Introduction
Tumor-promoting inflammation, recognized as the
eighth hallmark of cancer (1), is
highly involved in tumor growth, invasion and metastasis.
Inflammatory bowel diseases (IBDs), including ulcerative colitis
(UC) and Crohn's disease (CD), are associated with chronic
relapsing inflammation of the intestinal tract of unknown etiology
(2). IBD is somewhat common in western
countries, with a prevalence rate of 100–200/100,000. Over the past
10 years, the incidence of IBD has increased by approximately 10–20
times in China (3). Given the serious
harm and higher malignant transformation probability associated
with IBD, increasing numbers of individuals are becoming concerned
that this disease is a type of precancerous lesion (4). Currently, it is proposed that IBD is
caused by the multifactorial interactions between environment,
gene, infection and immune disorders (5). Activation of the intestinal immune system
and non-specific immune system, which leads to immunoreaction and
the inflammatory response, is important in the pathogenesis of
IBD.
XianJiTang, which has marked curative effects on
chronic diarrhoea, was created by Zhu et al (6). Long-term clinical practice and research
have demonstrated its efficacy (7,8).
JiaWeiXianJiTang (JWXJT), which is comprised of XianJiTang and
JianPi Chinese medicine, is administered to patients for diarrhoea,
colorectal cancer or advanced colorectal cancer surgery. As they
are inherently complex and are comprised of numerous components, a
characteristic of traditional Chinese medicine (TCM) recipes is
that they affect multiple targets and interact with other herbal
medicines. Studies investigating TCM at the cell and molecular
levels are difficult to conduct due to the unknown effective
components and mechanisms of action, as well as the unstable herbal
quality. The present study analyzed the effective components of
JWXJT and the therapeutic targets of IBD, and constructed a
relational network between them. Based on the results of network
analysis, the therapeutic targets of IBD and the mechanisms of
JWXJT were characterized at the cell and molecular levels, and the
regulatory interactions were analyzed in their entirety.
Materials and methods
Data preparation
The JWXJT was composed as follows: Agrimonia
pilosa var. japonica (30 g), Platycodon
grandiflorum (8 g), Coix lacryma-jobi (30 g),
Dolichos lablab (15 g), Plantago asiatica (15 g),
Codonopsis pilosula (9 g), Poria cocos (9 g),
Paeonia albiflora (9 g), Areca catechu (1.2 g),
Saussurea lappa (5 g), Hibiscus syriacus (9 g),
Prunus mume(4.5 g) and Glycyrrhiza uralensis (4.5 g).
It is proposed that patients with colorectal cancer that have not
undergone surgery and postoperative patients with colorectal cancer
who are susceptible to IBD, present with a deficiency of the spleen
and kidney, as well as symptoms, including an elevated heat,
dampness, phlegm and blood stasis. Deficiencies of the spleen and
kidney exist throughout the course of IBD, being significant in its
initiation and progression (9).
TCM-potential target database
(PTD)
The TCM-PTD (http://pharminfo.zju.edu.cn/ptd), which is dedicated
to providing accurate potential targets of TCM that are predicted
using state-of-the-art machine learning approaches, comprising
three databases ‘compounds’, ‘target’, and ‘total-relationship’.
The above three databases describe the sources of the compounds,
targets, as well as the interaction between compounds and targets
of the herbs.
Bibliographic database
The present study used the following databases: The
Wanfang Database (http://www.wanfangdata.com/), China National Knowledge
Infrastructure (CNKI; http://www.global.cnki.net/), and the VIP Database
(http://www.cqvip.com/). The following search
terms were used: ‘Inflammatory bowel disease’ or ‘enteritis’ or
‘target’.
Data analyses
The compounds of each herb in JWXJT and the targets
of IBD were screened in the TCM-PTD database. Following virtual
screening in the TCM-PTD database, discarding the repetitive data
and the data where the docking scores were less than five, the
final data were applied for further network construction. Network
construction was performed as follows: i) A compound-compound
target network was established by linking chemical compounds and
corresponding targets; ii) a herb-compound target-IBD target
network was constructed by connecting the 13 JWXJT herbs, the
corresponding compound targets, and the IBD targets that interacted
with the compound targets. The networks were generated using the
network visualization software Cytoscape version 3.2.1 (http://cytoscape.org/), which is used to visualize
biological pathways and networks of molecular interactions, and to
interact with these networks via profiles of gene expression,
annotations, as well as other state data. The software then offers
a basic set of features for data integration, analysis and
visualization for complicated network analysis.
Results
Drug targets associated with IBD
Four hundred and twenty-one, 410 and 58 articles
were retrieved from the Wanfang Database, CNKI and VIP Database,
respectively (Table I). The targets of
IBD associated with JWXJT were summarized as follows:
15-Hydroxyprostaglandin dehydrogenase (15-PGDH), 5′ AMP-activated
protein kinase (AMPK), bradykinin receptor, cellular tumor antigen
p53, cysteinyl leukotriene receptor (CYSLTR), dual specificity
mitogen-activated protein kinase (MAPK), eosinophil cationic
protein, glutathione-requiring prostaglandin D synthase, macrophage
colony-stimulating factor (M-CSF), nitric oxide (NO), prostaglandin
E2 receptor EP4 subtype (PTGE), prostaglandin reductase 2,
transforming growth factor (TGF) and tumor necrosis factor (TNF;
Fig. 1).
