Introduction
In various competitive sports, the importance of
recovery in training has become evident, and nutrition is
considered to play a major role. In recent years, supplements such
as amino acids have been used after training.
Wheat gluten hydrolysate (WGH), one of these
supplements, has attracted attention. WGH is a peptide prepared by
enzymatic treatment of wheat gluten; it has excellent
dispersibility and dissolution properties and is used as a
glutamine-enriching ingredient in enteral nutrients (for what is
known as immunonutrition) that are used perioperatively (1). In the field of sports, investigations
have been conducted on the effects of WGH on endurance exercise
(2–4) and weight training (4,5).
Koikawa et al reported that post-exercise consumption of WGH
suppressed subsequent muscle injury, as indicated by serum creatine
kinase (CK) activity (2) and the
effect was reproduced in a larger randomized control trial
(3). Similar results were also
obtained by pre-ingestion of WGH in weight training (5).
On the other hand, there have been no studies
concerning its effects on training in ball games, which involves
more complex movement. Among ball games, soccer involves complex
instantaneous movements that are repeatedly performed. In the
present study, we report on our investigation of the effects of WGH
consumption on muscle injury from soccer training in soccer players
in a double-blind crossover study.
Materials and methods
Subjects
Eight male soccer players belonging to a college
soccer club were enrolled in the study. They had a history of
competitive athletics since high school and were capable in
college-level competition. They were given thorough explanation of
the objectives, methods and ethical considerations of the study and
provided written consent for participation. After completion of the
exercise protocols, two subjects were excluded from the data
analyses since one presented with an elevated activity in serum
creatine kinase >1000 U/l due to a possible slight distortion
and the other subject was affected by a upper respiratory
infection. Characteristics of the remaining six subjects are
documented in Table I.
 | Table I.Characteristics of the subjects. |
Table I.
Characteristics of the subjects.
| Subjects
| |
|---|
| Characteristics | A | B | C | D | E | F | Mean ± SD |
|---|
| Age (years) | 19 | 20 | 19 | 19 | 19 | 19 | 19.2±0.4 |
| Height (cm) | 173.0 | 181.0 | 179.0 | 175.0 | 172.0 | 169.0 | 174.8±4.49 |
| Body weight (kg) | 62.0 | 76.0 | 73.0 | 75.0 | 71.0 | 65.0 | 70.3±5.65 |
| Soccer
positiona | MF | FW | MF | MF | DF | MF | |
| History of
competition (years) | 10 | 14 | 13 | 13 | 13 | 11 | 12.3±1.5 |
Study supplement
The test supplement in the form of a granulated
powder containing 6.0 g of WGH per packet was used. Other
ingredients included anhydrous glucose, anhydrous citric acid,
sweetener (sucralose), fragrance (lemon micron) and thickener
(pullulan). The placebo contained water soluble fiber (6.0 g)
instead of WGH, with other ingredients being the same. Supplements
were packaged in aluminum packets sealed on three sides, each
containing 9 g per packet. Test and placebo supplements were
prepared by Nisshin Pharma, Inc. (Tokyo, Japan). The detailed
ingredients are listed in Table
II.
| Table II.Composition of the supplement (per 9-g
packet). |
Table II.
Composition of the supplement (per 9-g
packet).
| Supplement | Ingredient | Content (g) |
|---|
| Test | Wheat gluten
hydrolysate | 6 |
| Anhydrous
glucose | 2 |
| Anhydrous citric
acid | 0.9 |
| Sucralose (as
sweetener) | 0.016 |
| Lemon flavor | 0.084 |
| Pullulan (as
thickener) | 0.135 |
| Placebo | Polydextrose | 6 |
| Anhydrous
glucose | 2 |
| Anhydrous citric
acid | 0.9 |
| Sucralose (as
sweetener) | 0.016 |
| Lemon flavor | 0.084 |
| Pullulan (as
thickener) | 0.135 |
Study design
A double-blind crossover method was used in this
study, with the subjects randomized into two groups. For the first
round of the study, subjects were divided into one group who
consumed WGH and another group who consumed the placebo (3 subjects
in the WGH group and 3 subjects in the placebo group). In the
second round, study supplements were alternated (3 subjects in the
WGH group and 3 subjects in the placebo group).
