Introduction
Pleural effusion is a common problem which manifests
in a wide range of local and systemic potentially life-threatening
diseases. Accurate diagnosis is difficult without resorting to
invasive procedures. In particular, diagnosis of malignant pleural
effusion presents a challenge since its differentiation from benign
effusion is often difficult using currently available parameters
derived from thoracosynthesis. Although essential for
distinguishing between a transudate and exudate (1), biochemical, microbiological and
cytological pleural fluid analyses have poor value for identifying
the cause of a pleural lymphocytic exudate (2). The sensitivity of cytological
examination of pleural fluid and blind needle biopsy, even when
combined together, is generally less than 75% (3–7).
Although there is a huge interest in biomarkers (cytokines, matrix
metalloproteinases, growth factors and tumor markers) for the
diagnosis of pleural effusions, their lack of sensitivity and
specificity limits their use. Moreover, there is a lack of accepted
and reliable diagnostic criteria particularly for malignancy based
on morphological imaging (CT and MR imaging) (8–10).
The development of inflammation in the pleura results in an
increased vascular permeability, and pleural liquid accumulation is
the result of increased fluid production and/or reduced lymph
drainage. This pleural fluid is enriched in proteins, inflammatory
cells and mediators (5,11). Cytokine-producing cells and
cytokines, such as the vascular endothelial growth factor (VEGF)
which is able to increase angiogenesis and enhance the permeability
of vascular endothelial cells (12,13),
are thought to be important in malignant pleural fluid formation
(14,15).
In malignant pleural effusion, neoplastic cells
infiltrate the pleural layer and growth progressively in the
pleural cavity.
Nerve growth factor (NGF), brain-derived
neurotrophic factor (BDNF), neurotrophin 3 (nT3) and neurotrophin 4
(nT4) comprise the mammalian neurotrophins (NTs), a family of
structurally related growth factors that play a crucial role in the
survival, development, differentiation, neurite outgrowth and
maintenance of a specific neuronal population in the nervous system
(16,17). They belong to a class of growth
factors, secreted proteins, which are capable of signaling
particular cells to survive, differentiate or grow mediated by two
classes of receptors, p75 and the ‘Trk’ family of tyrosine kinase
receptors.
Although classically known for their effects on
neurons, NTs are multifunctional growth factors and exert numerous
effects including differentiation of B-lymphocytes (18), histamine release from mast cells
(19), formation of
intramyocardial blood vessels (20) and growth of follicles in the
ovaries (21) on non-neuronal
cells, particularly in immunocompetent cells and lymphoid organs
(22). Interest in the NTs system
has grown particularly in regards to several lung diseases
(23–26). Under normal conditions, Trk B (the
physiological high-affinity receptor for BDNF) has been found to be
involved in the development and maintenance of the normal structure
of the lung (27,28). In addition, NTs play a role in the
modulation of certain human malignancies (29,30),
such as myeloma (31),
fibrosarcoma (32), hepatocellular
(33) and pancreatic (34) carcinoma as well as lung cancer
(35,36). More importantly, there is in
vitro evidence that compounds blocking NT signaling, such as
k252a, are able to block lung cancer cell progression (37). Yet, to date, the role of NTs in
malignant pleural effusion (38)
and in mesothelioma (39) has been
poorly investigated.
In the present study, we aimed to ascertain whether
determination of levels of four NTs (NGF, BDNF, nT3 and nT4) in
pleural fluid aids in identifying the etiology of non-neutrophilic
pleural effusions and, in particular, in differentiating malignant
from benign effusions.
Materials and methods
Patient selection
We conducted a prospective study, including 170
consecutive patients (mean age 66.4±13.4 years; range 18–96; 98
males and 72 females) who were treated at the Pneumology
Department, CHU, Liège, between 2004 and 2009. All patients
presented with an exudative pleural effusion for whom the
combination of chest X-ray, thoracic CT scanning (PQ 2000 4th
generation; Picker, Cleveland, OH, USA) and thoracocentesis failed
to provide an etiologic diagnosis. Therefore, the indication for
thoracoscopy was justified along with pleural biopsy. In the
chemical analysis, pleural effusion was considered to be an exudate
according to Light's criteria (1).
