Introduction
Breast cancer is the second most common type of
cancer worldwide and the most common in women (1,2). In
Brazil, it is estimated that 52,650 new cases of this tumor emerged
in 2012 (2), whereas in the USA and
western Europe, the estimate is for 500,000 new cases/year
(3). Despite the high incidence,
early diagnosis and introduction of more effective treatments make
it possible to reduce mortality and improve the quality of life of
patients with this disease (4).
Every prognostic marker employed for determining
global patient survival is capable of generating important
information related to the clinical behavior of mammary gland
tumors. However, in most cases, they neither predict disease
progression nor the response to chemotherapy (5,6).
According to vant’t Veer et al(5), women with breast cancer at the same
disease stage can have completely different responses to the same
treatment.
Systemic treatment of breast cancer includes the use
of cytotoxic, hormonal and immunotherapeutic agents. In general,
these treatments are active at the beginning of therapy in 90% of
primary breast cancers and 50% of metastases; however, after a
variable period, the disease tends to progress (1,7).
Better predictive and prognostics markers are needed
in clinical practice (8), since
studies of clinical and molecular characteristics of tumors allow
therapeutic strategies to be designed more efficiently and with
less toxicity (1,4,9). In
this context, the expression of antioxidant proteins in tumor cells
has been assessed as a predictive and prognosis factor of the
response to cytotoxic treatments (10–12).
Glutathione (GSH) is a tripeptide comprising of
glycine, cysteine and glutamic acid residues (13). Its synthesis requires the
participation of two enzymes consecutively. First glutamate
cysteine ligase enzyme (GCLC) conjugates glutamic acid and
cysteine, producing γ-glutamyl cysteine. This compound with its
sulfhydryl group (SH) is responsible for the antioxidant activity
of GSH. The second step is the binding of γ-glutamyl cysteine to
glycine catalyzed by glutathione synthetase (GSS), producing the
tripeptide γ-glutamyl cysteine glycine, known as GSH (14,15).
Glutathione peroxidase (GPX) contains selenium at a
catalytic site and uses GSH as an electron donor for the reduction
of H2O2 to H2O, converting itself
to its oxidized form, glutathione disulfide (GSSG) (16,17).
GSH is considered one of the most important agents of the
antioxidant defense system of the cell. Because it is conjugated to
GPX, GSH plays a role in the removal of xenobiotic and carcinogenic
agents (18).
High levels of GSH and/or GPX increase the
antioxidant capacity, as observed in many tumor cells. Although the
mechanism and the consequences of these changes are not well
characterized (17), recent
research has demonstrated that an increase in antioxidants in
neoplastic mammary tissue provides certain advantages to these
cells when compared to healthy tissue. The presence of these
enzymes in neoplastic cells may represent a low-grade response to
treatments that cause oxidative damage, such as radiotherapy and
various chemotherapeutics (19,20).
These previous findings show the importance of GSH
and GPX expression in tumor cells, making them potential predictive
and prognostic markers for breast cancer. Thus, the aim of this
study was to determine the prognostic and predictive values of GSH
and GPX expression and their relationship to several
clinicopathological parameters, patient overall survival, and
response to breast cancer treatment.
Materials and methods
Immunohistochemical study
Sample characterization
In a retrospective study, tumor fragments were
selected from 63 women aged 30 to 99 years (mean 58 years)
attending the Obstetrics and Gynecology service, Hospital de Base,
Faculty of Medicine of São José do Rio Preto from 2000 to 2005. The
clinicopathological parameters of the patients were obtained from
the service medical records.
Patients with no other malignancy who were subjected
to mastectomy/quandrantectomy but not to neoadjuvant
chemotherapy/radiotherapy were included in the study. All the
patients had been diagnosed with invasive ductal carcinoma. A panel
of classic prognostic markers were evaluated: estrogen receptor
(ER), progesterone receptor (PR), human epidermal growth factor
receptor-2 (HER-2/neu), p53 tumor-suppressor gene and the cell
proliferation marker, Ki-67. Furthermore, the patients were divided
in to 4 subgroups according to the immunohistochemistry of the
following markers: luminal A
(ER+PR+HER-2/neu−), luminal B
(ER+PR+HER-2/neu+),
HER-2/neu+, and triple-negative
(ER−PR−HER-2/neu−).
The parameters for histopathological evaluation were
those recommended by the International Union Against Cancer (UICC)
TNM classification of 1989. Among the entire group, 37 patients
(59%) who had received the same treatment including surgery and
adjuvant chemotherapy/radiotherapy
[5-fluorouracil/epirubicin/cyclophosphamide (FEC)] were designated
as group I; 19 patients (30%) who had received only adjuvant
chemotherapy were designated as group II and 7 patients (11%) who
had received no treatment after surgery were designated as group
III. The patients underwent clinical evaluation every 3–4 months.
Local tumor recurrence and metastasis in such cases were carefully
monitored, as well as the date and cause of death in order to
record the survival time of each patient.
Patient follow-up ranged from 120 to 2,704 days,
with a median of 1,473 days. For analysis of survival curves, the
patients were divided into higher and lower enzyme expression
groups using a cut-off value established by the receiver operating
characteristic curve (ROC). Only patients who died of tumor disease
were included in the final analysis. Patients with an incomplete
follow-up were excluded. The study was approved by the Research
Ethics Committee of the Faculty of Medicine of São José do Rio
Preto (protocol no. 25372009).
Immunohistochemical technique
For administration of the technique, blocks of
paraffin-embedded tumor fragments were cut to provide 3-μm
sections. The sections were prepared on silanized slides and
subsequently deparaffinized, rehydrated through graded alcohol and
incubated with 3% hydrogen peroxidase for 30 min to block
endogenous peroxidase activity. Antigen retrieval was carried out
in a Pan Steam (ARNO, São Paulo, Brazil) at 95°C with buffer for 35
min for each specific antibody (Table
I). After cooling, the slides were covered with bovine serum
albumin (BSA) solution for 30 min and incubated at 4°C overnight
with the antibodies described in Table
I.
 | Table ISpecifications and manufacturers of
the antibodies used for the study. |
Table I
Specifications and manufacturers of
the antibodies used for the study.
