Introduction
Invasive micropapillary carcinoma (IMPC) of the
breast is a morphologically distinct and aggressive variant of
invasive ductal carcinoma (IDC), accounting for <2% of all
invasive breast cancer cases (1).
Morphologically, IMPC exhibits a peculiar architecture
characterised by pseudopapillary structures that are composed of
cell clusters with inverted polarity floating in empty spaces and
lined by delicate strands of fibrous stroma (2). IMPC was first described in the
literature by Petersen in 1993 (3).
In the 2003 World Health Organisation (WHO) classification of
breast tumours (4), IMPC was listed
as a subtype of invasive carcinoma (1). However, in the literature, no
consensus has been reached regarding the amount of IMPC tissue in
the breast carcinoma required to make a diagnosis and determine the
type of IMPC (5). IMPC is
associated with a high incidence of axillary lymph node metastases
and local recurrence and poor clinical outcome (6). These clinical characteristics indicate
the significance of IMPC being recognised by surgeons and
pathologists. Therefore, the clinical and immunohistochemical
characteristics of IMPC were retrospectively examined.
Materials and methods
Patient selection
In total, the records of 25 patients diagnosed with
IMPC were retrieved from the histopathological medical records from
the Department of Pathology of Liaocheng People’s Hospital of
Shangdong Province (Liaocheng, China). These patients presented
over a six-year period, between July 2005 and July 2011. The
present study was conducted in accordance with the Declaration of
Helsinki and with approval from the Ethics Committee of Liaocheng
People’s Hospital. Written informed consent was obtained from all
participants.
Immunohistochemical staining
Haematoxylin and eosin were used to stain 10% of
formalin-fixed, paraffin-embedded 4-μm tissue sections.
Immunohistochemical studies on oestrogen receptor (ER),
progesterone receptor (PR), c-erbB-2 and epithelial membrane
antigen (EMA) were conducted. The slides were incubated overnight
at 55°C to enhance the adhesion of the sections to the slides.
Deparaffinisation in xylene and graded alcohol followed. Prediluted
monoclonal rabbit anti-human ER (1:240), monoclonal rabbit
anti-human PR (1:240), polyclonal rabbit anti-human c-erbB-2
(1:400) and monoclonal EMA (1:400) antibodies were obtained from
the Maixin Biotechnology Development Co., Ltd. (Fuzhou, Fujian,
China). The primary antibodies were applied for 60 min at room
temperature, then the slides were washed with phosphate-buffered
saline (PBS) three times for 5 min each. Next, the secondary mouse
anti-rabbit monoclonal secondary antibodies (RMA-0501, RMA-0502,
RMA-0156 and KIT-0011; Maixin Biotechnology Development Co., Ltd.)
was added and the slides were washed three times with PBS for 3 min
each. 3,3′-diaminobenzidine (Maixin Biotechnology Development Co.,
Ltd.) was then added and the slides were visualized under a
microscope (Eclipse 80i; Nikon Corporation, Tokyo, Japan).
Immunohistochemical evaluation
Using light microscopy, stained tissue sections were
reviewed by two pathologists blind to the diagnosis. All unclear
cases were discussed with an additional pathologist.
Morphologically, IMPC exhibited a peculiar architecture
characterised by pseudopapillary structures that were composed of
cell clusters with inverted polarity and floating in empty spaces
and lined by delicate strands of fibrous stroma. The cases were
fully characterised on the basis of morphological features
described in the original articles on IMPC by Tavassoli and Devilee
(1) and Fisher et al
(7). Histological grading was
performed using the modified Bloom-Richardson grading system.
