Introduction
Kinesin Family Member 3A (KIF3A) is regarded as a
motor protein, which is associated with the intraflagellar
transport system of primary cilia and maintenance of ciliogenesis
(1,2).
In addition, KIF3A plays a role in primary cilia formation and in
centriole cohesion and subdistal appendage organization and
function (3). In 2013, Barakat et
al reported that KIF3A is necessary for the initiation and
maintenance of medulloblastoma for the first time (4). Liu et al also proved that KIF3A
plays a critical role in prostate cancer (5). Recently, Kim et al found that
KIF3A is a class of tumor suppressors in non-small cell lung cancer
(6).
Previous findings showed that primary cilia
decreased in breast cancer (7–9). In
addition, the disrupted expression of KIF3A leads to ablate
ciliogenesis and tumorigenesis in glioblastoma (10).
Thus, we hypothesized that KIF3A may affect the
formation and/or pathological change of primary cilia in breast
cancer, and subsequently on tumor progression. Therefore, the aim
of this study was to explore the possible relationship of KIF3A and
breast cancer progression, and by analyzing such a relationship to
explore its possible clinical usage.
Materials and methods
Study subjects
The samples of tissue microarrays (Xinchao
Biotechnology Company, Shanghai, China) were collected from 140
tissues of mammary carcinoma patients and 90 adjacent
para-carcinoma tissues (2 cm from the tumor tissues) as controls.
Within the total of 230 cases, 70 self-contrast tissues were
included. A long-term follow-up was carried out to all the patients
as long as 14 years, while the survival rate was measured up to
2013 and 2014, respectively. Details of the clinicopathological
parameters are presented in the results.
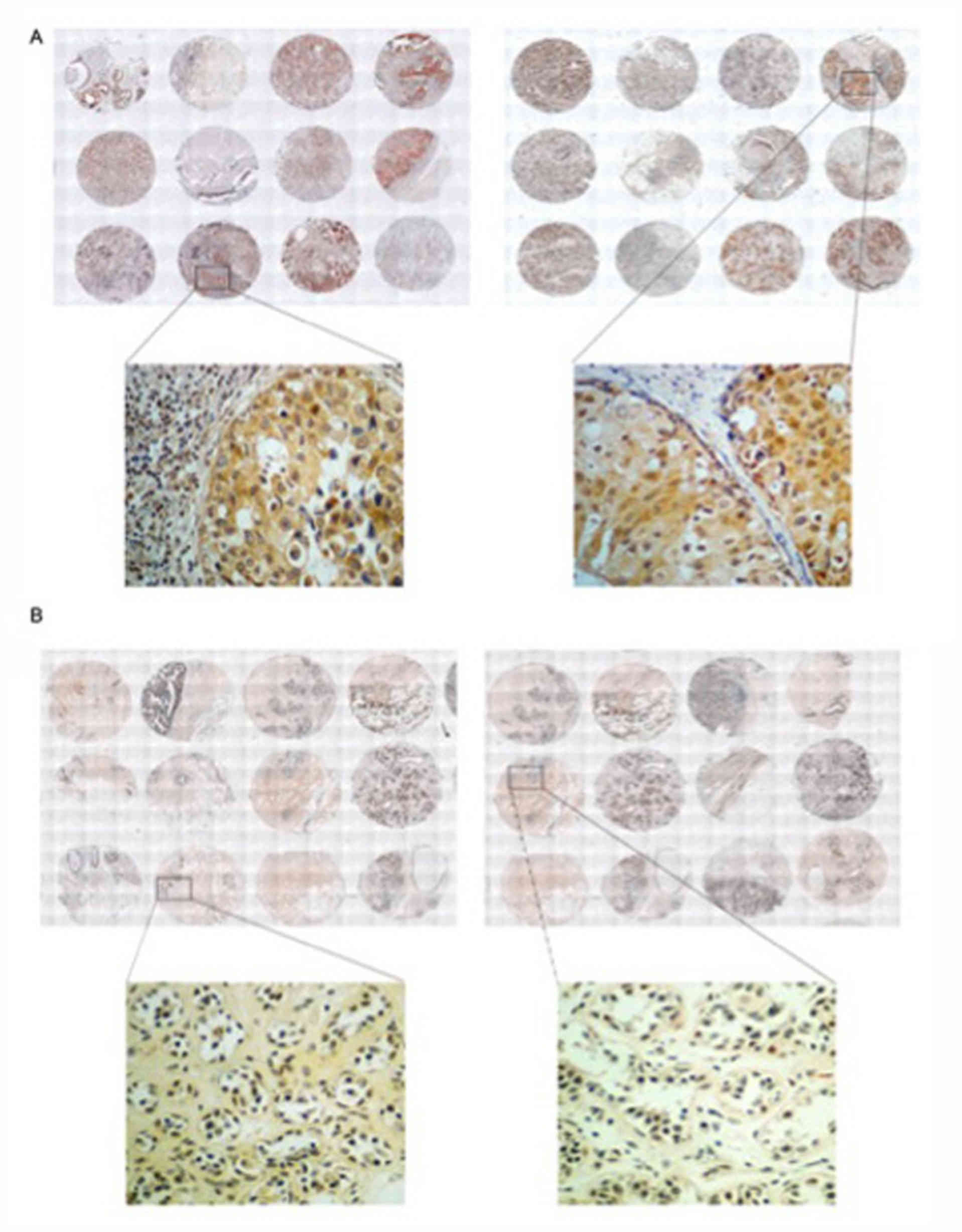
Immunohistochemical detection of
KIF3A
The expression level of KIF3A was detected by
immunohistochemical staining, performed according to the
instructions of the SP kit ZSGB-BIO, Beijing, China). The antibody
for KIF3A was rabbit polyclonal anti-KIF3A (1:800; cat. no. K3513;
