Introduction
It has been reported that undifferentiated embryonal
sarcoma of the liver (UESL) occurs in children aged between six and
15 years (1,2), however, some adult cases have also
been reported (3). The occurrence
of UESL in patients aged ≥45 years is extremely rare, with only 27
reported cases in the English language literature up to 2012.
Patients commonly complain of idiopathic upper abdominal pain,
lasting for >10 days (4). The
genetic aberrations of undifferentiated embryonal sarcoma (UES) are
not completely understood and the misdiagnosis rate of UES is high.
The most effective therapy is surgery, however, the prognosis of
UES is poor. Complete surgical resection and adjuvant chemotherapy
may benefit patients with UESL (5).
Currently, primary hepatic carcinoma, which was
first reported by Stocker and Ishak in 1978 (2), is a common disease in the hepatopathy
domain, but undifferentiated embryonal sarcoma of liver is an
infrequent type of tumor with a high malignancy and peak incidence
in late childhood. From 1978 to the present, there have only been
~150 cases reported (6).
The current case presents a 39-year-old male who was
diagnosed with UESL, and the features surrounding the UESL and all
the outcomes of this case are discussed.
Case report
The patient was a 39-year-old male with an uncertain
cause of fever and upper abdominal pain. The highest recorded
temperature was 39°C and this did not return to normal on its own
