Introduction
The incidence of coronary heart disease (CHD) is
increasing in Chinese society. To date, CHD is among the main
causes of mortality in Chinese adults (1). Since the introduction of coronary
intervention technology, the technique has become one of the
primary methods for the treatment of CHD. Coronary intervention has
been used successfully to treat a large number of patients with
acute myocardial infarction (MI), and the therapy substantially
improves the quality of life of patients with unstable angina
(2). Therefore, the number of
patients undergoing coronary intervention is increasing (3,4).
Concurrently, the prognosis of stenting has significantly improved
as a result of the widespread use of drug-eluting stents and
anticoagulation (2–4). In the Cangzhou region of China, the
number of patients who underwent percutaneous coronary intervention
(PCI) increased rapidly from 102 to 1,628 cases per year between
2000 and 2010 (unpublished data).
In recent decades, lifestyle factors have been
recognized as important determinants of health status and have
increasingly become a focus of research interest worldwide.
Previous studies have demonstrated (5–7) that
healthy lifestyle habits reduce disease and mortality rates, and
that sociodemographic parameters, such as gender, age, marital
status, economical level and paid employment, correlate with a
healthy lifestyle (8,9). In China, the substantial societal
changes brought on by modernization have altered lifestyle habits.
Compared with 10 years ago, Chinese individuals of today eat more,
drink more, smoke more, have increased anxiety and exercise less.
Therefore, the aim of the present retrospective analysis was to
investigate the impact of various daily lifestyle indicators,
including the dinner satiety rate, tobacco use, heavy alcohol use,
sleep pattern, anxiety and exercise, in patients with CHD who had
undergone a stent implantation over a 7-year follow-up period.
Patients and methods
Patients and procedures
In total, 129 consecutive patients with CHD and
indications for PCI and stent implantation, who were admitted to
the Cangzhou Central Hospital at Hebei Medical University
(Cangzhou, China) between March 2005 and March 2006, were recruited
for the study. The patients received lifelong oral aspirin (100 mg
daily) initiating subsequent to the procedure, and clopidogrel (75
mg daily) starting prior to the procedure and ending one year
subsequent to the procedure. The study was conducted in accordance
with the Declaration of Helsinki and with approval from the Ethics
Committee of Hebei Medical University. Written informed consent was
obtained from all the participants. Patients were eligible for
inclusion if they met the following criteria: i) Angiographically
confirmed stenosis of ≥75% in at least one proximal epicardial
coronary artery; and ii) underwent stent implantation according to
the American College of Cardiology/American Heart Association PCI
guidelines (10). Patients were
excluded from the study if they were aged <18 or >70 years,
and had a history of other organic diseases, diabetes, heart
failure or stage III hypertension. In addition, exclusion criteria
included unsatisfactory stent placement, such as poor adherence,
artery dissection and low flow, and mortality or MI within one
month following stent placement. Patients were also excluded if
coronary artery bypass grafting (CABG) was indicated initially,
however, PCI was performed instead.
Data collection and follow-up
Data entered into the database were collected from
patient charts or through bedside inquiry and physical examination.
In-hospital outcome data were complete for all the patients.
Following hospital discharge, the patients were monitored by
telephone, clinic visits and calls to their primary care
physicians; this information was corroborated with hospital
records. The clinical endpoint was a composite of target lesion
revascularization, defined as repeated PCI and CABG. The follow-up
period continued for 7 years (2006–2013), and the success rate was
88.37% (114/129).
Dinner satiety was defined as eating ≥200 g for
dinner almost daily, and tobacco use was defined as smoking ≥10
cigarettes a day. Heavy alcohol consumption was defined as
consuming ≥20 units alcohol at least three times a week or >60
units weekly. Regular sleep was defined as ≥4 days of regular sleep
each week. Anxiety was defined as a Hamilton Depression Rating
Scale score of <17 and a Hamilton Anxiety Rating Scale score or
>14 (11). Exercise was defined
as physical activity ≥3 days a week for a minimum of 1 h.