Sigma-Aldrich; Merck KGaA, Darmstadt, Germany). Results of the
staining were evaluated separately by three pathologists under
double-blind conditions and scored by the intensity of positive,
the positive rates and final score (score of positive rates
multiplied by score of intensity of positive). Detailed scoring
system and criteria are presented in Table I.
 | Table I.Methods of scoring system and criteria
for immunohistochemical results. |
Table I.
Methods of scoring system and criteria
for immunohistochemical results.
| Score | Criteria |
|---|
| Intensity of
positive |
|
| 0 | Negative (−) |
| 1 | Weakly positive
(+) |
| 2 | Medium positive
(++) |
| 3 | Strong positive
(+++) |
| Positive rate |
|
| 0 | No or 0% nuclear and
cytoplasm staining (−) |
| 1 | <15% or occasional
nuclear staining (1–15%) (+) |
| 2 | >15 to 75% clear
positive nuclear staining (++) |
| 3 | >75% positive
staining (+++) |
| Final score |
|
| 0 | Total score 0–2 |
| 1 | Total score 3–5 |
| 2 | Total score 6–8 |
| 3 | Total score 9–11 |
Statistical analysis
The Chi-square test was performed to analyze the
differences in the expression of KIF3A between the 140 tumor
tissues and 90 adjacent para-carcinoma tissues, as well as the
correlations of clinicopathological parameters of corresponding
patients. Kaplan-Meier survival values were calculated to evaluate
the connection between the expression level of KIF3A and the
survival rate. Survival between the groups was compared using the
log-rank test. Statistical significance was set at P<0.05, while
P<0.001 indicated extremely statistically significant. The
software used was SPSS Version 21.0 (SPSS, Inc., Chicago, IL,
USA).
Results
Expression pattern of KIF3A in breast
cancer
Tissue microarrays were used to detect the
expression status of KIF3A in 230 cases. The intensity of positive,
the positive rate and the final score were measured for further
statistical analysis, respectively (Tables II and III).
| Table II.Expression level of KIF3A in 140 cases
breast cancer patients and 90 para-carcinoma tissues. |
Table II.