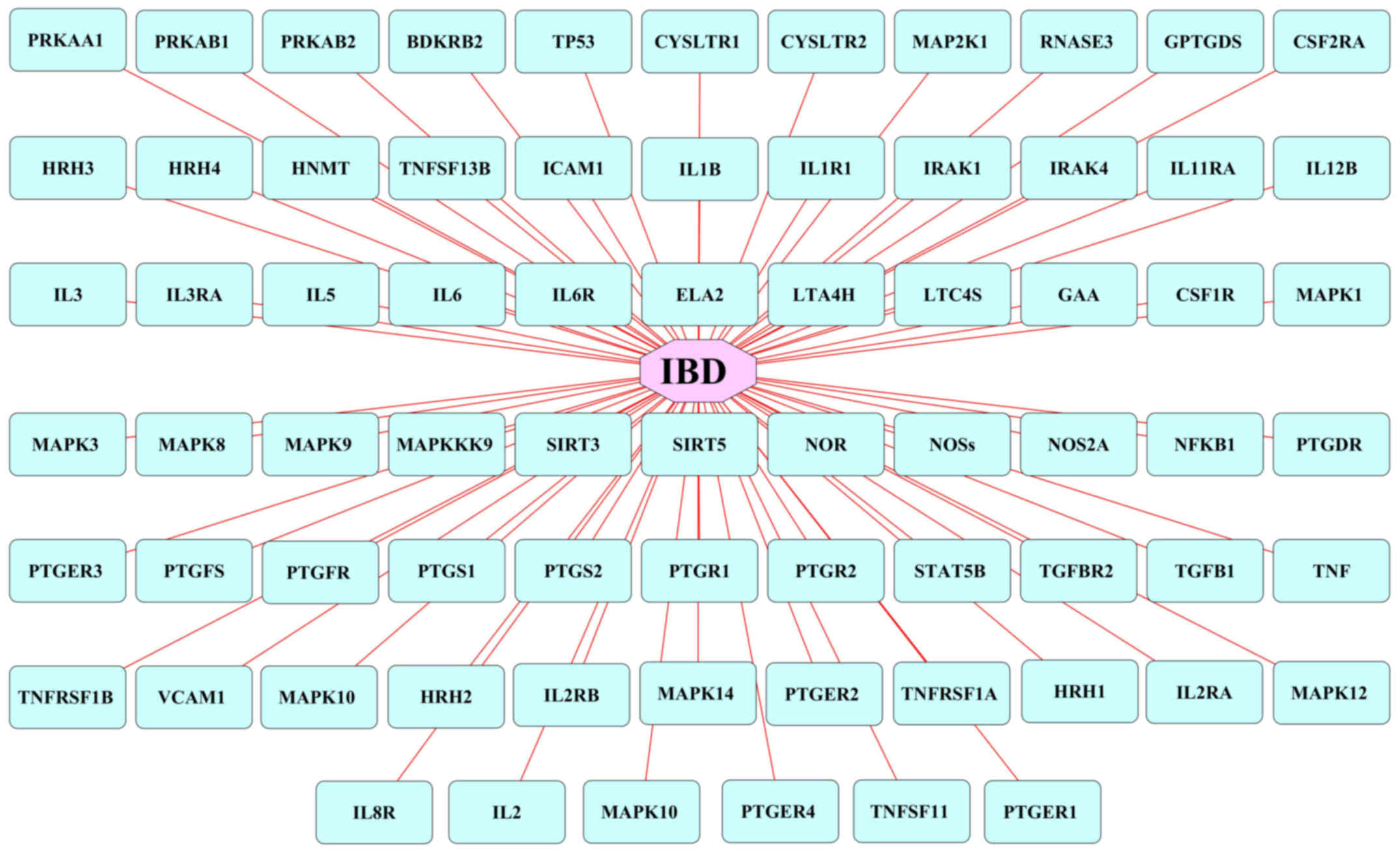 | Figure 1.Multiple targets of IBD. The blue
rectangles represent the targets associated with IBD. IBD,
inflammatory bowel disease; 15-PGDH, 15-hydroxyprostaglandin
dehydrogenase; AMPK, 5′ AMP-activated protein kinase; BDKRB2,
bradykinin receptor, cellular tumor antigen p53; CYSLTR, cysteinyl
leukotriene receptor; MAPK, dual specificity mitogen-activated
protein kinase; RNASE3, eosinophil cationic protein; GPTGDS,
glutathione-requiring prostaglandin D synthase; M-CSF, macrophage
colony-stimulating factor; NO, nitric oxide; PTGE, prostaglandin E2
receptor EP4 subtype; PTGR2, prostaglandin reductase 2; TGF,
transforming growth factor; TNF, tumor necrosis factor. |
 | Table I.Articles associated with the targets
of inflammatory bowel disease. |
Table I.
Articles associated with the targets
of inflammatory bowel disease.
|
| Articles (n) |
|---|
|
|
|
|---|
| Database | ‘Target’ and
‘IBD’ | ‘Target’ and
‘enteritis’ | Total |
|---|
| Wanfang Database | 126 | 295 | 421 |
| China National | 155 | 255 | 410 |
| Knowledge
Infrastructure |
|
|
|
| VIP Database | 28 | 30 | 58 |
Compound-compound target network
analysis
The compound-compound target network is shown in
Fig. 2, and includes 205 interactions
between 673 compounds in JWXJT and 76 compound targets. In the
network, certain targets demonstrated more interactions with
compounds than others. This indicated that a large number of
targets may be regulated by multiple compounds rather than just
one. For example, M-CSF and PGDH were regulated by multiple JWXJT
ingredients, including Saussurea lappa and Glycyrrhiza
uralensis. In addition, AMPK, interleukin (IL), CYSLTR, MAPK,
NO, PTGE, prostaglandin reductase 2 and TGF are regulated by more
than one compound.