| Antibody | Clonality | Dilution | Buffer | Company |
|---|
| Primary antibody
anti-ER | Monoclonal | 1:100 | Tris EDTA pH
9.0 | Dako |
| Primary antibody
anti-PR | Monoclonal | 1:100 | Tris EDTA pH
9.0 | Biocare
Medical |
| Primary antibody
anti-HER-2/neu | Polyclonal | 1:200 | Tris EDTA pH
9.0 | Dako |
| Primary antibody
anti-p53 | Monoclonal | 1:500 | Tris EDTA pH
9.0 | Zymed |
| Primary antibody
anti-Ki-67 | Monoclonal | 1:100 | EDTA pH 8.0 | Spring |
| Primary antibody
anti-GSH | Monoclonal | 1:100 | Citrate pH 6.0 | Millipore |
| Primary antibody
anti-GPX | Polyclonal | 1:1,200 | Citrate pH 6.0 | Abcam |
Subsequently they were washed with
phosphate-buffered saline (PBS) for 15 min and incubated with the
Easy Path kit (Erviegas, São Paulo, Brazil), which consisted of the
secondary antibody biotinylated anti-mouse, rabbit, and goat
immunoglobulins for 1 h and the streptavidin-peroxidase complex for
30 min, followed by washing with PBS for 15 min. We applied 0.5%
3,3′-diaminobenzidine tetrahydrochloride (DAB; Signet Laboratories,
Dedham, MA, USA) to the slides for 2–5 min at 20–22°C. The slides
were counterstained with Harris’s hematoxylin for 40 sec. Negative
controls were obtained by omitting the primary antibody, and liver
or prostate tissue served as an internal positive control in every
assay.
Evaluation of immunohistochemical
staining
To assess the immunoexpression of GSH and GPX,
multiple fields were examined on each slide, particularly
demarcated areas with distinct brown staining. The slides were
photographed and the enzymes were quantified by AxioVision software
and by observation through a ×40 lens of a Zeiss Axioskop2
microscope.
For each sample, three regions of tumor tissue were
selected and 20 spots of the tumor cells were marked within each
region, thereby analyzing 60 different spots of every sample to
average the relative intensity of immunoreactivity. The values were
obtained as arbitrary units (au), and the mean optical density
(MOD) indicated the specific staining intensity in the
immunoreactive areas.
The staining of HER-2/neu was considered by counting
the number of positively stained cells in the membrane and was
expressed as a percentage of the total tumor cells. According to
ASCO/CAP guidelines (21) the
following categories were defined: 0, no immunostaining; 1+, weak
or incomplete staining of the membrane in any proportion of tumor
cells; 2+, complete membrane staining or weak staining in 10% of
the tumor cells stained; 3+, uniform and intense staining of the
membrane in more than 30% of tumor cells. Tumors scored with 0 or
1+ were considered negative and those with scores 2+ or 3+ were
considered positive. Tumors were categorized into two groups in
relation to cellular proliferation according to the staining of
Ki-67 based on the count of the number of positively stained cells
and expressed as a percentage of the total: 0 or 1, no cellular
proliferation; 2 or 3, the presence of cellular proliferation. The
same parameter was used in the classification of the ER, PR and p53
tumor-suppressor gene: 0 or 1, no staining; 2, 3 or 4, presence of
staining.
Statistical analysis
The patients were separated into groups according to
the clinicopathological variables. The averages of the
densitometric analysis referring to the densitometry results and
the quantification of the different breast tumor groups were
compared by Student’s t-test or ANOVA, followed by the Bonferroni
test. The values are expressed as means ± SEM.
The cut-off for the risk of death was determined by
ROC. Survival curves were plotted by the Kaplan-Meier method, and
the differences between the curves were evaluated by a log-rank
test and hazard function. Multivariate logistic regression was
performed to evaluate the factors that influenced death. For all
tests, P<0.05 was considered to indicate a statistically
significant result. All analyses were performed using GraphPad
Prism 4 and StatsDirect software.
Molecular study
Sample characterization
Twelve core biopsies or tumor fragments >2 cm
were collected by surgery from the breast cancer patients who were
diagnosed with ductal carcinoma, who had not undergone chemotherapy
and/or radiation therapy prior to the point of collection. The
tumor fragments were washed in PBS containing 1%
penicillin/streptomycin, cut into microfragments with a scalpel and
incubated at 37°C in 5% CO2 with RPMI-1640 supplemented
with 20% BSA, 1% penicillin/streptomycin and 1% L-glutamine. The
cells were cultivated until they reached 80% confluence and were
subjected to immunocytochemistry using the primary antibodies
anti-cytokeratin, anti-vimentin and anti-calponin to confirm
epithelial origin.
Treatment of the cells in vitro
Cells were divided into two groups: control (no
treatment), and cells treated with 0.2 mg routine chemotherapy
(doxorubicin) for 24 h. At the end of the treatment, cell viability
was verified by cell counting in a Neubauer chamber (LaborOptik,
Bad Homburg, Hessen, Germany) with trypan blue dye (0.4%).
Quantitative PCR
Total RNA was extracted from the cell culture with
TRIzol (Invitrogen Life Technologies, São Paulo, Brazil) as
recommended by the laboratory and the total RNA from each sample
was reverse transcribed to complementary DNA (cDNA) using a High
Capacity cDNA kit (Applied Biosystems, Foster City, CA, USA).
Quantitative real-time polymerase chain reactions
were performed in triplicate using StepOnePlus™ System (Applied
Biosystems). Briefly, the reactions were performed in a 20 μl
volume with 10 μl of Power SYBR®-Green PCR Master Mix
(Applied Biosystems), 250 nM of each primer, and 10 ng of cDNA. PCR
conditions consisted of 50°C for 2 min, 95°C for 10 min, followed
by 35 cycles of 95°C for 15 sec and 60°C for 1 min. Following PCR,
dissociation curve analysis was performed to confirm the desired
single gene product: one cycle of 95°C for 15 sec, 60°C for 1 min,
and 95°C for 15 sec was carried out.
Each transcript level was normalized by division
with the expression values of HPRT1 used as an internal
control. Gene expression stability was analyzed by geNorm software.
The transcript level was calculated using the 2−Ct
method (22). The Ct was the
difference between the threshold cycles of the target and the
internal control and Ct was the difference between the average Ct
of the sample and the average Ct of the calibrator sample. The fold
difference (relative abundance) was calculated using the
2−ΔΔCT formula and plotted as mean ± SD of the
triplicate reactions. At least 3-fold differences were considered
significant.
A negative control was included in each reaction,
and one sample was chosen for reaction calibration. Experiments
were repeated when the coefficient of variation was higher than 5%.
After each reaction, the products were analyzed on 2% agarose gel
stained with ethidium bromide.
The gene was searched, selected in PubMed
(http://www.ncbi.nlm.nih.gov/entrez),
and synthesized from human messenger RNA already sequenced and
confirmed. Its design was made using the program PRIMER 3
(http://frodo.wi.mit.edu/cgi-bin/primer3/primer3_www.Cgi).
