Introduction
The iris has important physiological functions with
regard to regulating the amount of light that enters the eyes,
increasing focal depth and decreasing eyeball aberrations (1). Patients with apriority, traumatic or
surgical aniridia, or serious iris coloboma exhibit several
symptoms, including serious photophobia, monodiplopia, glare and
unsatisfactory corrected eyesight (2). Due to congenital dysplasia, trauma,
surgery, the integrity of the iris is damaged or missing and normal
morphology and size of pupil are damaged, referred to as the ‘iris
defect’. Furthermore, these patients also present with cataracts
and crystalline lens dislocation (3,4).
Various surgical techniques may be used to conduct IOL implantation
when patients exhibit with iris coloboma and cataracts (5,6). In
the present study, a review of patients treated with various
surgical techniques based on different iris coloboma and
crystalline lens anomalies was carried out, and the results of the
various treatments are reported.
Materials and methods
General data
A total of 56 patients, comprising 38 males and 18
females, with ages ranging from 2.5 to 45.2 years (mean, 21.6±2.4
years), who were treated with IOL implants at The Fourth Affiliated
Hospital of Kunming Medical University (Kunming, China) from
January 2006 to January 2011 were included in this study. The
numbers of patients who required monocular and binocular treatment
were 49 and 7, respectively. In total, 49 patients presented with
traumatic iris coloboma with cataracts or crystalline lens coloboma
and seven presented with congenital iris coloboma and cataracts.
The best corrected visual acuity was <0.1 in 33 cases, 0.1–0.4
in 21 cases and 0.5 in two cases. All patients experienced
photophobia and glare to varying degrees. Examination of the eye by
B-scan ultrasound (ODM2000; Shanghai Huan Hee Medical Devices Co.
Ltd. Shanghai, China) and ophthalmoscopy (OMEGA500, HEINE, HEINE
Optotechnik, Herrsching, Germany) was carried out to exclude
diseases of the fundus oculi. Various surgical techniques were used
based on the different degrees of iris coloboma, atrophy and lens
capsule damage. This study was conducted according to the
Declaration of Helsinki and was approved by the Ethics Committee of
the First Affiliated Hospital of Kunming Medical University.
Informed consent was obtained from all participants.
Surgical techniques
In total, 11 patients presented with iris coloboma
confined to one quadrant with an intact lens capsule, of which
eight exhibited traumatic iris coloboma with cataracts and three
had apriority iris coloboma with cataracts. These patients were
treated with iris sutures, cataract extirpation and IOL
implantation into the posterior chamber. The surgery used was
continuous circular capsulorhexis, which required either aspiration
or phacoemulsification extraction of the cataract and the
implantation of a collapsible type of IOL into the posterior
chamber. A 10-0 suture and a 1–2 needle were used to suture the
pupil.
A further six patients presented with an iris
coloboma confined within one quadrant, severe iris atrophy, and
significant crystalline lens coloboma caused by trauma. These
patients were treated with an annular suture at the pupil edge and
IOL implantation into the anterior chamber. A clear corneal
incision was performed and sodium hyaluronate (Shandong Bausch
& Lomb Freda Pharmaceutical Co. Ltd. Jinan, China) was injected
into the anterior chamber. The edge of the damaged iris was
continuously sutured with a polypropylene line in order to rebuild
the pupil. Subsequently, the IOL was implanted into the anterior
chamber, and the location of the IOL was adjusted to a central
position.
The study included two patients who presented with
binocular congenital iris coloboma and congenital cataracts, eight
with traumatic cataracts caused by traumatic debridement and
suturing of the monocular cornea, and two with binocular congenital
cataracts treated with optical iridectomy. These patients were each
treated with an artificial iris and IOL implantation. The surgery
for these patients required aspiration, extracapsular cataract
extraction, or phacoemulsification cataract extraction. A capsular
tension ring with an iris diaphragm was implanted into the lens
capsule. A Morcher Type 96G Partial Aniridia Ring (Morcher GmbH,
Stuttgart, Germany) was implanted into the eyes of patients with
partial iris coloboma, and a section of the iris diaphragm was
rotated to correspond with the section of the iris coloboma. If the
patients had a complete iris coloboma, two Morcher Type 50C
Aniridia Rings (Morcher GmbH) were implanted, and the corresponding
sections were folded to constitute a complete iris diaphragm. The
tensile ring and IOL location were adjusted following the insertion
of a collapsible type of IOL.