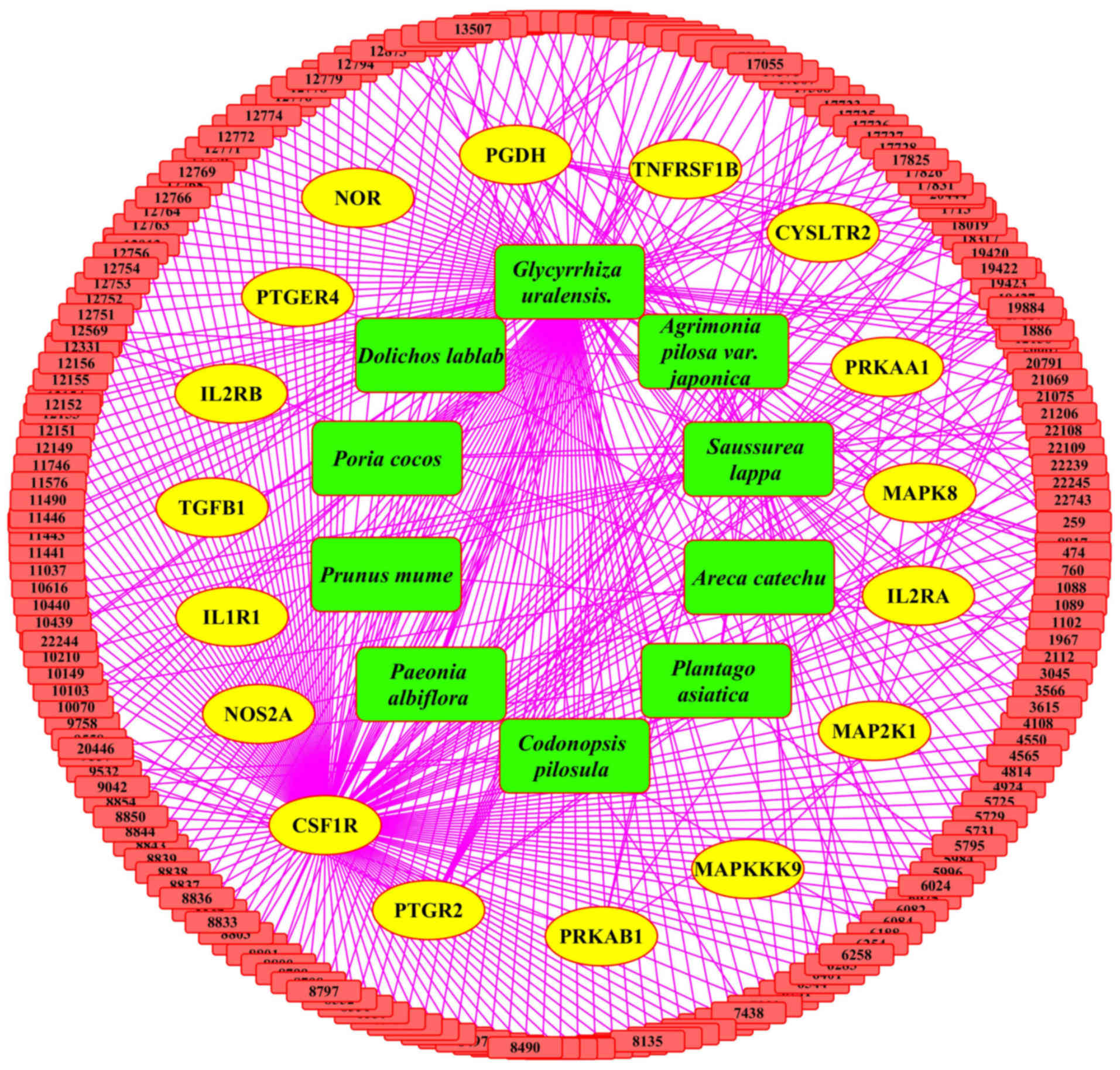 | Figure 2.Compound-compound target network
construction. Green rectangles represent the ingredients of JWXJT,
the yellow circles represent the predicted targets, and the red
rectangles represent the multiple compounds of JWXJT. JWXJT,
JiaWeiXianJiTang. 15-PGDH, 15-hydroxyprostaglandin dehydrogenase;
PRKAA1, 5′-AMP-activated protein kinase catalytic subunit α-1;
PRKAB1, 5′-AMP-activated protein kinase subunit β-1; CYSLTR2,
cysteinyl leukotriene receptor 2; MAP2K1, dual specificity
mitogen-activated protein kinase kinase 1; IL1R1, interleukin-1
receptor type I; IL2RA, interleukin-2 receptor α chain; IL2RB,
interleukin-2 receptor subunit β; CSF1R, macrophage
colony-stimulating factor 1 receptor; MAPK8, mitogen-activated
protein kinase 8; MAPKKK9, mitogen-activated protein kinase kinase
kinase 9; NOR, nitric oxide reductase; NOS2A, nitric oxide
synthase, inducible; PTGER4, prostaglandin E2 receptor EP4 subtype;
PTGR2, prostaglandin reductase 2; TGFB1, transforming growth factor
β-1; TNFRSF1B, tumor necrosis factor receptor superfamily member
1B. |
Herb compound target-IBD target
network analysis
The herb compound target-IBD target network was
constructed to identify the interactions between 13 herbs in JWXJT,
and the corresponding compound targets and IBD targets. The network
was composed of 205 interactions (13 herbs, 673 compound targets
and 76 IBD targets; Fig. 3).