Under the direction of the team coach, subjects
trained four-on-four on half a soccer field (43 m × 28.5 m) by
playing six sets of 5-min mini-games. There was a 3-min rest
between each set. Immediately after exercise stress, subjects
consumed either 3 packets of test or placebo supplement. In
addition, health and dietary surveys were conducted for the period
starting one day before until the day after exercise stress.
Subjects completed the health survey, which was in question and
answer form and included items such as physical subjective
condition, body weight, body temperature and bowel movements. For
the dietary survey, subjects answered questions on the content and
quantity of food consumed, and took photographs; nutritional intake
was calculated based on this information.
Blood samples were taken at rest before exercise
stress, immediately after exercise stress, and at 12 h after
exercise stress and serum creatine kinase (CK), lactate
dehydrogenase (LDH), aspartate aminotransferase (AST), alanine
transaminase (ALT) and white blood cell count (WBC) levels were
measured. SRL (Tokyo) conducted the analyses.
A one-week washout period was established at the end
of the first round of experiments. The supplements consumed by the
subjects were switched and the second round of experiments was
conducted. During the study period, with the exception of the
exercise stress established by the study, subjects were forbidden
from high intensity training associated with muscle injury. This
study was reviewed and approved by the Ethics Committee of the
Juntendo University School of Health and Sports Science.
Statistical analysis
Following ANOVA, Dunnett's method was used to
compare data before exercise, immediately after exercise and at 12
h after exercise, with the pre-exercise data used as a control. A
paired t-test was used to compare corrected CK levels (with
post-exercise levels expressed as 100) with levels at 12 h after
exercise in the WGH and placebo groups. The risk ratio was set at
<5%. SPSS ver. 19.0 (IBM, Chicago, IL) was used to analyze the
data.
Results
The results of the health, training and dietary
surveys during the study period showed no significant differences
between the WGH and placebo groups, and there were no results that
had an effect on the study findings (data not shown).
Alterations in blood parameters prior to and after
exercise are summarized in Table
III. Significant increases in serum CK and LDH were observed in
both groups after exercise when compared with pre-exercise levels.
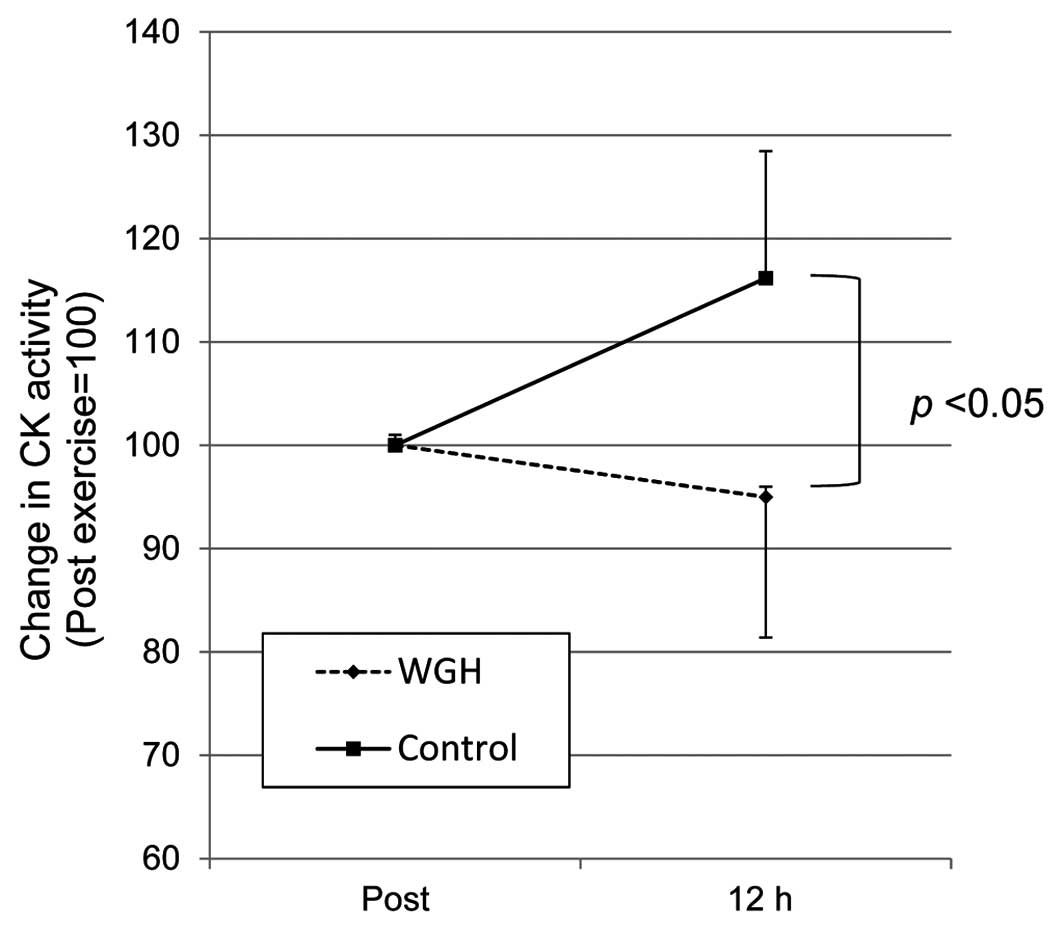
In the control group, the serum CK level was significantly higher
post exercise than the level prior to exercise, and the CK level