Thus, the pleural effusion had to meet at least one of the
following criteria: ratio of pleural fluid protein to serum protein
>0.5; ratio of pleural fluid lactic dehydrogenase (LDH) to serum
lactic dehydrogenase >0.6; pleural fluid lactic dehydrogenase
level greater than two-thirds of the upper limit of the serum
normal value. Neutrophilic pleurisy (>50% neutrophils) (2) and empyema were excluded from this
study. In our series thoracoscopy procedure allowed establishment
of a diagnosis in each case.
Pleural fluid analysis
A diagnostic thoracocentesis of the pleural fluid
(10 ml) was performed on each subject before thoracoscopy was
carried out. A first sample of 5 ml was subjected to routine
biochemical analysis, including tests for pleural protein, glucose,
LDH and amylase levels. A second sample of 5 ml was added to a tube
containing ethylenediamino-tetraic-potassium anticoagulant for
differential cell counting.
For NTs measurements, 20 ml of pleural fluid was
centrifuged at 400 x g for 10 min at 4°C. The supernatant was
separated from the cell pellet. The supernatant was immediately
stored at −70°C until the ELISA was performed.
NTs (BDNF, NGF, nT3 and nT4) levels were determined
according to the following commercially available enzyme-linked
immunosorbent assay (ELISA) kit (Duoset; R&D Systems Europe,
Abingdon, UK). The ELISA was validated by determination of the
assay sensitivity and spiking recovery. Assay sensitivity was
determined by calculating the mean response of 10 sets of blanks
and evaluating the mean plus 2 standard deviations on the standard
curve. The limit of detection was 5 pg/ml for BDNF, NGF and nT3 and
10 pg/ml for nT4. Spiking recovery was determined by adding 0, 7.5,
15.6, 31.2, 62.5, 125, 250 and 500 pg/ml of NTs to a pool of 10
pleural liquids. The recovery for BDNF, NGF, nT3 and nT4, at a
concentration of 62.5 pg/ml, was 99, 61, >96 and 80%,
respectively.
Etiologic diagnosis of pleural
exudate
The final diagnosis of the pleural effusion was
obtained by invasive pleural biopsy during a thoracoscopy. When a
diagnosis of benign disease was established, based on
histopathology, the patients were followed up for at least 18
months to ensure absence of a malignant pleural process. Benign
pleural effusions included both infectious (parapneumonic and
tuberculosis) and inflammatory pleural effusions. Malignant pleural
effusions were divided into three groups: i) pleural metastasis of
an extra-thoracic cancer, ii) pleural metastasis of a primary lung
cancer and iii) mesothelioma.
The size of the pleural effusion was estimated in
each patient by the total pleural fluid volume aspirated when
starting the thoracoscopy procedure.
The protocol was approved by the local ethics
committee, and informed consent was obtained from each subject
prior to the study.
Statistical analysis
All data were expressed as the median (range) levels
for pleural cell counts, pleural biochemical parameters and NTs.
Characteristics of pleural fluid and pleural cell counts in
malignant vs. benign pleural effusion were compared using the
non-parametric Mann-Whitney test. A Kruskall-Wallis analysis
(Dunn's multiple comparisons post-test) was used to compare pleural
neurotrophin levels in subgroups of malignant vs. benign pleural
effusions. To calculate correlations between variables, the
Spearman rank coefficient of correlation was used. The accuracy of
each pleural NT to distinguish malignant from benign pleural
lesions was calculated with receiver operating characteristic (ROC)
analyses. A p-value <0.05 was considered statistically
significant.
Results
Clinical diagnosis
Thoracoscopic biopsies indicated benign pleural
lesions in 59 patients and malignant pleural effusions in 111.
Demographic characteristics and pleural effusion etiologies are
provided in Table I. The gender
ratio was different with females accounting for 45% of the
malignant group, while only representing 36% of the benign group
(NS).
 | Table I.Demographic characteristics and
etiologies of the patients with malignant or benign pleural
effusions. |
Table I.
Demographic characteristics and
etiologies of the patients with malignant or benign pleural
effusions.