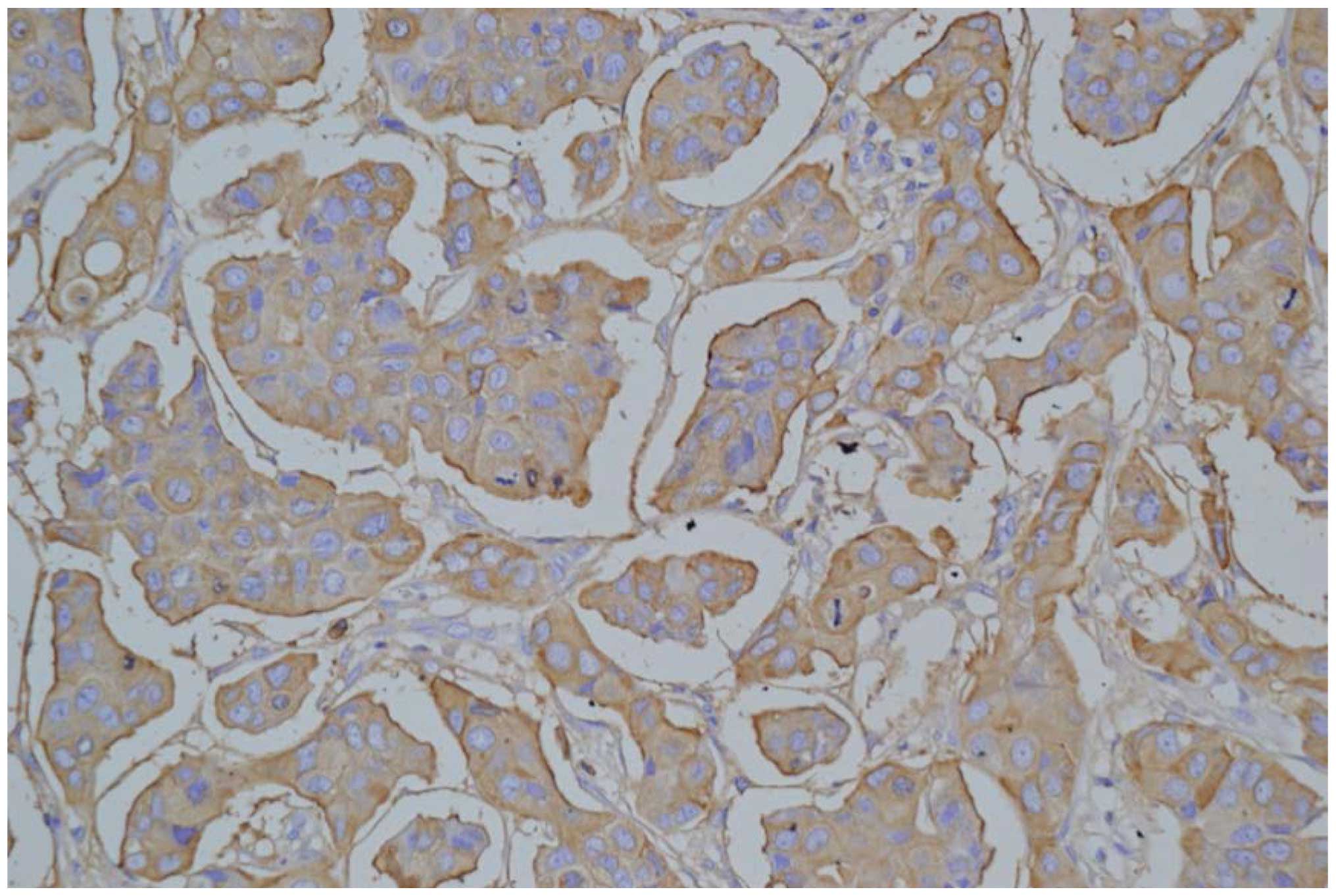
Immunohistochemical studies were carried out to determine the
characteristic pattern of EMA expression in IMPC to support the
diagnosis. ER and PR receptor status tests were performed
routinely, and the HER-2/neu status was determined by
immunohistochemistry (IHC), with or without fluorescence in
situ hybridisation (FISH), when requested by the clinician. The
evaluation of the ER, PR and HER-2 statuses was conducted in
accordance with the US guidelines (8).
