Introduction
Mycobacterium tuberculosis (MT) is seriously
harmful to human survival and health. Currently it constitutes the
second major cause of mortality due to infectious disease
worldwide. The scientific challenge in MT control has become
increasingly complicated with the emergence of new more severe
forms of tuberculosis: extensively drug-resistant tuberculosis
(XDR-TB) and human immunodeficiency virus (HIV)-TB co-infection
(1). The rapid and accurate
identification of MT is important for controlling the spread of
tuberculosis (TB).
With the rapid development of molecular biology and
technology, numerous genotyping methods have been established for
specific nucleic acid sequences. Spoligotyping is a rapid,
polymerase chain reaction (PCR)-based method for genotyping strains
of the MT complex. Its design was reported by Kamerbeek et
al in 1997 (2). Spoligotyping
data may be represented digitally; therefore, the results may be
readily shared among laboratories. With these advantages,
spoligotyping has been widely applied to identify MT strains
worldwide (3,4). Spoligotyping uses a highly variable
set of signaling characteristics to obtain phylogenetic
information. Thereby, Sola et al established a TB
polymorphism database in 2001 (5).
The 4th international spoligotyping database, SpolDB4, describes
1939 shared types (STs) of MT, representing a total of 39,295
strains from 122 countries. These strains have been tentatively
classified into 62 clades and/or lineages using a mixed
expert-based and bioinformatics approach (6). The prevalence of MT may relate to the
specific genotype family, identified by genotyping methods.
Different genotypes have unique molecular characteristics,
geographical distributions and pathogenicities (7,8).
From a genotype study of 3,000 strains of MT obtained from 19
countries, in 1995 van Soolingen et al found that the MT
Beijing genotype family has genetic characteristics that are unique
and significant (7). The MT
Beijing strain is widely distributed in Far East Asia and
approximately 86% of clinical isolates in China belong to this
family (3). This finding has had a
major impact on the epidemiological study of MT. The spread of the
MT Beijing strain has been reported in other countries in Asia and
Eastern Europe, particularly Russia (5,8–15).
Currently, MT Beijing strains are identified principally by the
number of spacers in the direct-repeat (DR) region of the MT
genome, which is characterized by the deletion of spacers 1–34 and
the presence of most of the spacers 35–43. In addition, certain MT
Beijing-like genotypes are characterized not only in terms of
deletions of spacers 1–34 but also by certain individual deletions
in spacers 35–43.
Henan Province is located in central China and in
the middle and lower reaches of the Yellow River. The primary part
of Henan is located to the south of the Yellow River. The total
area of Henan is 167,000 km2, accounting for 1.74% of
the total area of China. Henan has a total population of 98.69
million living in 109 counties, among which 31 are national poverty
counties and 13 are provincial poverty counties. The population of
migrant workers in Henan is huge with great mobility.
The MT Beijing family strains account for 13% of
global isolates of MT and cause approximately 33% of tuberculosis
infections worldwide (16,17). However, the reason that the MT
Beijing family has spread so prolifically compared with other
strains remains unknown. Studies from animal models have shown that
it may be due to its ability to bypass Bacillus Calmette-Guérin
(BCG) immunization (18). A large
number of epidemiological studies have investigated the correlation
between the MT Beijing family and drug resistance. These studies
have reached 4 conclusions: MT Beijing is endemic and is not
related to drug resistance; MT Beijing is widely prevalent and drug
resistant; MT Beijing is widespread and drug sensitive; and MT
Beijing has low levels of drug resistance. The differences in
findings may be attributable to the various technologies and
different drugs used in these studies (18) and/or the different subfamilies of
the MT Beijing strains, which have different properties (2). Therefore, it is important to continue
to investigate the correlation between MT Beijing strains and drug
resistance, which may help to reveal the reasons behind its
prevalence in Henan Province. Henan spans the middle and lower
reaches of the Yellow River. The high prevalence of
multidrug-resistant (MDR)-TB among the TB patients in Henan
Province has been a major challenge for MT control. According to a
report of the national drug resistance baseline (2007–2008) edited
by Ministry of Health of China, the rates of primary and acquired
MDR-TB were 5.71 and 25.64%, respectively. Using spoligotyping
technology, we have determined that the MT Beijing family is the
main genotype of MT circulating in Henan Province. To determine the
reasons for its prevalence, we conducted drug-sensitivity
experiments.
