Introduction
The receptor protein kinase MET was originally
identified as an activated oncogene (1), with hepatocyte growth factor (HGF),
also known as scatter factor (SF), as the primary ligand. Usually
MET is expressed in a variety of epithelial and mesenchymal cells.
MET and HGF have been known to induce cell proliferation,
angiogenesis, cell adhesion, invasion, motility and anti-apoptotic
responses (2,3). Previous studies have demonstrated a
significant MET overexpression in numerous tumor types including
glioblastoma (4), melanoma
(5), colorectal (6), breast (7), lung (8), gastric (9), thyroid (10) and prostate cancer (11). In addition, aberrant MET expression
has been found to be associated with a poor prognosis in a variety
of cancers (4,12).
MET expression occurs in the normal prostate
epithelium. In contrast to luminal cells, basal cells show
consistently high c-MET expression (13). Data on MET expression in prostate
cancer are conflicting. Certain studies have reported no
associations of high c-MET levels with Gleason grade, while others
have reported high MET protein expression in more advanced or
metastatic prostate cancer (11,13–15).
Recently, c-MET has been proposed as a candidate for targeted
cancer therapy in prostate cancer and other tumors (16). In addition, c-MET has been proposed
to be a regulator of response to anti-HER2 and anti-epidermal
growth factor receptor (EGFR) therapy. For example, in one study,
64 HER2-positive breast cancer patients with increased c-MET
expression demonstrated a decreased response to EGFR/HER2 inhibitor
therapy (17). Although the data
are controversial and mostly negative, the use of anti-EGFR/HER2
therapy remains under discussion for prostate cancer (18).
The aim of this study was to clarify the prevalence
and prognostic role of c-MET expression in prostate cancer by using
a pre-existing tissue microarray (TMA) including more than 4,000
prostate cancers, the majority with clinical follow-up data. The
data show an abundant expression of c-MET and demonstrate that
c-MET protein analysis does not serve as a prognostic marker for
prostate cancer patients.
Patients and methods
Patients
A pre-existing prostate cancer TMA consisting of
tissue samples from radical prostatectomy specimens of 4,177
patients, consecutively treated at the Department of Urology and
the Martini Clinic at the University Medical Center
Hamburg-Eppendorf (Hamburg, Germany) between 1997 and 2008
(Table I), was used in this study.
Follow-up data were available for 4,104 patients, ranging from 1 to
150 months (mean, 51 months). None of the patients received
neo-adjuvant or adjuvant therapy. Additional (salvage) therapy was
only initiated after biochemical relapse (BCR), the clinical
end-point of our study. Prostate-specific antigen (PSA) levels were
measured quarterly in the first year, followed by biannual
measurements in the second and annual measurements after the third
year following surgery. Recurrence was defined as a post-operative
PSA of 0.2 ng/ml and subsequent increase. The first PSA level above
or equal to 0.2 ng/ml was used to define the time of recurrence.
Patients without evidence of tumor recurrence were censored at the
last follow-up. All prostatectomy specimens were analyzed according
to a standard procedure. All prostates were completely
paraffin-embedded, including whole-mount sections as previously
described (19). A 0.6-mm tissue
core was punched out from each sample and transferred to a TMA
format as previously described (20). The 4,177 cores were distributed
among 9 TMA blocks each containing 129–522 tumor samples. Each TMA
block also contained various control tissues including normal
prostate tissue and other normal tissues. The utilization of
tissues and clinical data was in accordance with the Hamburger
Krankenhaus Gesetz (§12 HmbKHG) and approved by our local ethics
committee. According to this reputation, informed consent of
individual patients was not necessary.
 | Table IPathological and clinical data of the
arrayed prostate cancers. |
Table I
Pathological and clinical data of the
arrayed prostate cancers.