Expression level of KIF3A in 140 cases
breast cancer patients and 90 para-carcinoma tissues.
|
| Score |
|
|
|---|
|
|
|
|
|
|---|
| Item | 0 | 1 | 2 | 3 | No. | P-value |
|---|
| Intensity of
positive |
|
|
|
|
|
<0.001a |
|
Cancer | 4 | 22 | 56 | 58 | 140 |
|
|
Formal | 24 | 31 | 31 | 4 | 90 |
|
| No. | 28 | 53 | 87 | 62 | 230 |
|
| Positive rate |
|
|
|
|
|
<0.001a |
|
Cancer | 8 | 21 | 66 | 45 | 140 |
|
|
Formal | 23 | 16 | 46 | 5 | 90 |
|
| No. | 31 | 37 | 112 | 50 | 230 |
|
| Final score |
|
|
|
|
|
<0.001a |
|
Cancer | 8 | 32 | 52 | 48 | 140 |
|
|
Formal | 25 | 30 | 31 | 4 | 90 |
|
| No. | 33 | 62 | 83 | 52 | 230 |
|
| Table III.The expression level of KIF3A in 70
self-contrast patients. |
Table III.
The expression level of KIF3A in 70
self-contrast patients.
|
| Formal |
|
|
|---|
|
|
|
|
|
|---|
| Item | 0 | 1 | 2 | 3 | No. | P-value |
|---|
| Intensity of
positive |
|
|
|
|
| <0.001 |
|
Cancer |
|
|
|
|
|
|
|
0 | 1 | 3 | 7 | 6 | 17 |
|
|
1 | 0 | 5 | 11 | 10 | 26 |
|
|
2 | 1 | 2 | 9 | 11 | 23 |
|
|
3 | 0 | 0 | 2 | 2 | 4 |
|
|
No. | 2 | 10 | 29 | 29 | 70 |
|
| Positive rate |
|
|
|
|
| <0.001 |
|
Cancer |
|
|
|
|
|
|
|
0 | 1 | 3 | 8 | 4 | 16 |
|
|
1 | 2 | 1 | 6 | 5 | 14 |
|
|
2 | 0 | 5 | 18 | 14 | 37 |
|
|
3 | 0 | 0 | 2 | 1 | 3 |
|
|
No. | 3 | 9 | 34 | 24 | 70 |
|
| Final score |
|
|
|
|
| <0.001 |
|
Cancer |
|
|
|
|
|
|
|
0 | 1 | 5 | 6 | 5 | 17 |
|
|
1 | 2 | 7 | 6 | 9 | 24 |
|
|
2 | 0 | 5 | 11 | 10 | 25 |
|
|
3 | 0 | 0 | 2 | 1 | 3 |
|
|
No. | 3 | 17 | 25 | 25 | 70 |
|
The Chi-square test on the scores of intensity of
positive, positive rate and the final score, showed KIF3A
expression levels were significantly higher in 140 breast cancer
tissues than those in adjacent para-carcinoma tissues (P<0.01).
The same significant difference was also observed in the 70
self-contrast cases (Fig. 1).
Expression of KIF3A and
clinicopathological parameters
Currently used clinical pathological parameters of
the 230 breast cancer cases in this study are shown in Table IV. The average age of the patients
was 53 (from 31 to 83 years). Pathological grade was categorized as
grade I, II and III.
| Table IV.Regular clinicopathological
parameters of breast cancer. |
Table IV.
Regular clinicopathological
parameters of breast cancer.
|
Characteristics | No. |
|---|
| Age |
|
|
≤53 | 80 |
|
>53 | 60 |
| Pathology
grade |
|
| I | 12 |
|
I–II | 21 |
| II | 95 |
|
III |
7 |
| ER |
|
|
Positive | 88 |
|
Negative | 42 |
| PR |
|
|
Positive | 62 |
|
Negative | 51 |
| AR |
|
|
Positive | 101 |
|
Negative | 40 |
| HER2 |
|
|
Positive | 42 |
|
Negative | 89 |
| Lymph node
metastasis |
|
|
TnN0 | 86 |
|
TnNn | 46 |
| P53 |
|
|
Positive | 86 |
|
Negative | 47 |
| Ki-67 |
|
| − | 24 |
| + | 75 |
| ++ | 22 |
|
+++ | 10 |
| Ck56 |
|
|
Positive | 19 |
|
Negative | 112 |
| EGFR |
|
|
Positive | 38 |
|
Negative | 102 |
| TN |
|
|
TNBC | 18 |
|
NTNBC | 103 |
According to the intensity of positive, the positive
rate and the final score, the expression pattern of KIF3A and the
clinicopathological parameters in the 140 cases were evaluated,
respectively (Tables V–VII).