Groups
Patients were grouped according to the occurrence of
the clinical endpoint and to the association between daily
lifestyle indicators and CHD prognosis following PCI.
Statistical analysis
Median (range), mean (forecast standard deviation)
and percentage values were calculated for the overall sample. The
χ2 test was used to assess differences in the
categorical and continuous baseline variables between the
subgroups.
Independent prognostic variables were assessed using
multivariate logistic regression models that included dinner
satiety, tobacco use, heavy alcohol use, sleep pattern, anxiety and
exercise. P<0.05 was considered to indicate a statistically
significant difference, and statistical analysis was performed
using SPSS software (version 16.0; SPSS, Inc., Chicago, IL,
USA).
Results
Baseline characteristics
During the enrollment period, 129 consecutive
patients with PCI were surveyed. Patients were divided into two
groups according to whether they reached the clinical endpoint. The
repeat (re)-revascularization group included 38 patients who
underwent re-revascularization. The non-revascularization group
included 76 patients who did not reach the clinical endpoint. The
mean age of the patients was 55.9±7.8 years, and 66.7% of the
patients were male. No statistically significant differences were
observed in baseline demographics and clinical characteristics
between the two groups (P>0.05; Tables I and II).
 | Table I.Baseline demographic and clinical
characteristics of the study patients. |
Table I.
Baseline demographic and clinical
characteristics of the study patients.
| Characteristic | Re-revascularization
(n=38) | Non-revascularization
(n=76) | P-value |
|---|
| Agea, years | 55.8±8.21 | 56.4±7.56 | 0.176 |
| Male gender, n
(%) | 27 (71.05) | 49 (64.47) | 0.482 |
| BMIa, kg/m2 | 24.97±4.44 | 24.76±4.44 | 0.79 |
| Family history of
CAD, n (%) | 4 (10.53) | 9 (11.84) | >0.05 |
| Hyperlipidemia, n
(%) | 25 (65.79) | 49 (64.47) | >0.05 |
| Previous stroke, n
(%) | 4 (10.53) | 6 (7.89) | >0.05 |
| Stages I–II
hypertension, n (%) | 26 (68.42) | 45 (59.21) | 0.98 |
| Prior cardiovascular
disease, n (%) |
|
|
|
| Prior
MI | 10 (26.32) | 14 (18.42) | >0.05 |
| Prior
PCI | 4 (10.53) | 7 (9.21) | >0.05 |
| Clinical
presentation |
|
|
|
| Acute MI,
n (%) | 15 (39.47) | 29 (38.16) | >0.05 |
| Unstable
angina, n (%) | 14 (36.84) | 30 (39.47) | >0.05 |
| Chronic
stable angina, n (%) | 7 (18.42) | 12 (15.79) | >0.05 |
| Silent
ischemia, n (%) | 2 (5.26) | 5 (6.58) | >0.05 |
| Left
ventricular ejection fractiona | 50.3±7.9 | 51.4±6.6 | >0.05 |
| Medication at
discharge, n (%) |
|
|
|
|
β-blocker | 22 (57.89) | 39 (51.32) | >0.05 |
| ACEI or
ARB | 19 (50) | 34 (44.74) | >0.05 |
|
Statins | 32 (84.21) | 71 (93.42) | >0.05 |
|
Aspirin | 38 (100) | 76 (100) | >0.05 |
|
Clopidogrel | 36 (94.73) | 70 (92.11) | >0.05 |
| Dinner satiety, n
(%) | 32 (84.21) | 44 (57.89) | 0.005 |
| Tobacco use, n
(%) | 25 (65.79) | 13 (17.11) | 2.01E-07 |
| Heavy alcohol use,
n (%) | 20 (52.63) | 20 (26.32) | 0.006 |
| Regular sleep, n
(%) | 27 (60.53) | 46 (71.05) | 0.270 |
| Anxiety, n (%) | 22 (57.89) | 36 (47.37) | 0.289 |
| Exercise, n
(%) | 2 (5.26) | 21 (27.63) | 0.005 |
| Type of stent, n
(%) |
|
|
|
|
ZETA | 5 (13.16) | 11 (14.47) | >0.05 |
|
HEListent | 2 (5.26) | 4 (5.26) | >0.05 |
|
Driver | 5 (13.16) | 12 (18.42) | >0.05 |
|
Vision | 3 (7.89) | 5 (6.58) | >0.05 |
|
Cipher | 14 (36.84) | 24 (31.58) | >0.05 |
|
Firebird | 9 (23.68) | 20 (26.32) | >0.05 |
| Numbers of stents,
n (%) |
|
|
|
| 1 | 21 (55.26) | 49 (64.47) | >0.05 |
| 2 | 13 (34.21) | 21 (27.63) | >0.05 |
| 3 | 4 (10.53) | 6 (7.89) | >0.05 |
| 4 | 0 | 0 |
|
| Table II.Angiographic characteristics. |
Table II.