Benign pleural
effusions
|
| Age (years) | 68±13 |
| Gender (M/F) | 38/21 |
| Etiology |
| Infectious
pleurisies (n=9) |
| 6 parapneumonic
pleurisies |
| 3
tuberculosis |
| Inflammatory
pleurisies (n=50) |
| 1 Dressler's
syndrome |
| 2 chronic
pancreatitis |
| 3 heart
failures |
| 1
post-radic |
| 6 benign
asbestos |
| 1 uremic |
| 1
drug-induced |
| 1
post-traumatic |
| 3 connective
tissue diseases |
| 2 rheumatoid
arthritis |
| 1
scleroderma |
| 40 non-specific
chronic inflammatory changes |
|
Malignant pleural
effusions
|
| Age (years) | 65±14 |
| Gender (M/F) | 61/50 |
| Etiology |
| Pleural
metastases of extrathoracic tumors (n=50) |
| 18 breast
cancers |
| 5 ovarian
cancers |
| 5 kidney
cancers |
| 7 pancreatic
cancers |
| 4 colic
tumors |
| 2 rectal
carcinomas |
| 2 prostatic
carcinomas |
| 2
lymphomas |
| 1 skin
cancer |
| 1 genital
carcinoma |
| 1 acute
leukemia |
| 1 laryngeal
cancer |
| 1 unknown
primary |
| Pleural
metastases of lung cancer (n=51) |
| 11 squamous
non-small-cell carcinomas |
| 31
adenocarcinomas |
| 5 large-cell
carcinomas |
| 2 sarcomas |
| 2 small-cell
lung cancers |
| Mesothelioma
(n=10) |
Pleural cell counts and biochemical
parameters
Biochemical and cytological characteristics of the
pleural effusions are provided in Table II. There was no significant
difference in pleural protein, LDH, glucose and amylase level and
in protein Light's ratio between the malignant and benign pleural
effusions. However, LDH Light's ratio was significantly higher in
the malignant effusions (p<0.05) (Table II). There was no significant
difference in pleural cell counts between the benign and malignant
effusions (Table II).
| Table II.Pleural cell counts and biochemical
parameters in the malignant and benign pleural effusions. |
Table II.
Pleural cell counts and biochemical
parameters in the malignant and benign pleural effusions.
| Benign pleural
effusions (n=59) | Malignant pleural
effusions (n=111) |
|---|
|
RBC/mm3 | 2,515
(40–720,000) | 4,640
(0–1,840,000) |
|
WBC/mm3 | 710
(85–14,920) | 600 (4–10,000) |
| Neutrophils
(%) | 6 (0–47) | 11 (0–49) |
| Lymphocytes
(%) | 62 (3–98) | 52 (0–100) |
| Reticulo/monocytes
(%) | 15 (0–83) | 22 (0–94) |
| Eosinophils
(%) | 2 (0–73) | 1 (0–43) |
| Proteins (g/l) | 42 (20–62.9) | 41.3 (10–68.3) |
| LDH (UI/l) | 420
(286–1,735) | 551
(120–6,512) |
| Amylase (UI/l) | 39 (12–22,540) | 37.5 (4–903) |
| Glucose (g/l) | 0.90
(0.02–1.94) | 0.84
(0.14–2.73) |
| Protein Pl/blood
ratio | 0.60
(0.28–0.88) | 0.62 (0–1.16) |
| LDH Pl/blood
ratio | 0.94 (0.15–33) | 1.40 (0–27)a |
None of the pleural samples showed a positive
bacterial growth during the culture, even when the pleural effusion
was deemed to be of infectious origin.
Determination of neurotrophins in pleural
effusions
The median level of pleural BDNF was 17 pg/ml
(0–367) in patients with malignant pleural effusions, which was
significantly higher compared to the value of 8 pg/ml (0–51) found
in benign effusions (p<0.05) (Table
III). By contrast, no significant difference was found in NGF
and nT3 pleural levels between malignant and benign effusions
(Table III). nT3 was only observed
in 13.5% of the 170 pleural effusions, including 8 and 16% of
benign and malignant effusions, respectively (NS). nT4 was
undetectable with the exception of 1 patient with pleural
metastasis of squamous lung carcinoma.
| Table III.Comparison of pleural neurotrophin
levels in benign and malignant pleural effusions. |
Table III.