accord, and the upper abdominal pain was constant. The patient was
previously in good health and there was no hepatitis or any
particular pathography in the family and personal history. The
patient was being treated at another hospital, but the treatment
did not improve the symptoms and it was decided that the patient be
transferred to the Guangzhou General Hospital of Guangzhou Military
Command (Guangzhou, China) for further medical treatment.
On admission, the body temperature of the patient
was 38.5°C, the pulse rate was 80 beats/min and the blood pressure
was 120/78 mmHg. The patient experienced a little pain when
pressure was applied to the hepatic region. There was no evidence
of an underlying liver disease upon serological examination, and
tumor markers, including carcinoembryonic antigen (CEA) and
carbohydrate antigen (CA-199), were negative, with the exception of
α-feto protein (AFP) which was present at 13.14 μg/l (range, 0–7
μg/l). Serology was also negative for hepatitis A, B, C and E,
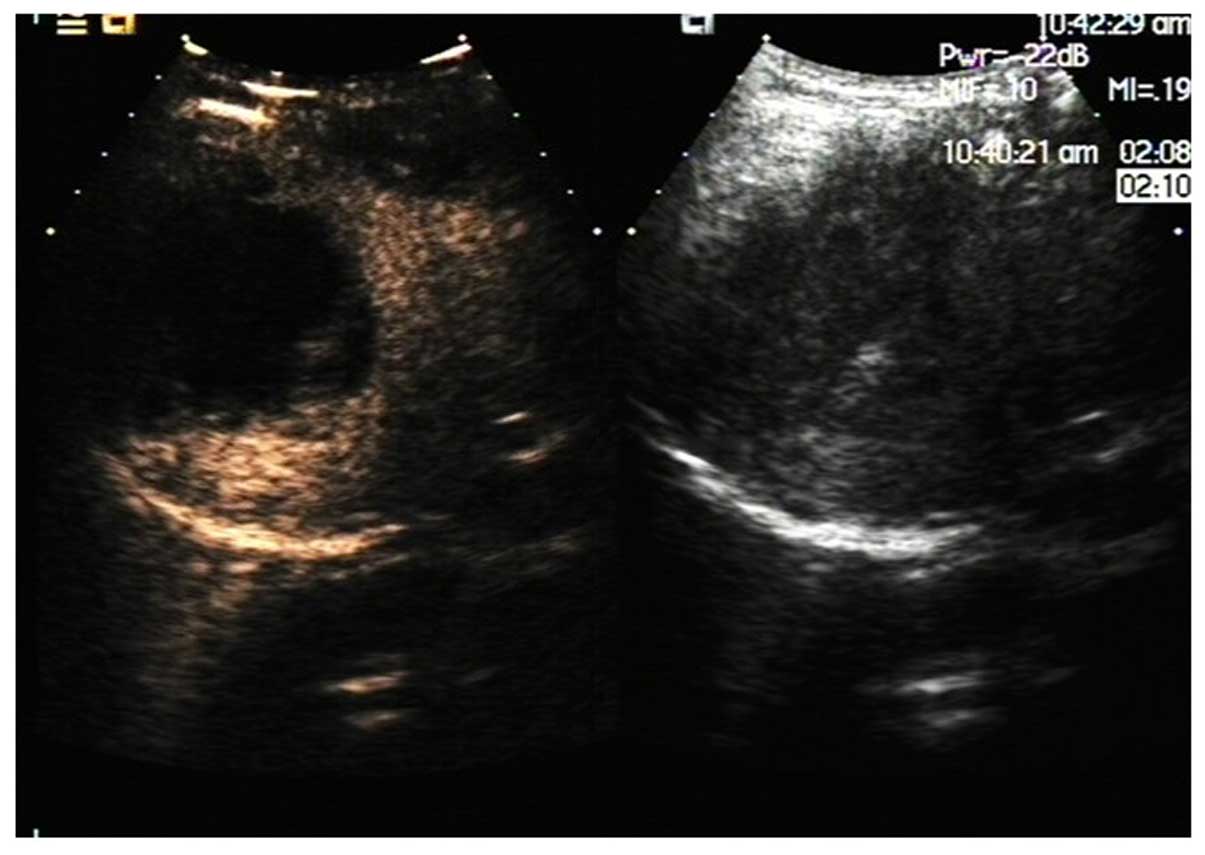
syphilis and human immunodeficiency virus. The abdominal
contrast-enhanced ultrasound revealed the presence of a cystic mass
(90×67 mm) in the right hepatic region with homogeneous enhancement
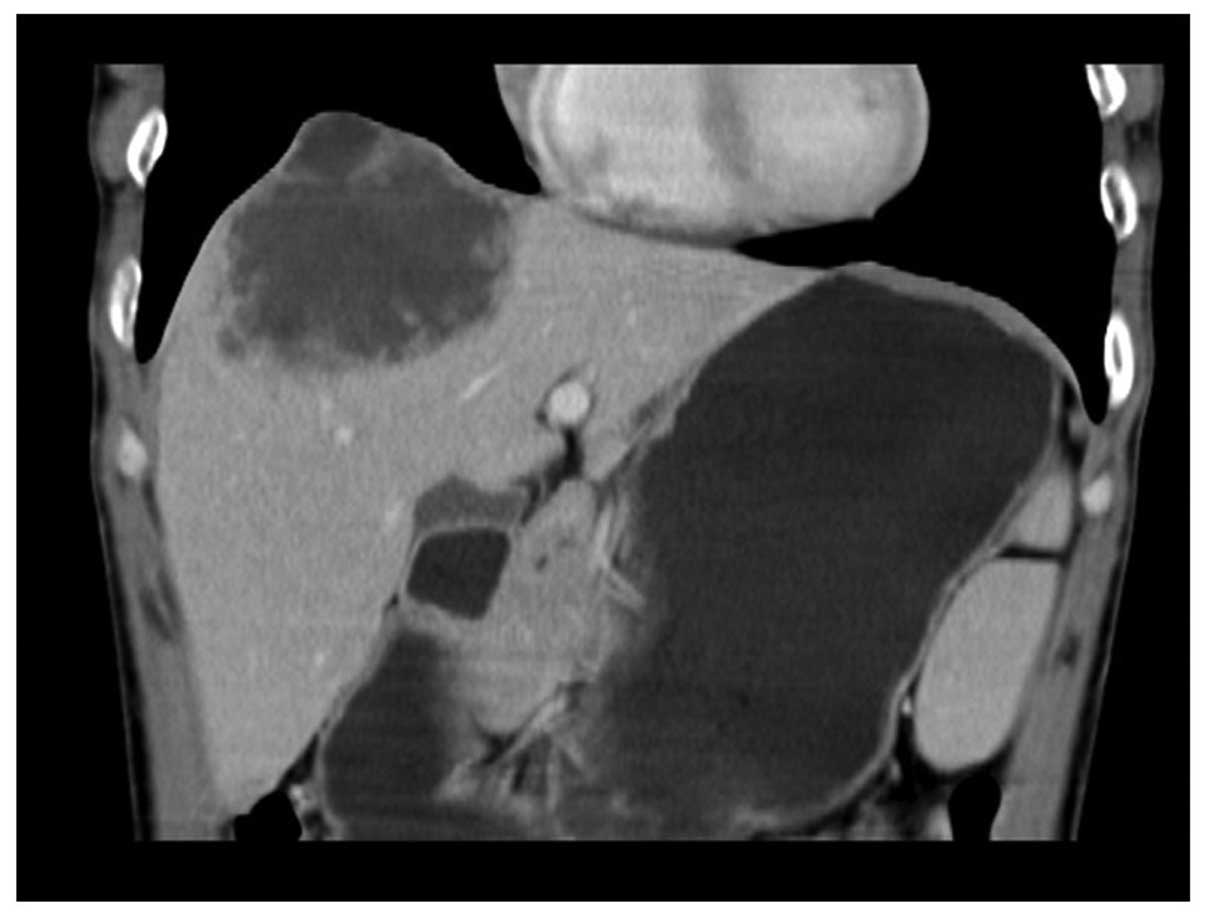
(Fig. 1). The abdominal computed
tomography (CT) scan showed a UESL of 90 mm in maximum diameter, as
