Introduction
In developing countries, tuberculosis (TB) is common
and may involve any system, including the respiratory,
gastrointestinal, cardiac, central nervous, musculoskeletal and
genitourinary systems. The data from World Health Organization
shows that in 2010, there were between 8.5 and 9.2 million cases of
TB globally, equivalent to 128 cases per 100,000 of the population
(1). The greatest amount of the
estimated number of cases occurred in Asia (59%) and Africa (26%)
(1). Pulmonary TB is the most
common. The urinary system has been reported to be the second most
commonly affected site of extrapulmonary TB (2). Due to diverse and atypical clinical
manifestations, urinary TB is easy to misdiagnosis. The positive
diagnostic rates of acid-fast bacilli in urine, intravenous
excretory urograms (IVUs) and B ultrasounds are limited. Computed
tomography (CT) scans are feasible and the mainstay for
investigating possible urinary TB. In the present study, two cases
of renal TB with markedly different clinical manifestations and CT
features are reported. Informed consent was obtained from the
patients. THe study was approved by the Biological and Medical
Ethics Committee of Puai Hospital, Tongji Medical College, Huazhong
University of Science and Technology (Wuhan, China).
Case reports
Case 1
A 63-year-old female was admitted to the Department
of Nephrology at the Puai Hosipital (Wuhan, China) with symptoms of
pain in the right loin for two months and fever for one day. The
patient had not experienced coughing, hemoptysis, weight loss,
night sweats or TB contact, but did have a history of hypertension
and diabetes mellitus. There was no past or family history of TB.