Comparison of pleural neurotrophin
levels in benign and malignant pleural effusions.
| Pleural
neurotrophins | Benign pleurisy
(n=59) | Malignant pleurisy
(n=111) |
|---|
| BDNF (pg/ml) | 8 (0–51) | 17 (0–367)a |
| NGF (pg/ml) | 0 (0–120.3) | 0 (0–376) |
| nT3 (pg/ml) | 0 (0–43) | 0 (0–137) |
| nT4 (pg/ml) | 0 (0-0) | 0 (0–28) |
Pleural BDNF levels were positively correlated with
pleural red cell counts (r=0.29, p<0.001), pleural neutrophil
counts (r=0.16, p<0.05) and with pleural effusion volume
(r=0.19, p<0.05). BDNF was negatively correlated with pleural
eosinophil counts (r=−0.22, p<0.05) and pleural glucose
(r=−0.22, p<0.01). No correlation was found with total pleural
protein levels (r=−0.10, p>0.05).
ROC curve of BDNF for distinguishing between
malignant and benign effusions is presented in Fig. 1. Only the measurement of BDNF
showed significant value in identifying malignant effusions with an
area under the curve (AUC) of 0.609 (p<0.05). Derived from this
curve, the best cut-off point was found to be 44 pg/ml which gave a
sensitivity, a specificity and an accuracy of 24, 99 and 50%,
respectively. Sensitivities and specificities for different cut-off
values for distinguishing benign from malignant pleurisies are
presented in Table IV.
| Table IV.Sensitivities, specificities,
negative predictive value (NPV) and positive predictive value (PPV)
for different cut-off values derived from ROC curves of BDNF for
distinguishing benign from malignant pleurisies. |
Table IV.
Sensitivities, specificities,
negative predictive value (NPV) and positive predictive value (PPV)
for different cut-off values derived from ROC curves of BDNF for
distinguishing benign from malignant pleurisies.
| Cut-off
(pg/ml) | Sensitivity
(%) | Specificity
(%) | NPV (%) | PPV (%) |
|---|
| 10 | 63 | 54 | 44 | 72 |
| 15 | 53 | 68 | 43 | 76 |
| 20 | 47 | 71 | 39 | 73 |
| 25 | 39 | 71 | 39 | 73 |
| 30 | 39 | 75 | 39 | 73 |
| 35 | 33 | 81 | 39 | 77 |
| 40 | 28 | 91 | 41 | 86 |
| 45 | 24 | 98 | 41 | 96 |
| 50 | 17 | 98 | 39 | 95 |
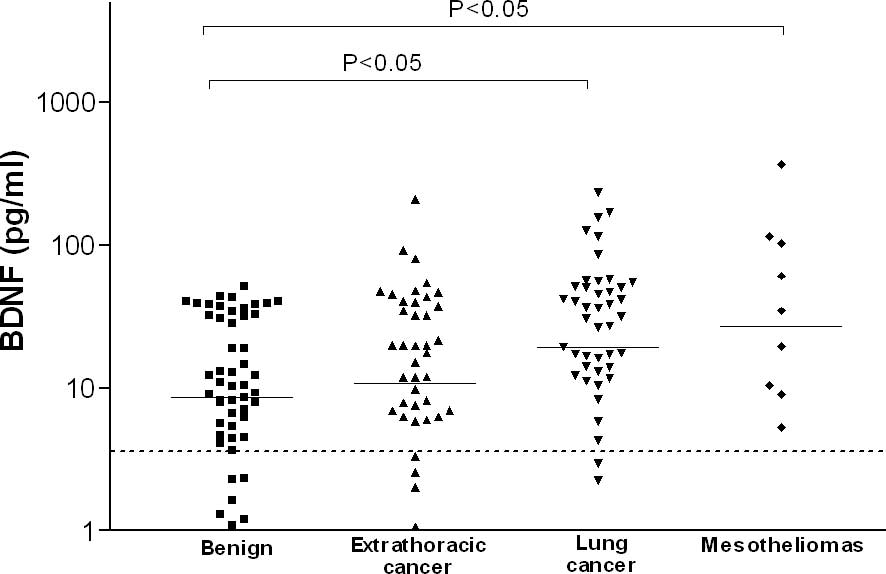
Regarding different subgroups of malignant and
benign pleural effusions, a significant difference in pleural BDNF
levels was noted, which was significantly higher in pleural
metastasis of lung cancer and in mesothelioma when compared to
benign effusions [19 pg/ml (0–232) and 27 pg/ml (0–367) vs. 8 pg/ml
(0–51), respectively, p<0.05] (Fig.