| No. of
patientsa
|
|---|
| Variable | Study cohort on TMA
(n=4,177) | Biochemical relapse
among categories (n=4,104) |
|---|
| Follow-up
(months) | | |
| Mean | 51.1 | - |
| Median | 38.1 | - |
| Age (years) | | |
| <50 | 119 | 119 |
| 50–60 | 1,249 | 1,237 |
| 60–70 | 2,388 | 2,347 |
| >70 | 277 | 260 |
| Pre-treatment PSA
(ng/ml) | | |
| <4 | 631 | 625 |
| 4–10 | 2,356 | 2,230 |
| 10–20 | 774 | 759 |
| >20 | 225 | 203 |
| pT category (AJCC
2002) | | |
| pT2 | 2,789 | 2,780 |
| pT3a | 806 | 786 |
| pT3b | 412 | 374 |
| pT4 | 25 | 33 |
| Gleason grade | | |
| ≤3+3 | 1,593 | 1,589 |
| 3+4 | 1,847 | 1,828 |
| 4+3 | 442 | 426 |
| ≥4+4 | 146 | 115 |
| pN category | | |
| pN0 | 1,882 | 1,840 |
| pN+ | 146 | 123 |
| Surgical margin | | |
| Negative | 3,255 | 3,224 |
| Positive | 751 | 717 |
Immunohistochemistry
Freshly cut TMA sections were stained on 1 day in a
single experiment. High-temperature pre-treatment of slides was
performed in an autoclave in citrate buffer, pH 7.8 for 5 min.
c-MET immunostaining was performed using a monoclonal antibody
(clone: EP1454, Abcam, Cambridge, UK, dilution 1:150). The Envision
system (Dako, Glostrup, Denmark) was used to visualize the
immunostaining. Only membranous staining was evaluated as
cytoplasmatic staining, if present, was always linked with stronger
membranous staining. The staining intensity (0, 1+, 2+, 3+) and the
fraction of positive tumor cells were recorded for each tissue
sample. A final score was created from these 2 parameters according
to the following scores: negative scores had a staining intensity
of 0; weak scores had a staining intensity of 1+ in ≤70% of tumor
cells or a staining intensity of 2+ in ≤30% of tumor cells;
moderate scores had a staining intensity of 1+ in >70% of tumor
cells or a staining intensity of 2+ in >30% but ≤70% of tumor
cells or a staining intensity of 3+ in ≤30% of tumor cells; and
strong scores had a staining intensity of 2+ in >70% of tumor
cells or a staining intensity of 3+ in >30% of tumor cells.
Statistic analysis
For statistical analysis, the JMP 8.0 software (SAS
Institute Inc., Cary, NC, USA) was used. Contingency tables were
calculated to determine the association between the c-MET
immunostaining score and clinicopathological variables. The
Chi-square test was used to identify significant associations.
Kaplan-Meier curves were generated for PSA recurrence-free
survival. The log-rank test was performed to determine the
significance of differences between stratified survival functions.
Cox proportional hazards regression analysis was performed to
determine the statistical independence and significance between
pathological, molecular and clinical variables.
Results
Technical issues
A total of 3,378 (81.6%) tumor samples were
successfully analyzed in our TMA analysis. The reasons for
non-informative cases (762; 19.4%) included a lack of tissue
samples or absence of unequivocal cancer tissue in individual TMA
samples.