| Table V.Relationship between KIF3A expression
and clinicopathological parameters in the140 cases by intensity of
positive. |
Table V.
Relationship between KIF3A expression
and clinicopathological parameters in the140 cases by intensity of
positive.
|
| Intensity of
positive |
|
|
|---|
|
|
|
|
|
|---|
| Item | 0 | 1 | 2 | 3 | No. | P-value |
|---|
| Age |
|
|
|
|
| 0.728 |
|
≤53 | 2 | 15 | 31 | 32 | 80 |
|
|
>53 | 2 | 7 | 25 | 26 | 60 |
|
| Pathology
grade |
|
|
|
|
| 0.000b |
| I | 1 | 7 | 4 | 0 | 12 |
|
|
I–II | 0 | 2 | 12 | 8 | 22 |
|
| II | 2 | 13 | 37 | 43 | 95 |
|
|
III | 0 | 0 | 2 | 5 | 7 |
|
| ER |
|
Positive | 2 | 12 | 35 | 39 | 88 | 0.463 |
|
Negative | 1 | 10 | 16 | 15 | 42 |
|
| PR |
|
Positive | 2 | 10 | 32 | 34 | 78 | 0.475 |
|
Negative | 0 | 11 | 20 | 20 | 51 |
|
| AR |
|
Positive | 4 | 12 | 36 | 48 | 100 | 0.021a |
|
Negative | 0 | 10 | 20 | 10 | 40 |
|
| HER2 |
|
Positive | 1 | 5 | 13 | 23 | 42 | 0.211 |
|
Negative | 2 | 17 | 38 | 32 | 89 |
|
| Lymph node |
| metastasis |
|
TnN0 | 4 | 4 | 23 | 37 | 86 | 0.013a |
|
TnNn | 0 | 18 | 21 | 16 | 46 |
|
| P53 |
|
Positive | 1 | 15 | 33 | 37 | 86 | 0.495 |
|
Negative | 2 | 7 | 21 | 16 | 46 |
|
| Ki-67 |
| − | 1 | 6 | 11 | 6 | 24 | 0.320 |
| + | 2 | 11 | 32 | 30 | 75 |
|
| ++ | 0 | 4 | 7 | 11 | 22 |
|
|
+++ | 0 | 1 | 3 | 6 | 10 |
|
| Ck56 |
|
Positive | 0 | 2 | 10 | 7 | 19 | 0.757 |
|
Negative | 3 | 20 | 43 | 46 | 112 |
|
| EGFR |
|
Positive | 4 | 19 | 43 | 36 | 102 | 0.023a |
|
Negative | 0 | 3 | 13 | 21 | 37 |
|
| TN |
|
TNBC | 0 | 6 | 5 | 7 | 18 | 0.046 |
|
NTNBC | 6 | 23 | 43 | 31 | 103 |
|
| Table VII.Relationship between KIF3A expression
and clinical pathological parameters in the140 cases by final
score. |
Table VII.