2). ROC analysis showed BDNF may help to distinguish between
pleural metastasis of lung cancer and benign effusion (AUC=0.664,
p<0.01; 72 and 59% for sensitivity and specificity,
respectively, for best threshold of 11 pg/ml), and between pleural
metastasis of lung and extrathoracic cancers (AUC=0.613, p<0.05;
69 and 56% for sensitivity and specificity, respectively, for best
threshold of 12 pg/ml) (Table V).
Finally, there was a strong trend for BDNF to identifying
mesothelioma from benign effusion (AUC=0.703, p=0.055; 40 and 100%
for sensitivity and specificity, respectively, for best threshold
of 51 pg/ml). We found no significant difference in the four
neurotrophin levels according to the etiology of the benign pleural
effusions [infectious (n= 9) vs. inflammatory (n=50)].
| Table V.Receiving operating characteristics
(ROC) curves of BDNF for distinguishing between the subgroups of
pleural effusions. |
Table V.
Receiving operating characteristics
(ROC) curves of BDNF for distinguishing between the subgroups of
pleural effusions.
| AUC | p-value | Cut-off
(pg/ml) | Sensitivity | Specificity |
|---|
| Lung cancer pleural
metastasis vs. benign pleurisy | 0.664 | 0.002 | 11 | 72 | 59 |
| Lung cancer vs.
extrathoracic tumor pleural metastasis | 0.613 | 0.040 | 12 | 69 | 56 |
| Lung cancer pleural
metastasis vs. mesothelioma | 0.516 | 0.590 | 57 | 40 | 88 |
| Extrathoracic tumor
pleural metastasis vs. benign pleurisy | 0.534 | 0.550 | 43 | 18 | 97 |
| Extrathoracic tumor
pleural metastasis vs. mesothelioma | 0.661 | 0.130 | 55 | 40 | 94 |
| Mesothelioma vs.
benign pleurisy | 0.703 | 0.055 | 51 | 40 | 100 |
In malignant pleural effusions, pleural nT3
concentrations were observed in 10% of pleural metastasis of
extrathoracic cancer, in 10% of mesothelioma and in 23.5% of
pleural metastasis of primary lung cancer (NS). In this last
subgroup, a higher proportion of pleural nT3 was detected in
squamous cell carcinoma in comparison to that in non-squamous cell
carcinoma (72.7 vs. 10%, p<0.0001) (Fig. 3).
Discussion
The aim of the present study was to assess the
levels of NTs in pleural effusion where etiology was not obvious.
The present study demonstrated for the first time in a large and
well-characterized population of patients with non-neutrophilic
exudates that, even though the pleural BDNF level was higher in
malignant pleural effusions, it exhibited a rather limited clinical
value in distinguishing between malignant and benign pleural
effusions.
ROC curve analysis indicated that BDNF at a
concentration of 44 pg/ml yields the best compromise between
sensitivity and specificity, although we recognize it to be fairly
modest as a diagnostic tool due to a low sensitivity (24%).
However, this can be compared to what is usually found with chest
CT scanner which has a sensitivity that may range from 22 to 35%
according to the morphological chosen criteria (40), while specificity is around 80%.
Even though several NTs were reported to influence
extrathoracic neoplastic cell differentiation and growth (29–32,41),
in our study only BDNF levels were found to be significantly
increased in malignant effusions. Moreover, these increased levels
were essentially due to lung cancer pleural metastasis and
mesothelioma.
Our study confirms in a larger series of patients
the results of Ricci et al who reported significantly higher
concentrations of BDNF in malignant pleural effusions in comparison
to inflammatory exudates and transudates (38).
The reason why BDNF is increased in malignant
effusions is not clear. Although we cannot exclude that increased
BDNF levels may partly be related to increased pleural endothelial
permeability, the lack of correlation between pleural BDNF and
protein levels suggests that there may be additional mechanisms
involved. Local production of BDNF by mesothelial cells, recruited
inflammatory and malignant cells is likely to contribute to the
increased levels found in malignant effusions and points to the
existence of an autocrine and/or paracrine mechanism (35,36,38).
Although we excluded pleural fluids with high neutrophil counts
(>50%), we found a significant correlation between neutrophil
counts and BDNF suggesting that recruited neutrophils may
contribute together with tumoral cells to local BDNF
production.