Immunohistochemistry
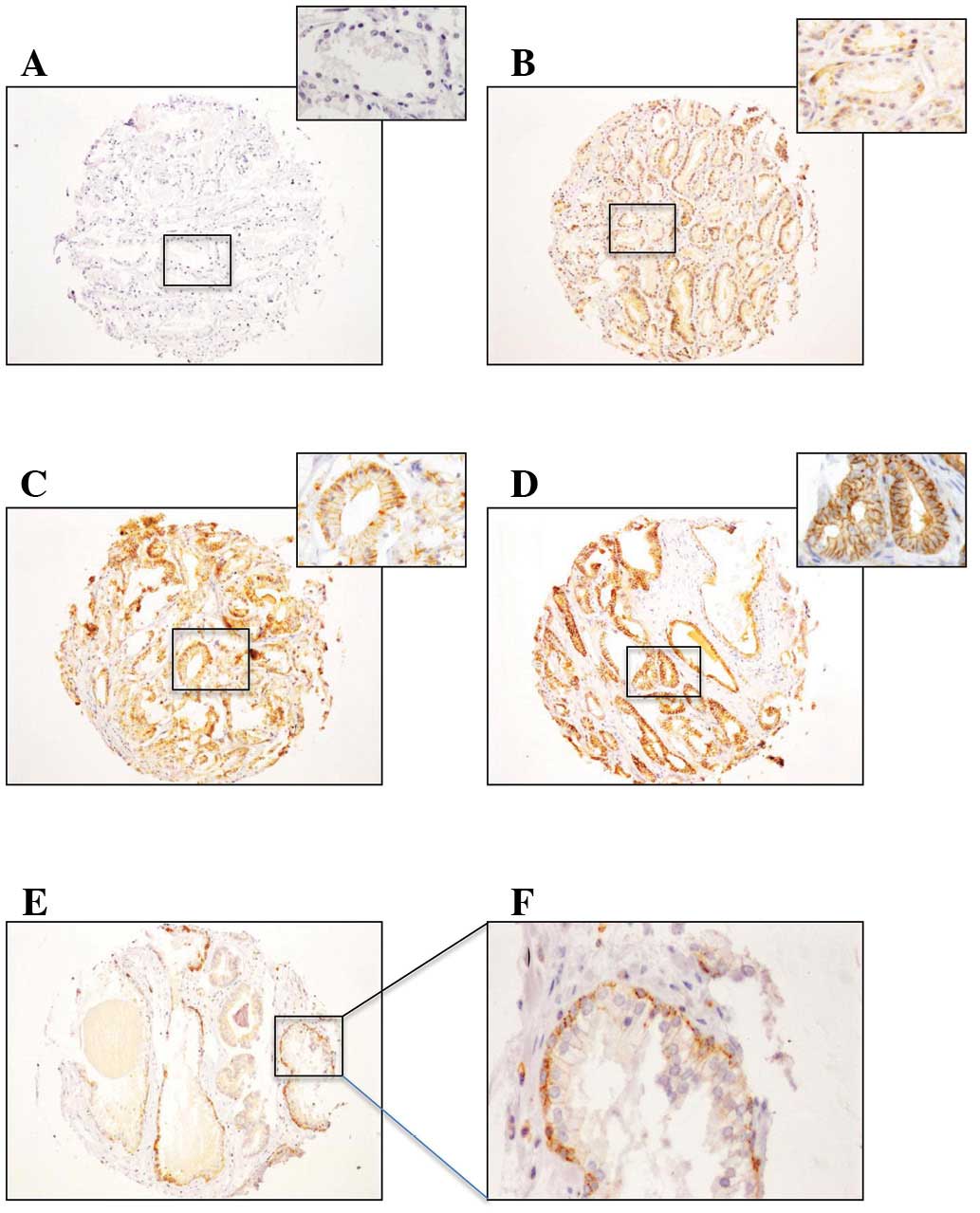
c-MET immunostaining revealed strong membrane
staining in our tissues. Although certain cytoplasmic staining was
sometimes observed, this was always associated with a markedly
higher staining level at the membranes. Membranous c-MET
immunostaining was recorded in 2,655 (78.6%) of 3,378 successfully
analyzed cases. Staining was weak in 780 (23.1%), moderate in 801
(23.7%) and strong in 1074 (31.8%) prostate cancers (Fig. 1B and C). In benign prostate
epithelium, c-MET was always strongly expressed in prostate basal
cells (Fig. 1E and F), with a
weaker expression in luminal cells as compared with the majority of
invasive cancers (Fig. 1A–D). The
association between c-MET immunostaining and tumor phenotype is
summarized in Table II.