Results
Clinical data
All the 25 patients were female. The mean age of the
patients was 52.3 years and the age range was 34–79 years. The
initial manifestation of carcinoma was a palpable mass in 21
patients (84%), a palpable mass with nipple discharge in two
patients (8%) and a screening mammographic abnormality in two
patients (8%). The breast cancer lesion was located in the left
breast in 14 patients (56%) and in the right breast in 11 patients
(44%). All the patients underwent mammography. Masses were noted in
23 patients (92%), microcalcifications were observed in 15 patients
(60%) and microcalcifications without mass or asymmetry were
observed in two patients (8%). The masses were found to be
irregular in shape with a high density and a non-circumscribed
margin, with the latter two patients exhibiting fine pleomorphic
microcalcifications. Ultrasound scanning (US) was performed in all
25 cases. The masses exhibited an irregular shape with a speculated
margin in 23 patients (92%), a hypoechoic pattern in 21 patients
(84%) and posterior acoustic shadowing in 17 patients (68%). On the
basis of the Breast Imaging-Reporting and Data System final
assessment (9), 23 patients (92%)
were classified as category 5 and two cases were classified as
category 4 (8%). The axillary lymph nodes in all 25 patients were
also examined, with 13 patients (52%) suspected to possess lymph
node metastasis. All 13 patients were confirmed to possess lymph
node metastasis upon pathological examination.
Pathological results
Seven patients that were negative for metastasis on
the US of the axillary lymph node were found to possess metastatic
lymph nodes upon pathological examination. Fine-needle aspiration
cytology of the breast was sought in eight of the cases and six of
these patients were diagnosed as carcinoma. Core-needle biopsy was
also performed in 18 patients, 16 of which were diagnosed with
carcinoma and five of these 16 cases were diagnosed with IMPC. In
total, 25 patients underwent modified radical mastectomy and two
patients underwent a lumpectomy. Of the 25 surgical specimens,
lymphovascular invasion was found in 11 (44%) patients, and
axillary lymph node metastases were identified in 20 (80%) cases.
The mean number of metastatic axillary lymph nodes was 5.7 (range,
3–21).
Immunohistochemical evaluation
Immunohistochemical analyses were carried out in all
25 cases. The findings revealed the expression of ER in 88% of the
cases (22/25) and PR in 64% of the cases (16/25). In terms of
c-erbB-2, an IHC score of 0 was demonstrated in one case (4%), 1+
in two cases (8%), 2+ in six cases (24%) and 3+ in 16 cases (64%).
Five out of the six cases with a score of 2+ were revealed by FISH
to possess gene amplification. Therefore, overexpression of the
c-erbB-2 protein was observed in 84% of the cases (21/25).
Immunohistochemical studies were carried out in all cases to