The patient had a temperature of 39.0°C, a blood pressure of 186/84
mmHg and tenderness of the right loin. Laboratory results showed a
white blood cell (WBC) count of 20.13×109/l (84.5%
neutrophils and 9.9% lymphocytes) and hemoglobin and platelet
levels were normal. Urine tested positive for WBCs, and no urinary
protein or microscopic hematuria was detected. Liver and renal
functions were normal. Purified protein derivative (PPD) and TB
antibody tests were negative. Staphylococcus aureus growth
was observed in blood culture and Enterococcus faecalis
growth was observed in uric culture. Other serological tests for
antinuclear antibodies, rheumatoid factor and HIV were negative.
Chest X-ray and abdominal ultrasound observations were normal.
Empiric antibiotic therapy of intravenous linezolid, norvancomycin
and imipenem was administered but was not successful. Symptoms of
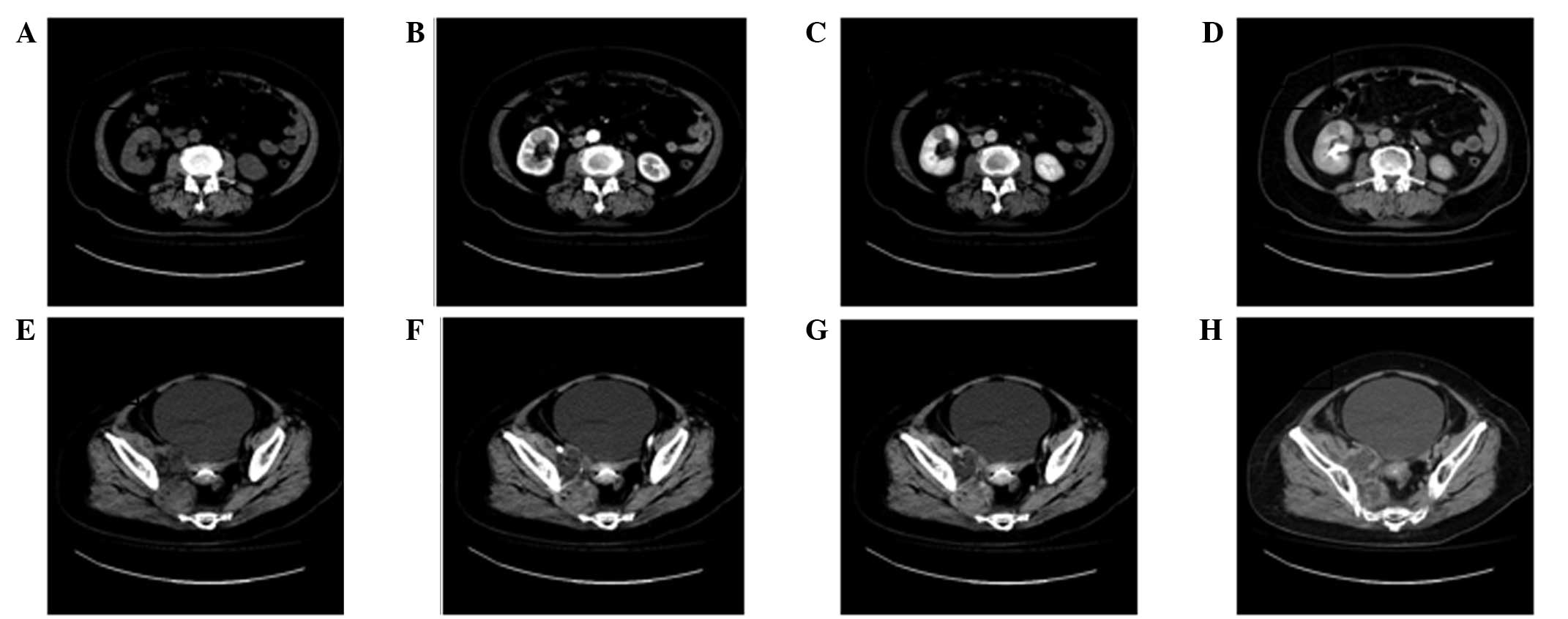
pain in the right loin and fever remained. An abdominal CT scan was
then performed, which identified a low density focus (1.9×2.1 cm)
in the lower pole of the right kidney and an iliopsoas abscess
(Fig. 1). On the basis of clinical
and laboratory observations, renal TB and iliopsoas abscess were
suspected. The patient was treated with the anti-TB agents
isoniazid (Xinyi, Shanghai, China), rifampicin (Yanan, Shanghai,
China) and ethambutol (Hongqi, Shenyang, China). One week later,
the body temperature had decreased to normal and the pain had
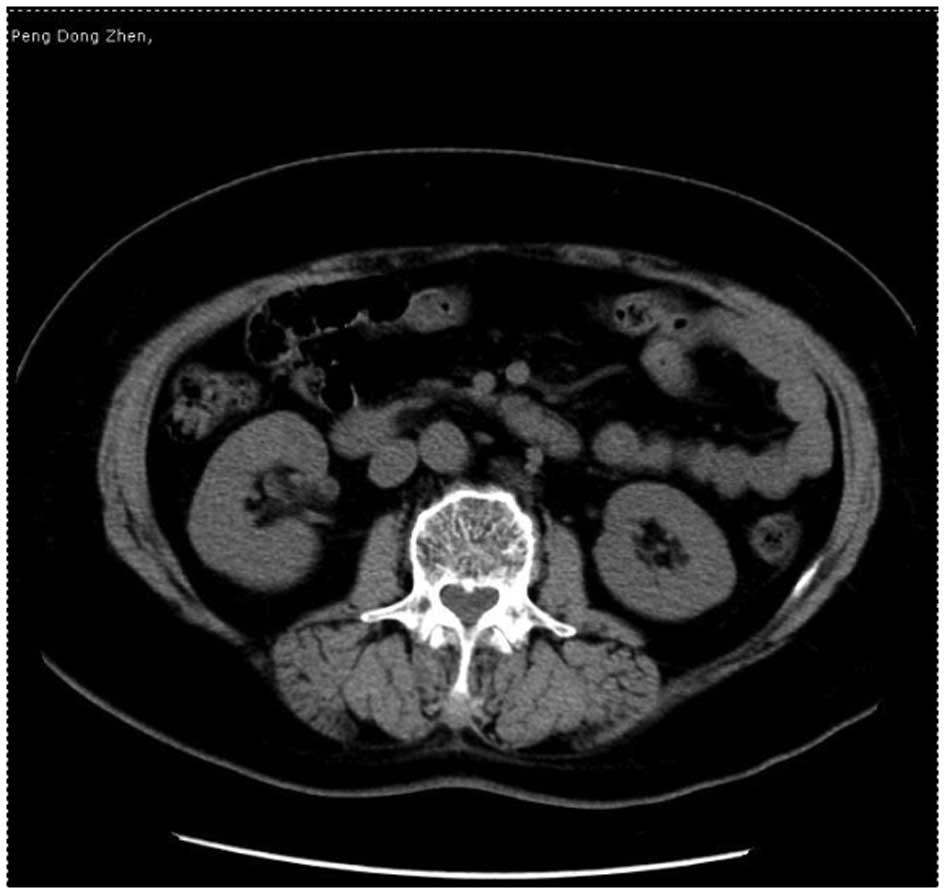
alleviated. After two months, repeated abdominal CT scans were
performed and the low density focus and iliopsoas abscess had
disappeared (Fig. 2).