Angiographic characteristics.
| Target lesion
coronary artery |
Re-revascularization (n=38) |
Non-revascularization (n=76) |
|---|
| Left main | 0 | 0 |
| Left anterior
descending | 19 | 40 |
| Left
circumflex | 8 | 15 |
| Right | 11 | 21 |
The study flow chart is shown in Fig. 1. At the end of the 7-year follow-up,
six patients had missed their follow-up, two patients had succumbed
to acute MI after three and five years, four patients had succumbed
to a non-cardiac disease and three patients with angina had refused
to undergo a repeat angiography.
Baseline data and procedure
results
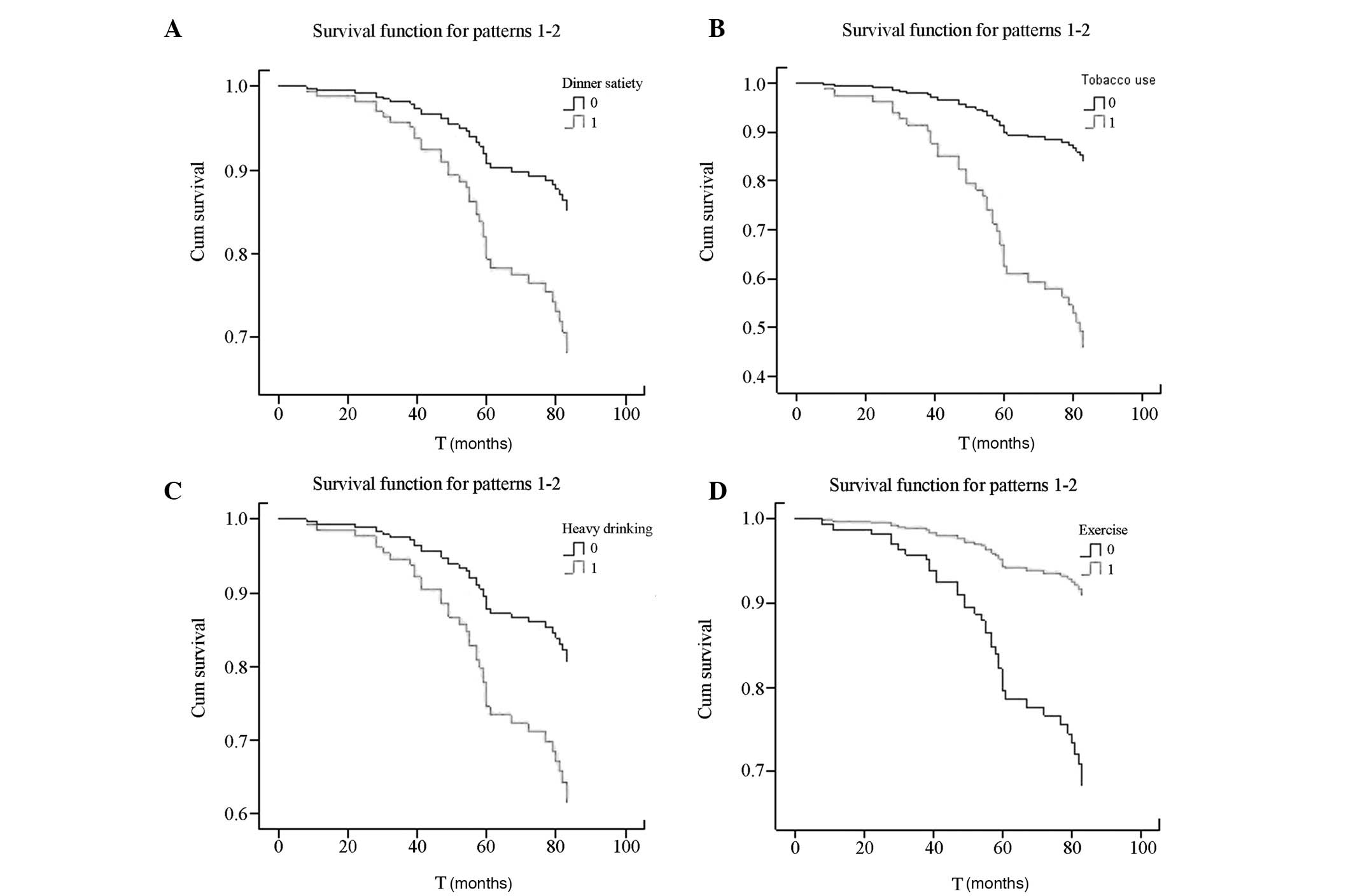
Incidence rates of dinner satiety (84.21%), tobacco
use (65.79%) and heavy alcohol use (52.63%) were significantly
higher in the re-revascularization group compared with the
non-revascularization group (57.89, 17.11 and 26.32%,
respectively). In addition, the exercise rate was significantly
lower in the re-revascularization group (5.26%) compared with the
non-revascularization group (27.63%; P<0.05) (Table I and Fig.
2).
Angiographic follow-up data
A repeat angiography revealed in-stent restenosis in
26% of the patients, stenoses at the entrance to or exit from a
stent in 29% of the patients and new lesions in 19% of the
patients. In 26% of the patients, the original lesions were found
to have deteriorated (Table III
and Fig. 3).
| Table III.Seven-year clinical follow-up. |
Table III.
Seven-year clinical follow-up.