In total, 27 patients with iris coloboma in more
than two quadrants, severe lens capsule coloboma, or crystalline
lens dislocation in more than one quadrant were treated by IOL with
iris implantation with a foldable intraocular lens. An incision of
~10 mm was opened on the edge of the corneosclera. The cataract was
removed, with aspiration as required, or the crystalline lens was
excised and sodium hyaluronate was injected into the anterior
chamber. The IOL with iris was implanted into the ciliary groove.
The polypropylene line was removed from the anterior chamber at the
ten o’clock position located 15 mm behind the edge of the
corneosclera and also removed from the four o’clock position. The
line was subsequently removed from the incision beside the edge of
the corneosclera, cut off and fastened to the loop of the IOL with
iris. A knot was tied at the end of the line and was covered by a
conjunctival flap.
Results
Iris sutures and IOL implantation
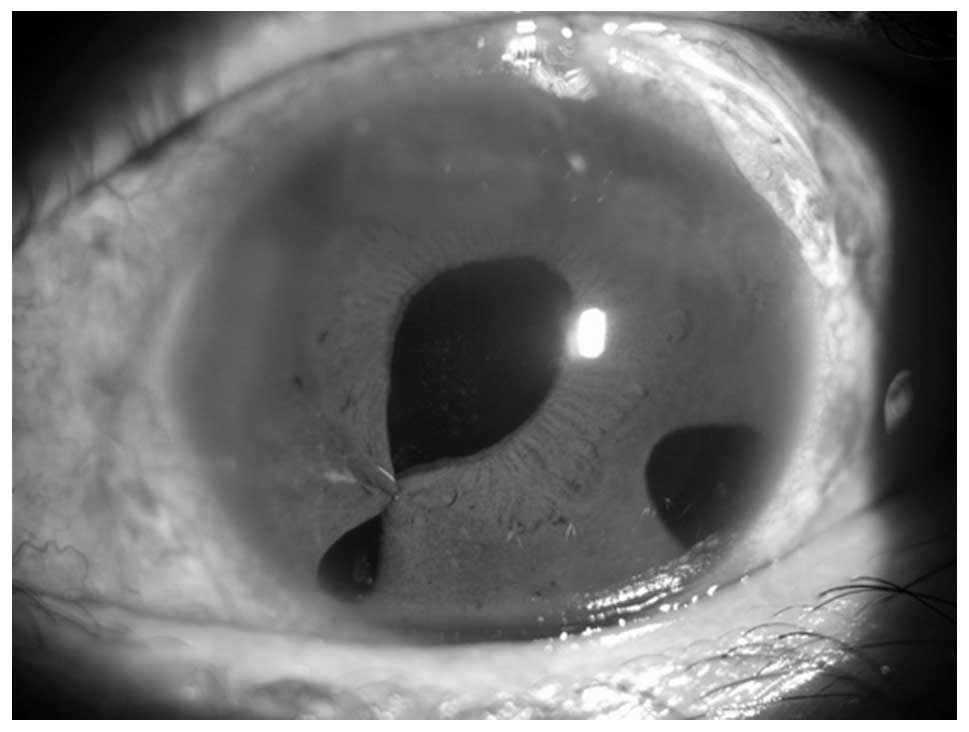
The vision of the eight patients with traumatic iris
coloboma from the 11 treated with iris sutures, cataract
extirpation and IOL implantation into the posterior chamber,
significantly improved. Three of these eight patients had a
corrected visual acuity of <0.1 and the other five patients had
a best corrected visual acuity of between 0.1 and 0.5. Among the
three patients with apriority iris coloboma, two patients had a
corrected visual acuity of 0.5–0.8 and one patient had a corrected
visual acuity of >0.8. The vision of these patients did not
improve following surgery due to amblyopia. The patients did not
exhibit photophobia. The patients’ pupils examined with a slit lamp
were observed to be round or oval in shape. The diameter of pupils
was between 3 and 4 mm, and the location of the posterior chamber
IOL was not shifted (Fig. 1).