was even higher at 12 h after exercise. When CK activity was
adjusted by the level after exercise expressed as 100, a
significant (p<0.05) difference was observed between the groups
at 12 h after exercise; these levels were 95.0±14.9 and 116.2±13.9
in the WGH and placebo groups, respectively (Fig. 1). On the other hand, LDH, ALT and
AST activities returned to pre-exercise levels at 12 h after
exercise with no differences between groups. WBC count was elevated
after exercise and returned to pre-exercise levels in both groups.
No correlation was found in post-exercise WBC levels and CK
activities after 12 h.
| Table III.Alterations in the blood activity
prior to and post soccer exercise training. |
Table III.
Alterations in the blood activity
prior to and post soccer exercise training.
| Group | CK (U/l) | AST (U/l) | ALT (U/l) | LDH (U/l) | WBC
(103/μl) |
|---|
| WGH | | | | | |
| Pre-exercise | 284.3±51.8a | 22.5±2.4b | 19.5±2.4 | 191.5±22.1c | 5.7±1.0 |
| Post-exercise | 362.0±37.0 | 26.8±2.6 | 21.2±2.4 | 235.0±21.4 | 7.6±2.4 |
| 12 h after
exercise | 343.3±56.3 | 23.5±2.8 | 18.3±3.0 | 206.3±11.5 | 6.1±1.0 |
| Control | | | | | |
| Pre-exercise |
177.5±35.1c,d | 20.2±2.0 | 17.7±4.8 | 178.3±14.3c | 6.1±0.9 |
| Post-exercise | 249.5±30.5 | 24.0±2.3 | 19.0±4.6 | 224.2±16.3 | 8.2±1.5 |
| 12 h after
exercise | 287.8±33.2 | 18.0±4.0 | 17.2±3.7 | 188.2±10.5 | 6.2±0.7 |
Discussion
Soccer is characterized by repeated sprints and
stops, and the endurance to run for an entire 90-min game is also
important. The soccer training employed in this study took place on
half a soccer field, and consisted of repeated sprints and stops
conducted based on adequate instructions by the team coach. This
type of soccer training is similar to an actual game format.
Previously, we investigated the suppressive effects of WGH on
muscle injury due to endurance exercise (2–4)
including half-marathons (3) and
from strength training (5) using
elevation of CK activity as an indicator. In the present study, we
investigated the effect on exercise stress from ball games. After
mini-games, CK and LDH levels were higher than pre-exercise levels,
thus confirming that muscle injury had occurred. On the other hand,
there were no distinct increases in ALT or AST levels. AST is
mainly present in cardiac muscle, liver, skeletal muscle and the
kidneys, while ALT is present in the liver, followed by kidneys and
other tissues. Therefore, injury resulting from mini-game
activities would be less evident than with CK and LDH, which exist
in abundance in skeletal muscle. Consequently, it is clear that
muscle injury due to the mini-game was not sufficiently severe to
show a significant difference in ALT or AST levels.