The HPRT1 gene was used as an endogenous control. Primers
used for amplification include: GSS foward, 5′-TGCTAAAGCCCCAGAGAG
AG-3′ and reverse, 5′-AGCAGGCAATTCTCAAAAGG-3′; GCLC foward,
5′-GCACAACGTTCTCAAGTG-3′ and reverse, 5′-TGGTTTGGGTTTGTCCTTTC-3′;
GPX foward, 5′-ATGGCGCAATTGTCCAAG-3′ and reverse, 5′-CTGGCC
TCCCCTTACAGTG-3′; HPRT1 foward, 5′-TTATAGTCAAG GGCATATCC-3′ and
reverse, 5′-AGCTTGCTGGTGAAA AGGAC-3′.
The genes were classified as underexpressed (samples
with less than -1 log3 measurement) and overexpressed (samples with
quantification greater than 1 log3).
Results
All tumors were histological grade II invasive
ductal carcinoma, with a preponderance of tumors of clinical stage
II (76.2%), in agreement with the TNM (tumor, node and metastasis)
classification.
Immunohistochemical procedure
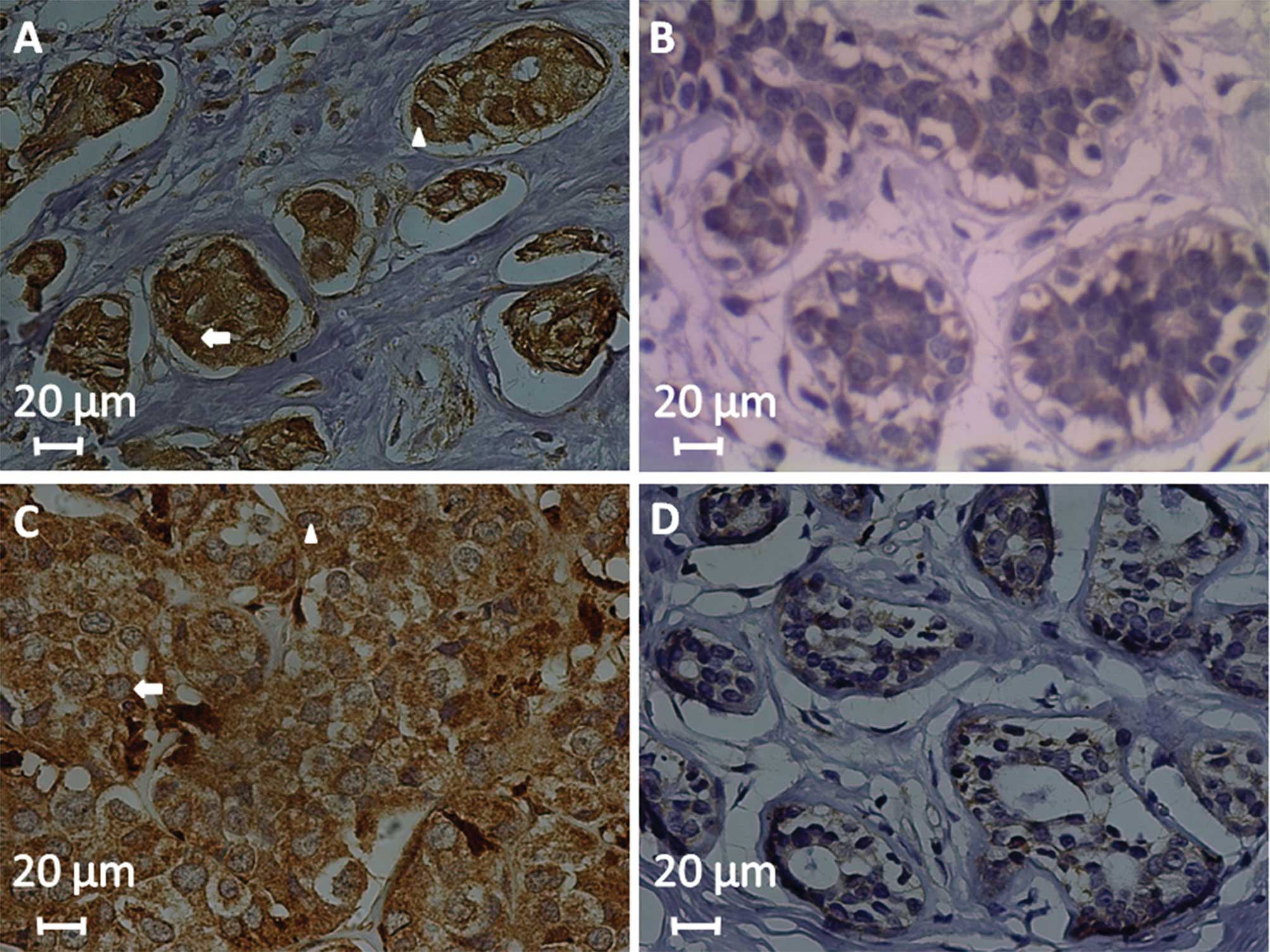
Immunostaining of GSH and GPX was evident in the
cytoplasm and focally in the nuclei of the neoplastic cells,
whereas the stroma showed no reactivity (Fig. 1).
Regarding the classical markers, GSH expression was
correlated with tumor ER-positivity, and GPX correlated with tumor
PR-negativity (P=0.03) (Table II).
Only 13 (20.6%) of the patients had tumors with luminal expression
A (ER+PR+HER-2/neu−), whereas 22
(35%) of the patients had tumors with luminal expression B
(ER+PR+HER-2/neu+); 41 (65%)
patients were HER-2/neu+ independently of the hormone
receptors, and 9 (14.2%) patients had a triple-negative
(ER− PR−HER-2/neu−) phenotype.
