Introduction
Renal artery aneurysms (RAAs) are a rare condition,
with an incidence rate of 0.01–1%, based on autopsy results and
previous angiographical studies (1).
RAA risk factors include atherosclerosis, fibrodysplasia,
arteritis, trauma and neurofibromatosis (2). The lesions are generally asymptomatic
and incidentally found during investigations performed for
different reasons (3). According to
the size of the aneurysm and clinical presentation, various
management options may be selected, such as observation or surgical
intervention, including aneurysmectomy and repair of RAA.
Nephron-sparing surgery has a similar outcome with radical
nephrectomy for localized renal cell carcinoma (RCC) (4). Coexistence of RCC and RAA in a single
patient is extremely rare. To the best of our knowledge, only three
cases of RCC with ipsilateral RAA have been reported (5,6), with
the patients receiving different treatment to patients with RCC and
contralateral RAA (7).
The present study reports the case of a 57-year-old
patient who exhibited a simultaneous operable RAA and RCC. In
addition, the study discusses possible suggestions for the
treatment of this condition.
Case report
A 57-year-old male patient was referred to the
Second Xiangya Hospital of Central South University (Changsha,
China) complaining of an abdominal pain that had persisted for four
days. The patient was otherwise healthy and denied any history of
trauma. Blood pressure and other physical examination results were
normal. In addition, laboratory tests showed normal levels of blood
urea nitrogen and creatinine, and urinalysis was normal. A computed
tomography (CT) scan revealed a 3.2×3.3 cm2 solid mass
in the upper pole of the right kidney and a 2.2×2.0 cm2
fusiform aneurysm near the renal hilum (Fig. 1A). CT angiography confirmed the
diagnosis of an RAA (Fig. 1B).
Informed consent was obtained from the patient prior
to surgery. A laparoscopic radical nephrectomy was subsequently
performed. Gross specimen examination following surgery confirmed a
2.6×2.3 cm2 aneurysm near the renal hilum, originating
at the first bifurcation, and a 3.0×3.5 cm2 renal mass.
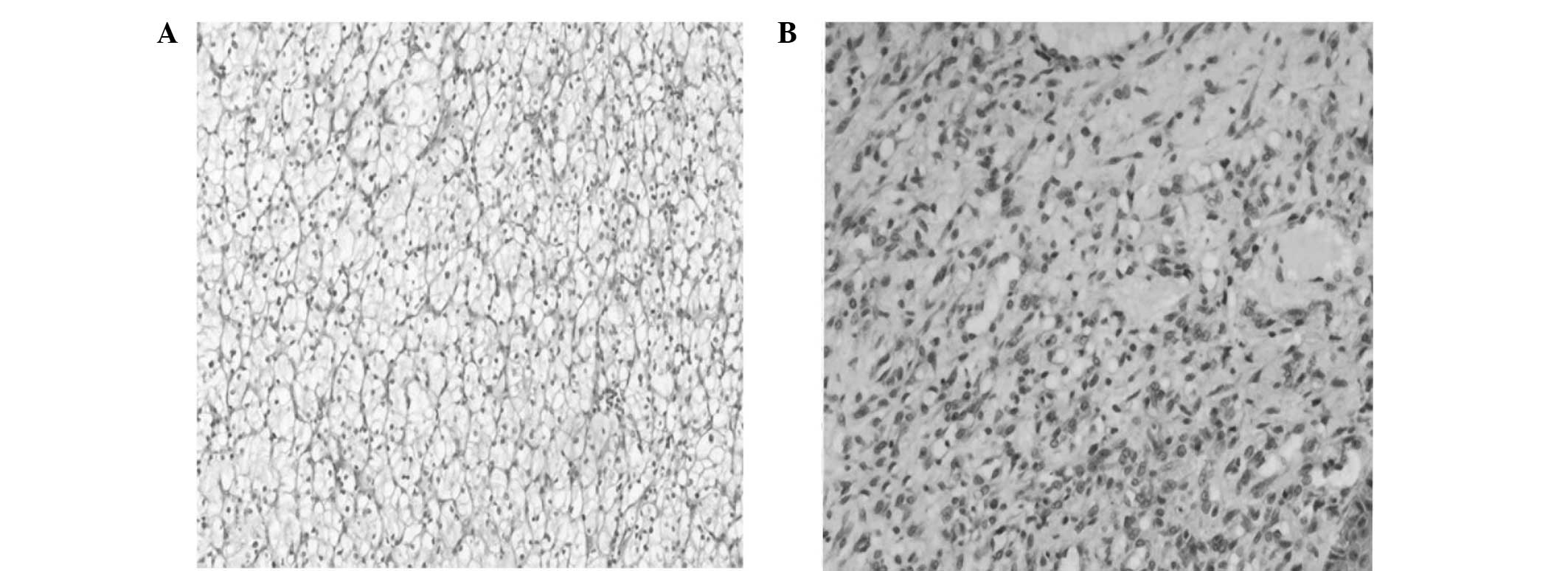
Pathological examination revealed the mass to be RCC (clear cell
type, T1aN0M0 staged) and the aneurysm to be a true aneurysm
(Fig. 2). The patient was
followed-up with renal function examinations and ultrasound scans
every three months, without any further treatment after surgery. At
12 months post-treatment, the patient was shown to be free of local
recurrence or metastasis
Discussion
The exact incidence rate of RAA remains unknown;
however, according to previous studies the incidence rate is ∼0.01%