determine the characteristic pattern of EMA expression to support
the diagnosis of IMPC (Fig. 1).
Follow-up
Follow-up information was available for all 25
patients. The mean follow-up period was 36.5 months (range, 1–55
months). Recurrence was noted in three patients, with one
recurrence in the contralateral breast tissues and two in the liver
and lung. Of the latter two patients, one succumbed to the disease
after seven months and the other succumbed after 29 months.
Discussion
IMPC is an uncommon, clinically aggressive variant
of IDC (10) that accounts for
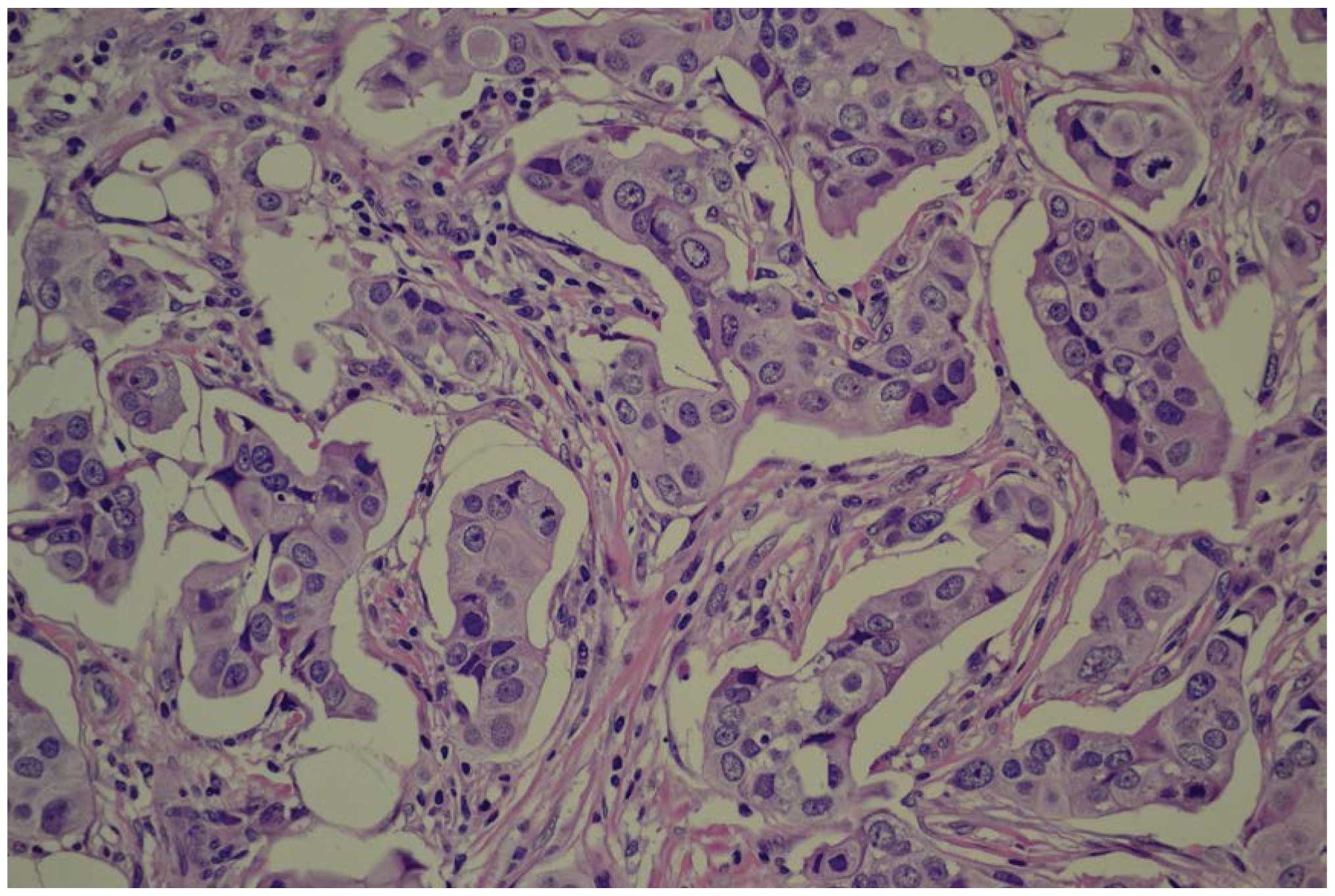
0.7–3% of all cases of breast cancer. Morphologically, IMPC
exhibits a peculiar architecture characterised by pseudopapillary
structures that consist of cell clusters with inverted polarity
floating in empty spaces and lined by delicate fibrous stroma
strands (Fig. 2) (2). The 2003 WHO classification of breast
tumours listed IMPC as a subtype of invasive carcinoma. However,
there was no percentage of the IMPC component within the tumour
that was proposed as a criterion for diagnosis (1). Certain experts hypothesise that the
size of the IMPC structure should be >5 mm (11,12).
Other studies support that the percentage of the IMPC should be
>75%. The literature has not reached a consensus regarding the
amount of IMPC necessary for a diagnosis and determining the type
of IMPC (13). Despite only a few
studies on IMPC imaging findings being conducted, it has been
previously reported that mammography may reveal IMPC as an
irregular, speculated or indistinct high-density mass and that US
may reveal IMPC as an irregular, indistinct or hypoechoic mass
(14). In the present study, masses
were also the most frequent mammographic finding. The masses were
characterised by an irregular shape and speculated margin in 23
patients (92%) and a hypoechoic pattern in 21 patients (84%). The
present results agree with those of a previous study, in which
microcalcifications were reported in 43–68% of cases (15). In the present study,
microcalcifications were identified in 60% (15/25) of the patients.
Tumours with any amount of this unique histological pattern,
regardless of the extent of the micropapillary component, exhibit a
more aggressive clinical behaviour and possess a poorer prognosis,
with a high degree of lymph node involvement (16). An invasive micropapillary pattern
has been described in tumours in several organs, including the
ovaries, salivary glands, colon, bladder and lungs. A clinical
finding is always associated with a poor prognosis and a high
incidence of lymph node metastasis (17). The mechanisms that result in the
development of metastatses are variable and require several steps,
including loss of contact with neighbouring cells, penetration of
vessel walls, adhesion at the novel localisation and angiogenesis.