| Follow-up data | Cases, n (%) |
|---|
| Missed
follow-up | 6 (4.65) |
| Mortality | 2 (1.55) |
| Cardiac
mortality | 4 (3.10) |
| Refusal | 3 (2.33) |
|
Re-revascularization (n=38) |
|
| Lesions
aggravated | 10 (26) |
|
In-stent restenosis | 10 (26) |
| New
lesions | 7 (19) |
|
Entrance and exit stenosis of
stent | 11 (29) |
Clinical outcome
A multivariate logistic regression analysis revealed
that dinner satiety, tobacco use, heavy alcohol use and exercise
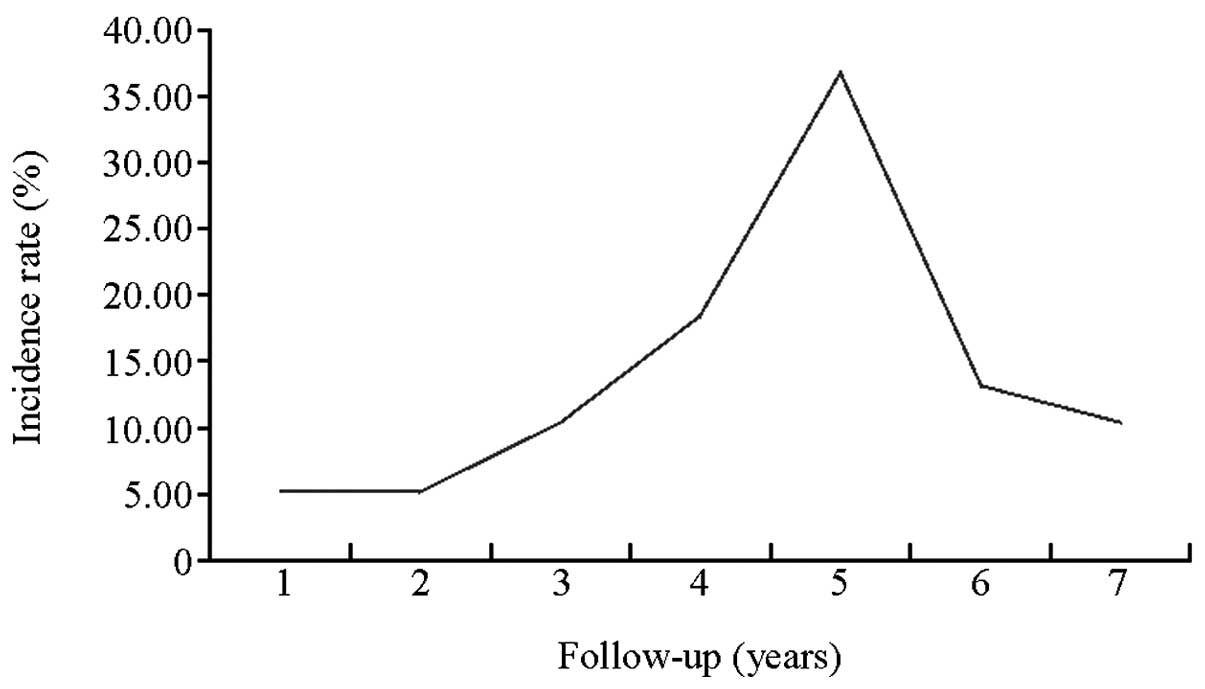
significantly impacted CHD (P<0.05; Table IV). The clinical endpoint was
reached in 55% of the cases between 3 and 5 years of the follow-up
period (Fig. 4).
| Table IV.Multivariate logistic regression
analysis of the prognostic factors for patients with PCI. |
Table IV.
Multivariate logistic regression
analysis of the prognostic factors for patients with PCI.
| Prognostic
factor | OR | 95% CI | P-value |
|---|
| Dinner satiety | 3.32 | 1.06–10.48 | 0.040 |
| Tobacco use | 11.71 | 3.95–34.71 | <0.001 |
| Heavy drinking | 3.74 | 1.27–10.98 | 0.017 |
| Regular sleep | 1.50 | 0.51–4.39 | 0.461 |
| Anxiety | 1.57 | 0.56–4.44 | 0.395 |
| Exercise | 0.14 | 0.02–0.65 | 0.013 |
Discussion
Numerous aspects influence patient prognosis
following coronary stent placement. A previous study (12) focused on a variety of causes for
in-stent restenosis; however, the present study found that the
in-stent restenosis rate (including stenosis at the entrance to and
exit from the stent) was only 55%. In addition, new lesions were
identified in 19% of the cases and deterioration of the original
lesions accounted for 26% of the cases. Thus, patient prognosis
following coronary stent placement was not only found to concern
in-stent restenosis, but was also shown to depend on new lesions
and the deterioration of original lesions. In the present study,
poor daily lifestyle habits were demonstrated to increase the
in-stent restenosis rate, accelerate the progression of the
original lesion and promote the emergence of new lesions.
The evening is an important period for physical rest
and self-healing, in which sympathetic nerve activity decreases and
parasympathetic nerve activity increases, resulting in the normal
secretion and regulation of a variety of circulatory endocrine
factors and hormones (13,14). Anxiety and irregular sleep disrupt
this balance to a certain extent, and eventually impair various
balance and repair mechanisms. The results from the current study
revealed that anxiety and irregular sleep did not significantly
differ between the two groups (P>0.05); however, the incidence
of anxiety and irregular sleep in the two groups was ~50% (Table I). This observation demonstrates that
anxiety and irregular sleep are relatively common phenomena in
patients with CHD, indicating that anxiety and irregular sleep may
be precipitating factors for developing vascular lesions (15–17).