Nevertheless, there was no correlation between GSH or GPX
expression and the different clinical groups (P>0.05).
| Table IIMean expression of GSH and GPX and
its correlation with clinicopathological characteristics of the
breast cancer patients. |
Table II
Mean expression of GSH and GPX and
its correlation with clinicopathological characteristics of the
breast cancer patients.
| Clinicopathological
factors | No. of patients n
(%) | MOD of GSH | MOD of GPX |
|---|
| Patient age
(years) |
| ≥50 | 16 (25.4) | 187.8±3.517 | 192.6±2.234 |
| <50 | 47 (75.6) | 184.3±3.253 | 194.1±4.240 |
| P-value | | 0.54 | 0.74 |
| Smoker |
| Yes | 11 (17.5) | 188.0±5.177 | 196.7±5.951 |
| No | 52 (82.5) | 184.3±2.887 | 192.2±2.041 |
| P-value | | 0.58 | 0.38 |
| Hormone
therapy |
| Yes | 11 (17.5) | 179.7±4.918 | 195.9±4.863 |
| No | 52 (82.5) | 186.3±2.842 | 192.3±2.164 |
| P-value | | 0.32 | 0.49 |
| Lymph node
involvement |
| Positive | 13 (20.6) | 186.2±4.546 | 193.7±4.464 |
| Negative | 50 (79.4) | 184.7±2.992 | 192.5±2.249 |
| P-value | | 0.81 | 0.80 |
| Histological
grade |
| I | 3 (4.7) | 175.5±21.50 | 191.0±5.000 |
| II | 50 (79.4) | 184.0±2.837 | 192.2±2.301 |
| III | 10 (15.9) | 190.9±5.360 | 194.9±3.650 |
| P-value | | 0.30 | 0.51 |
| Clinical stage |
| I | 4 (6.3) | 175.3±8.686 | 204.0±13.320 |
| II | 48 (76.2) | 185.4±3.112 | 192.6±2.207 |
| III | 9 (14.3) | 185.4±5.373 | 188.9±5.832 |
| IV | 2 (3.2) | 195.5±0.500 | 199.5±0.500 |
| P-value | | 0.75 | 0.51 |
| Median tumor
diameter (cm) |
| >3 cm | 13 (20.6) | 186.9±4.190 | 196.8±3.211 |
| ≤3 cm | 50 (79.4) | 184.5±3.022 | 192.0±2.329 |
| P-value | | 0.69 | 0.32 |
| Estrogen
receptor |
| Positive | 46 (73) | 188.1±2.089 | 191.4±2.484 |
| Negative | 17 (27) | 176.4±7.285 | 197.2±2.671 |
| P-value | | 0.03a | 0.19 |
| Progesterone
receptor |
| Positive | 37 (58.7) | 188.3±2.330 | 189.4±2.870 |
| Negative | 26 (41.3) | 1802±5.106 | 198.0±2.160 |
| P-value | | 0.11 | 0.03 a |
| HER-2/neu |
| Positive | 41 (65) | 188.1±2.199 | 193.1±2.447 |
| Negative | 22 (35) | 178.8±6.180 | 192.6±3.389 |
| P-value | | 0.08 | 0.90 |
| p53 |
| Positive | 44 (69.8) | 184.4±3.353 | 194.8±2.322 |
| Negative | 19 (30.2) | 186.4±3.747 | 188.7±3.606 |
| P-value | | 0.73 | 0.16 |
| Ki-67 cell
proliferation index |
| High | 30 (47.6) | 185.3±4.526 | 194.2±2.878 |
| Low | 33 (52.4) | 183.9±2.680 | 191.8±2.724 |
| P-value | | 0.78 | 0.54 |
Immunohistochemical expression of GSH and GPX was
assessed in relation to the clinical course of the patients, taking
into account local recurrence, metastasis and/or rate of mortality
(Table II). High expression of GPX
was significantly correlated with a high rate of patient mortality
(P=0.03) (Table III). Group I
showed higher GPX expression in patients that succumbed to disease
(P=0.02) and Group II showed higher GSH expression in patients with
metastasis (P=0.03) (Table
III).
| Table IIIAssociation of GSH and GPX expression
and treatment and clinical outcome of the breast cancer
patients. |
Table III
Association of GSH and GPX expression
and treatment and clinical outcome of the breast cancer
patients.
| Group | Clinical
outcome | No. of patients n
(%) | MOD of GSH | MOD of GPX |
|---|
| Total Group | Local
recurrence |
| Yes | 6 (9.5) | 179.7±3.412 | 196.3±9.315 |
| No | 57 (90.5) | 185.5±2.778 | 192.3±2.004 |
| P-value | | 0.50 | 0.56 |
| Metastasis |
| Yes | 23 (36.5) | 186.8±3.030 | 196.5±3.379 |
| No | 40 (63.5) | 183.9±3.617 | 190.9±2.389 |
| P-value | | 0.59 | 0.17 |
| Death due to
disease |
| Yes | 20 (32) | 183.5±3.549 | 199.1±2.867 |
| No | 43 (68) | 185.7±3.354 | 190.1±2.459 |
| P-value | | 0.68 | 0.03a |
| Group I | Local
recurrence |
| Yes | 5 (13.5) | 180.4±4.082 | 203.2±6.111 |
| No | 32 (86.5) | 184.1±4.326 | 192.3±2.705 |
| P-value | | 0.74 | 0.14 |
| Metastasis |
| Yes | 14 (38) | 181.6±4.223 | 196.3±4.908 |
| No | 23 (62) | 184.8±5.556 | 192.3±2.808 |
| P-value | | 0.68 | 0.44 |
| Death due to
disease |
| Yes | 13 (35) | 179.3±4.033 | 201.6±3.362 |
| No | 24 (65) | 185.9±5.393 | 189.5±3.163 |
| P-value | | 0.41 | 0.02a |
| Group II | Local
recurrence |
| Yes | 1 (5) | 176.0±0.000 | 158.0±0.000 |
| No | 18 (95) | 185.1±4.195 | 193.1±4.009 |
| P-value | | - | - |
| Metastasis |
| Yes | 6 (31.5) | 196.8±3.311 | 200.2±5.382 |
| No | 13 (68.5) | 179.9±4.954 | 187.2±5.384 |
| P-value | | 0.03a | 0.15 |
| Death due to
disease |
| Yes | 5 (26) | 189.2±8.789 | 190.0±5.030 |
| No | 14 (74) | 183.0±4.555 | 191.7±5.532 |
| P-value | | 0.51 | 0.86 |
| Group III | Local
recurrence |
| Yes | 0 (0) | - | - |
| No | 7 (100) | 193.3±2.168 | 195.3±4.412 |
| P-value | | - | - |
| Metastasis |
| Yes | 3 (43) | 191.0±2.309 | 195.0±11.060 |
| No | 4 (57) | 195.0±3.391 | 195.5±2.630 |
| P-value | | 0.41 | 0.96 |
| Death due to
disease |
| Yes | 2 (28.5) | 196.0±1.000 | 205.0±12.00 |
| No | 5 (71.5) | 192.2±2.956 | 191.4±3.641 |
| P-value | | 0.47 | 0.18 |
ROC was calculated to explore the performance, and
the threshold values for GSH and GPX expression were used to
predict the risk of mortality in breast cancer patients. The ROC
graph indicated calculations for sensitivity/specificity of the
patients. Thus, the best cut-off value for GSH to discriminate high
risk of death in all patients was MOD = 170 au (sensitivity = 30%
and specificity = 88%). For GPX the best cut-off in the total
population was: MOD = 200 au (sensitivity = 60% and specificity =
67%).