Relationship between KIF3A expression
and clinical pathological parameters in the140 cases by final
score.
|
| Final score |
|
|
|---|
|
|
|
|
|
|---|
| Item | 0 | 1 | 2 | 3 | No. | P-value |
|---|
| Age |
|
|
|
|
| 0.465 |
|
≤53 | 6 | 18 | 26 | 30 | 80 |
|
|
>53 | 2 | 14 | 26 | 18 | 60 |
|
| Pathology
grade |
|
|
|
|
| 0.001a |
| G
I | 3 | 6 | 3 | 0 | 12 |
|
| G
I–II | 0 | 4 | 13 | 5 | 22 |
|
| G
II | 4 | 21 | 32 | 38 | 95 |
|
| G
III | 0 | 1 | 3 | 3 | 7 |
|
| ER |
|
|
|
|
| 0.008a |
|
Positive | 5 | 15 | 39 | 24 | 83 |
|
|
Negative | 2 | 15 | 9 | 21 | 47 |
|
| PR |
|
|
|
|
| 0.135 |
|
Positive | 3 | 10 | 29 | 20 | 62 |
|
|
Negative | 2 | 20 | 20 | 25 | 67 |
|
| AR |
|
|
|
|
| 0.309 |
|
Positive | 7 | 19 | 37 | 37 | 100 |
|
|
Negative | 1 | 13 | 15 | 11 | 40 |
|
| HER2 |
|
|
|
|
| 0.344 |
|
Positive | 2 | 7 | 14 | 19 | 42 |
|
|
Negative | 5 | 23 | 35 | 26 | 89 |
|
| Lymph node
metastases |
|
|
|
|
| 0.218a |
|
TnN0 | 5 | 8 | 21 | 20 | 54 |
|
|
TnNn | 3 | 23 | 31 | 27 | 84 |
|
| P53 |
|
|
|
|
| 0.125 |
|
Positive | 2 | 22 | 29 | 33 | 86 |
|
|
Negative | 5 | 9 | 19 | 13 | 46 |
|
| Ki-67 |
|
|
|
|
| 0.023a |
| − | 2 | 6 | 10 | 6 | 24 |
|
| + | 4 | 19 | 29 | 23 | 75 |
|
| ++ | 1 | 3 | 8 | 10 | 22 |
|
|
+++ | 0 | 2 | 1 | 7 | 10 |
|
| Ck56 |
|
|
|
|
| 0.872 |
|
Positive | 0 | 4 | 8 | 7 | 19 |
|
|
Negative | 7 | 26 | 40 | 39 | 112 |
|
| EGFR |
|
|
|
|
| 0.054 |
|
Positive | 6 | 28 | 38 | 30 | 102 |
|
|
Negative | 2 | 4 | 14 | 17 | 37 |
|
| TN |
|
|
|
|
| 0.873 |
|
TNBC | 0 | 3 | 8 | 7 | 18 |
|
|
NTNBC | 3 | 17 | 43 | 40 | 103 |
|
In terms of the intensity of positive in the 140
breast cancer patients, the statistical analysis revealed that the
higher level expression of KIF3A was correlated with the status of
lymph node metastasis, pathological grade, and the expression of
androgen receptor (AR) and epidermal growth factor receptor (EGFR).
In addition, the Chi-square test on both the positive rate and
final score indicated that a higher level of expression of KIF3A
was correlated with higher pathology grade and the expression of
estrogen receptor (ER) and Ki-67.