well as cystic lesions with a low density that was reflected as a
fluid (Fig. 2). Therefore, the
initial diagnosis was a hepatic abscess and anti-infective therapy
(0.6 g levofloxacin intraveneously once a day and 0.5g ornidazole
intraveneously twice a day, both by intradermal injection) was
administered. There was no improvement following 10 days of
treatment and, therefore, the patient underwent ultrasound-guided
liver puncture drainage. An 18-gauge puncture needle was used and
the drainage tube was placed into the abscess cavity during the
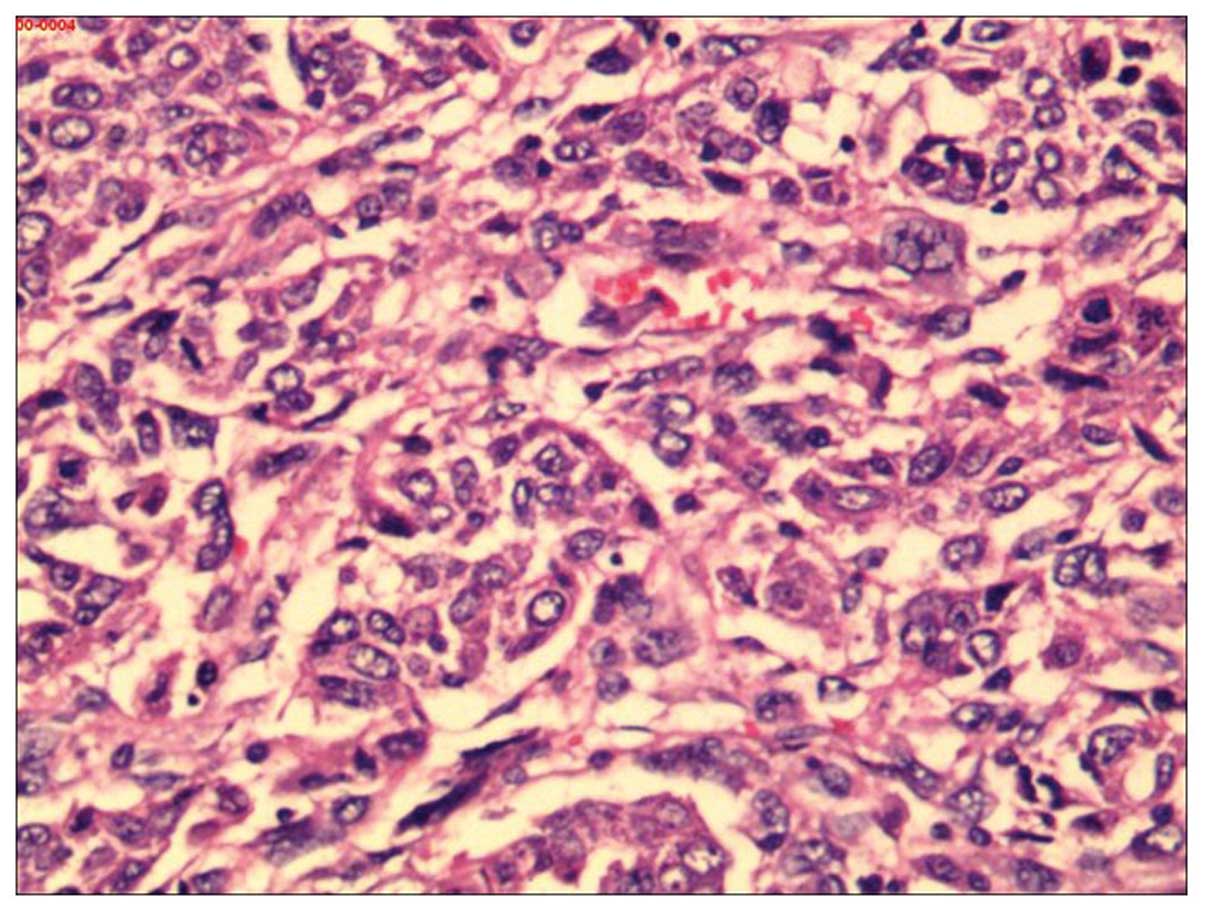
procedure, but it failed to drain the pus. The histopathological
analysis of the liver tissue obtained by biopsy revealed atypical,
multi-nucleated giant cells and abnormal cells (Fig. 3). By immunohistochemistry, the tumor
cells were positive for vimentin and α-1-antichymotrypsin; negative
for cytokeratin 7 (CK7), CK19, CK8/18, hepatocyte paraffin,
mucin-1, cluster of differentiation 31 (CD31), CD34 and AFP; and
the positive rate of Ki67 was 80%. Therefore, a diagnosis of UESL
was determined and the patient underwent liver tumor resection and
diaphragmatic tumor excision surgeries. During the surgery, the
liver showed moderate-diffuse nodular sclerosis and the right lobe
of the tumor diaphragmatic adhesions could not be separated. The
tumor ulceration is normally removed and violation of the diaphragm
is also taken into consideration (Fig.