The present study found that the dinner satiety rate
in the re-revascularization group (84.21%) was significantly higher
compared with that in the non-revascularization group (57.89%). A
previous study (18) demonstrated
that dinner satiety can affect sleep, and that high food
consumption during dinner is followed by a series of adverse
consequences. A high fat intake can elevate serum leptin levels and
decrease leptin receptor levels, leading to the leptin resistance
phenomenon (19). Leptin resistance
not only affects the transfer of satiation signals, but also
activates the sympathetic nervous system and affects the stability
of vascular endothelial cells through the endothelin (ET-1)
receptor, a downstream effector of nicotinamide adenine
dinucleotide phosphate oxidase (20,21).
Leptin resistance also promotes endothelial inflammatory factor
activity, which may lead to the development of atherosclerosis and
promote adenosine diphosphate-induced platelet aggregation to form
thromboses, thereby causing acute coronary events (22). Impaired dinner satiety is also one of
the main causes of excess weight and obesity, which are major risk
factors for CHD in the Chinese population (23,24). In
addition, smoking is a well-known independent risk factor for CHD.
The current study demonstrated that tobacco use in the
re-revascularization group (65.79%) was significantly higher when
compared with the non-revascularization group (17.11%). Smoking can
damage vascular endothelial function and stability, promote
myocardial hypoxia and cause coronary artery spasm (25). Furthermore, smoking can induce a
variety of factors, such as thromboxane A2, CD40 and prostacyclin,
that cause angiosclerosis-accelerated plaque formation, which
subsequently induces plaque rupture and thrombosis (26,27). In
a previous study, heavy drinking was found to be a risk factor for
cardiovascular disease (28); the
study found that alcohol consumption had a U-shaped curve
association with cardiovascular disease, particularly the incidence
of MI and CHD (29,30). Heavy drinking affects the normal
function of the body's clotting system and the vascular
endothelium. In addition, increased alcohol consumption can
activate oxidative stress and alter the activities of several
inflammatory cytokines, including ET-1, tumor necrosis factor-α,
interleukin-6 and nitric oxide, subsequently leading to plaque
formation and blood clots in the blood vessels (31–33).
Patients with CHD require exercise; however, the present study
found that just 5.26% of patients in the re-revascularization group
and 27.63% of patients in the non-revascularization group exercised
regularly. Previous studies have shown that adequate exercise
improves blood circulation, prevents thrombosis and embolism,
improves the internal functioning of the body, improves sleep,
relieves anxiety and restores normal nerve and humoral regulation
(34–36).
In the current study, 55% of patients exhibited
revascularization and showed poor daily lifestyle habits during the
3–5 years of the 7-year follow-up. The highest frequency of events
occurred in the fifth year of follow-up. Based on the analysis of
these results, the following hypothesis can be concluded: Among
patients with CHD who undergo stent implantation and do not improve
on their lifestyle choices, 55% of individuals are likely to
require revascularization in the subsequent 3–5-year period.
The present study had several important limitations.
The major limitation was the relatively small number of patients.
The study was a retrospective, randomized, single-blind study,
rather than a double-blind study. In addition, the type of stent
implanted was left to the discretion of the surgeon; thus,
different types of stents were used in different clinical
circumstances and the procedure was not standardized. Finally, few
of the patients who did not require revascularization received
angiographic follow-up.
In conclusion, despite major breakthroughs in the
prevention and treatment of CHD, this disease remains the most
common cause of mortality in the Asian Pacific region (37). PCI with stent placement is the gold
standard for treating patients with CHD; however,
re-revascularization is a recurring problem following PCI.
Currently, there is a large amount of data with regard to in-stent
restenosis; however, in numerous stent patients, deterioration of
the original lesions and new lesion sites have been found to occur
subsequent to the administration of sufficient treatment. In the
present study, daily lifestyle factors were demonstrated to
significantly affect the prognosis of patients with stents.
Therefore, future large-scale clinical trials are required with the
aim of offering more specific treatment guidance.