Although numerous studies have attempted to explain the peculiar
features of these tumours, the basis of their biological behaviour
remains unclear and additional efforts have to be made to improve
the understanding of this rare variant of carcinoma. Previous
studies have identified that heat shock protein 27 and L1 cell
adhesion molecules play an important role in the formation of the
specific pathological morphology of IMPC and in the high rate of
lymph node metastasis (18,19). Cluster of differentiation (CD)24 has
gained much attention due to its important role in the development
of cancer metastases and as a marker of malignancy in several
tumour types (20). One study has
demonstrated that IMPC may represent a distinct entity of breast
carcinoma that exhibits a high expression of CD24 compared with
IDC. This finding may explain the high lymph-vascular invasion
propensity and high metastatic capability of these tumours and may
be a useful tool as a future target of therapy (21). In the present study, 80% (20/25) of
the patients were confirmed to possess lymph node metastasis upon
pathological examination. Lymphovascular invasion was found in 11
patients (44%).
Although an ER- and PR-positive status is generally
associated with an improved differentiation of tumours and an
improved outcome (15), IMPC
appears to be an exception. This tumour type is characterised by
higher rates of ER and PR expression compared with other types
(22). Zekioglu et al
(16) reported that 68 and 61% of
lesions were positive for ER and PR, respectively, in IMPC. These
results are higher compared with those of common breast cancers.
The reported prevalence of c-erbB-2 was slightly higher than that
of IDCs. Walsh and Bleiweiss (23)
reported high percentages of ER and PR positivity (90 and 70%,
respectively) and nearly double the expected percentage of c-erbB-2
positivity (60%). The present study revealed ER expression in 88%
of the cases (22/25) and PR expression in 64% of the cases (16/25).
In terms of c-erbB-2, an IHC score of 0 was revealed in one case
(4%), 1+ in two cases (8%), 2+ in six cases (24%) and 3+ in 16
cases (64%). Five out of the six cases that scored 2+ were revealed
to possess gene amplification by FISH. Overexpression of the
c-erbB-2 protein was observed in 84% of the cases (21/25).
The preferred treatment for IMPC is mastectomy and
axillary clearance, with the addition of adjuvant chemotherapy for
the treatment of patients with lymph node metastasis or a tumour
size of >1 cm (24). A study
that reported 72 cases of IMPC (11) revealed that IMPC is more frequently
associated with lymphovascular invasion, extracapsular extension
from the lymph node, a high nuclear grade and an increased degree
of locoregional recurrence, particularly in the axilla and
supraclavicular regions. Therefore, axillary and supraclavicular
radiation therapy should be considered as a treatment for IMPC
patients that possess axillary node metastasis.
In summary, the imaging findings of IMPC through
mammography and US strongly suggested malignancy. There was no
identification of features that distinguish IMPC from typical IDC,
but the presence of frequent nodal metastases and a high positive
result subsequent to ER, PR and c-erbB-2 testing was identified in
IMPC. These characteristics could aid in the treatment and
evaluation of the prognosis of patients with IMPC.
References
|
1
|
Ellis IO, Schnitt SJ, Sastre-Garau X, et
al: Invasive micropapillary carcinoma. Pathology and Genetics of
Tumors of the Breast and Female Genital Organs (IARC WHO
Classification of Tumours). Tavassoli FA and Devilee P: IARC Press;
Lyon: pp. 35–36. 2003
|
|
2
|
Pettinato G, Manivel CJ, Panico L, Sparano
L and Petrella G: Invasive micropapillary carcinoma of the breast:
clinicopathologic study of 62 cases of a poorly recognized variant
with highly aggressive behavior. Am J Clin Pathol. 121:857–866.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Petersen JL: Breast carcinomas with an
unexpected inside-out growth pattern: rotation of polarization
associated with angioinvasion. Pathol Res Pract. 189:A7801993.
|
|
4
|
Tavassoli FA and Devilee P: World Health
Organization Classification of Tumors. Pathology and Genetics of
Tumors of the Breast and Female Genital Organs. IARC Press; Lyon:
2003
|
|
5
|
Siriaunkgul S and Tavassoli FA: Invasive
micropapillary carcinoma of the breast. Mod Patho. 6:660–662.