Serum CK is known to peak 24–48 h after exercise
stress, which is due to delayed-onset muscle injury accompanied by
inflammation (5). The fact that CK
levels were higher at 12 h after exercise than immediately after
exercise in the control group confirms that delayed-onset muscle
injury also occurred in the present study. On the other hand, in
the WGH group, 12 h after exercise, the mean levels were lower than
they were immediately after exercise, at a level at which there
were no statistically significant differences with pre-exercise
levels. These results are in accordance with those in investigation
of distance running (2–4) and showed that consumption of WGH
after exercise stress suppresses subsequent delayed-onset muscle
injury. In fact, when CK levels were normalized by values after
exercise stress expressed as 100, there was a significant
difference in comparison with the control group.
Inflammation plays a role in the post-exercise
increase in CK activity. Paulsen et al reported a positive
correlation bewteen post-exercise leukocyte count and CK activity
(6). Koikawa et al
suggested that the post-exercise WBC count could predict the peak
CK activity after exercise (2). In
contrast, in the present study, the WBC count did not show a
significant correlation. The WBC count after the mini-game
increased but the levels were within the reference range (Table III). This could be the reason that
the correlation was not apparent.
Ball games such as soccer frequently involve a
series of competitions, including league games and post-games, and
post-training recovery is crucial for improving competitive power.
As a result, post-exercise consumption of WGH may be useful as it
enables quick recovery.
However, the present study only investigated serum
CK kinetics in one training session, and it is necessary to
investigate the kinetics over a series of training sessions.
Additionally, in the present study, muscle injury was evaluated
based on serum CK dynamics, but to evaluate recovery or
overcompensation, evaluation from a more functional perspective
such as muscle strength, is also necessary.
In conclusion, consumption of WGH after soccer
training inhibited the release of CK into the blood for 12 h after
exercise stress. Thus, consumption of WGH after exercise appears to
suppress subsequent delayed-onset muscle injury and to accelerate
recovery.
Acknowledgements
This study was supported, in part, by
Nisshin Pharma, Inc., which was the manufacturer of the wheat
gluten hydrolysate supplement used in this study. A section of this
study was presented at the 18th Annual Meeting of the Japanese
Society of Clinical Medicine in 2007.
References
|
1.
|
Sawaki K, Takaoka I, Sakuraba K and Suzuki
Y: Effect of distance running and subsequent intake of glutamine
rich peptide on biomedical parameters of male Japanese athletes.
Nutr Res. 24:59–71. 2004. View Article : Google Scholar
|
|
2.
|
Koikawa N, Nakamura A, Nagaoka I, Aoki K,
Sawaki K and Suzuki Y: Delayed-onset muscle injury and its
modification by wheat gluten hydrolysate. Nutrition. 25:493–498.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Hirao T, Koikawa N, Aoki K, Sakuraba K,
Shimmura Y, Suzuki Y and Sawaki K: Female distance runners show a
different response to post-workout consumption of wheat gluten
hydrolysate compared to their male counterparts. Exp Ther Med.
3:641–644. 2012. View Article : Google Scholar
|
|
4.
|
Takanashi Y, Suzuki Y, Aoki K, Koikawa N,
Shimmura Y, Sakuraba K and Kaneko K: Effect of an intake of WGH on
strength training for a thrower's. Jpn J Clin Sports Med. (In
press).
|
|
5.
|
Armstrong RB: Mechanisms of
exercise-induced delayed onset muscular soreness: a brief review.
Med Sci Sports Exerc. 16:529–538. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Paulsen G, Benestad HB, Strøm-Gundersen I,
Mørkrid L, Lappegård KT and Raastad T: Delayed leukocytosis and
cytokine response to high-force eccentric exercise. Med Sci Sports
Exerc. 37:1877–1883. 2005. View Article : Google Scholar : PubMed/NCBI
|