Multivariate logistic regression showed that
clinical stages III or IV and metastasis were associated with an
increased risk of mortality in the breast cancer patients
(P<0.05) (Table IV). In
addition, in patients >50 years of age, high levels of cell
proliferation (Ki-67 positivity), local recurrence and higher GPX
expression showed a significant trend towards an increased risk of
mortality (P=0.05–0.06) (Table
IV).
| Table IVResults of the multivariate logistic
regression analysis. |
Table IV
Results of the multivariate logistic
regression analysis.
| Variables | OR | 95% CI | P-value |
|---|
| Age ≥50 years | 918.55 |
0.99–851,872.18 | 0.05a |
| Smoker | 2.30 | 0.00–6,851.12 | 0.83 |
| Large tumor size
(>3 cm) | 1.32 | 0.05–33.00 | 0.86 |
| Lymph node
involvement | 31.62 | 0.39–2517.38 | 0.12 |
| Staging III or
IV | 460.42 |
1.33–15,8371.26 | 0.03b |
| Histological grade
III | 0.01 | 0.00–86.94 | 0.32 |
| ER positivity | 14.97 | 0.42–525.45 | 0.13 |
| PR positivity | 0.007 | 0.00–1.73 | 0.07 |
| HER-2/neu
negativity | 11.26 | 0.33–378.73 | 0.17 |
| Cell proliferation
(Ki-67 positivity) | 66.57 | 0.75–5,905.44 | 0.06a |
| p53 positivity | 0.018 | 0.00–1.56 | 0.07 |
| Chemotherapy | 15.22 | 0.05–4,337.16 | 0.34 |
| Radiotherapy | 0.12 | 0.00–5.31 | 0.27 |
| Metastasis | 1,397.97 |
7.90–247,365.34 | 0.006b |
| Local
recurrence | 57,817.26 |
0.98–3,390,813,161.68 | 0.05a |
| High GSH
expression | 0.16 | 0.001–14.42 | 0.43 |
| High GPX
expression | 117.26 | 0.68–19,969.60 | 0.06a |
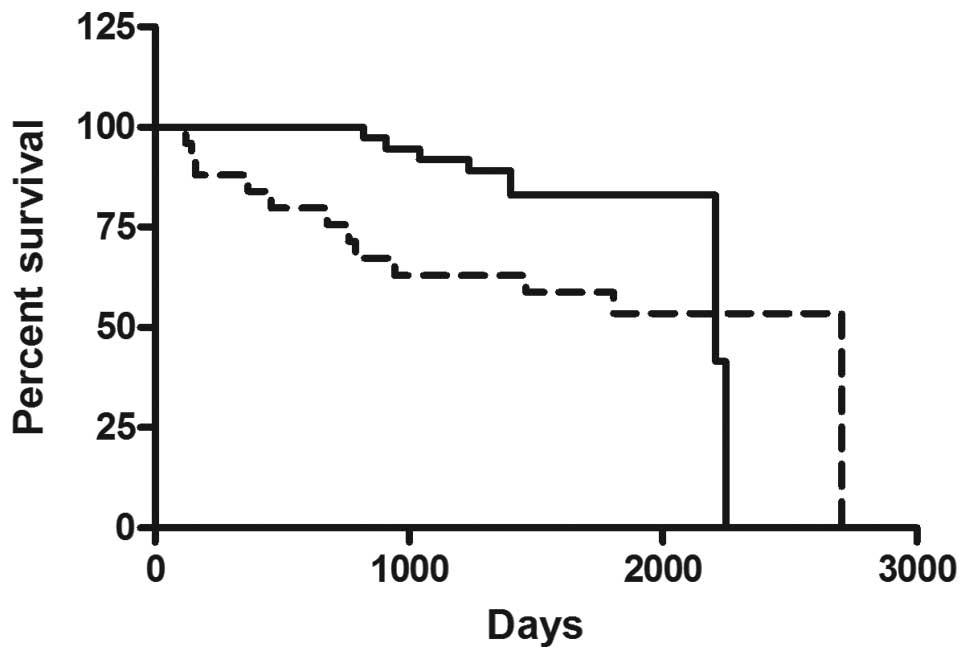
Patient follow-up ranged from 144 days (0.4 years)
to 2,704 days (7.4 years) with a median of 1,542 days (4.2 years).
For analysis of the survival curves, the patients were divided into
higher and lower enzyme expression groups using a cut-off value
established from the ROC curve. There was no correlation between
GSH expression and overall survival in groups I, II and III
(P>0.05). High GPX expression was correlated with a lower
overall survival rate in the entire group (P=0.03) (Fig. 2).
Quantitative PCR
Samples collected for the in vitro study were
from patients diagnosed with invasive ductal carcinoma; 3 patients
with histological grade I (25%), 6 with grade II (50%) and 3 with
grade III (25%). Only one patient had local recurrence and 1
patient died of metastasis. Following cell culture, the epithelial
origin was confirmed by immunocytochemistry, and GCLC, GSS and GPX
gene expression was evaluated after treatment with doxorubicin.
