Introduction
Primary graft failure resulting from
ischemia-reperfusion injury (IRI) remains one of the most severe
perioperative complications following lung transplantation. It
accounts for ~30% of patient mortality within 30 days following
lung transplantation (1). A growing
body of evidence suggested that IRI is associated with enhanced
inflammatory responses during reperfusion (2–4). Our
previous study and other reports from the literature have
demonstrated that an increased production of inflammatory
mediators, including tumor necrosis factor-α (TNF-α), interleukin
(IL)-1 and inducible nitric oxide synthase enzyme, which is
triggered by nuclear factor-κB (NF-κB), play a critical role in IRI
development (4–7). Therefore, a therapeutic strategy that
directly inhibits inflammatory responses may alleviate IRI
effectively.
Mesenchymal stem cells (MSCs) are emerging as a
potential cell therapy for various inflammatory diseases. Recent
studies have shown that transplantation of MSCs in animal models of
IRI in the liver, kidney, intestine, heart, brain and lung promotes
organ functional recovery and reduces tissue damages, indicating
that MSC transplantation could be a promising approach to promote
tissue repair or prevent IRI-induced tissue damage (8–15). MSCs
have been found to possess immunomodulatory properties. It has been
suggested that MSCs can mediate immunosuppression in vitro
by suppressing the activation and proliferation of T lymphocytes, B
lymphocytes and natural killer cells, inhibiting the
differentiation of dendritic cells and promoting the formation of
immature dendritic cells that carry inhibitory phenotype (16–18).
Although it is indicated that the protective effects of MSC
transplantation may be associated with MSC-mediated suppression of
inflammation and apoptosis, the molecular mechanism underlying
their beneficial effects remains unclear. In the present study, the
role and underlying mechanism of MSCs in modulating pulmonary
function and inflammation in a rat model of pulmonary IRI (5) was further investigated.
Materials and methods
Animals and study design
All animals were obtained from the Experimental
Center in Zhongshan Hospital, Fudan University (Shanghai, China),
and handling protocols were approved by the Institutional Animal
Care and Use Committee of Zhongshan Hospital, Fudan University.
Male Lewis rats (age, 8–10 weeks; body weight, 250–275 g) were
housed in a room with a constant temperature of 24°C under a 12-h
light/dark cycle. The rats had free access to tap water and food. A
total of 54 rats were divided randomly into the following three
groups (n=18 per group): Sham control, IRI + phosphate-buffered
saline (PBS) and IRI + bone marrow-derived MSCs (BMSCs) groups.
Rats in the sham control group received thoracotomy without IRI.
Rats in the IRI + PBS group underwent 1-h ischemia followed by 2-h
reperfusion and received an intravenous infusion of PBS at the
onset of reperfusion. Finally, rats in the IRI + BMSC group
underwent 1-h ischemia followed by 2-h reperfusion and received an
infusion of BMSCs at the onset of reperfusion.
Preparation of BMSCs
BMSCs Isolation and expansion of were performed as
previously described (19). Briefly,
male Lewis rats were sacrificed, following an overdose of
pentobarbital (100 mg/kg, intraperitoneally), and their bone marrow
was harvested by flushing the cavity of the femurs and tibias with
complete culture medium [Iscove's modified Dulbecco's medium with
10% fetal bovine serum and 1% pen-strep (Invitrogen Life
Technologies, Carlsbad, CA, USA)]. The harvested cells were washed
with complete media and centrifuged at 398.3 × g at 24°C for 5 min.
The supernatant was removed, and the cell pellet was then
re-suspended and cultured in complete media at 37°C with 5%
CO2 and 90% humidity for 3 days. Culture media were
replaced every 3 days. The BMSC population was enriched based on
its ability to adhere to the tissue culture plate. BMSCs were
collected at the third passage and detached using trypsin-free cell
detachment buffer (Invitrogen, Shanghai, China). Cells were
characterized by CD marker expression using flow cytometry (BD LSR
II Flow Cytometer System; BD Biosciences, San Jose, USA) and
immunofluorescence staining. Rat monoclonal CD73 (551123; 1:100),
mouse and rat monoclonal CD29 (561796; 1:100) and rat monoclonal
CD90 (554895; 1:100) were purchased from BD Biosciences, San Jose,
CA, USA). In addition, human and rat monoclonal CD45 (sc-70696;
1:50), and human and rat monoclonal CD34 antibodies (sc-7324; 1:5)
were purchased from Santa Cruz Biotechnology, Inc. (Dallas, TX,
USA). For immunofluorescence staining, BMSCs were cultured on
chamber slides. Following fixation, the cells were stained with
phycoerythrin-conjugated CD90 and fluorescein
isothiocyanate-conjugated CD29 (20). The fluorescent images were captured
using an inverted fluorescence microscope (IX70, Olympus
Corporation, Tokyo, Japan).