Case 2
A 53-year-old male presented with intermittent gross
hematuria for three months and left loin pain for two months. A
presumptive diagnosis of kidney calculi was made. The patient was
treated in a local hospital with antibiotics, which were
ineffective. The patient was admitted to the Department of
Nephrology at the Puai Hospital (Wuhan, China). The patient had a
history of diabetes mellitus, but no past or family history of TB.
Left renal area percussion pain was noted during physical
examination. Clinical tests had the following results: WBC total
count, 6.5×109/l (70.3% neutrophils); hemoglobin, 117
g/l; serum urea, 10.16 mmol/l; serum creatinine, 120.1 μmol/l;
serum uric acid, 400.2 μmol/l; serum calcium, 1.93 mmol/l; serum
phosphorus, 0.88 mmol/l; serum carbon dioxide, 20.9 mmol/l; and
erythrocyte sedimentation rate (ESR), 36 mm/h. Urinary WBC, urine
protein and microscopic hematuria tests were positive. TB antibody
[16 kDa, lipoarabinomannan (LAM) and 38 kDa] tests were positive
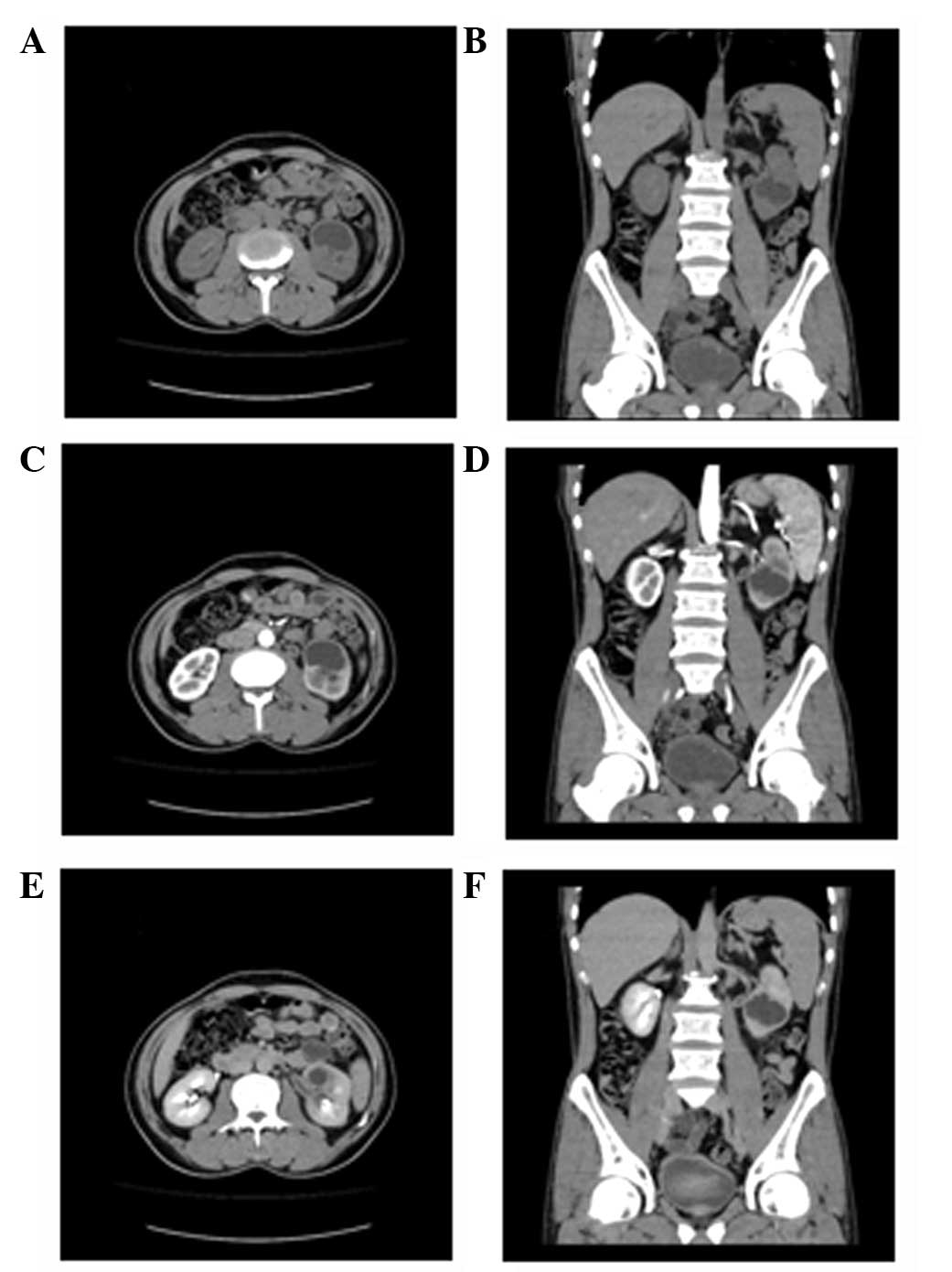
and acid-fast bacilli were detected in the urine. CT scans revealed
a low density focus (3.7×3.3 cm) in the left kidney with a slight
expansion of the pelvis, calices and ureter (Fig. 3). Urinary TB was suspected and the
patient was treated with anti-TB drugs for six months. Following
the treatment, the gross hematuria disappeared and the loin pain
was alleviated.
Discussion
The common manifestations of TB are fever, weight
loss and night sweats. However, in urinary TB these are unusual.
The clinical manifestations of urinary TB are nonspecific,
including back, flank and suprapubic pain, hematuria, increased
urinary frequency and nocturia, which may also indicate a
conventional bacterial urinary tract infection (3). In a study of 31 subjects with