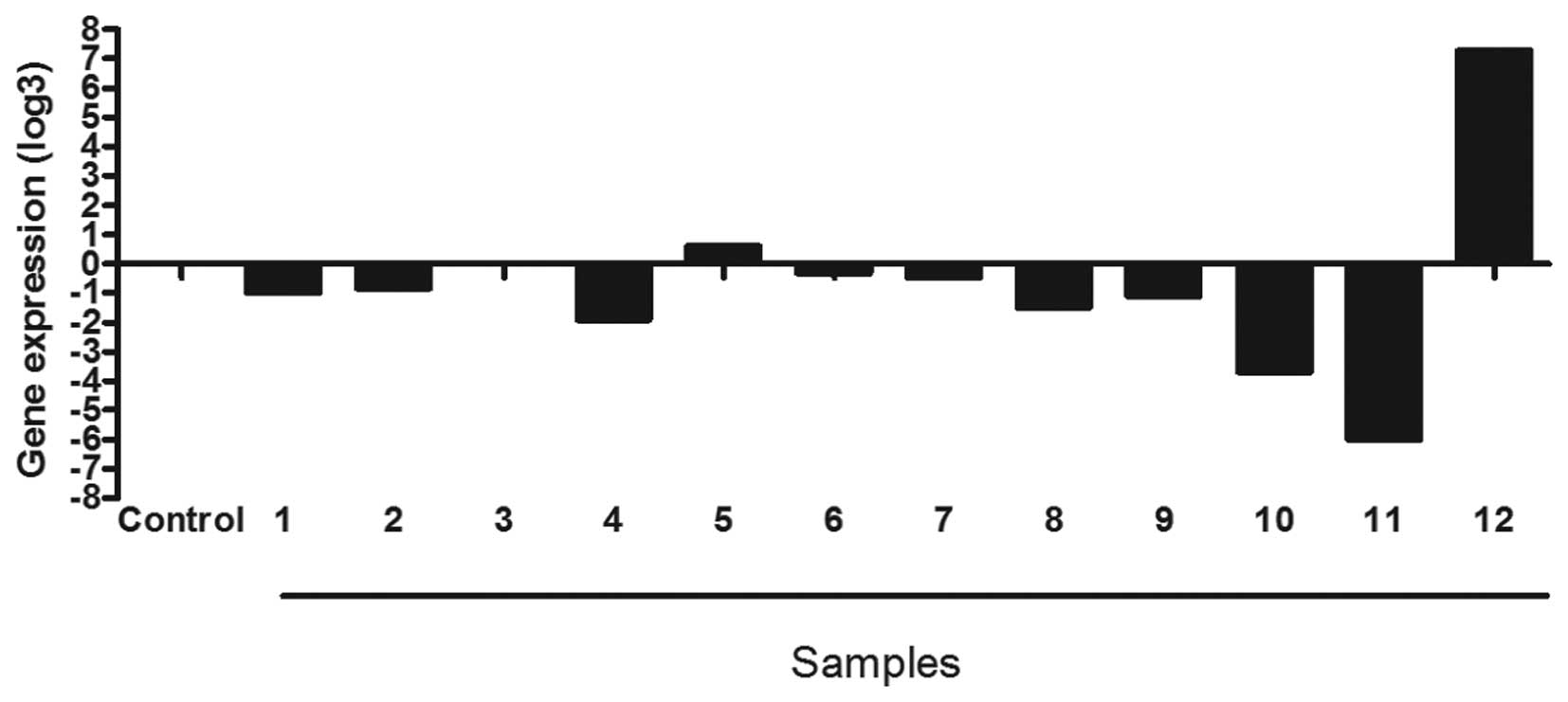
The GCLC gene, responsible for the first step in the
synthesis of GSH, was underexpressed in 7 (58.3%) of the culture
samples following treatment with chemotherapy. This gene was
overexpressed in one (8.3%) of the samples, and 4 (33.3%) samples
failed to reach the minimum level of expression in the log3 range
required to be considered indistinguishable from the controls
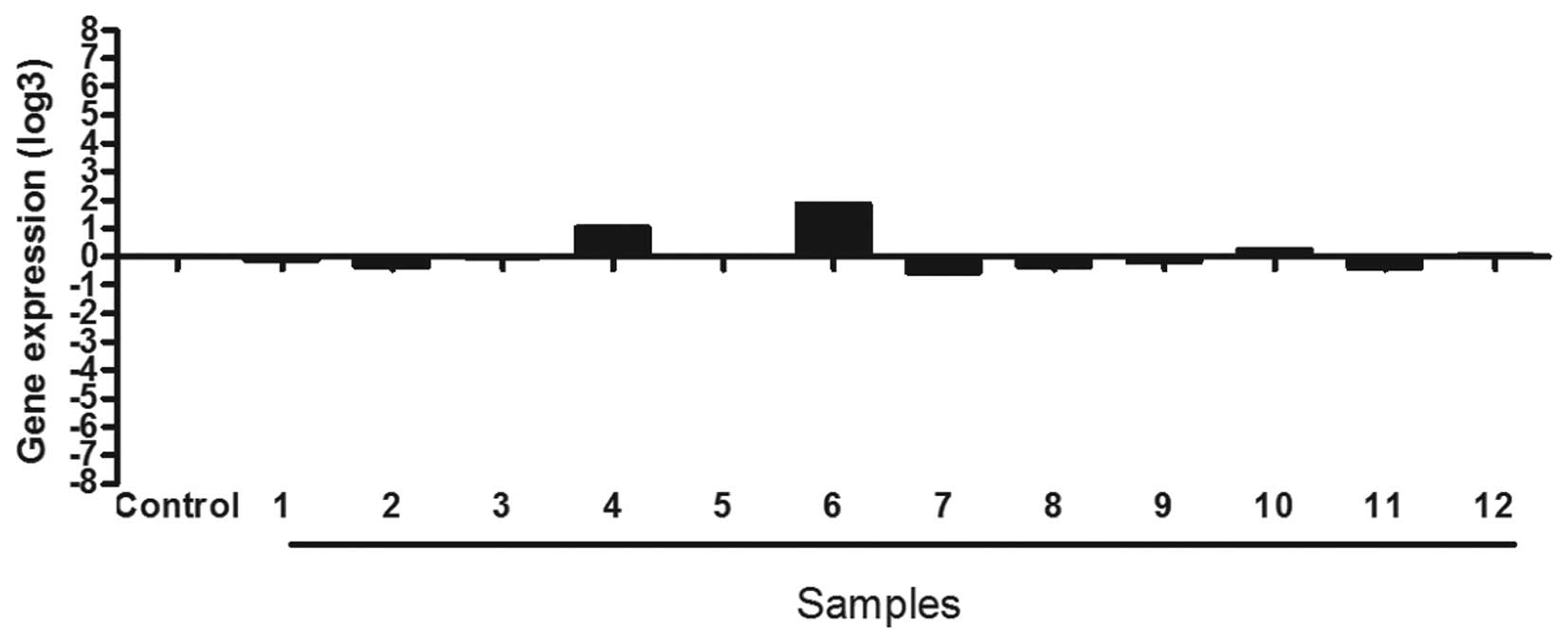
(Fig. 3). Only in 1 (8.3%) culture
sample treated with chemotherapy was the GSS gene overexpressed.
Eleven (91.6%) samples fail to reach the minimum level of
expression in the log3 range required to be considered
indistinguishable from the controls (Fig. 4).
The GPX gene was underexpressed in 6 (50%) of the
culture samples treated with chemotherapy. Only one (8.3%) sample
showed overexpression and 5 (41.6%) samples showed no significant
difference in expression compared to the control cells (Fig. 5).