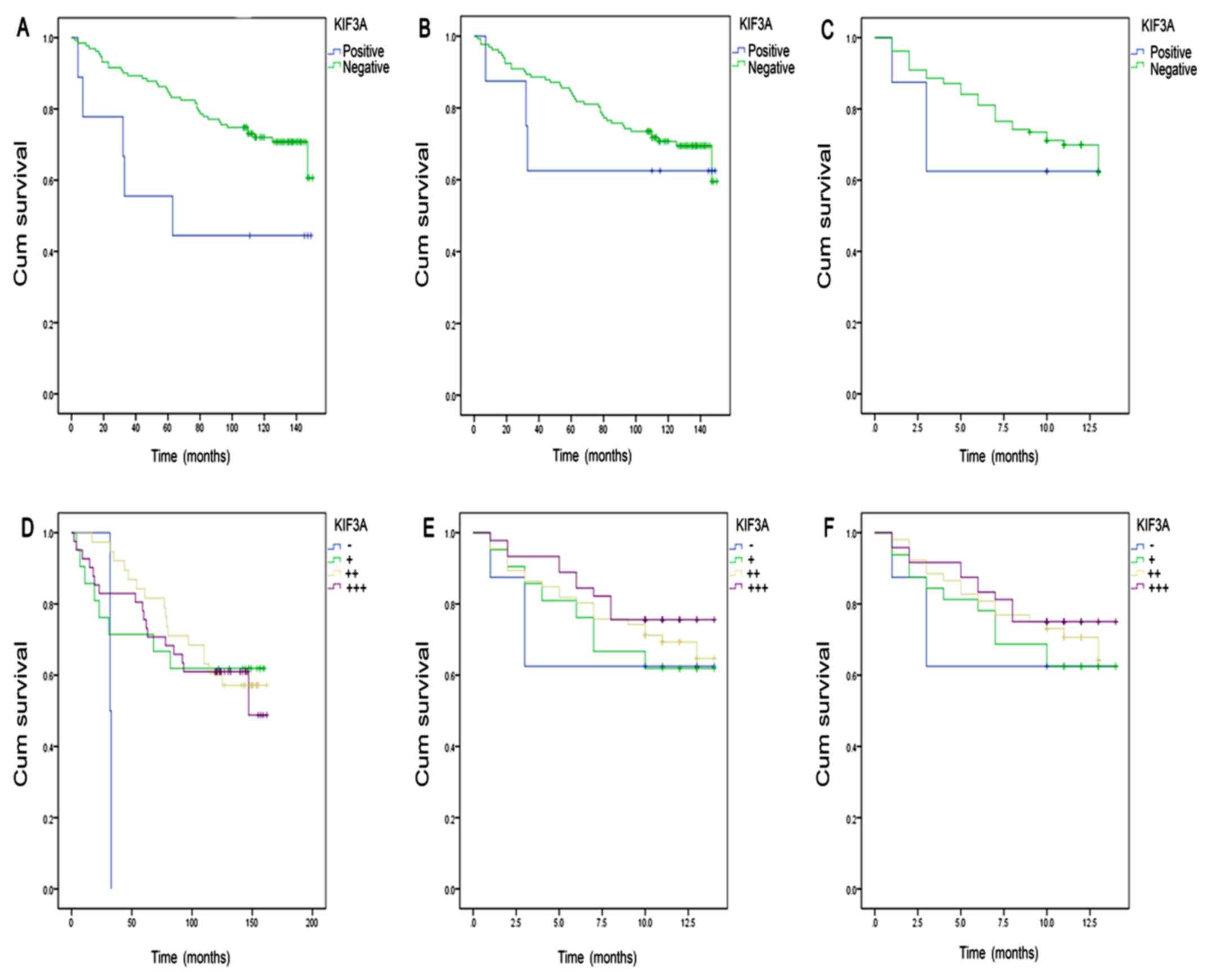
Expression of KIF3A and prognosis in
breast cancer patients
Kaplan-Meier analysis of the intensity of positive,
the positive rate and the final score was applied to explore the
association between KIF3A expression and the survival rate of 140
patients followed up to the year of 2013 and 2014.
For the cases followed up to 2013, grouped as KIF3A
positive (+, ++, +++) and negative (−), a statistical significance
was only identified between KIF3A expression and survival rate
(P=0.047) when evaluated by intensity of positive (Fig. 2 and Table
VIII).
| Table VIII.Correlation of KIF3A expression and
the survival rate of 140 breast cancer cases followed up to
2013. |
Table VIII.
Correlation of KIF3A expression and
the survival rate of 140 breast cancer cases followed up to
2013.
| Item | No. | P-value |
|---|
| Intensity of
positive |
|
0.047a |
|
Positive | 136 |
|
|
Negative |
4 |
|
| Positive rate |
| 0.628 |
|
Positive | 132 |
|
|
Negative |
8 |
|
| Final score |
| 0.635 |
|
Positive | 132 |
|
|
Negative |
8 |
|
For the cases up to 2014, positive (++) patients
showed an improved prognosis (P=0.045; Fig.2 and Table
IX).
| Table IX.Correlation of KIF3A expression and
the survival rate of 140 breast cancer cases followed up to
2014. |
Table IX.
