Introduction
Thoracic outlet syndrome (TOS) is a syndrome caused
by compression of the subclavian vein or artery or the brachial
plexus branches that cross the thoracic outlet. The neurovascular
bundle passes through the narrow confines of the interscalene
triangle as well as the costoclavicular triangle and the
subcoracoid space on its way from the neck through the axilla and
into the upper arm (1). In 85–97% of
TOS cases, compression occurs in the brachial plexus (2,3) where it
affects one or more of the nerves that innervate the upper limb
and/or blood vessels as they pass between the chest and upper
extremity. This includes the brachial plexus, the subclavian artery
and, rarely, the subclavian vein, which does not normally pass
through the scalene hiatus.
Fibrous dysplasia (FD) is a developmental skeletal
anomaly in which osteoblasts do not undergo normal morphological
differentiation and maturation, leading to the replacement of
normal marrow and cancellous bone by immature bone and fibrous
stroma (4,5). Between 6 and 20% of monostotic FD
occurs in the ribs, with the second rib being most commonly
affected (6). Approximately 55% of
patients with polyostotic FD have rib involvement (7), usually in the lateral or posterior
aspect of the rib. FD is typically asymptomatic unless the lesion
is large enough to cause local pressure symptoms and/or
pathological fractures (6,8). FD and other tumors of the first rib are
rare and those causing TOS are even more so.
Case reports
Informed consent
Written informed consent was obtained from all of
the patients.
Case 1
A 19-year-old male presented with a history of
hypoesthesia on the ulnar side of his right hand over three months,
at the Department of Hand Surgery, Huashan Hospital (Shanghai,
China). On physical examination, intrinsic muscular atrophy on the
right hand was noted along with hypoesthesia on the ulnar side of
the right forearm, hand, ring finger and little finger. The muscle
strength of adduction and abduction in the second to fourth fingers
was reduced, and thumb opposition function was restricted. The
Wright, Adson's and costoclavicular crushing provocation tests were
positive. In an imaging and nerve study a neck X-ray showed a
lesion in the first rib (Fig. 1),
computed tomography (CT) showed benign bone tumors or tumor-like
lesions in the first rib (Fig. 2),
and a bone scan showed an abnormal uptake of radioactivity in the
first and second right ribs (Fig.
3). Magnetic resonance (MR) imaging of the neck showed abnormal
signals in the right first rib and evidence of bone-borne disease.
Laboratory results were unremarkable. The diagnosis was TOS of the
lower trunk, occupying the first rib on the right side.
Case 2
A 29-year-old male visited the Department of Hand
Surgery, Huashan Hospital with a history of hypoesthesia and
progressive weakness of the left upper limb over six months.
Physical examination revealed no atrophy of the intrinsic muscles
of the hand but the flexion strength of the wrist and finger was
decreased. Thumb opposition function was normal. The Wright and
Adson's provocation tests were positive, while the costoclavicular
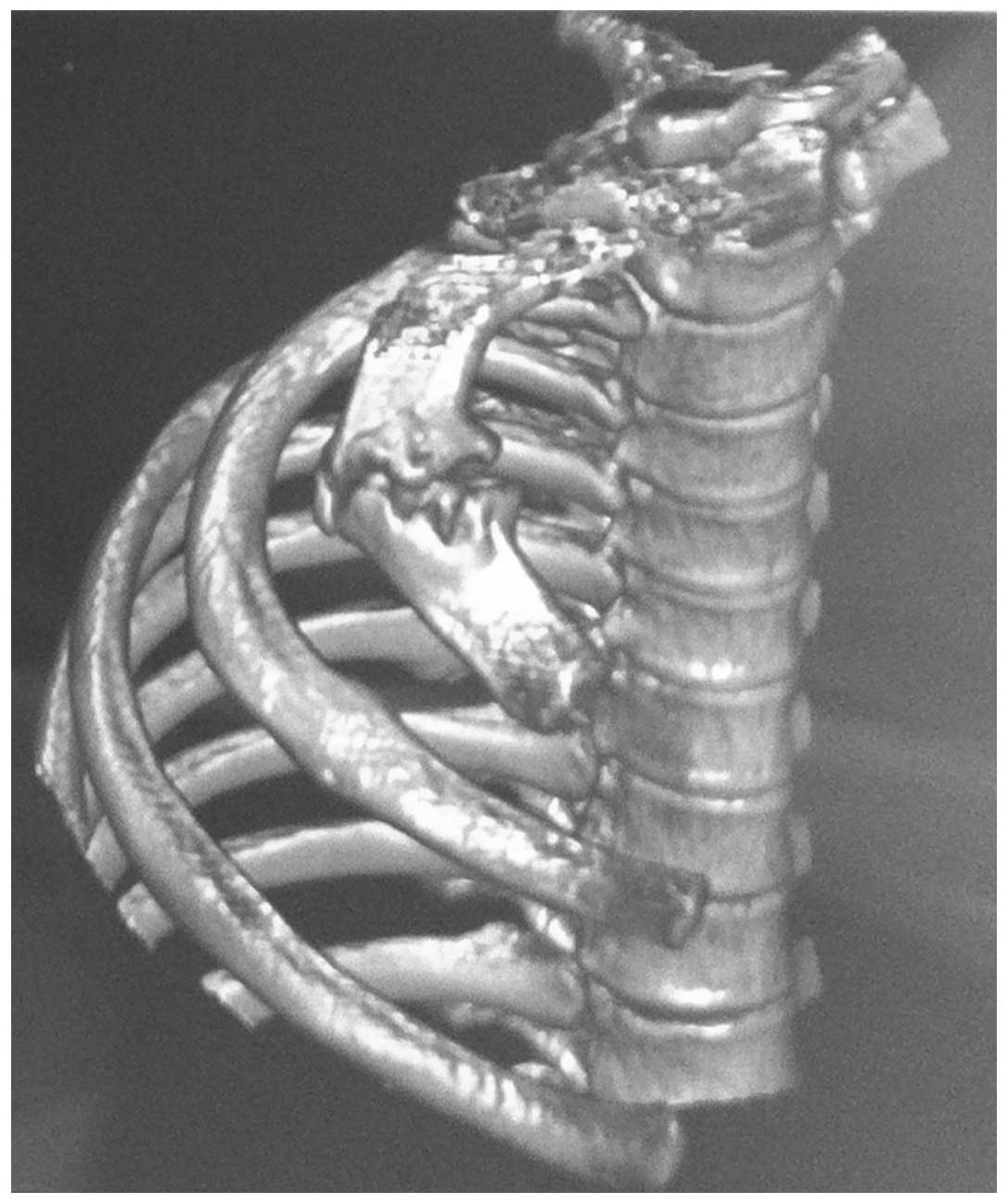