1993.
|
|
6
|
Yun SU, Choi BB, Shu KS, et al: Imaging
findings of invasive micropapillary carcinoma of the breast. J
Breast Cancer. 15:57–64. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Fisher ER, Palekar AS, Redmond C, Barton B
and Fisher B: Pathologic findings from the National Surgical
Adjuvant Breast Project (protocol no. 4) VI Invasive papillary
cancer. Am J Clin Pathol. 73:313–322. 1980.PubMed/NCBI
|
|
8
|
Hammond ME, Hayes DF, Wolff AG, Mangu PB
and Temin S: American society of clinical oncology/college of
American pathologists guideline recommendations for
immunohistochemical testing of estrogen and progesterone receptors
in breast cancer. J Oncol Pract. 6:195–197. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
American College of Radiology. BI-RADS:
Ultrasound. Breast Imaging Reporting and Data System (BI-RADS
atlas). 4th edition. American College of Radiology; Reston, VA: pp.
196–198. 2003
|
|
10
|
Ide Y, Horii R, Osako T, et al:
Clinicopathological significance of invasive micropapillary
carcinoma component in invasive breast carcinoma. Pathol Int.
61:731–736. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Chen L, Fan Y, Lang RG, et al: Breast
carcinoma with micropapillary features: clinicopathological study
and long-term follow-up of 100 cases. Int J Surg Pathol.
16:155–163. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Yu JI, Choi DH, Park W, et al: Differences
in prognostic factors and patterns of failure between invasive
micropapillary carcinoma and invasive ductal carcinoma of the
breast: matched case-control study. Breast. 19:231–237. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Guo X, Chen L, Lang R, et al: Invasive
micropapillary carcinoma of the breast: association of pathologic
features with lymph node metastasis. Am J Clin Pathol. 126:740–746.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Adrada B, Arribas E, Gilcrease M and Yang
WT: Invasive micropapillary carcinoma of the breast: mammographic,
sonographic, and MRI features. AJR Am J Roentgenol. 193:W58–W63.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kim DS, Cho N, Ko ES, et al: Imaging and
the clinical-pathologic features of invasive miropapillary
carcinoma of the breast. J Korean Radio Soc. 56:497–503. 2007.
|
|
16
|
Zekioglu O, Erhan Y, Ciris M, Bayramoglu H
and Ozdemir N: Invasive micropapillary carcinoma of the breast:
high incidence of lymph node metastasis with extranodal extension
and its immunohistochemical profile compared with invasive ductal
carcinoma. Histopathology. 44:18–23. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Li YS, Kaneko M, Sakamoto DG, Takeshima Y
and Inai K: The reversed apical pattern of MUC1 expression is
characteristics of invasive micropapillary carcinoma of the breast.
Breast Cancer. 13:58–63. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Gao X, Qian XL, Li YQ, Ren MJ and Fu L:
Expression and significance of Hsp27 in invasive micropapillary
carcinoma of the breast. Chin J Clin Oncol. 40:525–528. 2013.
|
|
19
|
Zhang C, Fan Y, Li WD, et al: Expression
and significance of L1-CAM in invasive micropapillary carcinoma of
the breast. Chin J Clin Oncol. 40:198–201. 2013.
|
|
20
|
Kristiansen G, Sammar M and Altevogt P:
Tumour biological aspects of CD24, a mucin-like adhesion molecule.
J Mol Histol. 35:255–262. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Simonetti S, Terracciano L, Zlobec I, et
al: Immunophenotyping analysis in invasive micropapillary carcinoma
of the breast: role of CD24 and CD44 isoforms expression. Breast.
21:165–170. 2012. View Article : Google Scholar
|
|
22
|
Tressrra F, Grases PJ, Fábregas R,
Férnandez-Cid A and Dexeus S: Invasive micropapillary carcinoma.
Distinct features of a poorly recognized variant of breast
carcinoma. Eur J Gynaecol Oncol. 20:205–208. 1999.
|
|
23
|
Walsh MM and Bleiweiss IJ: Invasive
micropapillary carcinoma of the breast: eighty cases of an
underrecognized entity. Hum Pathol. 32:583–589. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Rosen PP: Rosen’s Breast Pathology. 2nd
edition. Lippincott Williams & Wilkins; Philadelphia, PA: pp.
561–564. 2001
|