Correlation of KIF3A expression and
the survival rate of 140 breast cancer cases followed up to
2014.
| Item | No. | P-value |
|---|
| Intensity of
positive |
| 0.045a |
| 0 | 4 |
|
| 1 | 22 |
|
| 2 | 56 |
|
| 3 | 58 |
|
| Positive rate |
| 0.217 |
| 0 | 8 |
|
| 1 | 21 |
|
| 2 | 66 |
|
| 3 | 45 |
|
| Final score |
| 0.223 |
| 0 | 8 |
|
| 1 | 32 |
|
| 2 | 52 |
|
| 3 | 48 |
|
Discussion
KIF3 is a heterotrimeric complex that consists of
KIF3A, KIF3B, and kinesis-associated protein 3 (KAP3) (11), the complex is considered as
microtubule (MT)-dependent molecular motors that function in
intracellular transport (12), which
is expressed ubiquitously. KIF3A is involved in the anterograde
transport of membranous organelles, distinct from synaptic vesicle
precursors and from vesicles, also required for ciliary basal feet
formation and MT anchoring to mother centriole (3). Thus, KIF3A plays an important role in
the procedure of ciliogenesis.
KIF3A was also reported to be associated with
certain pathological processes. It has been reported that KIF3A is
involved in forming defective bone formation and osteopenia
(13) and defective osteoblastic
differentiation in dental mesenchymal stem/precursor cells
(14). Since 2013, the expression and
function of KIF3A has been regarded as statistically significantly
and correlated with several tumors such as glioblastoma, prostate
cancer and medulloblastoma (4,5,10). It has been demonstrated that
disruption of the expression of KIF3A leads to ablate ciliogenesis
and tumorigenesis in glioblastoma (10).
Since KIF3A is associated with ciliogenesis and
primary cilia decrease in breast cancer (7–9),
identifying the association of KIF3A and breast cancer progression
is of great importance. Our results showed that the expression of
KIF3A is extremely higher in breast cancer tissues than that in
para-carcinoma tissues, and this difference was confirmed by the 70
self-contrast tissues. Barakat et al have reported that the
difference of KIF3A expression has the same relationship with
primary cilia (4). Based on our
results, KIF3A is associated with progression of breast cancer.
No reports have previously focused on the
relationship between KIF3A expression and breast cancer
progression. Thus, we statistically analyzed the clinical
mainstream clinicopathological parameters. Our data suggested that
the high expression of KIF3A was correlated with clinical diagnosis
and prognosis including: lymph node metastasis, pathological grade,
AR, ER, EGFR and Ki-67. In clinic, these parameters are not
sufficient for the accurate diagnosis and prognosis of breast
cancer, particularly triple negative breast cancer. Thus, it is
imperative to add new parameters for breast cancer, and according
to findings of the present study, we suggest that KIF3A be a new
candidate parameter of breast cancer.
The expression of KIF3A was associated with survival
in breast cancer patients up to 2013. Furthermore, Kaplan-Meier
survival curves showed positive (++) KIF3A combined with longer
survival according to the data of 2014. Based on the statistical
analysis on the relationship with existing parameters and KIF3A,
the high expression of KIF3A is associated with ER, AR, EGFR and
Ki-67. Concerning the associated parameters, ER, AR and Ki-67 are
regarded as a reference index to evaluate prognosis status. Of
these, ER and AR are selected from hormonic effect and Ki-67 is
based on cell cycle, while KIF3A is associated with the
pathological change of primary cilia. Therefore, we suggest KIF3A
can be used as a new parameter to evaluate prognosis in a novel
way.
In conclusion, the high expression of KIF3A is
associated with the progression of breast cancer. Furthermore, its
high expression is also associated with breast cancer prognosis
parameters ER, AR, EGFR and Ki-67. These results indicate that
KIF3A can be used as a diagnostic indicator, and also as a new
prognosis parameter to evaluate breast cancer considering its
particular function on the pathological change of primary
cilia.