References
|
1
|
He J, Gu D, Wu X, et al: Major causes of
death among men and women in China. N Engl J Med. 353:1124–1134.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Biondi Zoccai G, Abbate A, D'Ascenzo F, et
al: Percutaneous coronary intervention in nonagenarians: pros and
cons. J Geriatr Cardiol. 10:82–90. 2013.PubMed/NCBI
|
|
3
|
Bangalore S, Gupta N, Guo Y and Feit F:
Trend in the use of drug eluting stents in the United States:
insight from over 8.1 million coronary interventions. Int J
Cardiol. 175:108–119. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Giacoppo D, Baber U and Mehran R: Current
developments in dual antiplatelet therapy after stenting. Minerva
Cardioangiol. 62:261–276. 2014.PubMed/NCBI
|
|
5
|
Nöthlings U, Ford ES, Kröger J and Boeing
H: Lifestyle factors and mortality among adults with diabetes:
Findings from the European Prospective Investigation into Cancer
and Nutrition-Potsdam study. J Diabetes. 2:112–117. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Hu FB, Liu Y and Willett WC: Preventing
chronic diseases by promoting healthy diet and lifestyle: public
policy implications for China. Obes Rev. 12:552–559. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Reddy P, Rankins D, Timoshanko A and
Dunbar JA: Life! in Australia: translating prevention research into
a large-scale intervention. Br J Diabetes Vasc Dis. 11:193–197.
2011. View Article : Google Scholar
|
|
8
|
Krueger PM and Chang VW: Being poor and
coping with stress: health behaviors and the risk of death. Am J
Public Health. 98:889–896. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Menotti A, Puddu PE, Lanti M, Maiani G,
Catasta G and Fidanza AA: Lifestyle habits and mortality from all
and specific causes of death: 40-year follow-up in the Italian
Rural Areas of the Seven Countries Study. J Nutr Health Aging.
18:314–321. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Smith SC Jr, Dove JT, Jacobs AK, et al:
American College of Cardiology; American Heart Association Task
Force on Practice Guidelines. Committee to Revise the 1993
Guidelines for Percutaneous Transluminal Coronary Angioplasty:
ACC/AHA guidelines of percutaneous coronary interventions (revision
of the 1993 PTCA guidelines) - executive summary. A report of the
American College of Cardiology/American Heart Association Task
Force on Practice Guidelines (committee to revise the 1993
guidelines for percutaneous transluminal coronary angioplasty). J
Am Coll Cardiol. 37:2215–2239. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hamilton M: A rating scale for depression.
J Neurol Neurosurg Psychiatry. 23:56–62. 1960. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Eisenstein EL, Anstrom KJ, Kong DF, et al:
Clopidogrel use and long-term clinical outcomes after drug-eluting
stent implantation. JAMA. 297:159–168. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Leproult R and Van Cauter E: Role of sleep
and sleep loss in hormonal release and metabolism. Endocr Dev.
17:11–21. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Copinschi G: Metabolic and endocrine
effects of sleep deprivation. Essent Psychopharmacol. 6:341–347.
2005.PubMed/NCBI
|
|
15
|
Lespérance F, Frasure-Smith N, Théroux P
and Irwin M: The association between major depression and levels of
soluble intercellular adhesion molecule 1, interleukin-6 and
C-reactive protein in patients with recent acute coronary
syndromes. Am J Psychiatry. 161:271–277. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Sherwood A, Hinderliter AL, Watkins LL,
Waugh RA and Blumenthal JA: Impaired endothelial function in
coronary heart disease patients with depressive symptomatology. J
Am Coll Cardiol. 46:656–659. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Pizzi C, Manzoli L, Mancini S and Costa
GM: Analysis of potential predictors of depression among coronary
heart disease risk factors including heart rate variability,
markers of inflammation and endothelial function. Eur Heart J.
29:1110–1117. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Lucassen EA, Zhao X, Rother KI, et al:
Sleep Extension Study Group: Evening chronotype is associated with
changes in eating behavior, more sleep apnea, and increased stress
hormones in short sleeping obese individuals. PLoS One.
8:e565192013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Ku IA, Farzaneh-Far R, Vittinghoff E,
Zhang MH, Na B and Whooley MA: Association of low leptin with
cardiovascular events and mortality in patients with stable
coronary artery disease: the Heart and Soul Study. Atherosclerosis.