Induction of pulmonary IRI
An in vivo hilar clamp model of IRI was
established as previously described (5). The rats were subjected to 1-h ischemia
by left lung hilar occlusion followed by 2-h reperfusion. Briefly,
rats were anesthetized using isoflurane as an inhalational
anesthetic (Baxter, Deerfield, IL, USA) in a drop jar. Following an
intramuscular injection of 0.04 mg atropine (American Reagent Inc.,
Shirley, NY, USA), the rats were endotracheally intubated with a
14-gauge angiocatheter (SURFLO; Terumo Medical Corporation, Tokyo,
Japan) and connected to a pressure-controlled ventilator (Harvard
Apparatus Co., South Natick, MA, USA). The mechanical ventilation
was controlled at a standardized inspired oxygen flow of 0.2 l/min
to achieve a rate of 75–85 breaths/min and a positive
end-expiratory pressure of 2 cm H2O. The rats were
positioned on their right side on a heating pad in order to
maintain a body temperature of 37–38°C. Blood pressure was
monitored with a XBP1000 non-invasive tail blood pressure system
(Kent Scientific Corp., Torrington, CT, USA) following the
initiation of anesthesia and continuously throughout the surgery. A
left posterior lateral thoracotomy was then performed by cutting
the fifth intercostal space to expose the left hilum. The left lung
was mobilized atraumatically, and 50 units of heparin (dissolved in
normal saline solution to obtain a total volume of 0.5 ml) were
administered via the dorsal penile vein. At 5 min after the
administration of heparin, the left hilum was exposed and a 6-0
prolene suture was placed around the hilum using a curved 22-gauge
gavage needle. The two ends of the suture were then threaded
through a 5 mm-long PE-50 tubing (American Health & Medical
Supply International Corp. Co., Ltd., Scarsdale, NY, USA). Ischemia
was initiated by pulling up on the suture and thus pushing the tube
against the hilum and occluding it. The application of a small
surgical clip to the suture on top of the tube followed, to
maintain the tension of the tube against the hilum. The thoracotomy
was then closed, the rats were extubated and the left lung was kept
ischemic for 1 h. After 1 h of ischemia, the rats were
re-anesthetized and re-intubated. Reperfusion was achieved through
the removal of the clip and the tube/suture. Next, the lung was
ventilated and reperfused, and the thoracotomy wound was closed.
The rats were subsequently reperfused for 2 h prior to analysis
(2). Sham animals only received
thoracotomy without hilar occlusion, while the rats that underwent
the induction of IRI received an intravenous infusion of PBS or
BMSCs at the onset of reperfusion.
Intravenous BMSC infusion
Ex vivo-expanded BMSCs were intravenously
injected into the rats via the dorsal penile vein (1×106
cells in 200 µl per rat) at the onset of reperfusion. Harvested
BMSCs were first filtered through a 40-µm filter, to obtain
single-cell suspensions, and kept in cold calcium and
magnesium-free PBS to prevent cell aggregation until injection. The
same amount of PBS was infused to the rats in the IRI + PBS group
in a similar manner.
Assessment of pulmonary function
The pulmonary function was assessed by analyzing
blood gases [arterial oxygen pressure (PaO2)/fraction of
inspired oxygen (FiO2), mmHg] on a Stat Profile pHOx
Plus L autoanalyzer (Nova Biomedical, Waltham, MA, USA). Blood
samples from the left and right pulmonary veins were collected
following reperfusion for blood gas analysis.
Estimation of lung edema
Lung edema was estimated by the lung wet-to-dry
(W/D) weight ratio. After the blood was completely drained, the
left lung was weighed immediately following harvesting, and then
placed in a vacuum oven (at 58°C) to completely dry until a stable
dry weight was achieved. The lung W/D weight ratio was then
calculated.
Evaluation of pulmonary microvascular
permeability
Lung microvascular permeability, which was induced
by IRI was determined using the Evans blue dye extravasation
technique (2). Evans blue (30 mg/kg;
Sigma-Aldrich, St. Louis, MO, USA) was injected into the tail vein
30 min prior to sacrifice. The pulmonary vasculature was then
perfused for 15 min using the isolated and buffer-perfused lung
system to remove extra dye that was lodged in the vasculature, and
then the left lung was harvested. The lung tissues were homogenized
in PBS to extract the Evans blue dye and then centrifuged at 5,000
× g for 30 min at 4°C. The absorbance of the supernatant was
measured at 620 nm using a G Series Vis Light Spectrophotometer
(Suzhou Taomsun Commerce and Trade Co., Ltd., Jiangsu, China).
Absorbance was corrected for the presence of heme pigments as
follows: A620 (corrected) = A620-(1.426 × A740 + 0.030).
Bronchoalveolar lavage (BAL) and
cytokine measurement
The left lung was selectively instilled with 5 ml
sterile saline via the endotracheal tube at the end of the
experiment. A clamp was placed across the right hilum to achieve
selective left lung lavage. The BAL fluid was immediately
centrifuged at 1,500 × g for 10 min at 4°C. The levels of
cytokine-induced neutrophil chemoattractant-1 (CINC-1), IL-1β and
TNF-α in the BAL fluid were analyzed using ELISA (R&D Systems
Inc., Minneapolis, MN, USA), as previously described (5).