Glycyrrhiza uralensis demonstrated the highest degree of
distribution followed by Saussurea lappa, Codonopsis
pilosula and Poria cocos, the interactions of which with
other herbs were more than one, thus, demonstrating their
significance in the network.
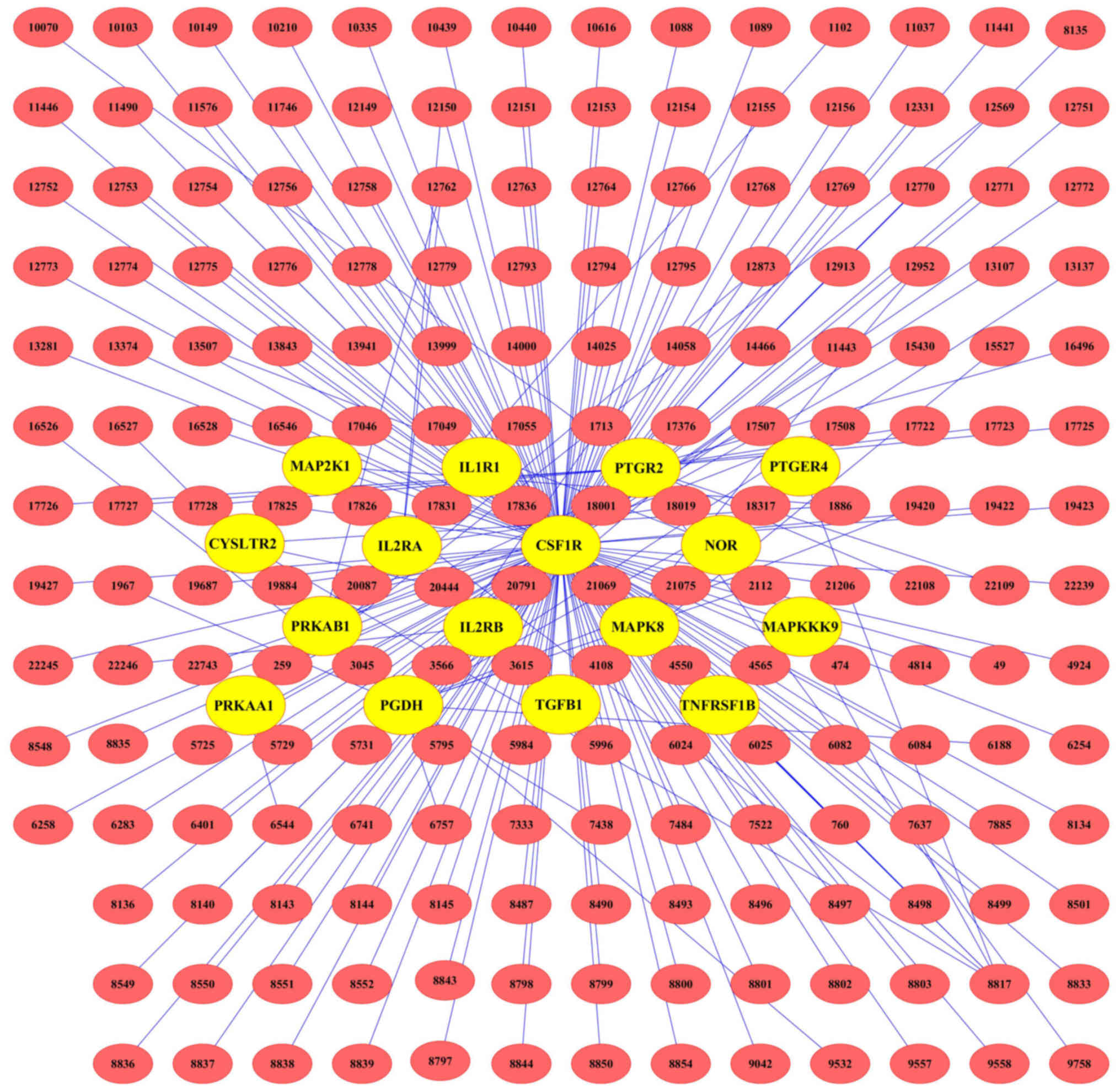 | Figure 3.Herb compound target-IBD target
network construction. Red rectangles represent the multiple
compounds of JWXJT and the yellow circles represent the IBD
targets. IBD, inflammatory bowel disease; JWXJT, JiaWeiXianJiTang.
15-PGDH, 15-hydroxyprostaglandin dehydrogenase; PRKAA1,
5′-AMP-activated protein kinase catalytic subunit α-1; PRKAB1,
5′-AMP-activated protein kinase subunit β-1; CYSLTR2, cysteinyl
leukotriene receptor 2; MAP2K1, dual specificity mitogen-activated
protein kinase kinase 1; IL1R1, interleukin-1 receptor type I;
IL2RA, interleukin-2 receptor α chain; IL2RB, interleukin-2
receptor subunit β; CSF1R, macrophage colony-stimulating factor 1
receptor; MAPK8, mitogen-activated protein kinase 8; MAPKKK9,
mitogen-activated protein kinase kinase kinase 9; NOR, nitric oxide
reductase; PTGER4, prostaglandin E2 receptor EP4 subtype; PTGR2,
prostaglandin reductase 2; TGFB1, transforming growth factor β-1;
TNFRSF1B, tumor necrosis factor receptor superfamily member 1B. |
Glycyrrhiza uralensis and Codonopsis
pilosula regulated multiple targets, including M-CSF-1 receptor
and PGDH (Fig. 4). Furthermore,
Agrimonia pilosa var. japonica, Platycodon
grandiflorum, Paeonia albiflora, Areca catechu,
Saussurea lappa, Hibiscus syriacus, Prunus
mume, Plantago asiatica, Coix lacryma-jobi,
Dolichos lablab and Poria cocos also regulated more
than one target.