in the general population (8).
Causes of an RAA include atherosclerosis, fibrodysplasia,
arteritis, trauma and neurofibromatosis (2). Patients with an RAA may be asymptomatic
or present with a variety of symptoms. The majority of patients
present with hypertension and flank pain, and hematuria is
exhibited in certain cases. However, in the present case, abdominal
pain was the only symptom.
There are numerous options for the treatment of
RAAs, including observation, surgical and endovascular repair, and
radical or partial nephrectomy. Asymptomatic patients with an
aneurysm of <2 cm in diameter may have their treatment followed
by radiographic examination (2). The
appropriate surgical intervention for RAAs remains controversial.
Generally, aneurysms of >2 cm in diameter, with symptoms
including flank pain, hematuria or hypertension, are regarded as
cause for surgical intervention (9).
The main surgical interventions for an RAA include aneurysmectomy
with primary closure or patch angioplasty, revascularization and
embolization. Complicated intrarenal aneurysms may require an ex
vivo procedure with arterial revascularization and
autotransplantation of the kidney.
Coexistence of RCC and an RAA in a single patient is
very rare; thus, few approaches for the treatment of this condition
have been described. Hafez et al reported a series of 48
patients with RCC and renal artery disease (RAD) over a 30-year
period; however, only two cases presented with RCC and RAA
simultaneously (10). In order to
improve the understanding of the management of patients with
simultaneous RCC and RAA, a review of the English literature was
conducted using the PubMed database. However, only four cases were
ultimately identified (5–7), as shown in Table I.
 | Table I.Association between RAA and RCC in
previous studies. |
Table I.
Association between RAA and RCC in
previous studies.
| Reference | Age (years) | Gender | Location of RAA and
RCC | Symptom | Treatment | Prognosis |
|---|
| 5 | 49 | Male | Ipsilateral | Hypertension | Radical
nephrectomy | Survival |
| 6 | 56 | Male | Ipsilateral | Hypertension | Radical
nephrectomy | Survival |
| 6 | 70 | Female | Ipsilateral | Hypertension | Radical
nephrectomy | Survival |
| 7 | 47 | Male | Contralateral | Hypertension | Radical nephrectomy
and contralateral aneurysmectomy | Survival |
All four cases had a history of hypertension, and
one patient had a history of trauma. Three out of the four cases
had ipsilateral RCC and RAA and were treated with radical
nephrectomy. The fourth case exhibited RCC with contralateral RAA,
and was treated with a radical nephrectomy and contralateral
aneurysmectomy. The outcomes of all four cases were favorable.