Histopathological examination of lung
tissues
Following the sacrifice of the rats, the heart and
lungs were rapidly dissected, and the pulmonary circulation was
perfused via the right ventricle with 20 ml normal saline. The left
lung was then removed, and half of the lung tissue was cut into
three equal sections (cranial to caudal end) and fixed in buffered
formalin for histological analyses. Histopathological examination
was performed on 4-µm paraffin-embedded and formalin-fixed lung
tissue sections. Hematoxylin and eosin-stained tissue sections were
used to determine the IRI score according to previously established
criteria (21). The severity of
acute pulmonary injury was scored between 0 and 4 according to
comprehensive assessments of alveolar congestion, hemorrhage, edema
and infiltration of inflammatory cells in the airspace or the
vessel wall. The scoring system was as follows: Score 0, minimal
damage; score 1, mild damage; score 2, moderate damage; score 3,
severe damage; and score 4, maximal damage. Two pathologists,
blinded to the tissue information, conducted histological
assessments independently. The mean score from the two pathologists
was used for each rat.
Reverse transcription-quantitative
polymerase chain reaction (RT-qPCR)
The mRNA levels of TNF-α, IL-1β, IL-6 and IL-10 in
the rat lung tissues were measured. Total RNA was extracted from
the left lung using TRIzol® reagent (Invitrogen Life Technologies,
Carlsbad, CA, USA), according to the manufacturer's instructions.
Next, complementary DNA was synthesized using oligo (dT) primer and
reverse transcriptase (Takara Bio Inc., Kusatsu, Japan). RT-qPCR
reactions were performed using SYBR® Premix Ex Taq™ (Takara Bio
Inc.) and 0.2 mmol/l of gene-specific primers with the following
thermal cycler conditions: 95°C for 10 min, followed by 40 cycles
of 95°C for 15 sec and 60°C for 1 min. β-actin was used as the
internal control. The sequences for PCR primers are displayed in
Table I. PCR products were analyzed
using agarose gel electrophoresis and the relative mRNA level of
the target gene to the housekeeping gene was calculated based on:
2(β-actin cycle threshold-target gene cycle
threshold).
 | Table I.Primer sequences for reverse
transcription quantitative polymerase chain reaction. |
Table I.
Primer sequences for reverse
transcription quantitative polymerase chain reaction.
| Primer | Forward (5′-3′) | Reverse (5′-3′) |
|---|
| β-actin |
AACCCTAAGGCCAACCGTGAAAA |
CGACCAGAGGCATACAGGGACAA |
| TNF-α |
GCTCTGTGAGGCGACTGGCG |
CCGTAAGGAAGGCTGGGCGC |
| IL-1β |
GCCTCGTGCTGTCTGACCCATG |
AGGGGGCTCCCTAGCATGTCCT |
| IL-10 |
GCCAGACCCACATGCTCCGAG |
GCAGTCCAGTAGATGCCGGGTG |
| IL-6 |
TCTGTCTCGAGCCCACCAGGA |
AACGGAACTCCAGAAGACCAGAGCA |
Statistical analysis
SPSS software, version 16.0 (SPSS, Inc., Chicago,
IL, USA) was used for all statistical analyses. Data are presented
as the mean ± standard error. The comparison among the data was
performed using a one-way analysis of variance, or the Student's
t-test for unpaired data using Bonferroni correction. P<0.05 was
considered to indicate a statistically significant difference.