Materials and methods
This study was approved by the Institutional Review
Board of the Center for Disease Control and Prevention of Henan
Province (China) and written informed consent was obtained from
each participant.
MT strains
A total of 443 isolates of MT were included
in this study. The isolates were obtained from projects that were
surveyed for the national drug resistance baseline for TB and from
clinical patients from the Henan province in 2009. Samples were
cultured and isolated with regular Löwenstein-Jensen (L-J) medium
to obtain positive cultures, which were then kept at −80°C. The
standard MT strain, H37Rv, was used as the control; it was provided
by the National Tuberculosis Reference Laboratory of the Chinese
Center for Disease Control and Prevention, Beijing, China.
Identification of drug resistance
Strain identification and drug-susceptibility
testing were performed according to World Health
Organization/International Union Against Tuberculosis and Lung
Disease (WHO/IUATLD) guidelines (19). A total of 344 strains were tested
for susceptibility to 4 drugs: isonicotinylhydrazide (INH, 0.2
μg/ml), rifampicin (RFP, 40.0 μg/ml), ethambutol (EMB, 2.0 μg/ml)
and streptomycin (SM, 4.0 μg/ml). Positive cultures were defined by
a ratio of resistant clones in drug-containing medium to control
medium of >1%.
Preparation of DNA of MT
Collected isolates were inoculated in L-J medium at
37°C for 2–4 weeks. A loop of colonies was placed in 500 μl
Tris-ethylenediamine tetraacetic acid (EDTA) buffered solution
(TE), inactivated at 80°C for 30 min. The mixture was then treated
in boiling water for 10 min. The supernatants were cleared of large
debris by centrifugation at 12,000 rpm for 2 min and were
subsequently kept at −20°C.
Spoligotyping technology
Hybrid membranes of spoligo-typing, mini-blotter
sample-board and biotin-labeled primers DRa and DRb (DRa: 5′-GGT
TTT GGG TCT GAC GAC-3′, DRb: 5′-CCG AGA GGG GAC GGA AAC-3′) were
purchased from Isogen Life Science (De Meern, Netherlands). The
streptavidin-POD (peroxidase)-conjugate and chemiluminescence (ECL)
detection system were purchased from Roche Applied Science
(Mannheim, Germany). All steps were performed according to the
instructions provided by Isogen. Detailed procedures were described
previously by Kamerbeek et al (2). The DNA of MT was firstly amplified by
primers DRa and DRb and then hybridized with membranes comprising
43 oligonucleotide probes (Table
I).
 | Table IOligonucleotide probes used in this
study. |
Table I
Oligonucleotide probes used in this
study.
| Space no. | Oligonucleotide
sequence (primer 5′-3′) |
|---|
| 1 |
ATAGAGGGTCGCCGGTTCTGGATCA |
| 2 |
CCTCATAATTGGGCGACAGCTTTTG |
| 3 |
CCGTGCTTCCAGTGATCGCCTTCTA |
| 4 |
ACGTCATACGCCGACCAATCATCAG |
| 5 |
TTTTCTGACCACTTGTGCGGGATTA |
| 6 |
CGTCGTCATTTCCGGCTTCAATTTC |
| 7 |
GAGGAGAGCGAGTACTCGGGGCTGC |
