recurrence |
|
| 0.010a |
|
Absent | 19 | 13 |
|
|
Present | 29 | 4 |
|
| Status |
|
| 0.020a |
|
Alive/SID | 23 | 14 |
|
| SD | 25 | 3 |
|
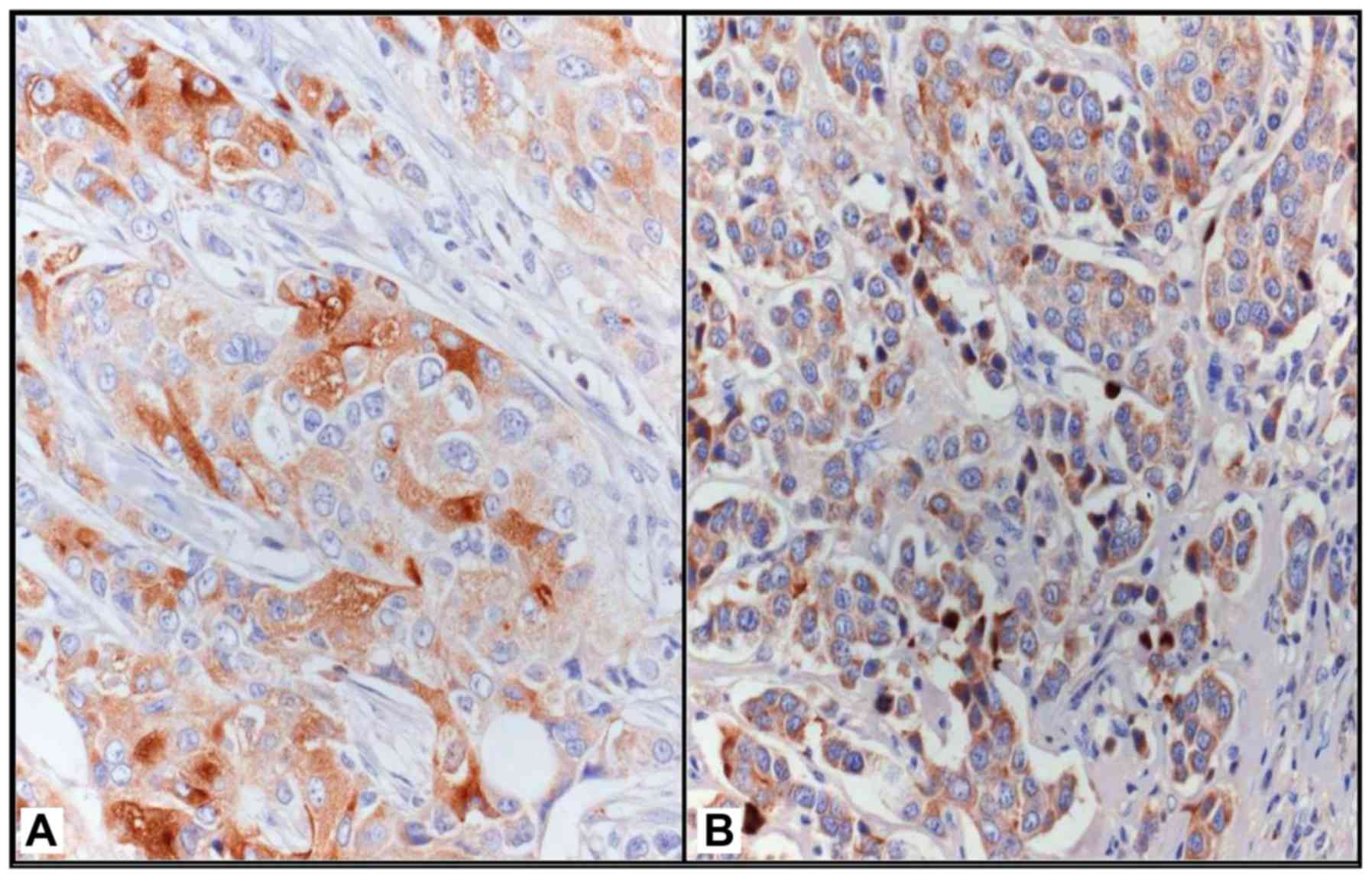
LF immunostaining was mainly localized in the
cytoplasm of neoplastic elements and occasionally in the nucleus of
the same cells; 17 cases (26.15%) exhibited an ID score of >2
and were therefore considered as positive for LF (Fig. 1). Statistical analyses showed that LF
positivity was significantly associated with a low Ki-67 LI
(<20%; P=0.040), the absence of recurrence (P=0.010) and alive
status (P=0.020).