In the present case, the RCC was relatively small
(3.2×3.3 cm2), which indicated a good operative outcome.
In addition, the RAA was relatively large (2.2×2.0 cm2),
which according to the aforementioned criteria, required surgical
intervention. Two surgical approaches were proposed, partial
nephrectomy with RAA repair and radical nephrectomy.
In the majority of patients with RCC and RAD,
nephron-sparing surgery is considered to be the best approach and
several studies have demonstrated excellent clinical results
(11,12). One retrospective study indicated that
RAA repair is feasible and safe (13). However, the total ischemia time of
RAA recovery ranges between 60 and 155 min (median, 70 min) and is
even longer ex vivo (range, 140–450 min; median, 302 min)
due to the complexity of the procedure (13).
In the present case, a partial nephrectomy may have
considerably increased the duration of the procedure and the risk
of an unfavorable patient outcome. In order to avoid this risk, and
in consideration of the patients strong contralateral renal
function, a radical nephrectomy was performed. The patient remained
healthy one year after surgery, with no indications of metastasis
or deficient renal function.
In conclusion, the incidence rate of simultaneous
RCC with an RAA is very low. To the best of our knowledge, there
are only three reported cases of RCC with ipsilateral RAA in
English literature. There are no medical guidelines or
recommendations for this condition. Radical nephrectomy appears to
be the most practical approach at present; however, further
research is required into the efficacy of the various treatment
options for this rare condition.
References
|
1
|
Fleshner NE and Johnston KW: Repair of an
autotransplant renal artery aneurysm: case report and literature
review. J Urol. 148:389–391. 1992.PubMed/NCBI
|
|
2
|
Novick AC: Management of renovascular
disease. A surgical perspective. Circulation. 83:(2 Suppl).
I167–I171. 1991.PubMed/NCBI
|
|
3
|
Ferrante A, Di Stasi C, Pierconti F and
Snide F: Incidental finding of right renal venous aneurysm in a
patient with symptomatic ipsilateral renal carcinoma: a case
report. Cardiovasc Pathol. 14:327–330. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ghavamian R and Zincke H: Open surgical
partial nephrectomy. Sem Urol Oncol. 19:103–113. 2001.
|
|
5
|
Casillas RA, Romero L and Virgilio C:
Coexisting renal cell carcinoma and renal artery aneurysm. Ann Vasc
Surg. 16:353–357. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Selli C, Carini M, Turini D and Schifano
A: Renal cell carcinoma associated with renal artery aneurysm.
Report of two cases. Urol Int. 38:374–377. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ichiyanagi O, Ishigooka M, Suzuki Y, et
al: Renal cell carcinoma with renal artery aneurysm. Int Urol
Nephrol. 30:385–390. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hageman JH, Smith RF, Szilagyi E and
Elliot JP: Aneurysms of the renal artery: problems of prognosis and
surgical management. Surgery. 84:563–572. 1978.PubMed/NCBI
|
|
9
|
Bastounis E, Pikoulis E, Georgopoulos S,
et al: Surgery for renal artery aneurysms: a combined series of two
large centers. Eur Urol. 33:22–27. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Hafez KS, Krishnamurthi V, Campbell SC and
Novick AC: Contemporary management of renal cell carcinoma with
coexistent renal artery disease: update of the Cleveland Clinic
experience. Urology. 56:382–386. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hafez KS, Novick AC and Campbell SC:
Patterns of tumor recurrence and guidelines for followup after
nephron sparing surgery for sporadic renal cell carcinoma. J Urol.
157:2067–2070. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Lerner SE, Hawkins CA, Blute ML, et al:
Disease outcome in patients with low stage renal cell carcinoma
treated with nephron sparing or radical surgery. J Urol.
155:1868–1873. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Seki T, Koyanagi T, Togashi M, et al:
Experience with revascularizing renal artery aneurysms: is it
feasible, safe and worth attempting? J Urol. 158:357–362. 1997.
View Article : Google Scholar : PubMed/NCBI
|