| 8 |
CGTGAAACCGCCCCCAGCCTCGCCG |
| 9 |
ACTCGGAATCCCATGTGCTGACAGC |
| 10 |
TCGACACCCGCTCTAGTTGACTTCC |
| 11 |
GTGAGCAACGGCGGCGGCAACCTGG |
| 12 |
ATATCTGCTGCCCGCCCGGGGAGAT |
| 13 |
GACCATCATTGCCATTCCCTCTCCC |
| 14 |
GGTGTGATGCGGATGGTCGGCTCGG |
| 15 |
CTTGAATAACGCGCAGTGAATTTCG |
| 16 |
CGAGTTCCCGTCAGCGTCGTAAATC |
| 17 |
GCGCCGGCCCGCGCGGATGACTCCG |
| 18 |
CATGGACCCGGGCGAGCTGCAGATG |
| 19 |
TAACTGGCTTGGCGCTGATCCTGGT |
| 20 |
TTGACCTCGCCAGGAGAGAAGATCA |
| 21 |
TCGATGTCGATGTCCCAATCGTCGA |
| 22 |
ACCGCAGACGGCACGATTGAGACAA |
| 23 |
AGCATCGCTGATGCGGTCCAGCTCG |
| 24 |
CCGCCTGCTGGGTGAGACGTGCTCG |
| 25 |
GATCAGCGACCACCGCACCCTGTCA |
| 26 |
CTTCAGCACCACCATCATCCGGCGC |
| 27 |
GGATTCGTGATCTCTTCCCGCGGAT |
| 28 |
TGCCCCGGCGTTTAGCGATCACAAC |
| 29 |
AAATACAGGCTCCACGACACGACCA |
| 30 |
GGTTGCCCCGCGCCCTTTTCCAGCC |
| 31 |
TCAGACAGGTTCGCGTCGATCAAGT |
| 32 |
GACCAAATAGGTATCGGCGTGTTCA |
| 33 |
GACATGACGGCGGTGCCGCACTTGA |
| 34 |
AAGTCACCTCGCCCACACCGTCGAA |
| 35 |
TCCGTACGCTCGAAACGCTTCCAAC |
| 36 |
CGAAATCCAGCACCACATCCGCAGC |
| 37 |
CGCGAACTCGTCCACAGTCCCCCTT |
| 38 |
CGTGGATGGCGGATGCGTTGTGCGC |
| 39 |
GACGATGGCCAGTAAATCGGCGTGG |
| 40 |
CGCCATCTGTGCCTCATACAGGTCC |
| 41 |
GGAGCTTTCCGGCTTCTATCAGGTA |
| 42 |
ATGGTGGGACATGGACGAGCGCGAC |
| 43 |
CGCAGAATCGCACCGGGTGCGGGAG |
PCR reaction system
Upstream and downstream primers, dNTP, buffer for
Taq, Taq and DNA template were mixed together and added to 50 μl
double-distilled water. PCR was performed using Taq polymerase
under standard conditions at 96°C for 3 min, then at 96°C for 1
min, 55°C for 1 min and 72°C for 30 sec. This procedure was
repeated for 30 cycles and finally the mixture was kept at 72°C for
10 min.
Membrane hybridization
The labeled membrane was transferred to a
mini-blotter sample-board. The PCR product was then added and the
board was incubated at 60°C for 60 min. The membrane was then
washed at 60°C with 2X SSPE/0.5% SDS for 10 min, followed by
incubation with l2X SSPE/0.5% SDS containing 2.5 μl
streptavidin-biotin at 42°C for 60 min. Finally, the membrane was
washed twice with 2X SSPE/0.5%SDS at 42°C for 60 min and twice with
2X SSPE for 5 min.
Chemiluminescence detection of hybrid
DNA
The membrane was incubated with an ECL detection
system for 1 min and then covered with a transparent plastic film.
The membrane was then placed into a dark cassette and exposed to
X-ray film.
Epidemiological data
Epidemiological data included the age of the
patients and the sources of the strains. A total of 443 isolates
were collected from 2007 to 2009; 334 were from >60-year-old
patients and 109 were from ≤60-year-old patients.
Statistical analysis
Genotype data were analyzed using the MIRU-VNTRplus
web-based application (http://www.miru-vntrplus.org/MIRU/index.faces).
Statistical data were analyzed using the χ2 test.
P<0.05 was considered to indicate a statistically significant
result.