217:503–508. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Rajendran K, Devarajan N, Ganesan M and
Ragunathan M: Obesity, Inflammation and Acute Myocardial
Infarction-Expression of leptin, IL-6 and high sensitivity-CRP in
Chennai based population. Thromb J. 10:132012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Knudson JD, Payne GA, Borbouse L and Tune
JD: Leptin and mechanisms of endothelial dysfunction and
cardiovascular disease. Curr Hypertens Rep. 10:434–439. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Elbatarny HS and Maurice DH:
Leptin-mediated activation of human platelets: involvement of a
leptin receptor and phosphodiesterase 3A-containing cellular
signaling complex. Am J Physiol Endocrinol Metab. 289:E695–E702.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Hou X, Lu J, Weng J, et al: Chinese
National Diabetes and Metabolic Disorders Study Group: Impact of
waist circumference and body mass index on risk of cardiometabolic
disorder and cardiovascular disease in Chinese adults: a national
diabetes and metabolic disorders survey. PLoS One. 8:e573192013.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Bays H and Dujovne C: Pharmacotherapy of
obesity: currently marketed and upcoming agents. Am J Cardiovasc
Drugs. 2:245–253. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Gu D, Kelly TN, Wu X, et al: Mortality
attributable to smoking in China. N Engl J Med. 360:150–159. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Barua RS and Ambrose JA: Mechanisms of
coronary thrombosis in cigarette smoke exposure. Arterioscler
Thromb Vasc Biol. 33:1460–1467. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Bliden KP, Dichiara J, Lawal L, et al: The
association of cigarette smoking with enhanced platelet inhibition
by clopidogrel. J Am Coll Cardiol. 52:531–533. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Klatsky AL, Armstrong MA and Friedman GD:
Alcohol and mortality. Ann Intern Med. 117:646–654. 1992.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Emberson JR, Shaper AG, Wannamethee SG,
Morris RW and Whincup PH: Alcohol intake in middle age and risk of
cardiovascular disease and mortality: accounting for intake
variation over time. Am J Epidemiol. 161:856–863. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Goldberg DM, Hahn SE and Parkes JG: Beyond
alcohol: beverage consumption and cardiovascular mortality. Clin
Chim Acta. 237:155–187. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Albert CM, Manson JE, Cook NR, Ajani UA,
Gaziano JM and Hennekens CH: Moderate alcohol consumption and the
risk of sudden cardiac death among US male physicians. Circulation.
100:944–950. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Guan Z, Lui CY, Morkin E and Bahl JJ:
Oxidative stress and apoptosis in cardiomyocyte induced by
high-dose alcohol. J Cardiovasc Pharmacol. 44:696–702. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
O'Keefe JH, Bybee KA and Lavie CJ: Alcohol
and cardiovascular health: the razor-sharp double-edged sword. J Am
Coll Cardiol. 50:1009–1014. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Luk TH, Dai YL, Siu CW, et al: Effect of
exercise training on vascular endothelial function in patients with
stable coronary artery disease: a randomized controlled trial. Eur
J Prev Cardiol. 19:830–839. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Hedbäck B, Perk J, Hörnblad M and Ohlsson
U: Cardiac rehabilitation after coronary artery bypass surgery:
10-year results on mortality, morbidity and readmissions to
hospital. J Cardiovasc Risk. 8:153–158. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Yu CM, Lau CP, Chau J, McGhee S, Kong SL,
Cheung BM and Li LS: A short course of cardiac rehabilitation
program is highly cost effective in improving long-term quality of
life in patients with recent myocardial infarction or percutaneous
coronary intervention. Arch Phys Med Rehabil. 85:1915–1922. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Meng Khoo C and Tai ES: Trends in the
incidence and mortality of coronary heart disease in asian pacific
region: The Singapore experience. J Atheroscler Thromb. 21(Suppl
1): S2–S8. 2014. View Article : Google Scholar : PubMed/NCBI
|