crushing test was negative. A neuroimaging study with
three-dimensional (3D) CT reconstruction showed first rib expansion
(Fig. 4). Neck MR results were
abnormal with a decreased signal on the right in the first rib, and
evidence of bone-borne disease (Fig.
5). Electromyography showed reduced nerve conduction velocity
in the medial cutaneous nerve of the forearm. A chest X-ray showed
a lesion in the first rib (Fig. 6)
and laboratory results were unremarkable. A diagnosis of TOS in the
lower trunk with a mass in the first rib on the left side was
made.
Surgical procedure
Once a diagnosis has been made, surgery should be
contemplated only if conservative management has failed. In the
present two cases, it was clear that TOS was caused by a tumor in
the first rib and that the lesion required resection. There are two
popular procedures for first rib resection: A transaxillary and a
supraclavicular approach. In the current cases a new
thoracoscopy-assisted supraclavicular approach was used. For the
extirpation of the first rib the patient took a supine position.
Using the supraclavicular route, the subclavian vasculature and
brachial plexus were decompressed and released carefully (Fig. 7). The upper edge of the first rib was
stripped, the thoracoscope was placed on the body of the patient
and three ports of entry were made for thoracoscopy access
(Fig. 8). The lower edge of the
first rib was then stripped (Fig. 9)
and the rib was resected in a straightforward manner using the
supraclavicular route (Fig. 10).
Final pathology confirmed FD after two weeks, and the patients did
not have any complications. After a week, when the patients left
the hospital, the symptoms of numbness, hypoesthesia and the
feeling of weakness had improved.
Discussion
TOS caused by a tumor in the first rib is rare and,
to the best of our knowledge, has been reported only 12 times in
the English-language literature over the past one and a half
centuries, with the majority of cases due to osteochondroma
(9). A variety of surgical
approaches have been used, including the intercapulovertebral route
for posterior tumors and thoracotomy, supraclavicular, and
transaxillary approaches for anterior tumors. The first reported
excision of a cervical rib was performed by Coote at St.
Bartholomew's Hospital (London, UK) in 1861 (10). With the description of a simpler
technique of first rib resection in 1966 using an axillary approach
(11), surgical relief of this
common syndrome became technically easier and more acceptable to
the patient and physician (12). In
some previous cases of common TOS in our department, the cervical
or first rib was resected using the single supraclavicular
approach, in order to protect the brachial plexus. However, in the
two cases reported in the present study, expansive lesions were
observed in the first rib, and if isolated and resected using the
single supraclavicular approach a traction of nerves and vessels
may occur. Therefore, our group decided to resect the ribs under
the assistance of thoracoscopy, and more attention was paid during
the supraclavicular incision, in order to protect the nerves and
vessels.