4). The patient returned to our hospital to receive regular CT
examinations and, after 2 months, it was found that the tumor had
recurred, as shown by the CT imaging. The patient did not accept
the option of postoperative chemotherapy due to economic problems
and poor knowledge of the tumor.
Discussion
UESL is a type of rare malignant mesenchymal tumor
that has the characteristics of a low incidence rate, a high degree
of malignancy, high mortality and poor prognosis. In recent years,
few studies have been published on UESL in the literature and the
pathogenesis of UESL remains unknown. Certain studies report that
gene mutations may be associated with the occurrence of UESL, but
studies have shown no clear correlation between the disease and
hepatitis virus infection (7–9). The
present case was without hepatitis virus infection and is
concordant with the previous studies.
UESL commonly occurs in the right hepatic lobe, but
occurrence in the left and double lobe have been found and reported
in the literature (10). The
incidence of this disease has no significant difference between
genders (11–13), but certain studies have indicated
that the occurrence in males is slightly more common compared with
that in females (14–16). In the present case, the UESL was
located in the right lobe of the liver in a male. The patient may
develop a fever, abdominal pain, weight loss and other non-specific
symptoms, as UESL has a lack of characteristic clinical
manifestations. Additionally, the disease has a lack of associated
serological examination standards and medical imaging
characteristics. Therefore, a definite clinical diagnosis is
difficult (17). The predominant
symptoms of the present case were fever and abdominal pain, and the
serum liver function biomarkers, CEA and CA199, were normal. Only
AFP was mildly elevated and there was no other clinical specificity
identified.
A review of the associated literature has identified
that UESL can be misdiagnosed as a hepatic cyst due to CT
examination of a large number of UESL cases showing cystic changes,
so the misdiagnosis rate is as high as 23.5%, clinically (18,19).
By contrast, specific studies have indicated that the results of
examination by ultrasound and CT imaging of UESL were conflicting,
as the light group in ultrasound showed irregular hyperechoic,
hypoechoic or mixed, but the CT has shown low-density cystic
changes. Therefore, there is a certain belief that if there were
variations of ultrasound and CT imaging in liver lesions, then it
is necessary to take UESL into consideration. The CT imaging in the
present case was similar to the early CT imaging of the
hepatapostema, according to a slightly hypodense shadow, a clear
edge, uneven density, no obvious parenchymatous lesion and the
separate, enhanced disjunctive enhancement. There was an equi-echo
display in the light echo of the liver ultrasonic images. Thus, the
clinical misdiagnosis occurred. Pathological morphology and
immunohistology are the most significant methods for the diagnosis
of UESL and the clinical treatment effect is unsatisfactory. The
liver biopsy was taken by percutaneous transhepatic cholangiography
(PTC) following the failure of the liver-puncture drainage.
UESL is a type of tumor with a high degree of
malignancy, fast clinical progression and unfavorable prognosis.
Surgical excision is a significant way to treat UESL early. Faraj
et al (11) indicated that
the average survival rate of patients who had accepted chemotherapy
or radiation therapy following surgery was higher compared with
simple surgical cases. At present, there are only four child case
studies on the treatment of the UESL by orthotropic liver
transplantation; however, for adult treatment of UESL, using liver
transplantation has been considered controversial (12,13).