Univariate analysis showed that a high pT stage
(P=0.040) and the absence of LF immunoexpression (P=0.030) were
significantly associated with shorter DFS times (Table II). Multivariate analysis for DFS
demonstrated that patient age, pT stage and Ki-67 LI were
independent variables (Table I).
| Table II.Associations between LF and
recurrence. |
Table II.
Associations between LF and
recurrence.
|
|
|
|
| Univariate | Multivariate |
|---|
|
|
|
|
|
|
|
|---|
| Variables | Patients, n | Disease
progression, n (%) | P-value | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Age, years |
|
| 0.460 |
| 0.120 |
| 0.02a |
|
≤70 | 33 | 15 (45) |
| 1.0 |
| 1.0 |
|
|
>70 | 32 | 18 (56) |
| 1.6 (0.8–3.8) |
| 2,3 (1.1–4.1) |
|
| pT |
|
| 0.250 |
| 0.040a |
| 0.001a |
| 1 | 36 | 15 (42) |
| 1.0 |
| 1.0 |
|
| 2 | 21 | 12 (57) |
| 1.3 (0.6–2.6) |
| 1.0 |
|
| 3 | 2 | 1 (50) |
| 1.6 (0.1–15.1) |
| 1.0 |
|
| 4 | 6 | 5 (83) |
| 3.8 (0.7–18.7) |
| 5.9 (1.9–17.9) |
|
| pN |
|
| 0.800 |
| 0.250 |
|
|
| N0 | 35 | 17 (49) |
| 1.0 |
|
|
|
| N+ | 30 | 16 (53) |
| 1.4 (0.7–2.7) |
| NSS |
|
| Histological
grade |
|
| 0.310 |
| 0.150 |
|
|
| 2 | 24 | 10 (42) |
| 1.0 |
|
|
|
| 3 | 41 | 23 (56) |
| 1.6 (0.8–3.8) |
| NSS |
|
| Ki-67 LI |
|
| 0.080 |
| 0.150 |
| 0.007a |
| Low
(≤20%) | 31 | 12 (39) |
| 1.0 |
| 0.3 (0.1–0.1) |
|
| High
(>20%) | 34 | 21 (62) |
| 1.6 (0.8–3.8) |
| 1.0 |
|
| LF expression |
|
| 0.010a |
| 0.030a |
|
|
|
Absent | 48 | 29 (60) |
| 2.9 (1.2–6.2) |
|
|
|
|
Present | 17 | 4 (24) |
| 1.0 | | NSS |
|
Univariate analysis for CSS showed that an age
>70 years (P=0.007) and a high pT stage (P=0.030) were
significant negative prognostic factors (Table III). The absence of LF
immunoexpression was not associated with shorter CSS times, since
statistical significance was not reached (P=0.060; Table III). At multivariate analysis,
patient age (P=0.004), pT stage (P=0.008) and Ki-67 LI (P=0.040)
emerged as independent variables (Table
III).
| Table III.Associations between LF and
survival. |
Table III.
Associations between LF and
survival.