In contrast, the absence of a correlation between
pleural LDH, a marker of tumor activity, and BDNF supports the
hypothesis that pleural BDNF levels may not be directly related to
tumor growth itself, but rather to an interaction between malignant
cells and local mesenchymal or inflammatory cells. The significant
relationship between the volume of pleural effusion and BDNF is in
keeping with the role of this NT in controlling pleural fluid
homeostasis (35,38). Implication of BDNF in vascular
permeability regulation is further supported by the recognition of
its involvement in cerebral edema and subsequent neuronal tissue
damage (42).
Immunohistochemical analysis showed that Trk B
receptors, the BDNF receptors, were expressed in several neoplastic
cells, fibroblasts and blood vessels (21,35).
Activation of Trk B receptors may be a key mechanism in tumor cell
survival after detachment from extracellular matrix (a process
called ‘anoikis’) (43). The
particularly elevated levels of BDNF in malignant pleural fluid
from lung cancer cells known to express high level of Trk B
receptors (36) may cause a more
aggressive pleural invasion as compared to extrathoracic tumors.
Notably, an inverse relationship was found between pleural glucose
and BDNF levels. This supports the idea that BDNF is increased when
metabolic activity of the pleura is intense as in tumor cell
proliferation (44,45). Additionally, a strong correlation
was found between pleural red cell counts and BDNF levels which is
in line with the role of BDNF in pleural neoangiogenesis, a
phenomenon critical for tumor proliferation.
In contrast to BDNF, neither NGF nor nT3 were found
to be significantly increased in pleural effusion of malignancies.
Furthermore, nT3 pleural levels were only detected in 13.5% of all
pleurisies, with a trend to a higher percentage of detection in
malignant pleurisies (16%) vs. benign effusion (8%). Pleural nT3
level was observed in the majority of squamous cell lung carcinoma
(73% of cases) which sharply contrasts to what was observed in
other types of lung cancer histology (∼10%). Our data corroborate
those reported by Ricci et al for lung surgical samples
(36).
NGF has been reported to be more commonly a
regulator of differentiation and/or survival than a cancer cell
growth factor (38).
Down-regulation of NGF has even been demonstrated in aggressive
human malignancies (46). In light
of this view, we find no surprise that NGF levels were not
increased in the malignant pleural effusions.
In conclusion, albeit of a limited diagnosis value,
our results demonstrated in a large patient series that malignant
pleural effusions display increased BDNF levels which may
contribute to the local growth and invasiveness of tumors. This may
offer a novel target in the treatment strategy for malignant
pleural diseases.
References
|
1.
|
Light RW, Macgregor MI, Luchsinger PC and
Ball WC Jr: Pleural effusions: the diagnostic separation of
transudates and exudates. Ann Intern Med. 77:507–513. 1972.
View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Light RW, Erozan YS and Ball WC Jr: Cells
in pleural fluid. their value in differential diagnosis. Arch
Intern Med. 132:854–860. 1973. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Poe RH, Israel RH, Utell MJ, Hall WJ,
Greenblatt DW and Kallay MC: Sensitivity, specificity, and
predictive values of closed pleural biopsy. Arch Intern Med.
144:325–328. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Prakash UB and Reiman HM: Comparison of
needle biopsy with cytologic analysis for the evaluation of pleural
effusion: analysis of 414 cases. Mayo Clin Proc. 60:158–164. 1985.
View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Sahn SA: State of the art. The pleura. Am
Rev Respir Dis. 138:184–234. 1988.PubMed/NCBI
|
|
6.
|
Schönfeld N and Loddenkemper R: Pleural
biopsy and thoracoscopy. Eur Respi Mon. 9:135–152. 1998.
|
|
7.
|
Von Hoff DD and LiVolsi V: Diagnostic
reliability of needle biopsy of the parietal pleura. A review of
272 biopsies. Am J Clin Pathol. 64:200–203. 1975.PubMed/NCBI
|
|
8.
|
Dedrick CG, McLoud TC, Shepard JA and
Shipley RT: Computed tomography of localized pleural mesothelioma.