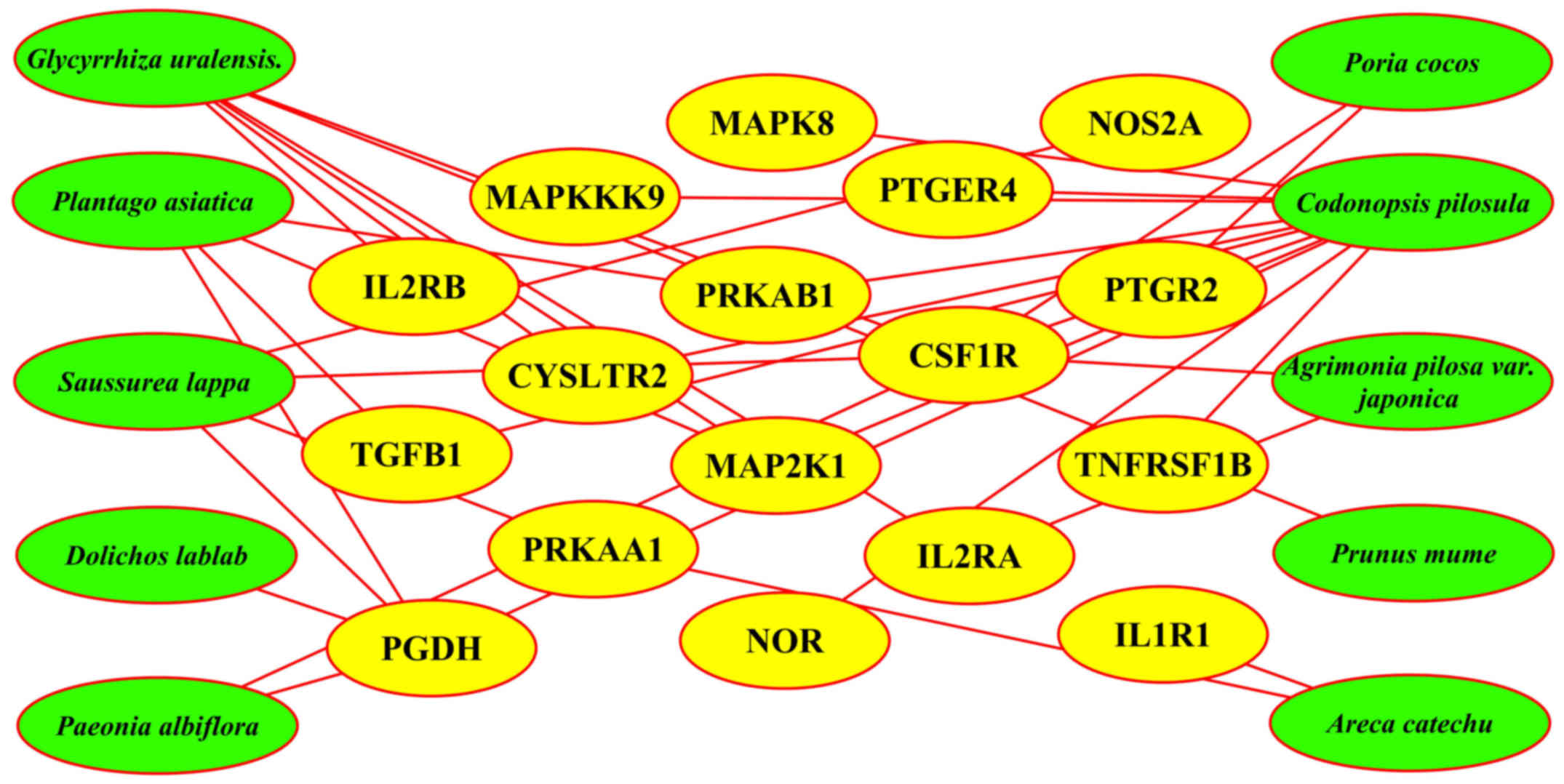 | Figure 4.Chinese herbal medicine and target
network construction. Green rectangles represent ingredients of
JWXJT and the yellow circles represent the screened targets. JWXJT,
JiaWeiXianJiTang. 15-PGDH, 15-hydroxyprostaglandin dehydrogenase;
PRKAA1, 5′-AMP-activated protein kinase catalytic subunit α-1;
PRKAB1, 5′-AMP-activated protein kinase subunit β-1; CYSLTR2,
cysteinyl leukotriene receptor 2; MAP2K1, dual specificity
mitogen-activated protein kinase kinase 1; IL1R1, interleukin-1
receptor type I; IL2RA, interleukin-2 receptor α chain; IL2RB,
interleukin-2 receptor subunit β; CSF1R, macrophage
colony-stimulating factor 1 receptor; MAPK8, Mitogen-activated
protein kinase 8; MAPKKK9, mitogen-activated protein kinase kinase
kinase 9; NOR, nitric oxide reductase; NOS2A, nitric oxide
synthase, inducible; PTGER4, prostaglandin E2 receptor EP4 subtype;
PTGR2, prostaglandin reductase 2; TGFB1, transforming growth factor
β-1; TNFRSF1B, tumor necrosis factor receptor superfamily member
1B. |
Discussion
In the present study, the potential molecular
mechanism of effective components of the TCM, JWXJT on IBD were
investigated using network pharmacology technology. JWXJT is
composed of Agrimonia pilosa var. japonica,
Platycodon grandiflorum, Coix lacryma-jobi,
Dolichos lablab, Plantago asiatica, Codonopsis
pilosula, Poria cocos, Paeonia albiflora,
Areca catechu, Saussurea lappa, Hibiscus
syriacus, Prunus mume and Glycyrrhiza uralensis.