Results
Isolation and characterization of
BMSCs
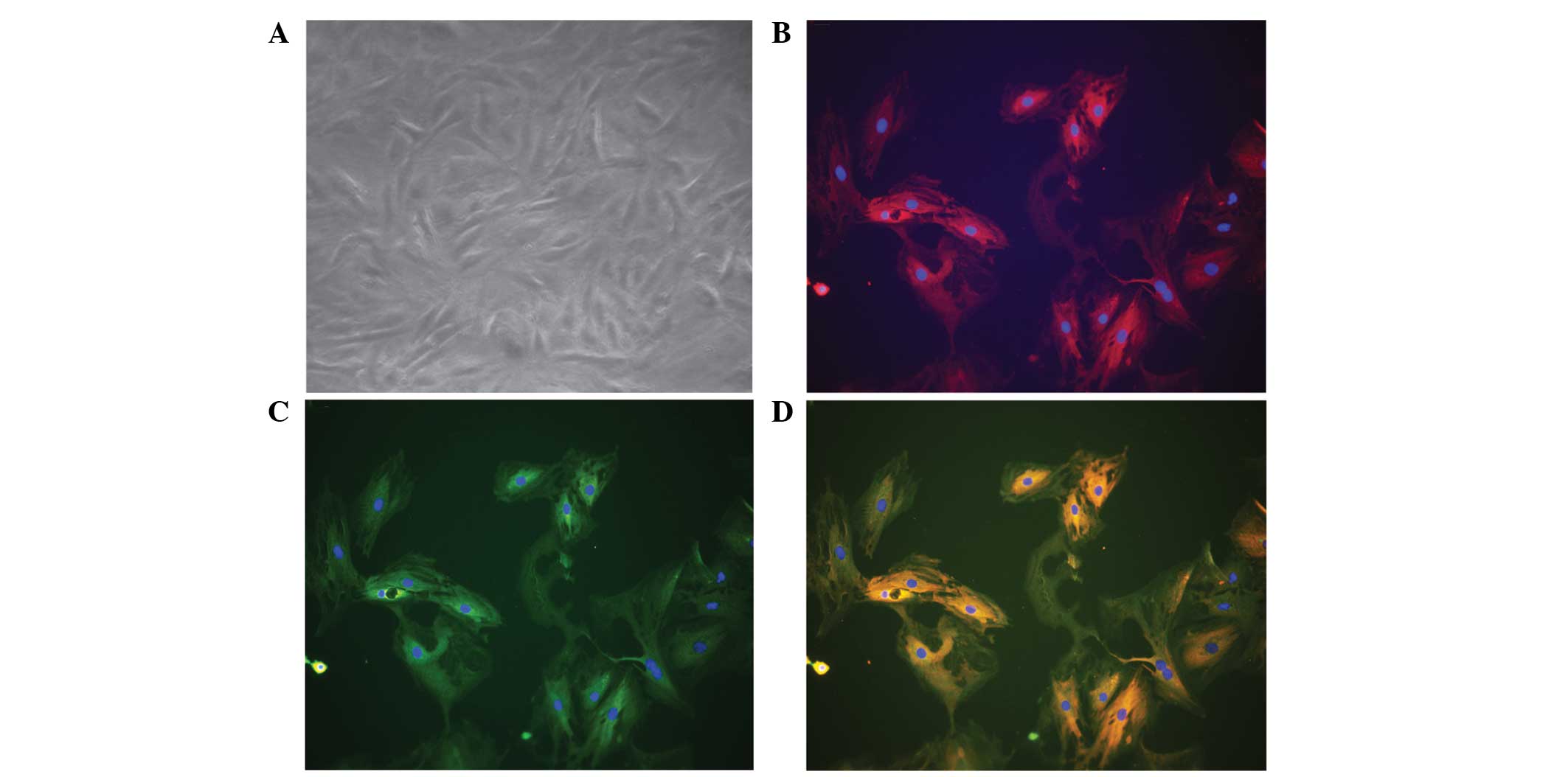
Cultured BMSCs isolated from the bone marrow of male
rats appeared as fibroblast-like spindle shape on tissue culture
plate (Fig. 1A). Immunofluorescence
staining revealed that these cells were positive for CD90 (Fig. 1B and D) and CD29 (Fig. 1C and D). To further characterize
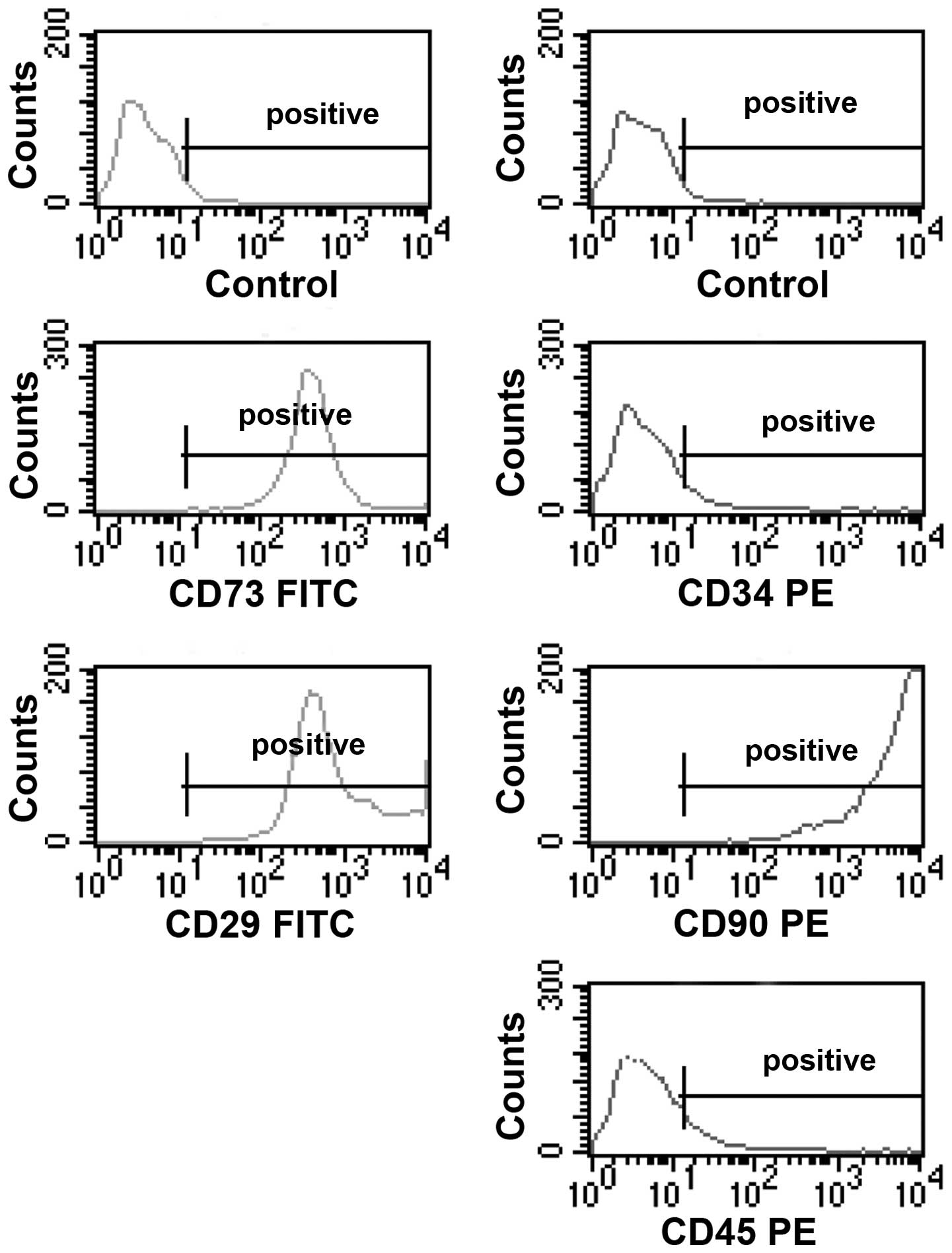
these cells, the expression of a panel of markers, including CD29,
CD34, CD45, CD73 and CD90, were examined by flow cytometry. The
BMSCs were found to be positive for CD29, CD73 and CD90, and
negative for CD34 and CD45 (Fig.
2).
BMSC infusion preserves pulmonary
function and reduces lung edema in rats with pulmonary IRI
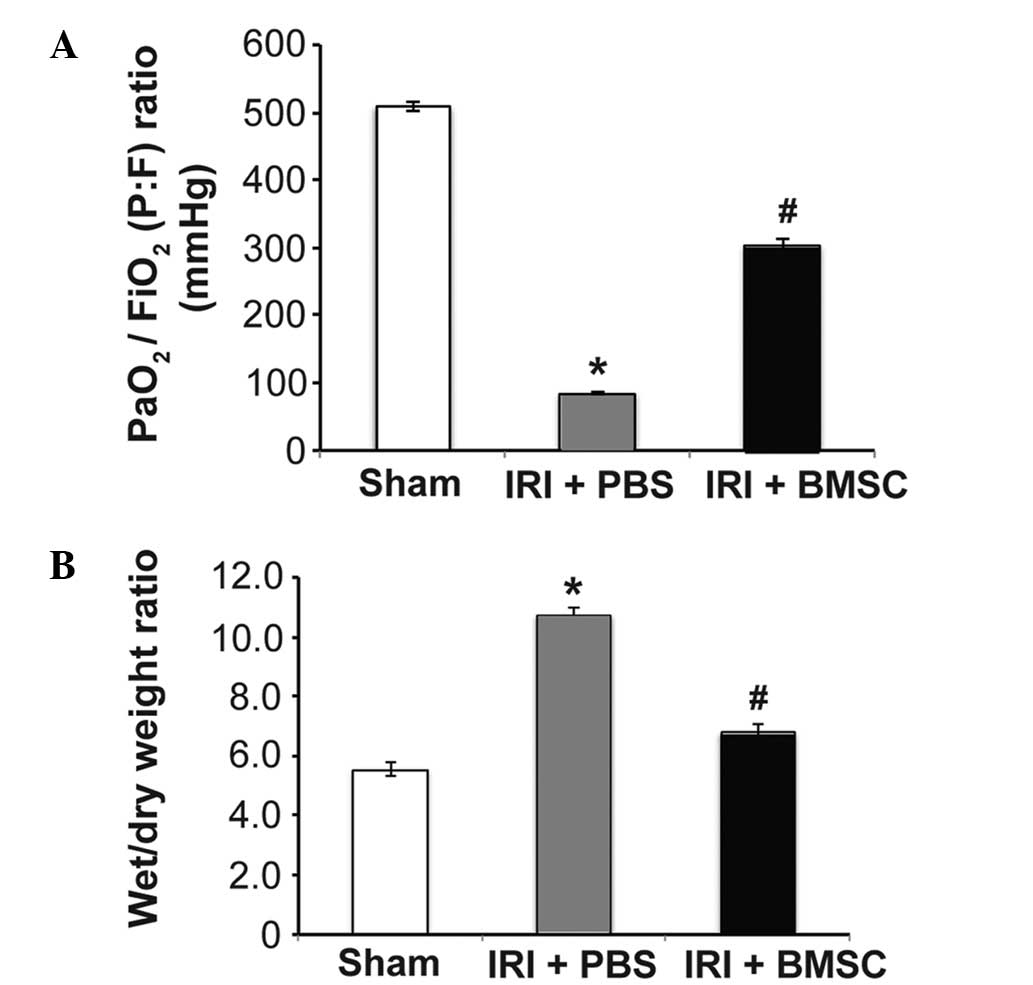
The mean arterial blood oxygenation
[PaO2/FiO2 ratio, mmHg] in rats from the IRI
+ PBS group decreased markedly 2 h after ischemia when compared
with that in rats from the sham control group (P<0.05, Fig. 3A), suggesting that pulmonary function
was severely impaired in rats with IRI. Notably, the mean arterial
blood oxygenation in the IRI + BMSC group was significantly higher
than that in the IRI + PBS group, indicating that BMSC infusion
following ischemia preserved the pulmonary function in rats
(P<0.05, Fig. 3A). In addition to
preserving pulmonary function, BMSC infusion also attenuated lung
edema in rats following ischemia. The W/D weight ratio of lung
tissues was significantly reduced in rats from the IRI + BMSC group
compared with that in rats from the IRI + PBS group (P<0.05,
Fig. 3B). These results suggest that
BMSC infusion may preserve pulmonary function in rats following
ischemia.