Results
Beijing family strains are the most
common genotype of MT in Henan
The MT strains were genotyped by spoligotyping, and
then the genotype clusters were analyzed using the MIRU-VNTRplus
web-based application. The results revealed that the 443 strains
may be categorized into 4 MT gene clusters (Beijing and
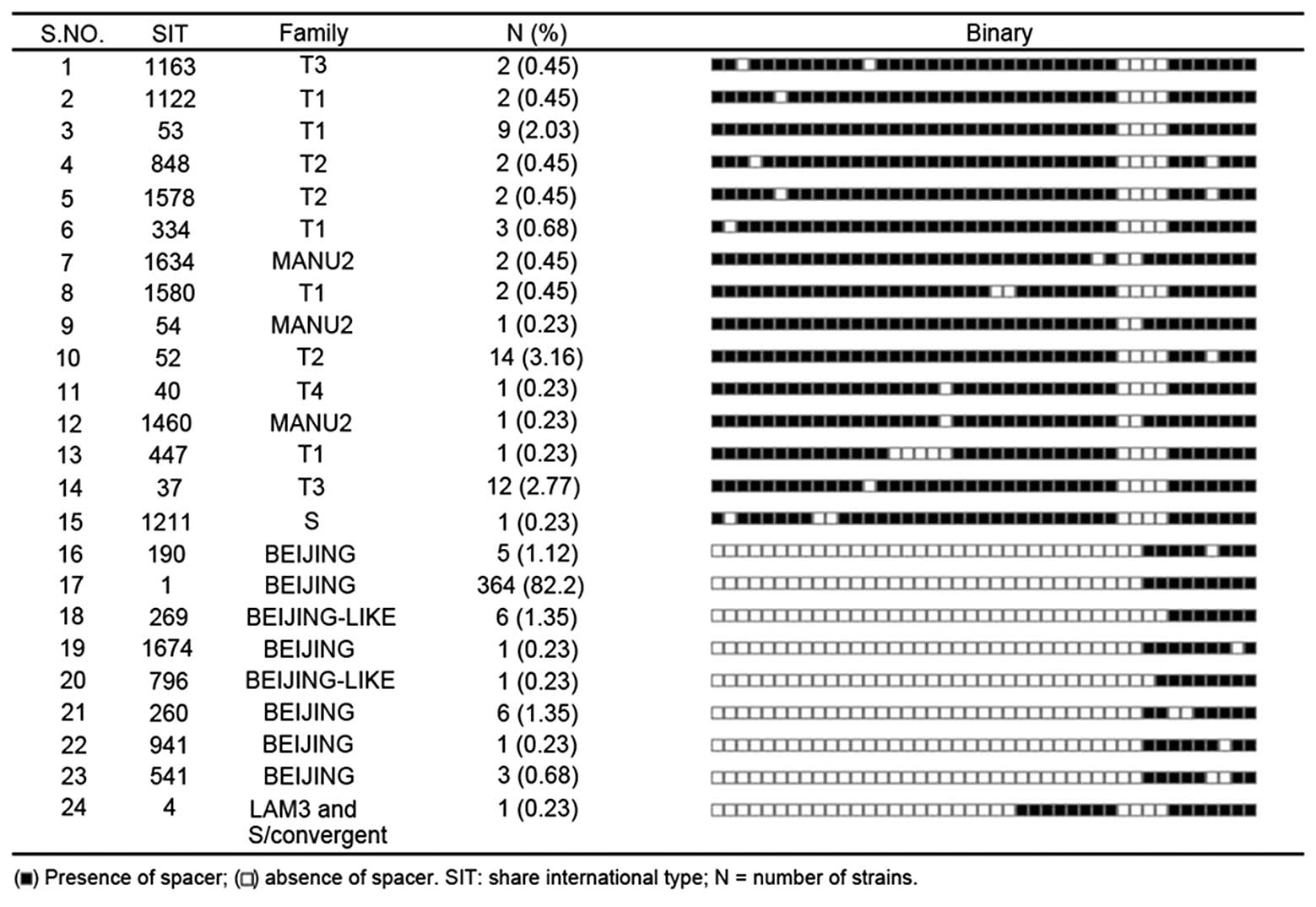
Beijing-like, T, Manu, and S and LAM3) and 24 genotypes (Fig. 1). The 387 MT Beijing strains
accounted for 87.4% of the TB cases recorded in Henan, T type
accounted for 11.3%, Manu type accounted for 0.9%, S and LAM3
accounted for 0.45% (Table
II).
| Table IIGenotyping results. |
Table II
Genotyping results.