Compounds from Saussurea lappa and Glycyrrhiza
uralensis have the greatest number of targets. It was
hypothesized that they were the most important components of JWXJT,
presenting as the monarch herbs according to ‘Sovereign and subject
Musa acts’. This refers to monarch, minister, assistant and guide,
which describe the status of different herbs in the TCM
prescription, as well as the variations in compatibility of
different herbs, from the perspective of multi-drug usage. Monarch
herbs are those in the prescription that exert the predominant
therapeutic effect on the disease/TCM syndromes. These are
considered to be the indispensable prescription herbs, which
perform the main actions, and exert the initial and most important
effect (10). Compounds from
Codonopsis pilosula and Poria cocos also have
numerous targets, potentially the less important components in
JWXJT, representing the minister herbs (that support the monarch
herbs in the treatment of the primary disease/TCM syndromes).
Compounds from Agrimonia pilosa var. japonica,
Paeonia albiflora, Areca catechu, Prunus mume
and Dolichos lablab had the fewest targets. It could be
speculated that they are the accessory components in JWXJT, serving
as the assistant and guide herbs. Compounds from Platycodon
grandiflorum, Coix lacryma-jobi and Hibiscus
syriacus did not have any targets, although these three herbs
are often administered in clinical TCM treatment for IBD or other
diseases. The reason for this deficiency of targets may be due to
the insufficient data capacity of the TCM-PTD or that the data was
not up-to-date.
Herb compounds, which exert more effects in 15-PGDH,
AMPK, IL-2 and M-CSF-1, and fewer effects in CYSLTR, MAPK, NO and
PTGE, may inhibit and reduce the expression levels of inflammatory
mediators and inflammatory lesions in tissues. This explains the
effect of JWXJT on the immune system, which may be referred to as
FuZheng therapy according to TCM. Whereby FuZheng refers to
enhancing physical fitness and improving the body's resistance to
disease, accompanied by other methods, including appropriate
nutrition and functional exercises, so as to overcome disease and
restore health.
The key molecule for negative regulation of
inflammation is 15-PGDH. It degrades prostaglandin and antagonizes
cyclooxygenase (COX)-2 in vivo (11). AMPK represses expression levels of
inflammation inhibitory genes, such as TNF-α, IL-1β, IL-6 and
inducible nitric oxide synthase (iNOS), reduces the bioactivity of
nuclear factor (NF)-κB, promotes the expression of nicotinamide
phosphoribosyltransferase and peroxisome-proliferator-activated
receptor γ coactivator (PGC)-1α, increases NAD+ content,
and enhances the acetylation enzyme activity of Sirtuin 1 (12–17). In the
early stages of IBD, p53 protein overexpression and microsatellite
instability are demonstrated, which are early events in the
occurrence and progression of IBD (18,19).
However, p53 represses the inflammatory response, which is
regulated by NF-κB (20). The
expression of iNOS has been identified to be positively correlated
with the expression of hypoxia-inducible factor-1 in IBD patients
(21), and a negative correlation was
identified between IBD and ILs (22,23).
Granulocyte-macrophage colony-stimulating factor (GM-CSF) and TGF
are highly expressed in IBD (24,25). GM-CSF
therapy reduces inflammation in the colon of mice (26) and TGF-β promotes restoration of the
intestinal mucosa (27). MAPK, an
important regulatory factor, limits inflammatory responses and
promotes the resolution of inflammation (28). Furthermore, anti-TNF monoclonal
antibody therapy effectively blocks IBD (29). Certain types of TCM treatment enhance
the immune system function of IBD patients by reducing TNF-α
expression levels (30).
The most common type of chronic intestinal
inflammation associated with colorectal cancer is IBD, consisting
of UC and CD. In younger patients, the inflammation is more severe
and the development of IBD into colorectal cancer is considered to
be more dangerous. Colorectal cancer caused by IBD is referred to
as colitis-associated cancer (CAC), which accounts for 15% of the
cause of mortality in IBD patients (31). The study by Kassam et al
(31) revealed that the formation of
CAC is an ‘inflammation-dysplasia-carcinoma’ sequential
pathological process, and multiple immune cells, cytokines and
other immune mediators are involved in the carcinogenesis of
colorectal cancer. CAC is predominantly caused by aggravation of
IBD by immunological dysfunction, and abnormal activation of the
NF-κB and Janus kinase/signal transducers and activators of
transcription signaling pathways. A large quantity of inflammatory
cells and pro-inflammation cytokines, such as TNF, IL-6, IL-17 and
IL-23, in the intestines activate reactive oxygen species and
reactive nitrogen intermediates, and alter biological processes,
including cellular growth, apoptosis and proliferation (32). Furthermore, consistent chronic
inflammation induces the dysregulation of signaling pathways, such
as the Wnt, p53, KRAS and TGF signaling pathways, resulting in
tumor development (19,20) Interferon-γ, TGF-β and IL-17 in patients
with DC and colon cancer exert inflammatory and immune regulation
functions (33). In addition, NF-κB,
TNF-α, IL-1, IL-6, IL8 and IL-27 have significant roles in CAC
(34–36). The expression of protease activated
receptor-2 (PAR-2) positively correlated with the expression of
COX-2 in patients with UC, and the increased expression levels of
PAR-2 and COX-2 promoted the occurrence and development of colon
cancer by cooperating with TF and PGE-2 (37). A previous study demonstrated that
granulocyte-colony stimulating factor (G-CSF) expression in a mouse
model increased during the course of CAC development. Furthermore,
inhibiting the secretion of G-CSF hindered the process of CAC
(38).