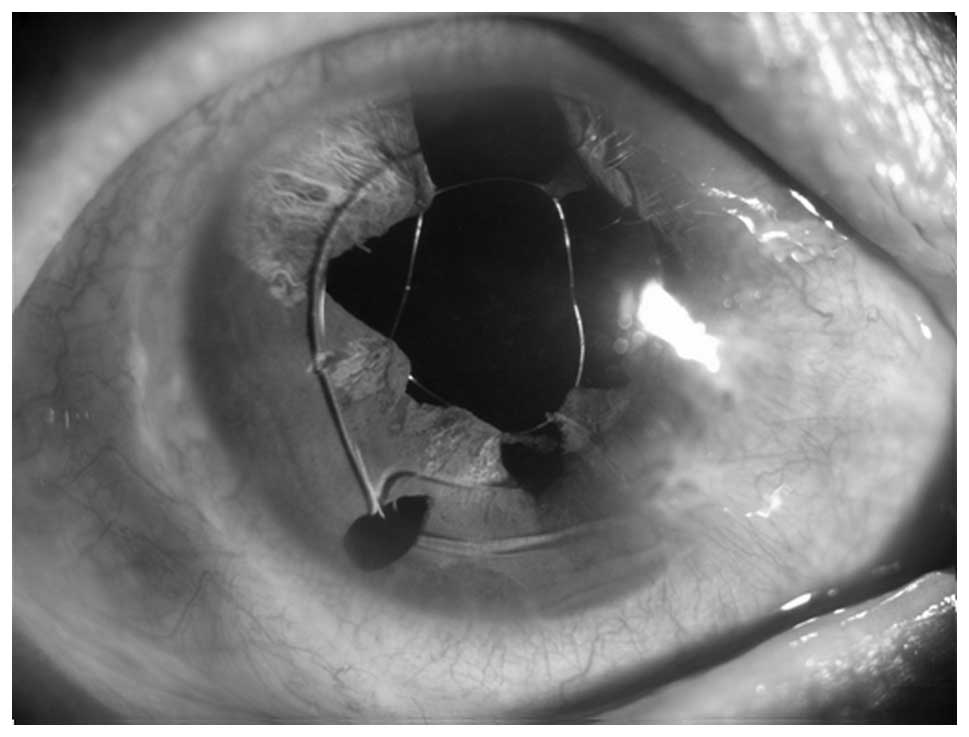
Annular suture and IOL implantation
Of the six patients treated with an annular suture
to the pupil edge and IOL implantation into the anterior chamber,
the corrected visual acuity of four patients improved to 0.1–0.4,
whereas the other two patients had a corrected visual acuity of
0.6. Furthermore, the patients no longer presented with
photophobia. Under slit lamp observation, the polypropylene line
caused each section of the residual atrophic iris to form rounded
pupils; the reconstituted pupils were capable of supporting a IOL
in the anterior chamber (Fig.
2).