BMSC infusion alleviates pulmonary
tissue damage induced by IRI
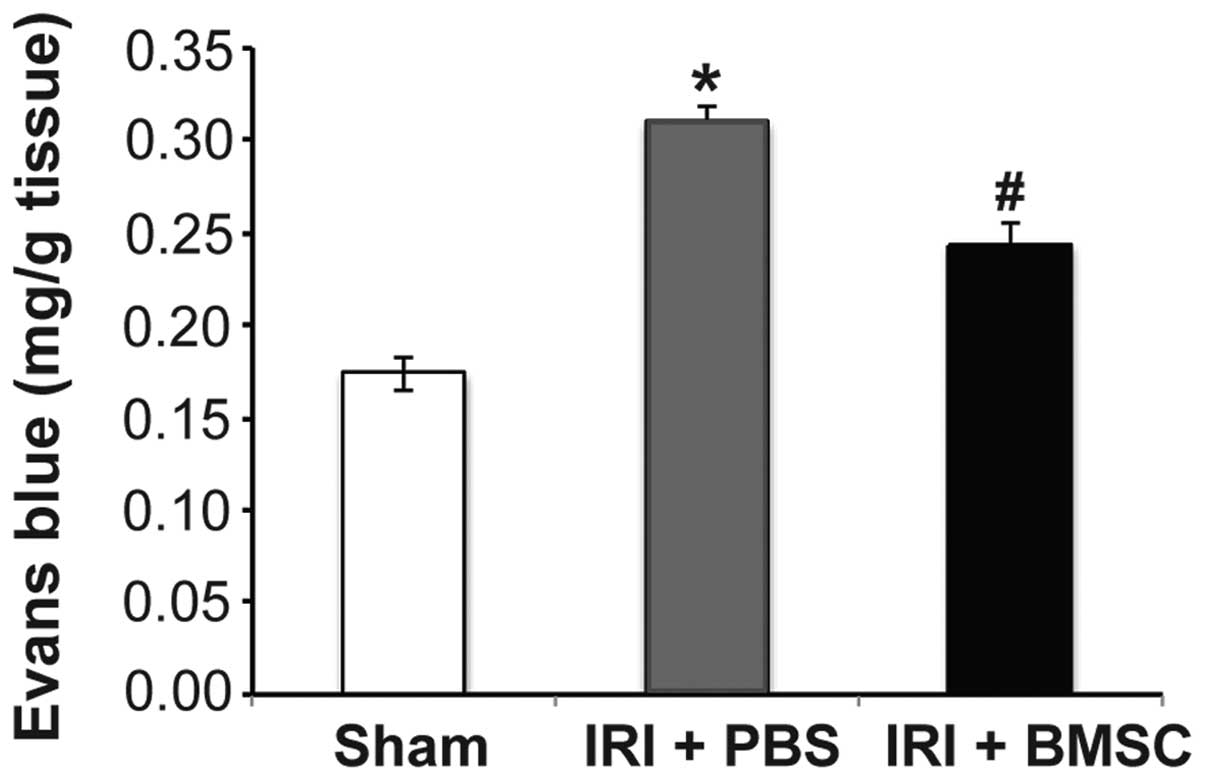
Based on the beneficial effects of BMSC infusion on
pulmonary function, we hypothesized that the pulmonary tissue
damage caused by IRI may be alleviated by BMSC infusion. Indeed,
the Evans blue assay results demonstrated that pulmonary
microvascular leakage was significantly reduced in rats from the
IRI + BMSC group compared with that in rats from the IRI + PBS
group (P<0.05; Fig. 4). To
further verify that BMSC infusion reduces pulmonary tissue damage,
the total injury score of the rats from each group was assessed. A
representative image of a left lung from each group is illustrated
in Fig. 5. Compared with the lung
tissue from the sham control group (Fig.