| Strains | Proportion | Strain no. |
|---|
| Beijing and
Beijing-like | 87.4% | 387 |
| T (T1, T2, T3,
T4) | 11.3% | 50 |
| Manu | 0.9% | 4 |
| S and LAM3 | 0.45% | 2 |
Multidrug resistance is significantly
higher in the MT Beijing strains than in the non-Beijing
strains
In addition to determining genotype clusters, drug
sensitivity tests were performed on each of the 443 strains
studied. Of these, 387 strains were Beijing-type MT, and of these,
30 were MDR, accounting for 7.8% (Table III). However, no MDR strain was
found among the 56 non-Beijing strains studied. Significant
differences were found between the 2 families using the
χ2 test (χ2=4.5570, P<0.05; Table III). Our results revealed that 12
(27%) of the MDR strains were resistant to INH + RIF + SM + EMB, 10
(2.3%) were resistant to INH + RIF + SM, 6 (1.4%) were resistant to
INH + RIF and 2 (0.5%) were resistant to INH + RIF + EMB. Overall,
73.9% of the MT Beijing strains and MT Beijing-like strains were
sensitive to drugs. The percentage is similar to that in the
non-Beijing strains. Also, we observed no differences in any drug
resistance between the MT Beijing and non-Beijing strains.
| Table IIIDifferences in the characteristics
between MT Beijing (n=387) and non-Beijing (n=56) family
strains. |
Table III
Differences in the characteristics
between MT Beijing (n=387) and non-Beijing (n=56) family
strains.
| Factors | Beijing n (%) | Non-Beijing n
(%) | χ2 | P-value |
|---|
| Gender | | | | |
| Male | 275 (71.0) | 35 (62.5) | | |
| Female | 112 (28.9) | 21 (37.5) | 1.7060 | 0.1915 |
| Pan-susceptible | 286 (73.9) | 44 (78.6) | | |
| Drug-resistance | 71 (18.3) | 12 (21.4) | 0.0715 | 0.7891 |
| MDR-TB | | | | |
| INH + RIF | 6 (1.4) | | | |
| INH + RIF +
SM | 10 (2.3) | | | |
| INH + RIF +
EMB | 2 (0.5) | | | |
| INH + RIF + SM +
EMB | 12 (2.7) | | | |
| Total MDR | 30 (7.8) | | 4.5570 | 0.0328 |
Age significantly correlates with the
distribution of the Beijing strains
To further investigate the cause of the widespread
MT Beijing isolates in Henan, we assessed the distribution of
Beijing strains in different age groups (Table IV). Notably, the age of 60 years
formed a very clear boundary. Beijing strains accounted for 94.5%
of isolates from ≤60-year-old patients but only 67.7% of those from
>60-year-old patients.
| Table IVDistribution of the Beijing genotype
by age group. |
Table IV
Distribution of the Beijing genotype
by age group.
| Age (Years) | Beijing strains n
(%) | Odds ratio | 95% CI | P-value |
|---|
| <25 | 85 (96.6) | 1 | - | |
| 26–40 | 110 (94.5) | 0.97 | 0.21–4.45 | 1.00 |
| 41–60 | 125 (94.6) | 0.90 | 0.21–3.85 | 1.00 |
| 61–75 | 44 (67.7) | 0.06 | 0.02–0.23 | <0.0001 |
| >76 | 23 (52.3) | 0.04 | 0.01–0.14 | <0.0001 |
Geography significantly correlates with
the distribution of Beijing strains
To determine the distribution MT Beijing isolates in
Henan Province, we classified TB according to geographic location.
The proportion of Beijing isolates was then determined (Table V). Beijing strains accounted for
97.1% of TB cases in Fugou County in the eastern part of Henan
Province. The rate of MT Beijing in Xinmi was similar to that in
Zhongmo; Xinmi and Zhongmo are located in the central part of Henan
Province. MT Beijing isolates accounted for 88.9% of TB cases in
Whishi, also in eastern Henan. In Nanyang, which is located in the
most southern part of Henan, Beijing strains accounted for 87.6% of
TB cases. MT Beijing isolates accounted for 67.6% of cases in Song
County in the most western part of Henan. These data reveal that
the distribution of the MT Beijing genotype family extends from the
eastern to the central areas of Henan and also from the southern
end to the western edge. This is the first report of these
characteristics of MT Beijing in Henan.
| Table VDistribution of the Beijing genotype
by region. |
Table V
Distribution of the Beijing genotype
by region.
| Region | Beijing strains n
(%) | Pearson’s
χ2 value | P-value |
|---|
| Song County | 46 (67.6) | | |
| Zhongmo County | 57 (90.5) | | |
| Xinmi County | 65 (91.5) | 31.76 | <0.0001 |
| Fugou County | 67 (97.1) | | |
| Nanyang County | 64 (87.6) | | |
| Weishi County | 88 (88.9) | | |
In this study, we typed 443 isolates of MT in Henan
Province using spoligotyping technology. These data elucidated the
epidemiology of MT in the region. In total, 443 isolates were
collected from TB patients in six counties. Multiple strains were
recorded in each county: Song County (68 strains), Zhongmo (63
strains), Xinmi (71 strains), Fugou (69 strains), Nanyang (73
strains) and Weishi (99 strains).