Discussion
Studies concerning the association between
immunohistochemical expression of GSH, as well as GPX, the
clinicopathological parameters of breast cancer patients are
sparse. The majority of previous studies have used biochemical
methods to quantify the activity of these proteins, comparing
patients with breast cancer and healthy control patients (19,20,23,24).
In this study, tumors considered ER-positive
presented higher expression of the GSH protein when compared to
those that were ER-negative. In addition, PR-negative tumors
presented higher expression of GPX compared to those that were
PR-positive. According to Fernandes et al(25), individual analyses of the hormonal
receptors are not conclusive. With the combined evaluation of
hormonal receptors and the HER-2/neu protein, mammary carcinomas
can be grouped into 4 main subtypes that provide important
information related to the degree of malignancy and therapeutic
response to certain drugs (25,26).
Triple-negative carcinomas are considered more aggressive than the
luminal A or B subtypes, or even those overexpressing HER-2/neu.
There was no statistical correlation between GSH and GPX expression
and these carcinoma subtypes.
The immunohistochemical expression of GSH and GPX
was also related to the clinical progression of the breast cancer
patients. Patients that received only adjuvant chemotherapy (Group
II) and had metastases showed higher GSH expression. Ballatorri
et al(17) demonstrated that
a high level of GSH increased the antioxidant capacity of
neoplastic cells, making them more resistant to chemotherapy. Based
on this, high expression of GSH can be characterized as an
indicator of low response to chemotherapy in those analyzed
patients in this study, and may have contributed to the development
of metastasis.
High expression of GPX was associated with a high
rate of mortality, upon univaried and multivariate analyses. In
addition, patients with lower GPX expression had a lower overall
survival time. The association between high GPX expression and
mortality remained significant when evaluated only in the patients
restricted to the group of 37 women treated with adjuvant
chemotherapy and radiotherapy (Group I). The correlations found in
this study may be explained on the basis of enzymatic reactions
catalyzed by GPX. Some chemotherapeutic and radiotherapeutic
protocols potentially increase the already existent oxidative
stress in neoplastic processes, causing damage to DNA and cell
death (27). High levels of GPX are
known to correlate with cellular responses to oxidative stress. In
this way, cytotoxic treatments can reduce intracellular GPX
concentrations, based on the high concentration of GSSG in the
environment, or, on the other hand, cytotoxic treatments can induce
GPX expression as a cellular response to a high concentration of
H2O2(17,20,28,29). A
high level of GPX helps prevent oxidative damage that would
otherwise lead to tumor cell death due to the applied treatments
(18,19).
In vitro studies corroborate the
participation of GSH and GPX in cellular resistance to treatments.
In this study, there was no significant expression of GSS after
treatment with doxorubicin, whereas the GCLC and GPX genes were
underexpressed in 58.8 and 50% of the samples, respectively.
Many studies have demonstrated that alterations in
expression of genes responsible for the synthesis of GSH or GPX
usually occur after in vitro treatment with doxorubicin or
similar drugs. It is suggested that a large production of reactive
oxygen species (ROS) following treatment with doxorubicin is
responsible for the cytotoxicity noted in neoplastic cells, and as
a consequence, these cells overexpress genes responsible for the
synthesis of antioxidants, such as GSH and GPX, making them more
resistant to oxidative damages (30). Ozkan and Fiskin (31) found that the application of
epirubicin (analogous to the structure of doxorubicin) in mammary
neoplastic cells reduced GSH and GPX activity within 24 h of in
vitro exposure. More unlikely, a study by Ilvsova et
al(32) showed that the total
GSH concentration in the blood of breast cancer patients increased
significantly 24 h after doxorubicin administration.
Han et al(33), using the MCF-7 breast cancer cell
line, found a high sensitivity to doxorubicin when the levels of
GSH decreased. Vibet et al(34) using docosahexaenoic acid, known to
increase the oxidative mechanism of chemotherapeutics in mammary
neoplastic cells when combined with doxorubicin, showed that a high
concentration of ROS, due to this treatment, inhibited GPX
activity. The same finding was noted in animal models of breast
cancer. In this way, Sun et al(35) observed that high
H2O2 concentrations increased the sensivity
of tumor cells in vitro and in vivo not only to
doxorubicin, but to ionizing radiation. In contrast, Di et
al(36) demonstrated that GSH
overexpression did not prevent apoptosis in tumor cells after
treatment with doxorubicin, suggesting that the cytotoxicity of
this drug is not directly correlated with ROS production.
In conclusion, GPX was highly expressed in breast
cancer cells of patients with a worse clinical outcome and reduced
overall survival who underwent chemotherapy and radiotherapy. Thus,
it is suggested that GPX has an important role in the progression
of this disease, especially as a possible prognostic marker for
these patients. In addition, there was a relationship between
application of the chemotherapeutic drug doxorubicin and reduced
expression of the GPX gene, making it a candidate marker for
predicting therapeutic responses in breast cancer cases, yet this
needs to be confirmed in larger studies.
Acknowledgements
The authors thank the Capes/Coordenação de
Aperfeiçoamento de Pessoal de Nível Superior and FAPESP/Fundação de
Amparo à Pesquisa do Estado de São Paulo for their financial
support. We are also grateful to Dr Dalisio de Santi Neto,
Pathologist of the Department of Pathology and Forensic Medicine -
FAMERP for the collaboration in this study.
References
|
1
|
Gonzalez-Angulo AM, Moraes-Vasquez F and
Hortobagyl GN: Overview of resistance to systemic therapy in
patients with breast cancer. Adv Exp Med Biol. 608:1–22. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Instituto Nacional do Câncer (INCA).
Estimativas da incidência e mortalidade por câncer no Brasil.
Ministério da Saúde Rio de Janeiro. http://www.inca.gov.br/estimativa/2010/index.asp?link=conteudo_view.asp&ID=5.
Accessed Nov. 20, 2011
|
|
3
|
Gralow J, Ozols RF, Bajorin DF, et al:
Clinical cancer advances 2007: major research advances in cancer
treatment, prevention, and screening - a report from the American
Society of Clinical Oncology. J Clin Oncol. 26:313–325. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Hicks DG and Kulkarni S: Trastuzumab as
adjuvant therapy for early breast cancer. Arch Pathol Lab Med.
132:1008–1015. 2008.PubMed/NCBI
|
|
5
|
vant’t Veer LJ, Paik S and Hayes DF: Gene
expression profiling of breast cancer: a new tumor marker. J Clin
Oncol. 23:1631–1635. 2005.PubMed/NCBI
|
|
6
|
Pedersen L, Gunnarsdottir KA, Rasmussen
BB, et al: The prognostic influence of multifocality in breast
cancer patients. Breast. 13:188–193. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Duffy MJ and Crown J: A personalized
approach to cancer treatment: how biomarkers can help. Clin Chem.