genitourinary TB in Nigeria, 51.6% had fever, 22.6% had dysuria and
others had back, loin or abdominal pain/tenderness (4). TB should be suspected particularly
with sterile pyuria or when there is no response to the usual
antibiotics (3). In the first case
in the present study, the patient had a fever. In addition, uric
and blood cultures were positive, but the bacterium differed. It
was presumed that one or both were contamination.
Based on the presence or absence of underlying
disease, iliopsoas abscesses may be classified into primary (30%
cases) or secondary (70% cases) (5). The most common origin of primary
iliopsoas abscesses is Staphylococcus aureus (88%). Other
organisms, including Streptococci (5%) and Escherichia
coli (3%) may also be involved (6). A primary iliopsoas abscess is caused
by the hematogenous or lymphatic spread of bacteria, while a
secondary iliopsoas abscess is likely to occur from the direct
spread of infection from an adjacent structure (7,8). All
the major abdominal and pelvic structures are in close contact with
the iliopsoas muscle; therefore, any infection in these structures
is able to spread to the iliopsoas muscle. Gastrointestinal
diseases, genitourinary problems, femoral vessel catheterization,
vertebral osteomyelitis and endocarditis may all lead to secondary
ilioposoas abscesses (5). In a
series of 124 patients with secondary iloposoas abscesses, the most
common origin was skeletal infection (50.5%), followed by
alimentary tract (24.8%) and renal infections (17.5%) (8). In the first case of the present
study, an ilioposoas abscess was identified. As there was a low
density focus in the right kidney, it was suspected that the
ilioposoas abscess was secondary.