Discussion
The MT Beijing genotype family represented 87.4% of
the total TB cases in Henan Province. This rate is higher than in
Ho Chi Minh City, Vietnam (53%) and Hanoi (58%) (20). MDR-TB accounted for 7.8% of the MT
Beijing strains, but multidrug resistance did not emerge in the
non-Beijing families, in types T1, T2, T3, T4 and other types.
Therefore, the monitoring of the MT Beijing isolates should be
focused on the surveillance of MDR strains.
Age significantly correlated with the distribution
of the Beijing family strains (Table
IV). The proportion of Beijing isolates in the ≤60-year-old
group was significantly higher than in the >60-year-old group.
Additional studies of the transmission characteristics in different
age groups are urgently required. Although we were not able to
determine the detailed proportions of recent transmission exactly,
these data suggest that the present TB patients were subject to
recent transmission. Dou et al found that MT Beijing
isolates accounted for 52.5% of cases in a genotyping study of 356
cases of MT in Taipei (21). In
their study, Beijing family isolates that emerged more recently
were found to have greater multidrug resistance and to be more
prevalent in younger individuals. The more recent strains of MT
Beijing accounted for 85.3% of TB cases in patients aged <25
years, which suggests that this strain is likely to become
prevalent in Taipei. Since the results of this study are similar to
those of the current study, it is important that we continue with
our investigations.
Finally, we found that geography also significantly
correlated with the distribution of the MT Beijing genotypes.
Distribution of the MT Beijing family spanned the eastern to
central parts of Henan Province as well as the southern end to the
westernmost area. The varying distribution of MT Beijing among
these regions is worthy of note and its causes require further
investigation. In a study of TB samples isolated from 22 regions in
China, Liu et al found that MT Beijing strains in northern
China (83.91% of all TB cases) accounted for a significantly higher
proportion of cases than in the southern region (66.4% of all TB
cases) (22). This result suggests
that subfamilies of Beijing strains may exist in different regions.
Our preliminary study indicated that Beijing strains may spread
from east to west across the Henan Province. Further studies are
required to verify this theory.
To our knowledge, this is the first genotyping study
of MT using spoligotyping in Henan. Our data demonstrate that the
most common genotype of MT in Henan is the MT Beijing family.
Multidrug resistance correlated with the prevalence of the Beijing
family in the area. The proportion of MT Beijing strains was higher
in younger age groups, suggesting that it has spread more rapidly
recently. Finally, our preliminary study showed that MT Beijing
strains may spread from east to west across the Henan Province.
Acknowledgements
This study was supported by a Henan
Medical Science and Technology Research Grant (No. 201003140). We
appreciate the valuable comments from other members of our
laboratories.
References
|
1
|
Thomas SK, Iravatham CC, Moni BH, et al:
Modern and ancestral genotypes of Mycobacterium tuberculosis
from Andhra Pradesh, India. PLoS One. 6:e275842011.PubMed/NCBI
|
|
2
|
Kamerbeek J, Schouls L, Kolk A, et al:
Simultaneous detection and strain differentiation of
Mycobacterium tuberculosis for diagnosis and epidemiology. J
Clin Microbiol. 35:907–914. 1997.PubMed/NCBI
|
|
3
|
van Soolingen D, Borgdorff MW, de Haas PE,
et al: Molecular epidemiology of tuberculosis in the Netherlands: a
nationwide study from 1993 through 1997. J Infect Dis. 180:726–736.
1999.PubMed/NCBI
|
|
4
|
Driscoll JR: Spoligotyping for molecular
epidemiology of the Mycobacterium tuberculosis complex.
Methods Mol Biol. 551:117–128. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Sola C, Filliol I, Legrand E, Mokrousov I
and Rastogi N: Mycobacterium tuberculosis phylogeny
reconstruction based on combined numerical analysis with IS1081,
IS6110, VNTR, and DR-based spoligotyping suggests the existence of
two new phylogeographical clades. J Mol Evol. 53:680–689. 2001.