In conclusion, the network pharmacology analyses
revealed that the therapeutic effect of JWXJT on IBD functioned by
affecting molecular targets of IBD via the effective compounds of
JWXJT, for example, by antagonizing various pathogenic links of
IBD, as well as inhibiting inflammatory responses in IBD. In
addition, the scientific theory of the TCM, Fuzheng Quxie, used
modern biological evidence to explain the TCM principles of
monarch, minister, assistant and guide. The present study
characterized, in detail, the action mechanism of JWXJT, which
included enhancing the immune system and restraining novel blood
vessel growth by regulating 15-PGDH, AMPK, IL-2 and M-CSF-1, as
well as inhibiting adverse inflammatory reactions. Network
pharmacology is able to predict the underlying mechanisms of TCM,
and the current results provide a direction for future complex
basic biological studies, which will, in part, prevent waste of
resources.
Acknowledgements
The present study was supported by the Natural
Science Foundation of China (grant no. 81473628), Fund of Science
and Technology Commission of Shanghai (grant no. 14Z1438900),
Shanghai Health Development Planning Commission Translational
Medicine Focus Issue (grant no. 20124024) and the Natural Science
Foundation of China (grant nos. 81573749 and 81303102).
Glossary
Abbreviations
Abbreviations:
|
JWXJT
|
JiaWeiXianJiTang
|
|
IBD
|
inflammatory bowel disease
|
|
TCM
|
traditional Chinese medicine
|
|
UC
|
ulcerative colitis
|
|
CD
|
Crohn's disease
|
|
CAC
|
colitis-associated cancer
|
References
|
1
|
Kim TH, Rowat AC and Sloan EK: Neural
regulation of cancer: From mechanobiology to inflammation. Clin
Transl Immunology. 5:e782016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Cooperative Group of Inflammatory Bowel
Diseases of Digestive Disease of Chinese Medical Association, .
Chinese consensus on standard management of inflammatory bowel
diseases (2007, Jinan). Chin J Digestion. 27:545–550. 2007.
|
|
3
|
Ye L, Cao Q and Cheng J: Review of
inflammatory bowel disease in China. Scientific World Journal.
2013.2013. 296470http://dx.doi.org/10.1155/2013/296470PubMed/NCBI
|
|
4
|
Zhao YJ and Yuan YZ: Clinical study on the
relationship between inflammatory bowel disease and colorectal
neoplasms. J Dig Dis. 10:113–117. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Dhaneshwar SS: Colon-specific prodrugs of
4-aminosalicylic acid for inflammatory bowel disease. World J
Gastroenterol. 20:3564–3571. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Zhu LC, Zhu BX, et al: Zhu Lingchun
medication experience. Publishing house of Shanghai university of
TCM; 1989
|
|
7
|
Qiu ZJ, Zhu JP and Ma XQ: Zhu Lingchun
clinical experience in the treatment of chronic colitis and
characteristic, the famous old medical liangchunzhu 19 clinical
experience in the series. Liaoning J Tradit Chin Med. 28:399–400.
2001.
|
|
8
|
Zhong LL, Ji W and Wang D: The clinical
application of XianJiTang treating of chronic diarrhea, experience
prescription of Zhu Liangchun. Jilin J Tradit Chin Med.
32:1098–1099. 2012.(In Chinese).
|
|
9
|
Chen WT, Liu X, Ren JL, et al: Based on
cluster analysis of postoperative patients with colorectal cancer
medicine research. Chin Arch Tradit Chin Med. 1:101–104. 2016.
|
|
10
|
Shin JH, Jun SL, Hwang SY and Ahn SH:
Analytical research to determine the effects of the components of
ONGABO on the viability of HepG2 cancer cells by using the
sovereign, minister, assistant and courier principle. J
Pharmacopuncture. 15:42–51. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Cheng X: Mechanism of COX-2 controling
15-PGDH expression in gastric cancer cells (unpublished PhD
thesis)The Fourth Military Medical University; 2010
|
|
12
|
Giri S, Nath N, Smith B, Viollet B, Singh
AK and Singh I:
5-aminoimidazole-4-carboxamide-1-beta-4-ribofuranoside inhibits
proinflammatory response in glial cells: A possible role of
AMP-activated protein kinase. J Neurosci. 24:479–487. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Hattori Y, Suzuki K, Hattori S and Kasai
K: Metformin inhibits cytokine-induced nuclear factor kappaB
activation via AMP-activated protein kinase activation in vascular
endothelial cells. Hypertension. 47:1183–1188. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Zhang K, Deng CS, Zhu YQ and Zhang YM:
Significance of nuclear factor-NF-κB, cyclooxygenase 2 and
inducible nitric oxide synthase expression in human ulcerative
colitis tissues. World Chin J Digestology. 10:575–578. 2002.
|
|
15
|
Minami M, Shimizu K, Okamoto Y, Folco E,
Ilasaca ML, Feinberg MW, Aikawa M and Libby P: Prostaglandin E
receptor type 4-associated protein interacts directly with
NF-kappaB1 and attenuates macrophage activation. J Biol Chem.