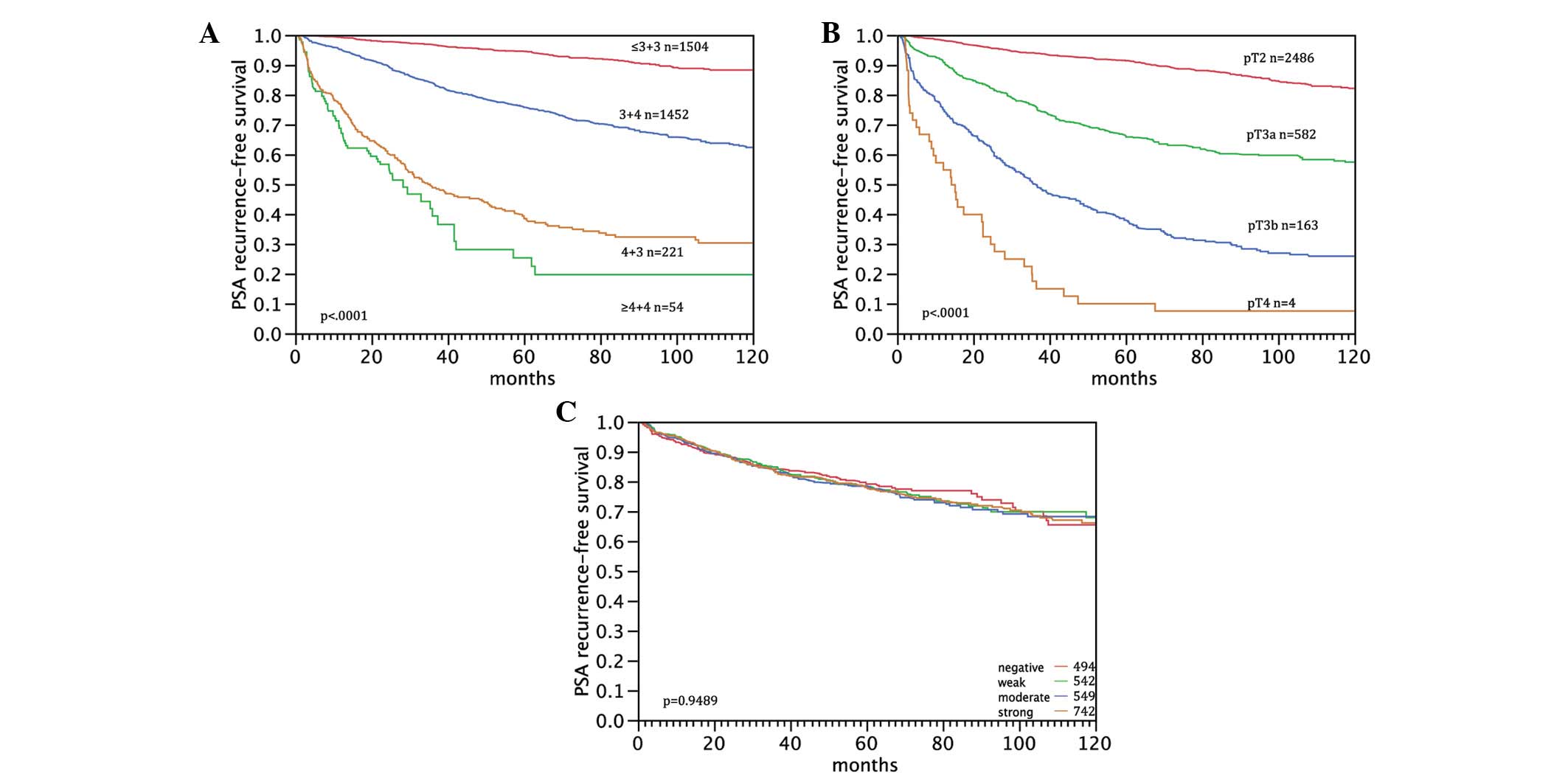
Significant associations were demonstrated between strong c-MET
expression and high Gleason grade (P=0.0018) as well as increased
pre-operative PSA levels (P=0.0064). c-MET staining levels were not
associated with tumor stage (P=0.1191), nodal stage (P=0.3907),
surgical margin status (P=0.758) or pre-operative PSA level
(P=0.0064). Follow-up data were available for 4,104 patients and
3,378 cases were successfully analyzed. As predicted, Gleason grade
and pT stage were significantly associated with PSA recurrence in
this patient subset (P<0.0001 each; Fig. 2A and B). However, c-MET protein
expression levels were not associated with the risk of PSA
recurrence (P=0.949, Fig. 2C).