5A), the lung tissue from the IRI + PBS group was severely
damaged (Fig. 5B). H&E staining
revealed that the alveolar structure was intact in the lung from
the sham control group (Fig. 5D),
while the alveoli in the lung from the IRI + PBS group were
severely injured (Fig. 5E). Although
the alveoli in the lung from the IRI + BMSC group exhibited mild
damage compared with that in the sham control group, the alveolar
structure was maintained (Fig. 5F).
In addition, the lung tissue from the IRI + BMSC group showed
milder damage than the lung tissue from the IRI + PBS group
(Fig. 5C vs. 5B, respectively). The
average pulmonary injury score of the IRI + BMSC group was
significantly lower compared with that of the IRI + PBS group
(P<0.05, Fig. 5G), therefore
indicating that BMSC infusion can alleviate IRI-induced pulmonary
tissue damage.
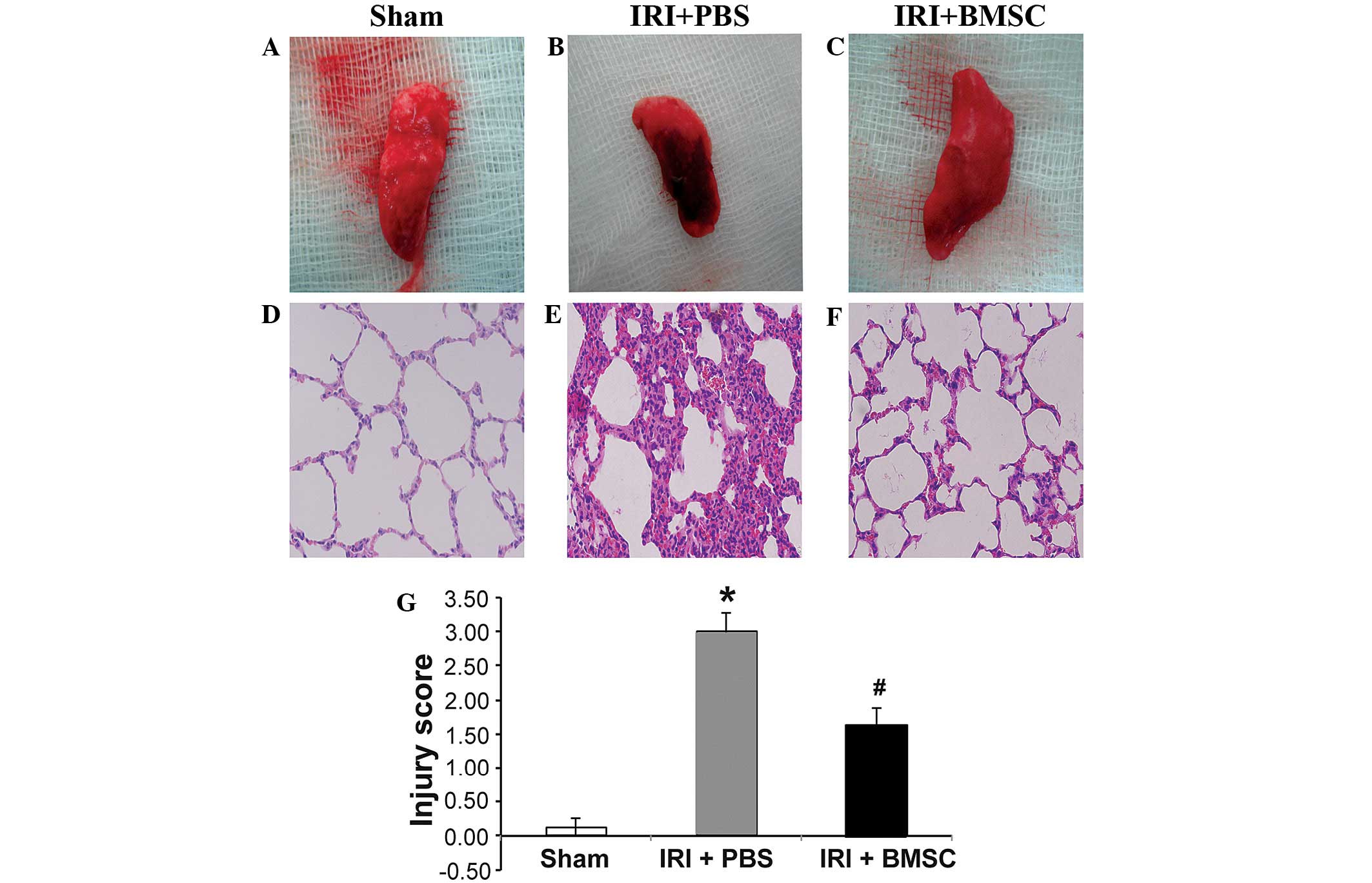 | Figure 5.BMSC infusion decreases IRI-induced
pulmonary tissue damage. Images of left lung tissue from the (A)
sham control, (B) IRI + PBS and (C) IRI + BMSC groups. Images of
the H&E staining in the (D) sham, (E) IRI + PBS and (F) IRI +
BMSC groups. The lungs were harvested following reperfusion.