|
|
|
|
| Univariate | Multivariate |
|---|
|
|
|
|
|
|
|
|---|
| Variables | Patients, n | Succumbed to
disease, n (%) | P-value | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Age, years |
|
| 0.120 |
| 0.007a |
| 0.004a |
|
≤70 | 33 | 10 (30) |
| 1.0 |
| 1.0 |
|
|
>70 | 32 | 18 (56) |
| 2.6 (1.2–5.2) |
| 3.3 (1.4–7.4) |
|
| pT |
|
| 0.070 |
| 0.030a |
| 0.008a |
| 1 | 36 | 11 (31) |
| 1.0 |
| 1.0 |
|
| 2 | 21 | 11 (52) |
| 1.7 (0.7–3.7) |
| 1.0 |
|
| 3 | 2 | 1 (50) |
| 2.1 (0.1–24.1) |
| 1.0 |
|
| 4 | 6 | 5 (83) |
| 4.3 (0.8–20.8) |
| 4.4 (1.4–13.4) |
|
| pN |
|
| 0.620 |
| 0.340 |
|
|
| N0 | 35 | 14 (40) |
| 1.0 |
|
|
|
| N+ | 30 | 14 (47) |
| 1.4 (0.6–3.6) |
|
|
|
| Histological
grade |
|
| 0.300 |
| 0.120 |
|
|
| 2 | 24 | 8 (33) |
| 1.0 |
|
|
|
| 3 | 41 | 20 (49) |
| 1.8 (0.8–3.8) |
|
|
|
| Ki-67 LI |
|
| 0.150 |
| 0.610 |
| 0.04a |
| Low
(≤20%) | 31 | 12 (39) |
| 1.0 |
| 0.3 (0.1–0.1) |
|
| High
(>20%) | 34 | 16 (47) |
| 1.2 (0.5–2.5) |
| 1.0 |
|
| LF expression |
|
| 0.020a |
| 0.060a |
|
|
|
Absent | 48 | 25 (52) |
| 2.9 (1.2–6.2) |
|
|
|
|
Present | 17 | 3 (18) |
| 1.0 |
|
|
|
Discussion
It is well known that lactating breast tissue, as
well as ductules and intralobular duct epithelial cells in normal
and dysplastic tissue, strongly stain for LF (25); consequently, LF has been considered a
potential marker for glandular or acinar differentiation, similar
to its use in other malignancies (9,18,22). However, in breast cancer, the
association between LF expression and clinical parameters is not
well defined (24), even if it has
been hypothesized that tumors with high LF expression retain a
certain degree of physiological control over cell growth, which may
explain a good prognosis (25).
In the present TNBC series, an LF immunostaining
rate (ID score) of >2 was found in ~26.15% of cases, and was
significantly associated with a low Ki-67 LI (<20%), the absence
of recurrence and an alive status. Therefore, given the aggressive
course of TNBC, the presence of LF-immunopositive cases may
identify a more indolent subtype of the disease with peculiar
clinical characteristics, including less aggressive biological
behavior and a more favorable prognosis; by contrast, shorter DFS
and CSS times were significantly associated with the absence of LF
immunoexpression.
However, a similar capability to select a TNBC
subgroup with low biological aggressiveness has been attributed to
androgen (AR) expression (6,7); in particular, AR has been shown to be a
favorable prognostic factor of DFS and overall survival, with
significantly decreased recurrence and mortality risks (6,7,32). Furthermore, in a series of 105 TNBC
patients with stage II or III disease treated with neoadjuvant
chemotherapy based on docetaxel and doxorubicin, the prognostic and
the predictive role of Ki-67 has been analyzed, identifying two
distinct subgroups of TNBC with different Ki-67 expression,
responses and prognoses (33). In the
present study, Ki-67 emerged as an independent variable for DFS and
CSS in TNBC, further highlighting its prognostic value. In
addition, TNBC LF-positive cases always expressed lower levels of
Ki-67, displaying a significant inverse association between Ki-67
LI and LF immunoreactivity, thus representing a further element to
assess a favorable group of TNBC characterized by a low risk of
recurrence and a better prognosis.
In conclusion, the results of the present study
appear to be notable with regard to the field of TNBC, although
further validation in large prospective studies is required to
enable LF to be a promising biomarker. In fact, together with
previous studies, the results of the present study show that the
first immunohistochemical application of LF in TNBC appears to
favor the selection of patients with a less aggressive behavior,
particularly in combination with Ki-67 status and AR expression.
However, additional investigations are also required with regard to
the potential of LF in cancer treatment, due to its nutraceutical
function and its ability to potentiate chemotherapy.
References
|
1
|
Prat A, Parker JS, Karginova O, Fan C,
Livasy C, Herschkowitz JI, He X and Perou CM: Phenotypic and
molecular characterization of the claudin-low intrinsic subtype of
breast cancer. Breast Cancer Res. 12:R682010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Perou CM: Molecular stratification of
triple-negative breast cancers. Oncologist. 16:(Suppl 1). S61–S70.
2011. View Article : Google Scholar
|
|
3
|
Lehmann BD, Bauer JA, Chen X, Sanders ME,
Chakravarthy AB, Shyr Y and Pietenpol JA: Identification of human
triple-negative breast cancer subtypes and preclinical models for
selection of targeted therapies. J Clin Invest. 121:2750–2767.