| Table IIMET expression and tumor
phenotype. |
Table II
MET expression and tumor
phenotype.
| Variable | No. of successfully
analyzed samples | c-MET
immunohistochemistry result
| P-value | |
|---|
| Negative (%) | Weak (%) | Moderate (%) | Strong (%) |
|---|
| All tumors | 3,378a | 21.4 | 23.1 | 23.7 | 31.8 | |
| Tumor stage | | | | | | |
| pT2 | 2,203 | 22.2 | 23.5 | 22.9 | 31.4 | 0.1191 |
| pT3a | 695 | 20.3 | 20.4 | 25.0 | 34.2 | |
| pT3b | 335 | 20.0 | 26.0 | 23.9 | 30.1 | |
| pT4 | 21 | 4.8 | 23.8 | 19.0 | 52.4 | |
| Gleason grade | | | | | | |
| ≤3+3 | 1,204 | 24.1 | 25.0 | 21.2 | 29.7 | 0.0018 |
| 3+4 | 1,567 | 20.9 | 21.6 | 25.1 | 32.4 | |
| 4+3 | 362 | 16.6 | 22.7 | 26.0 | 34.8 | |
| ≥4+4 | 118 | 16.9 | 26.3 | 16.9 | 39.8 | |
| Nodal stage | | | | | | |
| N0 | 1,529 | 18.3 | 21.9 | 24.3 | 35.5 | 0.3907 |
| N+ | 123 | 23.6 | 23.6 | 19.5 | 33.3 | |
| Surgical
margin | | | | | | |
| Negative | 2,602 | 21.4 | 23.5 | 23.3 | 31.8 | 0.758 |
| Positive | 632 | 21.8 | 21.5 | 24.4 | 32.3 | |
| Pre-operative PSA
level (ng/ml) | | | | | | |
| <4 | 468 | 16.9 | 22.4 | 25.4 | 35.3 | 0.0064 |
| 4–10 | 1,918 | 20.9 | 22.7 | 24.7 | 31.8 | |
| 10–20 | 645 | 25.6 | 24.3 | 20.6 | 29.5 | |
| >20 | 191 | 26.7 | 22.5 | 17.8 | 33.0 | |
Discussion
In the present study, the frequency and the
potential clinicopathological role of c-MET protein expression was
investigated in prostate cancer. The data demonstrate that c-MET
expression is abundant in prostate cancer but lacks a clear
association with an unfavorable phenotype or a poor clinical
outcome. Membranous c-MET staining was observed in 2,655 (78.6%) of
3,378 successfully analyzed cancers and strong c-MET expression was
significantly associated with a high Gleason grade (P=0.0018).
These results are within the range of previous studies using
immunohistochemistry, although the reported c-MET expression levels
vary from 33 to 84% (11,13–15).
However, the number of analyzed tumors was markedly lower in these
studies compared with the present cohort. Pisters et
al(15) analyzed a cohort of
43 primary prostate cancers. They observed c-MET expression in 84%
of cases and revealed an association between c-MET expression and
advanced grade prostate cancers (P<0.001). Another group
examined 108 prostate cancers and observed c-MET expression in 45%
of cases. Their group distinguished between cytoplasmic or luminal
membrane staining. No correlation was observed with Gleason grade
(11). Watanabe et
al(14) investigated a cohort
of 36 patients, 33% of ‘latent’ and 71% of ‘clinical significant’
prostate cancers displayed cytoplasmic c-MET expression. In total,
38% of low-grade and 80% of high-grade prostate cancers presented
c-MET expression. Knudsen et al(13) analyzed a cohort of 90 low-grade
tumors (Gleason score 6 or 7). c-MET expression was observed in 51%
of cancers. They could not identify any correlation between c-MET
expression and disease progression. Overall, these studies
demonstrate a wide range of c-MET expression rates and are not
always consistent with our findings.