54:1770–1779. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Thomas E and Berner G: Prognostic and
predictive implications of HER2 status for breast cancer patients.
Eur J Oncol Nurs. 4:10–17. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Duffy MJ, O’Donovan N and Crown J: Use of
molecular markers for predicting therapy response in cancer
patients. Cancer Treat Rev. 37:151–159. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Pastore A, Federici G, Bertini E and
Piemonte F: Analysis of glutathione: implication in redox and
detoxification. Clin Chem Acta. 333:19–39. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Townsend DM and Tew KD: The role of
glutathione-S-transferase in anti-cancer drug resistance. Oncogene.
22:7369–7375. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Jardim BV, Moschetta MG, Gelaleti GB, et
al: Glutathione transferase pi (GSTpi) expression in breast cancer:
An immunohistochemical and molecular study. Acta Histochem.
114:510–517. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Huber PC, Almeida WP and Fatima A:
Glutationa e enzimas relacionadas: papel biológico e importância em
processos patológicos. Quím Nova. 31:1170–1179. 2008.
|
|
14
|
Carnicer MJ, Bernardini S, Bellincampi L,
et al: Role of γ-glutamyl cysteine synthetase (γ-GCS) gene
expression as marker of drug sensitivity in acute myeloid
leukemias. Clin Chem Acta. 365:342–345. 2006.
|
|
15
|
Uchida M, Sugaya M, Kanamaru T and
Hisatomi H: Alternative RNA splicing in expression of the
glutathione synthetase gene in human cells. Mol Biol Rep.
37:2105–2109. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Valko M, Leibfritz D, Moncol J, et al:
Free radicals and antioxidants in normal physiological functions
and human disease. Int J Biochem Cell Biol. 39:44–84. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Ballatori N, Krance SM, Notenboom S, et
al: Glutathione dysregulation and the etiology and progression of
human diseases. Biol Chem. 390:191–214. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Kumaraguruparan R, Balachandran C, Manohar
BM and Nagini S: Altered oxidant-antioxidant profile in canine
mammary tumours. Vet Res Commun. 29:287–296. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Rajneesh CP, Manimaran A, Sasikala KR and
Adaikappan P: Lipid peroxidation and antioxidant status in patients
with breast cancer. Singapore Med J. 49:640–643. 2008.PubMed/NCBI
|
|
20
|
Kasapović J, Pejić S, Stojiljković V, et
al: Antioxidant status and lipid peroxidation in the blood of
breast cancer patients of different ages after chemotherapy with
5-fluorouracil, doxorubicin and cyclophosphamide. Clin Biochem.
43:1287–1293. 2010.PubMed/NCBI
|
|
21
|
Hammond ME, Hayes DF, Dowsett M, et al:
American Society of Clinical Oncology/College of American
Pathologists guideline recommendations for immunohistochemical
testing of estrogen and progesterone receptors in breast cancer. J
Clin Oncol. 28:2784–2795. 2010. View Article : Google Scholar
|
|
22
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(−ΔΔCT) method. Methods. 25:402–408. 2001.
|
|
23
|
Yeh CC, Hou MF, Wu SH, et al: A study of
glutathione status in the blood and tissues of patients with breast
cancer. Cell Biochem Funct. 24:555–559. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Kasapović J, Pejić S, Todorović A, et al:
Antioxidant status and lipid peroxidation in the blood of breast
cancer patients of different ages. Cell Biochem Funct. 26:723–730.
2008.
|
|
25
|
Fernandes RC, Bevilacqua JL, Soares IC, et
al: Coordinated expression of ER, PR and HER2 define different
prognostic subtypes among poorly differentiated breast carcinomas.
Histopathology. 55:346–352. 2009. View Article : Google Scholar
|
|
26
|
Basu S, Chen W, Tchou J, et al: Comparison
of triple-negative and estrogen receptor-positive/progesterone
receptor-positive/HER2-negative breast carcinoma using quantitative
fluorine-18 fluorodeoxyglucose/positron emission tomography imaging
parameters: a potentially useful method for disease
characterization. Cancer. 112:995–1000. 2008.
|
|
27
|
Murawaki Y, Tsuchiya H, Kanbe T, et al:
Aberrant expression of selenoproteins in the progression of
colorectal cancer. Cancer Lett. 259:218–230. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Li S, Yan T, Yang JQ, et al: The role of
cellular glutathione peroxidase redox regulation in the suppression
of tumor cell growth by manganese superoxide dismutase. Cancer Res.
60:3927–3939. 2000.PubMed/NCBI
|
|
29
|
Estrela JM, Ortega A and Obrador E:
Glutathione in cancer biology and therapy. Crit Rev Clin Lab Sci.
43:143–181. 2006. View Article : Google Scholar
|
|
30
|
Gaudiano G, Koch TH, LoBello M, et al:
Lack of glutathione conjugation to adriamycin in human breast
cancer MCF-7/DOX cells. Inhibition of glutathione S-transferase
p1-1 by glutathione conjugates from anthracyclines. Biochem
Pharmacol. 60:1915–1923. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Ozkan A and Fiskin K: Protective effect of
antioxidant enzymes against drug cytotoxicity in MCF-7 cells. Exp
Oncol. 28:86–88. 2006.PubMed/NCBI
|
|
32
|
Ilvasova D, Mixon G, Wang F, et al:
Markers of oxidative status in a clinical model of oxidative
assault: a pilot study in human blood following doxorubicin
administration. Biomarkers. 14:321–325. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Han XQ, Li ZH, Zhang JG, et al: Effect of
decreased GSH on sensitivity of breast cancer cells to ADM. Sichuan
Da Xue Xue Bao Yi Xue Ban. 36:770–774. 2007.(In Chinese).
|
|
34
|
Vibet S, Goupille C, Bougnoux P, et al:
Sensitization by docosahexaenoic acid (DHA) of breast cancer cells
to anthracyclines through loss of glutathione peroxidase (GPx1)
response. Free Radic Biol Med. 44:1483–1491. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Sun W, Kalen AL, Smith BJ, et al:
Enhancing the antitumor activity of adriamycin and ionizing
radiation. Cancer Res. 69:4294–4300. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Di X, Shiu RP, Newsham IF and Gewirtz DA:
Apoptosis, autophagy, accelerated senescence and reactive oxygen in
the response of human breast tumor cells to adriamycin. Biochem
Pharmacol. 77:1139–1150. 2009. View Article : Google Scholar : PubMed/NCBI
|