283:9692–9703. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Fulco M, Cen Y, Zhao P, Hoffman EP,
McBurney MW, Sauve AA and Sartorelli V: Glucose restriction
inhibits skeletal myoblast differentiation by activating SIRT1
through AMPK-mediated regulation of Nampt. Dev Cell. 14:661–673.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Jäger S, Handschin C, St-Pierre J and
Spiegelman BM: AMP-activated protein kinase (AMPK) action in
skeletal muscle via direct phosphorylation of PGC-1alpha. Proc Natl
Acad Sci USA. 104:12017–12022. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Li J, Lai MD and Huang Q: Alterations of
p53 gene and microsatellite instability in ulcerative colitis and
ulcerative colitis-associated colorectal cancer. Zhejiang Da Xue
Xue Bao Yi Xue Ban. 33:108–114. 2004.(In Chinese). PubMed/NCBI
|
|
19
|
Wang H, Li Y, Zhang WW and Wang XQ: The
expression of P53, K-ras and hMSH2 in ulcerative colitis-associated
colorectal cancer. Chin J Digestion. 1:6–9. 2005.
|
|
20
|
Liu G, Park YJ, Tsuruta Y, Lorne E and
Abraham E: p53 Attenuates lipopolysaccharide-induced NF-kappaB
activation and acute lung injury. J Immunol. 182:5063–5071. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Xu CM, Dong WG, Yu BP, et al: Expression
of hypoxia-inducible factor-1alpha (HIF-1α) and inducible nitric
oxide synthase (iNOS) genes in inflammatory bowel disease. J The
Fourth Mil Med Univ. 17:1558–1561. 2004.
|
|
22
|
Xu L: The role of interleukin-2 and
platelet activation in the pathogenesis of ulcerative colitis
(unpublished PhD thesis)Fudan University; 2003
|
|
23
|
Qin Z, Wu C and Chen MM: Ulcerative
colitis patients of fecal calcium protein and serum interleukin-2
level and its clinical significance. Guangxi Medical Journal.
5:671–673. 2016.
|
|
24
|
Wang Y: GM-CSF and IL-1β role in the
malignant transformation of chronic enteritis and mechanism
research. The Chinese people's liberation army military academy of
medical sciences. 2014.
|
|
25
|
Wei WJ, Xu JM, Mei Q and Tang H:
Relationship between expression of transforming growth factor-β1
and its receptor in colonic mucosa with clinicopathology in
patients with ulcerative colitis. Clin J Gastroenterol. 13:341–344.
2008.
|
|
26
|
Lin Y, Cui Y, et al: Application of
particle - macrophage colony stimulating factor study curative
effect for the treatment of inflammatory bowel disease in mice.
Prog Anat Sci. 2:123–126. 2014.
|
|
27
|
Tu P, Zhang XH and Zhou XJ: Updated
correlation between angiopoietic factors and inflammatory bowel
disease. J Med Postgraduates. 20:1223–1226. 2007.
|
|
28
|
Yin W and Mei ZZ: Dual specificity
phosphatase-1: A negative regulator of inflammatory response. Int J
Immunol. 35:338–340. 2012.
|
|
29
|
Feng B, Lin ZJ and Bai H: Relationship
between anti-tumor necrosis factor-α monoclonal antibody and
chronic colitis in mice. Chin J Pract Internal Med. 26:280–282.
2006.
|
|
30
|
Song YY, Ren Y, Liu YZ, Liu W and Liu F:
Effect of Chinese medicine on tumor necrosis factor-α in treatment
of ul-cerative colitis. China Modern Doctor. 14:81–83. 2015.
|
|
31
|
Kassam Z, Belga S, Roifman I, Hirota S,
Jijon H, Kaplan GG, Ghosh S and Beck PL: Inflammatory bowel disease
cause-specific mortality: A primer for clinicians. Inflamm Bowel
Dis. 20:2483–2492. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Qu N, Xu M, Mizoguchi I, Furusawa J,
Kaneko K, Watanabe K, Mizuguchi J, Itoh M, Kawakami Y and Yoshimoto
T: Pivotal roles of T-helper 17-related cytokines, IL-17, IL-22,
and IL-23, in inflammatory diseases. Clin Dev Immunol.
2013:2013.968549 View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Li XY: Alteration of the percentage of T
helper 17 lymphocytes and interleukin-6 and −17 expression in
elderly colorectal cancer patients (unpublished PhD thesis)Dalian
Medical University; 2014
|
|
34
|
Yang H: NF-κB/IL-6 pathway in relation to
the colitis associated colorectal cancer development (unpublished
PhD thesis)Zhengzhou University; 2014
|
|
35
|
Feng DM: Determination and clinical
significance of sIL-2R, IL-8 and TNF-alpha in the inflammatory
bowel disease colorectal cancer (unpublished PhD thesis)Yanbian
University; 2013
|
|
36
|
Cui Y, Liu ZJ, Zhao ZG, Zheng P-Y and
Huang D-F: Significance of interleukin-27 expression in the
intestinal mucosa of patients with inflammatory bowel disease.
World Chin J Digestology. 1:39–43. 2010. View Article : Google Scholar
|
|
37
|
Ma X, Xie Yk, Liu T, Zhang Q, Wang CH,
Zhou CJ and Gao YJ: Relative research between PAR-2 and COX-2
expressed in intestinal mucosa of patients with ulcerative colitis.
Chin J Curr Adv Gen Surg. 2:107–111. 2013.
|
|
38
|
Shi XY, Yuan W, Tang WY, et al: The
expression of G-CSF in colitis-associated cancer. Oncology
Progress. 2:168–171, 174. 2016.
|