It is possible that these controversial data are
partly attributable to sampling issues as these studies have all
analyzed markedly small patient cohorts and are characterized by
highly variable definitions of c-MET-positivity. Watanabe et
al(14) considered a tumor
sample as positive if more than 30% of the tumor cells stained for
c-MET, while Humphrey et al required only more than 5% to
classify a tumor as positive (11). Knudsen et al(13) evaluated at least moderate staining
intensity as c-MET positive. In addition, the staining of the
secretory cells differs from the previous described studies. In the
report by Pisters et al(15), secretory cell c-MET expression is
limited to the central zone. Other studies do not note regional
variation of expression (11,14).
In contrast Knudsen et al(13) did not observe expression of c-MET
in secretory cells.
c-MET is frequently expressed in a variety of other
cancers. For some cancers, including cholangiocarcinoma, gastric or
skin cancer, a clear correlation between c-MET expression level and
a poor prognosis has been demonstrated (5,21,22).
A skin cancer study revealed significant overexpression of c-MET in
all skin cancers with stronger positive responce in malignant
melanomas. c-MET expression was stronger in deeper melanomas than
in superficial ones (5). However,
other investigations identified no significant association between
c-MET expression level and clinicopathological parameters (23). Accordingly c-MET could only be used
as a prognostic marker in certain cancer types, but not in
others.
The high frequency of expression in prostate and
other cancer types makes c-MET an attractive potential therapeutic
target. Recently, several studies with c-MET inhibitors were
realized or are in progress (24,25).
Recently published studies demonstrate the anti-proliferative
efficacy of c-MET inhibitors in combination with androgen ablation
therapy for advanced prostate cancer (16,17).
This illustrates that co-targeting of c-MET and androgen signaling
pathway might be a therapeutic option for the treatment of prostate
cancer in the future (16).
In conclusion, the results of this study reveal that
c-MET is frequently overexpressed in prostate cancer. A significant
correlation was demonstrated between strong c-MET expression and
high Gleason grade, but not with other clinicopathological
parameters. Although c-MET appears to be involved in the
progression of prostate cancer, this study does not confirm a role
of c-MET as a prognostic marker in patients with prostate
cancer.
References
|
1
|
Cooper CS, Park M, Blair DG, et al:
Molecular cloning of a new transforming gene from a chemically
transformed human cell line. Nature. 311:29–33. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Knudsen BS and Edlund M: Prostate cancer
and the met hepatocyte growth factor receptor. Adv Cancer Res.
91:31–67. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Peruzzi B and Bottaro DP: Targeting the
c-Met signaling pathway in cancer. Clin Cancer Res. 12:3657–3660.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kong DS, Song SY, Kim DH, et al:
Prognostic significance of c-Met expression in glioblastomas.
Cancer. 115:140–148. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Lee YJ, Kim DH, Lee SH, Kim DW, Nam HS and
Cho MK: Expression of the c-Met proteins in palignant skin cancers.
Ann Dermatol. 23:33–38. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
De Oliveira AT, Matos D, Logullo AF, et
al: MET Is highly expressed in advanced stages of colorectal cancer
and indicates worse prognosis and mortality. Anticancer Res.
29:4807–4811. 2009.PubMed/NCBI
|
|
7
|
Matteucci E, Bendinelli P and Desiderio
MA: Nuclear localization of active HGF receptor Met in aggressive
MDA-MB231 breast carcinoma cells. Carcinogenesis. 30:937–945. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ichimura E, Maeshima A, Nakajima T and
Nakamura T: Expression of c-met/HGF receptor in human non-small
cell lung carcinomas in vitro and in vivo and its prognostic
significance. Jpn J Cancer Res. 87:1063–1069. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kuniyasu H, Yasui W, Yokozaki H, Kitadai Y
and Tahara E: Aberrant expression of c-met mRNA in human gastric
carcinomas. Int J Cancer. 55:72–75. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Belfiore A, Gangemi P, Costantino A, et
al: Negative/low expression of the Met/hepatocyte growth factor
receptor identifies papillary thyroid carcinomas with high risk of
distant metastases. J Clin Endocrinol Metab. 82:2322–2328.