View Article : Google Scholar
|
|
6
|
Brudey K, Driscoll JR, Rigouts L, et al:
Mycobacterium tuberculosis complex genetic diversity: mining
the fourth international spoligotyping database (SpolDB4) for
classification, population genetics and epidemiology. BMC
Microbiol. 6:232006. View Article : Google Scholar
|
|
7
|
van Soolingen D, Qian L, de Haas PE, et
al: Predominance of a single genotype of Mycobacterium
tuberculosis in countries of east Asia. J Clin Microbiol.
33:3234–3238. 1995.PubMed/NCBI
|
|
8
|
Roetzer A, Schuback S, Diel R, et al:
Evaluation of Mycobacterium tuberculosis typing methods in a
4-year study in Schleswig-Holstein, Northern Germany. J Clin
Microbiol. 49:4173–4178. 2011.PubMed/NCBI
|
|
9
|
Brosch R, Gordon SV, Marmiesse M, et al: A
new evolutionary scenario for the Mycobacterium tuberculosis
complex. Proc Natl Acad Sci USA. 99:3684–3689. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Abebe F and Bjune G: The emergence of
Beijing family genotypes of Mycobacterium tuberculosis and
low-level protection by bacille Calmette-Guérin (BCG) vaccines: is
there a link? Clin Exp Immunol. 145:389–397. 2006.PubMed/NCBI
|
|
11
|
Bifani PJ, Mathema B, Kurepina NE and
Kreiswirth BN: Global dissemination of the Mycobacterium
tuberculosis W-Beijing family strains. Trends Microbiol.
10:45–52. 2002.
|
|
12
|
Glynn JR, Whiteley J, Bifani PJ, Kremer K
and van Soolingen D: Worldwide occurrence of Beijing/W strains of
Mycobacterium tuberculosis: a systematic review. Emerg
Infect Dis. 8:843–849. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Diaz R, Kremer K, de Haas PE, et al:
Molecular epidemiology of tuberculosis in Cuba outside of Havana,
July 1994–June 1995: utility of spoligotyping versus IS6110
restriction fragment length polymorphism. Int J Tuberc Lung Dis.
2:743–750. 1998.PubMed/NCBI
|
|
14
|
Cole ST, Brosch R, Parkhill J, et al:
Deciphering the biology of Mycobacterium tuberculosis from
the complete genome sequence. Nature. 393:537–544. 1998.
|
|
15
|
Filliol I, Driscoll JR, van Soolingen D,
et al: Global distribution of Mycobacterium tuberculosis
spoligotypes. Emerg Infect Dis. 8:1347–1349. 2002.
|
|
16
|
López B, Aguilar D, Orozco H, et al: A
marked difference in pathogenesis and immune response induced by
different Mycobacterium tuberculosis genotypes. Clin Exp
Immunol. 133:30–37. 2003.PubMed/NCBI
|
|
17
|
European Concerted Action on New
Generation Genetic Markers and Techniques for the Epidimiology and
Control of Tuberculosis: Beijing/W genotype Mycobacterium
tuberculosis and drug resistance. Emerg Infect Dis. 12:736–743.
2006.
|
|
18
|
Parwati I, van Crevel R and van Soolingen
D: Possible underlying mechanisms for successful emergence of the
Mycobacterium tuberculosis Beijing genotype strains. Lancet
Infect Dis. 10:103–111. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
World Health Organization
(WHO)/International Union Against Tuberculosis and Lung Disease
(IUATLD): Global working group on antituberculosis drug resistance
surveillance [S]. Guidelines for surveillance of drug resistance in
tuberculosis. 1997
|
|
20
|
Anh DD, Borgdorff MW, Van LN, et al:
Mycobacterium tuberculosis Beijing genotype emerging in
Vietnam. Emerg Infect Dis. 6:302–305. 2000. View Article : Google Scholar
|
|
21
|
Dou HY, Tseng FC, Lin CW, et al: Molecular
epidemiology and evolutionary genetics of Mycobacterium
tuberculosis in Taipei. BMC Infect Dis. 8:1702008. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Liu Q, Yang D, Xu W, et al: Molecular
typing of Mycobacterium tuberculosis isolates circulating in
Jiangsu province, China. BMC Infect Dis. 11:2882011.
|