There have been only five reports of TOS caused by
FD and the optimal management of these lesions is unknown (Table I). In all cases removal of the tumor
was associated with amelioration of symptoms.
 | Table I.Thoracic outlet syndrome cases caused
by first rib lesion and the resection approaches taken. |
Table I.
Thoracic outlet syndrome cases caused
by first rib lesion and the resection approaches taken.
| First author, year
(ref)a | Type | Resection |
|---|
| Devin, 1981 (13) | Neurogenic | Subclavicular
approach with a medial clavicular resection |
| Karanjia, 1990
(14) | Neurogenic and
venous | Transaxillary
excision |
| Melliere, 1991
(9) | Neurogenic and
arterial | Supraclavicular
excision of the medial clavicle and first rib |
| de Montpréville, 1995
(15) | Subclavian
vessels |
Transcervical-thoracic approach with
resection of the medial clavicle |
| Kemp, 2012 (16) | Neurogenic | Thoracotomy |
In conclusion, in cases of TOS caused by FD in the
first rib, particularly with expansive growth, the tumors are
difficult to resect from supraclavicular or transaxillary
approaches. Thoracotomy may lead to greater surgical injury and a
longer recovery time. In these cases consideration should be given
to a thoracoscopy-assisted supraclavicular approach in order to
obtain full vascular/nerve control and a cleaner stripping of the
lower edge in the first rib.
References
|
1
|
Pang D and Wessel HB: Thoracic outlet
syndrome. Neurosurgery. 22:105–121. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Roos DB: The thoracic outlet syndrome is
underrated. Arch Neurol. 47:327–328. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Stanton PE Jr, Vo NM, Haley T, et al:
Thoracic outlet syndrome: a comprehensive evaluation. Am Surg.
54:129–133. 1988.PubMed/NCBI
|
|
4
|
Fitzpatrick KA, Taljanovic MS, Speer DP,
et al: Imaging findings of fibrous dysplasia with histopathologic
and intraoperative correlation. Am J Roentgenol. 182:1389–1398.
2004. View Article : Google Scholar
|
|
5
|
Resnick D, Kyriakos M and Greenway GD:
Tumors and tumor-like lesions of bone: imaging and pathology of
specific lesionsDiagnosis of Bone and Joint Disorders. Resnick D:
4. 4th. WB Saunders; Philadelphia, PA: pp. 3833–3848. 2002
|
|
6
|
Kricun ME: Tumors of the ribsImaging of
Bone Tumors. 1st. WB Saunders; Philadelphia, PA: pp. 304–328.
1993
|
|
7
|
Harris WH, Dudley HR Jr and Barry RJ: The
natural history of fibrous dysplasia. An orthopaedic, pathological
and roentenographic study. J Bone Joint Surg Am. 44-A:207–233.
1962.PubMed/NCBI
|
|
8
|
Jeung MY, Gangi A, Gasser B, et al:
Imaging of chest wall disorders. RadioGraphics. 19:617–637. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Melliere D, Ben Yahia NE, Etienne G, et
al: Thoracic outlet syndrome caused by tumor of the first rib. J
Vasc Surg. 14:235–240. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Coote H: Exostosis of the left transverse
process of the seventh cervical vertebra, surrounded by blood
vessels and nerves, successful removal. Lancet. 1:360–361. 1861.
View Article : Google Scholar
|
|
11
|
Roos DB: Transaxillary approach for first
rib resection to relieve thoracic outlet syndrome. Ann Surg.
163:354–358. 1966. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Roos DB: Experience with first rib
resection for thoracic outlet syndrome. Ann Surg. 173:429–442.
1971. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Devin R, Branchereau A, Pelissier JF, et
al: Thoracic outlet compression syndrome by tumour of the first rib
(authors transl). Chirurgie. 107:749–754. 1981.[(In French)].
PubMed/NCBI
|
|
14
|
Karanjia ND and Sayer RE: Thoracic outlet
syndrome due to monostotic fibrous dysplasia of the first rib. J R
Coll Surg Edinb. 35:1111990.PubMed/NCBI
|
|
15
|
Thomas de Montpréville V, Dulmet E, Ponlot
R and Dartevelle P: Giant bilateral fibrous dysplasia of first
ribs: compression of mediastinum and thoracic outlet. Eur Respir J.
8:1028–1029. 1995.PubMed/NCBI
|
|
16
|
Kemp CD, Rushing GD, Rodic N, et al:
Thoracic outlet syndrome caused by fibrous dysplasia of the first
rib. Ann Thorac Surg. 93:994–996. 2012. View Article : Google Scholar : PubMed/NCBI
|