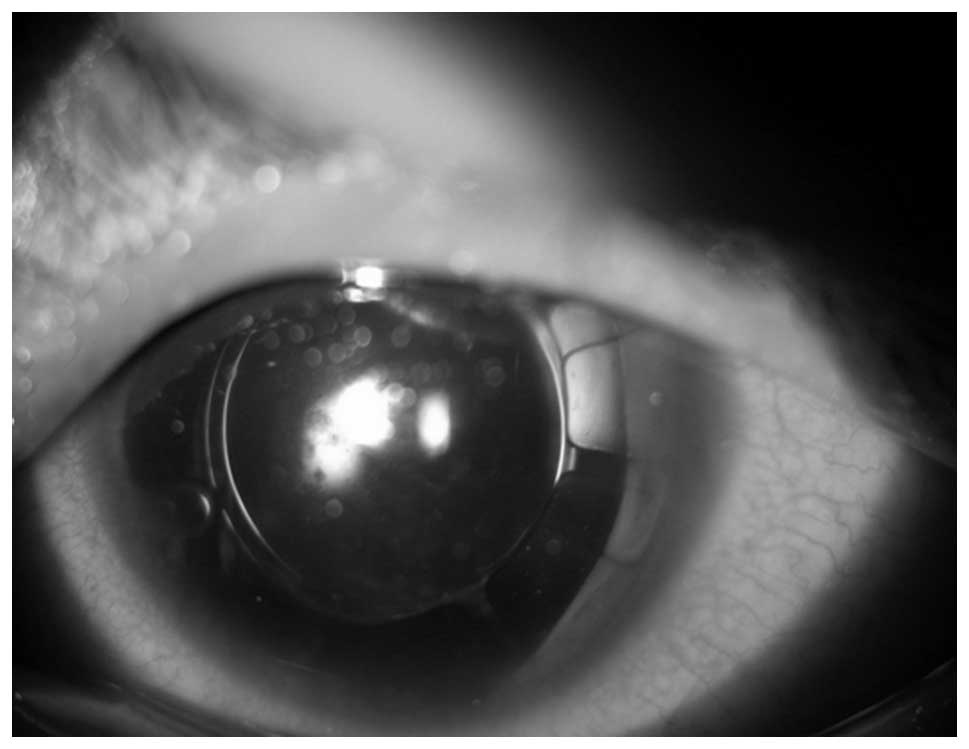
Artificial iris and IOL implantation
Among the 12 patients treated with artificial iris
and IOL implantation into the lens capsule, the corrected visual
acuity of the two congenital cataract patients was <0.1 due to
amblyopia. In the remaining 10 patients, the corrected visual
acuity was 0.1–0.4 for six patients, 0.5–0.8 for three patients and
>0.8 for one patient. There was no occurrence of photophobia.
The artificial iris and IOL did not shift in the follow-up visit.
The artificial iris constituted or complemented the coloboma iris,
and the location of the IOL in the capsular bag did not shift
(Fig. 3).
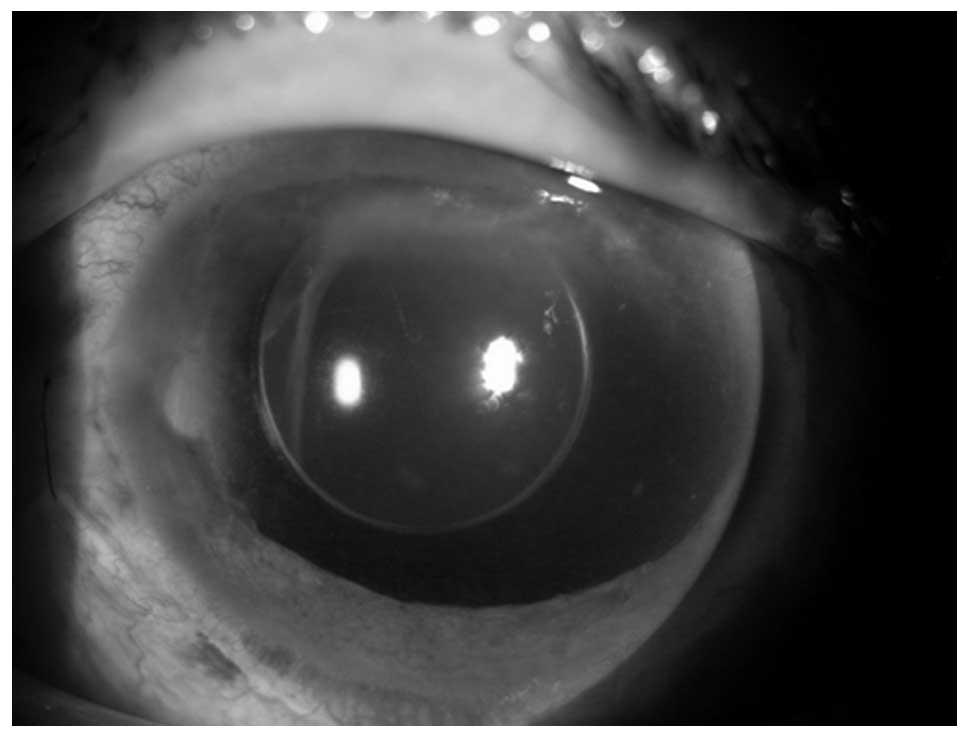
Of the 27 patients treated by IOL with iris
implantation into the ciliary groove, the corrected visual acuity
of five patients was <0.1. In addition, 14 patients had a
corrected visual acuity of 0.1–0.4 and eight had a corrected visual
acuity of 0.8. Of the 27 patients, 18 presented with no
photophobia, and nine patients presented with slight photophobia.