2011. View
Article : Google Scholar : PubMed/NCBI
|
|
4
|
Lehmann BD, Bauer JA, Schafer JM,
Pendleton CS, Tang L, Johnson KC, Chen X, Balko JM, Gómez H,
Arteaga CL, et al: PIK3CA mutations in androgen receptor-positive
triple negative breast cancer confer sensitivity to the combination
of PI3K and androgen receptor inhibitors. Breast Cancer Res.
16:4062014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kashiwagi S, Yashiro M, Takashima T,
Nomura S, Noda S, Kawajiri H, Ishikawa T, Wakasa K and Hirakawa K:
Significance of E-cadherin expression in triple-negative breast
cancer. Br J Cancer. 103:249–255. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ricciardi GR, Adamo B, Ieni A, Licata L,
Cardia R, Ferraro G, Franchina T, Tuccari G and Adamo V:
Correction: Androgen receptor (AR), E-Cadherin, and Ki-67 as
emerging targets and novel prognostic markers in triple-negative
breast cancer (TNBC) patients. PLoS One. 10:e01326472015.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Safarpour D and Tavassoli FA: A targetable
androgen receptor-positive breast cancer subtype hidden among the
triple-negative cancers. Arch Pathol Lab Med. 139:612–617. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Abd-Elazeem MA and Abd-Elazeem MA: Claudin
4 expression in triple-negative breast cancer: Correlation with
androgen receptors and Ki-67 expression. Ann Diagn Pathol.
19:37–42. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Caselitz J, Jaup T and Seifert G:
Lactoferrin and lysozyme in carcinomas of the parotid gland. A
comparative immunocytochemical study with the occurrence in normal
and inflamed tissue. Virchows Arch A Pathol Anat Histol. 394:61–73.
1981. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Tuccari G and Barresi G:
Immunohistochemical demonstration of lactoferrin in follicular
adenomas and thyroid carcinomas. Virchows Arch A Pathol Anat
Histopathol. 406:67–74. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Cabaret V, Vilain MO, Delobelle-Deroide A
and Vanseymortier L: Immunohistochemical demonstration of
ceruloplasmin and lactoferrin in a series of 59 thyroid tumors. Ann
Pathol. 12:347–352. 1992.(In French). PubMed/NCBI
|
|
12
|
Tuccari G, Giuffrè G, Crisafulli C and
Barresi G: Immuno-histochemical detection of lactoferrin in human
astrocytomas and multiforme glioblastomas. Eur J Histochem.
43:317–322. 1999.PubMed/NCBI
|
|
13
|
Zhou Y, Zeng Z, Zhang W, Xiong W, Wu M,
Tan Y, Yi W, Xiao L, Li X, Huang C, et al: Lactotransferrin: A
candidate tumor suppressor-Deficient expression in human
nasopharyngeal carcinoma and inhibition of NPC cell proliferation
by modulating the mitogen-activated protein kinase pathway. Int J
Cancer. 123:2065–2072. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Tuccari G, Barresi G, Arena F and
Inferrera C: Immuno-cytochemical detection of lactoferrin in human
gastric carcinomas and adenomas. Arch Pathol Lab Med. 113:912–915.
1989.PubMed/NCBI
|
|
15
|
Walmer DK, Padin CJ, Wrona MA, Healy BE,
Bentley RC, Tsao MS, Kohler MF, McLachlan JA and Gray KD: Malignant
transformation of the human endometrium is associated with
overexpression of lactoferrin messenger RNA and protein. Cancer
Res. 55:1168–1175. 1995.PubMed/NCBI
|
|
16
|
Farley J, Loup D, Nelson M, Mitchell A,
Esplund G, Macri C, Harrison C and Gray K: Neoplastic
transformation of the endocervix associated with downregulation of
lactoferrin expression. Mol Carcinog. 20:240–250. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Giuffrè G, Arena F, Scarfì R, Simone A,
Todaro P and Tuccari G: Lactoferrin immunoexpression in endometrial
carcinomas: Relationships with sex steroid hormone receptors (ER
and PR), proliferation indices (Ki-67 and AgNOR) and survival.