AJR Am J Roentgenol. 144:275–280. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Leung AN, Muller NL and Miller RR: CT in
differential diagnosis of diffuse pleural disease. AJR Am J
Roentgenol. 154:487–492. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Sahn SA: Malignant pleural effusions. Clin
Chest Med. 6:113–125. 1985.
|
|
11.
|
Antony VB, Godbey SW, Kunkel SL, Hott JW,
Hartman DL, Burdick MD and Strieter RM: Recruitment of inflammatory
cells to the pleural space. chemotactic cytokines, IL-8 and
monocyte chemotactic peptide-1 in human pleural fluids. J Immunol.
151:7216–7223. 1993.PubMed/NCBI
|
|
12.
|
Ferrara N and Henzel WJ: Pituitary
follicular cells secrete a novel heparin-binding growth factor
specific for vascular endothelial cells. Biochem Biophys Res
Commun. 161:851–858. 1989. View Article : Google Scholar
|
|
13.
|
Senger DR, Galli SJ, Dvorak AM, Perruzzi
CA, Harvey VS and Dvorak HF: Tumor cells secrete a vascular
permeability factor that promotes accumulation of ascites fluid.
Science. 219:983–985. 1983. View Article : Google Scholar
|
|
14.
|
Duysinx BC, Corhay JL, Hubin L, Nguyen D,
Henket M and Louis R: Diagnostic value of interleukine-6,
transforming growth factor-beta 1 and vascular endothelial growth
factor in malignant pleural effusions. Respir Med. 102:1708–1714.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Thickett DR, Armstrong L and Millar AB:
Vascular endothelial growth factor (VEGF) in inflammatory and
malignant pleural effusions. Thorax. 54:707–710. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Allen SJ and Dawbarn D: Clinical relevance
of the neurotrophins and their receptors. Clin Sci. 110:175–191.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
17.
|
Bibel M and Barde YA: Neurotrophins: key
regulators of cell fate and cell shape in the vertebrate nervous
system. Genes Dev. 14:2919–2937. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
18.
|
Otten U, Ehrhard P and Peck R: Nerve
growth factor induces growth and differentiation of human B
lymphocytes. Proc Natl Acad Sci USA. 86:10059–10063. 1989.
View Article : Google Scholar : PubMed/NCBI
|
|
19.
|
Nassenstein C, Braun A, Nockher WA and
Renz H: Neurotrophin effects on eosinophils in allergic
inflammation. Curr Allergy Asthma Rep. 5:204–211. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
20.
|
Wagner N, Wagner KD, Theres H, Englert C,
Schedl A and Scholz H: Coronary vessel development requires
activation of the TrkB neurotrophin receptor by the Wilms' tumor
transcription factor Wt1. Genes Dev. 19:2631–2642. 2005.PubMed/NCBI
|
|
21.
|
Paredes A, Romero C, Dissen GA, et al:
TrkB receptors are required for follicular growth and oocyte
survival in the mammalian ovary. Dev Biol. 267:430–449. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
22.
|
Vega JA, Garcia-Suarez O and Germana A:
Vertebrate thymus and the neurotrophin system. Int Rev Cytol.
237:155–204. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
23.
|
Dagnell C, Grunewald J, Idali F, et al:
Increased levels of nerve growth factor in the airways of patients
with sarcoidosis. J Intern Med. 264:463–471. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
24.
|
Fox AJ, Patel HJ, Barnes PJ and Belvisi
MG: Release of nerve growth factor by human pulmonary epithelial
cells: role in airway inflammatory diseases. Eur J Pharmacol.
424:159–162. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
25.
|
Freund-Michel V and Frossard N:
Overexpression of functional TrkA receptors after internalisation
in human airway smooth muscle cells. Biochim Biophys Acta.
1783:1964–1971. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
26.
|
Ricci A, Graziano P, Bronzetti E, et al:
Increased pulmonary neurotrophin protein expression in idiopathic
interstitial pneumonias. Sarcoidosis Vasc Diffuse Lung Dis.
24:13–23. 2007.PubMed/NCBI
|
|
27.
|
Garcia-Suarez O, Perez-Pinera P, Laura R,
et al: TrkB is necessary for the normal development of the lung.