The clinical manifestations of renal TB are
nonspecific and biopsy of the kidney or abscess is invasive. In one
study, the positive diagnostic rate of acid-fast bacilli in urine
sedimentation was 42.7% and the positive diagnostic rates of IVU
and B ultrasound were 69.1 and 28.3%, respectively (9). CT is the mainstay for investigating
possible urinary TB and has demonstrated a positive diagnostic rate
of 84.3% (9). Features of renal TB
in CT are multiple and complex. In the early stages of the disease,
CT plain scans manifest as a single low density focus with edge
blur, which has a significantly lower density than renal tissue in
enhanced scans and may mimic malignancy. In the two cases of the
present study, a low density focus was observed in the CT scans. As
the disease progresses, spot-like or irregular calcification may be
observed in the focus or at the edge. In a study of 19 cases of
abdominal TB, 50% of CT scans identified renal calcification and
~75% of renal tuberculous involvement was unilateral (10). Expansion of the pelvis, calices and
ureter may be observed in advanced renal TB (11). In the second case of the present
study, the patient presented with gross hematuria. The expansion of
the pelvis, calices and ureter was easy to misdiagnosis as kidney
calculi. Characteristic lobar calcification is often observed in
end-stage TB (tuberculous autonephrectomy) (11).
In conclusion, the clinical and CT manifestations of
renal TB are varied and may be misdiagnosed. In cases where there
is no response to the usual antibiotic treatment in patients with
fever or gross hematuria, TB should be suspected.
References
|
1
|
World Health Organisation. Global
tuberculosis report 2013. World Heath Organisation; Geneva,
Switzerland: 2013
|
|
2
|
Engin G, Acunaş B, Acunaş G and Tunaci M:
Imaging of extrapulmonary tuberculosis. Radiographics. 20:471–488.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Eastwood JB, Corbishley CM and Grange JM:
Tuberculosis and the kidney. J Am Soc Nephrol. 12:1307–1314.
2001.PubMed/NCBI
|
|
4
|
Orakwe JC and Okafor PI: Genitourinary
tuberculosis in Nigeria: a review of thirty-one cases. Niger J Clin
Pract. 8:69–73. 2005.PubMed/NCBI
|
|
5
|
Mallick I, Thoufeeq M and Rajendran TP:
Illiopsoas abscesses. Postgrad Med J. 80:459–462. 2004. View Article : Google Scholar
|
|
6
|
Ricci MA, Rose FB and Meyer KK:
Pyogenicpsoas abscess: worldwide variations in etiology. World J
Sur. 10:834–843. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Adelekan MO, Taiwo SS and Onile BA: A
review of psoas abscess. Afr J Clin Exper Microbiol. 5:55–63.
2004.
|
|
8
|
Navarro López V, Ramos JM, Meseguer V, et
al: Microbiology and outcome of iliopsoas abscess in 124 patients.
Medicine (Baltimore). 88:120–130. 2009.PubMed/NCBI
|
|
9
|
Qiu SP, Liu ZW, Chen JX, Deng CH, Zheng KL
and Mei Y: A clinical study of 281 cases of renal tuberculosis.
Chin J Urol. 23:398–400. 2002.
|
|
10
|
Zissin R, Gayer G, Chowers M,
Shapiro-Feinberg M, Kots E and Hertz M: Computerized tomography
findings of abdominal tuberculosis: report of 19 cases. Isr Med
Assoc J. 3:414–418. 2001.PubMed/NCBI
|
|
11
|
Burrill J, Williams CJ, Bain G, Conder G,
Hine AL and Misra RR: Tuberculosis: a radiologic review.
Radiographics. 27:1255–1273. 2007. View Article : Google Scholar
|