Acknowledgements
We gratefully thank Professor Tao Yi for providing
technical support.
Funding
This study was supported by the National Major
Scientific and Technological Special Project for ‘Significant New
Drugs Development’ (2013zx09301304001).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
PX and SC carried out most of the experimental work,
performed the immunohistochemical staining of tissue chip. SC
analyzed the data. PX wrote the paper. All authors read and
approved the final manuscript.
Ethics approval and consent to
participate
This study was based on the samples of tissue
microarrays brought from Xinchao, Shanghai.
Consent for publication
All authors have agreed to submit the
manuscript.
Competing interests
All authors declares that they have no conflict of
interest.
References
|
1
|
Kolpakova-Hart E, Jinnin M, Hou B, Fukai N
and Olsen BR: Kinesin-2 controls development and patterning of the
vertebrate skeleton by Hedgehog- and Gli3-dependent mechanisms. Dev
Biol. 309:273–284. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Rosenbaum JL and Witman GB: Intraflagellar
transport. Nat Rev Mol Cell Biol. 3:813–825. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Hirokawa N: Kinesin and dynein superfamily
proteins and the mechanism of organelle transport. Science.
279:519–526. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Barakat MT, Humke EW and Scott MP: Kif3a
is necessary for initiation and maintenance of medulloblastoma.
Carcinogenesis. 34:1382–1392. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Liu Z, Rebowe RE, Wang Z, Li Y, Wang Z,
DePaolo JS, Guo J, Qian C and Liu W: KIF3a promotes proliferation
and invasion via Wnt signaling in advanced prostate cancer. Mol
Cancer Res. 12:491–503. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kim M, Suh YA, Oh JH, Lee BR, Kim J and
Jang SJ: KIF3A binds to β-arrestin for suppressing Wnt/β-catenin
signalling independently of primary cilia in lung cancer. Sci Rep.
6:327702016. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
McDermott KM, Liu BY, Tlsty TD and Pazour
GJ: Primary cilia regulate branching morphogenesis during mammary
gland development. Curr Biol. 20:731–737. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Menzl I, Lebeau L, Pandey R, Hassounah NB,
Li FW, Nagle R, Weihs K and McDermott KM: Loss of primary cilia
occurs early in breast cancer development. Cilia. 3:72014.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Yuan K, Frolova N, Xie Y, Wang D, Cook L,
Kwon YJ, Steg AD, Serra R and Frost AR: Primary cilia are decreased
in breast cancer: Analysis of a collection of human breast cancer
cell lines and tissues. J Histochem Cytochem. 58:857–870. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Hoang-Minh LB, Deleyrolle LP, Siebzehnrubl
D, Ugartemendia G, Futch H, Griffith B, Breunig JJ, De Leon G,
Mitchell DA, Semple-Rowland S, et al: Disruption of KIF3A in
patient-derived glioblastoma cells: Effects on ciliogenesis,
hedgehog sensitivity, and tumorigenesis. Oncotarget. 7:7029–7043.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Guo X, Macleod GT, Wellington A, Hu F,
Panchumarthi S, Schoenfield M, Marin L, Charlton MP, Atwood HL and
Zinsmaier KE: The GTPase dMiro is required for axonal transport of
mitochondria to Drosophila synapses. Neuron. 47:379–393. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ichinose S, Ogawa T and Hirokawa N:
Mechanism of Activity-Dependent Cargo Loading via the
Phosphorylation of KIF3A by PKA and CaMKIIa. Neuron. 87:1022–1035.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Qiu N, Xiao Z, Cao L, Buechel MM, David V,
Roan E and Quarles LD: Disruption of Kif3a in osteoblasts results
in defective bone formation and osteopenia. J Cell Sci.
125:1945–1957. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Jiang S, Chen G, Feng L, Jiang Z, Yu M,
Bao J and Tian W: Disruption of kif3a results in defective
osteoblastic differentiation in dental mesenchymal stem/precursor
cells via the Wnt signaling pathway. Mol Med Rep. 14:1891–1900.
2016. View Article : Google Scholar : PubMed/NCBI
|