1997.PubMed/NCBI
|
|
11
|
Humphrey PA, Zhu X, Zarnegar R, et al:
Hepatocyte growth factor and its receptor (c-MET) in prostatic
carcinoma. Am J Pathol. 147:386–396. 1995.PubMed/NCBI
|
|
12
|
Birchmeier C, Birchmeier W, Gherardi E and
Vande Woude GF: Met, metastasis, motility and more. Nat Rev Mol
Cell Biol. 4:915–925. 2003. View
Article : Google Scholar : PubMed/NCBI
|
|
13
|
Knudsen BS, Gmyrek GA, Inra J, et al: High
expression of the Met receptor in prostate cancer metastasis to
bone. Urology. 60:1113–1117. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Watanabe M, Fukutome K, Kato H, et al:
Progression-linked overexpression of c-Met in prostatic
intraepithelial neoplasia and latent as well as clinical prostate
cancers. Cancer Lett. 141:173–178. 1999. View Article : Google Scholar
|
|
15
|
Pisters LL, Troncoso P, Zhau HE, Li W, von
Eschenbach AC and Chung LW: c-met proto-oncogene expression in
benign and malignant human prostate tissues. J Urol. 154:293–298.
1995. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Tu WH, Zhu C, Clark C, Christensen JG and
Sun Z: Efficacy of c-Met inhibitor for advanced prostate cancer.
BMC Cancer. 10:5562010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Varkaris A, Corn PG, Gaur S, Dayyani F,
Logothetis CJ and Gallick GE: The role of HGF/c-Met signaling in
prostate cancer progression and c-Met inhibitors in clinical
trials. Expert Opin Investig Drugs. 20:1677–1684. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Gross ME, Jo S and Agus DB: Update on
HER-kinase-directed therapy in prostate cancer. Clin Adv Hematol
Oncol. 2:53–56. 642004.PubMed/NCBI
|
|
19
|
Erbersdobler A, Fritz H, Schnöger S, et
al: Tumour grade, proliferation, apoptosis, microvessel density,
p53, and bcl-2 in prostate cancers: differences between tumours
located in the transition zone and in the peripheral zone. Eur
Urol. 41:40–46. 2002. View Article : Google Scholar
|
|
20
|
Bubendorf L: High-throughput microarray
technologies: from genomics to clinics. Eur Urol. 40:231–238. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Miyamoto M, Ojima H, Iwasaki M, et al:
Prognostic significance of overexpression of c-Met oncoprotein in
cholangiocarcinoma. Br J Cancer. 105:131–138. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Amemiya H, Menolascino F and Peña A: Role
of the expression of c-Met receptor in the progression of gastric
cancer. Invest Clin. 51:369–380. 2010.(In Spanish).
|
|
23
|
Freudlsperger C, Alexander D, Reinert S
and Hoffmann J: Prognostic value of c-Met expression in oral
squamous cell carcinoma. Exp Ther Med. 1:69–72. 2010.PubMed/NCBI
|
|
24
|
Previdi S, Abbadessa G, Dalò F, France DS
and Broggini M: Breast cancer-derived bone metastasis can be
effectively reduced through specific c-MET inhibitor tivantinib
(ARQ 197) and shRNA c-MET knockdown. Mol Cancer Ther. 11:214–223.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Liu X, Wang Q, Yang G, et al: A novel
kinase inhibitor, INCB28060, blocks c-MET-dependent signaling,
neoplastic activities, and cross-talk with EGFR and HER-3. Clin
Cancer Res. 17:7127–7138. 2011. View Article : Google Scholar : PubMed/NCBI
|