The IOL and optical parts shifted slightly in three patients. The
IOL with iris was located in the ciliary sulcus and was well placed
in the center. The patients’ photophobia improved to varying
degrees following surgery (Fig.
4).
Early postoperative complications
Early postoperative complications included hyphema,
increased intraocular pressure and uveitis, which were improved
following pharmacotherapy. The IOL and optical parts shifted
slightly in three patients.
Discussion
Researchers have attempted several different
surgical techniques to solve the problems associated with IOL
implantation and to improve the photophobic conditions of patients
with iris coloboma. Previous studies have used a lid suture
(7), corneal interlamellar dye
(8) and colored corneal contact
lenses (9) in order to solve
photophobia following surgery. However, these methods have led to
an unsatisfactory appearance with corneal discoloration and patient
intolerance (7,10,11).
To date, various surgical techniques and intraocular implantation
methods have been developed.
When the extent of the iris coloboma is small, it is
possible to directly suture the existing iris and reconstruct the
pupils. In the present study, this surgical technique was applied
to patients with an iris coloboma of small range, and whose
remaining iris was capable of being sutured. This technique
involves a simple surgery with no excessive pulling of the iris and
minimizes the harm to the corneal endothelium and any reaction from
the iris. The surgical techniques were chosen based on the
condition of the phacocele (4).
When the surplus iris was atrophic to varying degrees and the range
of the iris coloboma was small, it was not possible to suture the
iris to form a round pupil and decrease the patients’ photophobia.
Thus, annular suturing of the iris using a polypropylene line was
conducted. This technique may adequately utilize the remaining iris
in order to reconstruct the pupils. It may also be a requirement
for IOL implantation into the anterior chamber (12). For patients with a healthy
phacocele, and whose crystalline lens was not shifted or had only a
slight shift, IOL surgery with artificial iris implantation into
the phacocele is the ideal technique for the treatment of iris
coloboma with a cataracts. This technique fits in much the same
position as normal physiology. Papillary block and a shift in the
iris diaphragm or IOL rarely occurred. Furthermore, there was no
friction with the ciliary body or remaining iris. Thus, the
inflammatory response was low following surgery. Additionally this
surgery is minimally invasive, and is achieved using a general
clear corneal incision to the cataract (11). When the iris and phacocele were
seriously damaged, the IOL technique, with the iris fixed in the
ciliary groove, was used. Further postoperative complications were
observed with this technique, such as intraocular hemorrhaging,
inflammatory response and secondary glaucoma, due to the large size
of the implant and brittle character (13,14).
Other than the previously mentioned methods, other
surgical techniques have been used to solve the problems associated
with IOL implantation in patients with iris coloboma, including the
following: i) A prosthetic iris system, which may be capable of
solving the aesthetic problems and photophobia associated with iris
coloboma, as it is possible to make a personalized prosthetic iris
that matches with the remaining iris with respect to position,
size, and color (15). ii) An
anterior chamber IOL with iris, in which an outer border of
artificial iris acts as a holding device for the IOL positioned at
the center of the implant. This IOL is implanted into the anterior
chamber, and the holding device is fixed to the remaining iris
(16). iii) An artificial iris and
IOL with haptic parts, comprising a central IOL encircled by an
artificial iris with a slender appendage used to fix the implant to
the ciliary sulcus (17).