Oncol Rep. 16:257–263. 2006.PubMed/NCBI
|
|
18
|
Giuffrè G, Barresi V, Skliros C, Barresi G
and Tuccari G: Immunoexpression of lactoferrin in human sporadic
renal cell carcinomas. Oncol Rep. 17:1021–1026. 2007.PubMed/NCBI
|
|
19
|
Tuccari G, Giuffrè G, Scarfì R, Simone A,
Todaro P and Barresi G: Immunolocalization of lactoferrin in
surgically resected pigmented skin lesions. Eur J Histochem.
49:33–38. 2005. View
Article : Google Scholar : PubMed/NCBI
|
|
20
|
Ieni A, Barresi V, Grosso M, Rosa MA and
Tuccari G: Immuno-localization of lactoferrin in cartilage-forming
neoplasms. J Orthop Sci. 14:732–737. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ieni A, Barresi V, Grosso M, Rosa MA and
Tuccari G: Lactoferrin immuno-expression in human normal and
neoplastic bone tissue. J Bone Miner Metab. 27:364–371. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ieni A, Barresi V, Branca G, Giuffrè G,
Rosa MA and Tuccari G: Immunoexpression of lactoferrin in bone
metastases and corresponding primary carcinomas. Oncol Lett.
5:1536–1540. 2013.PubMed/NCBI
|
|
23
|
Charpin C, Lachard A, Pourreau-Schneider
N, Jacquemier J, Lavaut MN, Andonian C, Martin PM and Toga M:
Localization of lactoferrin and nonspecific cross-reacting antigen
in human breast carcinomas. An immunohistochemical study using the
avidin-biotinperoxidase complex method. Cancer. 55:2612–2617. 1985.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Ha NH, Nair VS, Reddy DN, Mudvari P,
Ohshiro K, Ghanta KS, Pakala SB, Li DQ, Costa L, Lipton A, et al:
Lactoferrin endothelin-1 axis contributes to the development and
invasiveness of triple-negative breast cancer phenotypes. Cancer
Res. 71:7259–7269. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Tuccari G and Barresi G: Lactoferrin in
human tumours: Immunohistochemical investigations during more than
25 years. Biometals. 24:775–784. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Penco S, Caligo MA, Cipollini G,
Bevilacqua G and Garré C: Lactoferrin expression in human breast
cancer. Cancer Biochem Biophys. 17:163–178. 1999.PubMed/NCBI
|
|
27
|
Benaïssa M, Peyrat JP, Hornez L, Mariller
C, Mazurier J and Pierce A: Expression and prognostic value of
lactoferrin mRNA isoforms in human breast cancer. Int J Cancer.
114:299–306. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Ieni A and Tuccari G: Comments on the
‘Prognostic impact and clinicopathological correlation of CD133 and
ALDH1 expression in invasive breast cancer’. J Breast Cancer.
19:96–98. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Ieni A, Barresi V, Branca G, Giuffrè G,
Rosa MA and Tuccari G: Immunohistochemical Investigation of
lactoferrin in human bone primary and metastatic tumours. Int J Lab
Med Res. 1:IJLMR-105.
|
|
30
|
Ieni A, Giuffrè G, Lanzafame S, Nuciforo
G, Curduman M, Villari L, Roz E, Certo G, Cabibi D, Salomone E, et
al: Morphological and biomolecular characteristics of
subcentimetric invasive breast carcinomas in Sicily: A multicentre
retrospective study in relation to trastuzumab treatment. Oncol
Lett. 3:141–146. 2012.PubMed/NCBI
|
|
31
|
Goldhirsch A, Winer EP, Coates AS, Gelber
RD, Piccart-Gebhart M, Thürlimann B and Senn HJ: Panel members:
Personalizing the treatment of women with early breast cancer:
Highlights of the St Gallen international expert consensus on the
primary therapy of early breast cancer 2013. Ann Oncol.
24:2206–2223. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Ieni A, Barresi V, Ricciardi GR, Adamo B,
Adamo V and Tuccari G: Prognostic value of androgen receptor
expression in triple negative breast carcinomas: Personal
experience and comments on a review about ‘Triple-negative breast
cancer: Treatment challenges and solutions’ by Collignon et
al. Breast Cancer (Dove Med Press). 8:157–159. 2016.PubMed/NCBI
|
|
33
|
Rakha EA, El-Sayed ME, Green AR, Lee AH,
Robertson JF and Ellis IO: Prognostic markers in triple-negative
breast cancer. Cancer. 109:25–32. 2007. View Article : Google Scholar : PubMed/NCBI
|