Only surgical treatment was performed in the present case without
any further postoperative treatment, and it was indicated that
tumor recurrence had occurred 2 months later by a hospital review
of the CT imaging. It has been revealed that UESL is a type of
infrequent liver disease with characteristics that include rapid
progression and an unfavorable prognosis. For patients with liver
lesions and a fever of an undetermined origin, extracting a biopsy
by PTC and performing pathological morphology and immunohistology
testing early is necessary.
References
|
1
|
Lenze F, Birkfellner T, Lenz P, et al:
Undifferentiated embryonal sarcoma of the liver in adults. Cancer.
112:2274–2282. 2008.
|
|
2
|
Stocker JT and Ishak KG: Undifferentiated
(embryonal) sarcoma of the liver: report of 31 cases. Cancer.
42:336–348. 1978.
|
|
3
|
Nishio J, Iwasaki H, Sakashita N, et al:
Undifferentiated (embryonal) sarcoma of the liver in middle-aged
adults: smooth muscle differentiation determined by
immunohistochemistry and electron microscopy. Hum Pathol.
34:246–252. 2003.
|
|
4
|
Jia C, Zhao W, Dai C, et al:
Undifferentiated embryonal sarcoma of the liver in a middle-aged
adult with systemic lupus erythematosus. World J Surg Oncol.
11:2442013.
|
|
5
|
Lyu S, Shi X, Liang Y, et al: Diagnosis
and therapy of primary undifferentiated embryonal sarcoma of the
liver. Chin Med J (Engl). 127:1585–1587. 2014.
|
|
6
|
Kim M, Tireno B and Slanetz P:
Undifferentiated embryonal sarcoma of the liver. Am J Roentgenol.
190:W261–W262. 2008.
|
|
7
|
Li XW, Gong SJ, Song WH, et al:
Undifferentiated liver embryonal sarcoma in adults: a report of
four cases and literature review. World J Gastroenterol.
16:4725–4732. 2010.
|
|
8
|
Stocker JT and Ishak KG: Undifferentiated
(embryonal) sarcoma of the liver: report of 31 cases. Cancer.
42:336–348. 1978.
|
|
9
|
Lack EE, Schloo BL, Azumi N, et al:
Undifferentiated (embryonal) sarcoma of the liver. Clinical and
pathologic study of 16 cases with emphasis on immunohistochemical
features. Am J Surg Pathol. 15:1–16. 1991.
|
|
10
|
Vick DJ, Goodman ZD, Deavers MT, et al:
Ciliated hepatic foregut cyst: a study of six cases and review of
the literature. Am J Surg Pathol. 23:671–677. 1999.
|
|
11
|
Faraj W, Mukherji D, El Majzoub N, et al:
Primary undifferentiated embryonal sarcoma of the liver mistaken
for hydatid disease. World J Surg Oncol. 8:582010.
|
|
12
|
Kelly MJ, Martin L, Alonso M and Altura
RA: Liver transplant for relapsed undifferentiated embryonal
sarcoma in a young child. J Pediatr Surg. 44:e1–e3. 2009.
|
|
13
|
Dower NA, Smith LJ, Lees G, et al:
Experience with aggressive therapy in three children with
unresectable malignant liver tumors. Med Pediatr Oncol. 34:132–135.
2000.
|
|
14
|
Li XW, Gong SJ, Song WH, et al:
Undifferentiated liver embryonal sarcoma in adults: a report of
four cases and literature review. World J Gastroenterol.
16:4725–4732. 2010.
|
|
15
|
Dai CL, Xu F, Shu H, et al:
Undifferentiated (embryonal) sarcoma of liver in adult: a case
report. World J Gastroenterol. 11:926–929. 2005.
|
|
16
|
Yang L, Chen LB, Xiao J and Han P:
Clinical features and spiral computed tomography analysis of
undifferentiated embryonic liver sarcoma in adults. J Dig Dis.
10:305–309. 2009.
|
|
17
|
Kalra N, Vyas S, Jyoti Das P, et al:
Undifferentiated embryonal sarcoma of liver in an adult
masquerading as complicated hydatid cyst. Ann Hepatol. 10:81–83.
2011.
|
|
18
|
Charfi S, Ayadi L, Toumi N, et al: Cystic
undifferentiated sarcoma of liver in children: a pitfall diagnosis
in endemic hydatidosis areas. J Pediatr Surg. 43:E1–E4. 2008.
|
|
19
|
Aggarwal S, Guleria S, Dinda AK, et al:
Embryonal sarcoma of the liver mimicking a hydatid cyst in an
adult. Trop Gastroenterol. 22:141–142. 2001.
|