Following the rapid development of surgical
techniques and intraocular implants, various methods have been made
available for the treatment of patients with iris coloboma, wherein
the implantation of an IOL is necessary. Once the range or degree
of iris coloboma, the integrity of the phacocele, surgical skill,
risk and cost have been estimated, the selection of various
surgical techniques for solving the problems with the patients’
vision and photophobia is possible.
References
|
1
|
Eagle RC: Congenital, developmental, and
degenerative disorders of the iris and ciliary body. Principles and
Practice of Ophthalmology. Clinical Practice. Albert DM and
Jacobiec FA: 2nd edition. WB Saunders; Philadelphia, PA: pp.
1151–1153. 2000
|
|
2
|
Beekhuis WH, Drost NH and van der
Velden/Samderubun EM: A new treatment for photophobia in
posttraumatic aniridia: a case report. Cornea. 17:338–341. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Palacz O, Lubiński W and Barnyk K:
Implantation of posterior chamber lenses with trans-scleral
fixation. Klin Oczna. 101:433–436. 1999.(In Polish).
|
|
4
|
Kim JH, Kang MH, Kang SM and Song BJ: A
modified iris repair technique and capsular tension ring insertion
in a patient with coloboma with cataracts. Korean J Ophthalmol.
20:246–249. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Migneco MK: Contact lens management of
aniseikonia and photophobia induced by trauma. Eye Contact Lens.
31:252–253. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Cionni RJ, Karatza EC, Osher RH and Shah
M: Surgical technique for congenital iris coloboma repair. J
Cataract Refract Surg. 32:1913–1916. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Artificial iris-lens diaphragm in
reconstructive surgery for aniridia and aphakia. Osher RH and Burk
SE: Cataract surgery combined with implantation of an artificial
iris. J Cataract Refract Surg. 25:1540–1547. 1999.PubMed/NCBI
|
|
8
|
Burris TE, Holmes-Higgin DK and
Silvestrini TA: Lamellar intrastromal corneal tattoo for treating
iris defects (artificial iris). Cornea. 17:169–173. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Chung MY, Miller KM and Weissman BA:
Morcher iris reconstruction lens and rigid contact lens for
traumatic aniridia. Eye Contact Lens. 35:108–110. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Hanumanthu S and Webb LA: Management of
traumatic aniridia and aphakia with an iris reconstruction implant.
J Cataract Refract Surg. 29:1236–1238. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Mavrikakis J and Casey JM:
Phacoemulsification and endocapsular implantation of an artificial
iris intraocular lens in traumatic cataract and aniridia. J
Cataract Refract Surg. 28:1088–1091. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
de Keizer RJ, Razzaq L, Tassignon MJ and
Verbeek AM: Iris melanoma in a child treated with iridectomy and a
phakic iris repair implant lens: a case report of 8 years
postoperative follow-up. Br J Ophthalmol. 94:953–954.
2010.PubMed/NCBI
|
|
13
|
Reinhard T, Englhardt S and Sundmacher R:
Black diaphragm aniridia intraocular lens for congenital anirida:
long-term follow-up. J Cataract Refract Surg. 26:375–381. 2000.
View Article : Google Scholar
|
|
14
|
Srinivasan S, Yuen C, Watts M and Prasad
S: Endocapsular iris reconstruction implants for acquired iris
defects: a clinical study. Eye (Lond). 21:1109–1113. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Burk SE, Da Mata AP, Snyder ME, Cionni RJ,
Cohen JS and Osher RH: Prosthetic iris implantation for congenital,
traumatic, or funcional iris deficiencies. J Cataract Refract Surg.
27:1732–1740. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Sminia ML, Odenthal MP, Gortzak-Moorstein
N, Wenniger-Prick LJ and Völker-Dieben HJ: Implantation of the
Artisan iris reconstruction intraocular lens in 5 children with
aphakia and partial aniridia caused by perforating ocular trauma. J
AAPOS. 12:268–272. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Pozdeyeva NA, Pashtayev NP, Lukin VP and
Batkov YN: Artificial iris-lens diaphragm in reconstructive surgery
for aniridia and aphakia. J Cataract Refract Surg. 31:1750–1759.
2005. View Article : Google Scholar : PubMed/NCBI
|