Respir Physiol Neurobiol. 167:281–291. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
28.
|
Prakash Y, Thompson MA, Meuchel L,
Pabelick CM, Mantilla CB, Zaidi S and Martin RJ: Neurotrophins in
lung health and disease. Expert Rev Respir Med. 4:395–411. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
29.
|
Fanburg-Smith JC and Miettinen M:
Low-affinity nerve growth factor receptor (P75) in
dermatofibrosarcoma protuberans and other nonneural tumors: a study
of 1,150 tumors and fetal and adult normal tissues. Hum Pathol.
32:976–983. 2001. View Article : Google Scholar
|
|
30.
|
Kruttgen A, Schneider I and Weis J: The
dark side of the NGF family: neurotrophins in neoplasias. Brain
Pathol. 16:304–310. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
31.
|
Pearse RN, Swendeman SL, Li Y, Rafii D and
Hempstead BL: A neurotrophin axis in myeloma: TrkB and BDNF promote
tumor-cell survival. Blood. 105:4429–4436. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
32.
|
Knezevich SR, McFadden DE, Tao W, Lim JF
and Sorensen PH: A novel ETV6-NTRK3 gene fusion in congenital
fibrosarcoma. Nat Genet. 18:184–187. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
33.
|
Yang ZF, Ho DW, Lam CT, et al:
Identification of brain-derived neurotrophic factor as a novel
functional protein in hepatocellular carcinoma. Cancer Res.
65:219–225. 2005.PubMed/NCBI
|
|
34.
|
Okada Y, Eibl G, Guha S, Duffy JP, Reber
HA and Hines OJ: Nerve growth factor stimulates MMP-2 expression
and activity and increases invasion by human pancreatic cancer
cells. Clin Exp Metastasis. 21:285–292. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
35.
|
Hoyle GW: Neurotrophins and lung disease.
Cytokine Growth Factor Rev. 14:551–558. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
36.
|
Ricci A, Greco S, Mariotta S, et al:
Neurotrophins and neurotrophin receptors in human lung cancer. Am J
Respir Cell Mol Biol. 25:439–446. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
37.
|
Perez-Pinera P, Hernandez T, Garcia-Suarez
O, et al: The Trk tyrosine kinase inhibitor K252a regulates growth
of lung adenocarcinomas. Mol Cell Biochem. 295:19–26. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
38.
|
Ricci A, Mariotta S, Pompili E, et al:
Neurotrophin system activation in pleural effusions. Growth
Factors. 28:221–231. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
39.
|
Davidson B, Reich R, Lazarovici P, et al:
Expression of the nerve growth factor receptors TrkA and P75 in
malignant mesothelioma. Lung Cancer. 44:159–165. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
40.
|
Yilmaz U, Polat G, Sahin N, Soy O and
Gulay U: CT in differential diagnosis of benign and malignant
pleural disease. Monaldi Arch Chest Dis. 63:17–22. 2005.PubMed/NCBI
|
|
41.
|
Davidson B, Reich R, Lazarovici P, et al:
Expression and activation of the nerve growth factor receptor TrkA
in serous ovarian carcinoma. Clin Cancer Res. 9:2248–2259.
2003.PubMed/NCBI
|
|
42.
|
Janis LS and Stein DG: Intraseptal
injections of NGF attenuates edema formation following septal
lesions in the rat. Neurosci Lett. 214:21–24. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
43.
|
Douma S, van Laar T, Zevenhoven J,
Meuwissen R, van Garderen E and Peeper DS: Suppression of anoikis
and induction of metastasis by the neurotrophic receptor TrkB.
Nature. 430:1034–1039. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
44.
|
Duysinx B, Nguyen D, Louis R, Cataldo D,
Belhocine T, Bartsch P and Bury T: Evaluation of pleural disease
with 18-fluorodeoxyglucose positron emission tomography imaging.
Chest. 125:489–493. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
45.
|
Gupta NC, Rogers JS, Graeber GM, et al:
Clinical role of F-18 fluorodeoxyglucose positron emission
tomography imaging in patients with lung cancer and suspected
malignant pleural effusion. Chest. 122:1918–1924. 2002. View Article : Google Scholar
|
|
46.
|
Zhu ZW, Friess H, Wang L, Di Mola FF,
Zimmermann A and Buchler MW: Down-regulation of nerve growth factor
in poorly differentiated and advanced human esophageal cancer.
Anticancer Res. 20:125–132. 2000.PubMed/NCBI
|