Photographs of the lungs were captured and then the lung tissues
were fixed and sectioned. The pulmonary tissue sections were
stained with H&E (n=6). (G) BMSC infusion significantly reduced
the pulmonary injury severity score, which was assessed according
to the histopathological analysis of the lung tissues. The
evaluation was conducted by two independent pathologists, blinded
to the tissue information. Data are presented as the mean ±
standard error (n=6). *P<0.05, vs. sham group;
#P<0.05, vs. IRI + PBS group. BMSCs, bone
marrow-derived mesenchymal stem cells; IRI, ischemia-reperfusion
injury; PBS, phosphate-buffered saline; H&E, hematoxylin and
eosin. |
BMCS infusion suppresses pulmonary
inflammation
The mechanism underlying the beneficial effects of
BMSC infusion was subsequently investigated. Based on previous
studies on BMSC transplantation in other diseases (13,16), we
hypothesized that BMSCs alleviates IRI-induced pulmonary tissue
damage in rats by suppressing inflammation. The results from the
RT-qPCR demonstrated that the mRNA expression levels of the
pro-inflammatory cytokines TNF-α, IL-1β and IL-6 were significantly
increased, while the expression of the anti-inflammatory cytokine
IL-10 was significantly reduced in the lung tissue from the IRI +
PBS group, compared with that from the sham control group
(P<0.05; Fig. 6A and B).
Furthermore, BMSC infusion significantly reduced the IRI-mediated
overexpression of the pro-inflammatory cytokines TNF-α, IL-1β, and
IL-6 (P<0.05, Fig. 6A and B).
Notably, BMSC infusion significantly stimulated the IL-10
expression (P<0.05; Fig. 6A and
B). Consistent with the RT-qPCR results, the ELISA results
revealed that the pro-inflammatory cytokines CINC-1, IL-1β and
TNF-α in BAL fluid reached their highest expression levels in the
IRI + PBS group, and that BMSC infusion significantly reduced the
IRI-mediated secretion of these cytokines (P<0.05, Fig. 6C). These findings clearly suggested
that BMSC infusion reduced IRI-mediated inflammation.
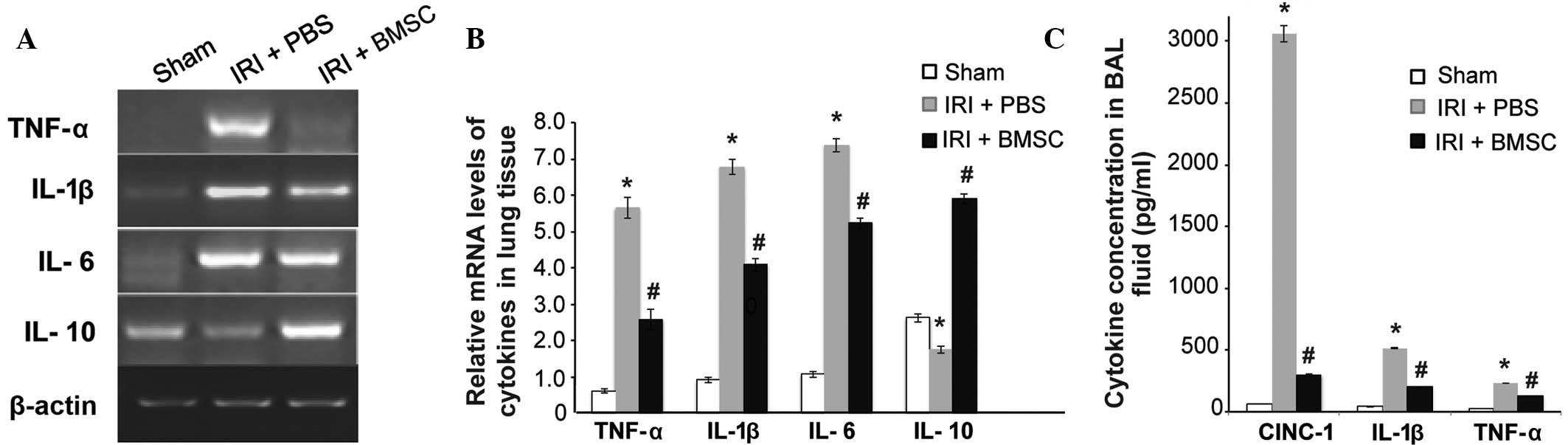 | Figure 6.BMSC infusion significantly reduced
the pro-inflammatory cytokine levels and stimulated the
anti-inflammatory cytokine levels. (A) Image of agarose
electrophoresis of the reverse transcription-quantitative
polymerase chain reaction product. (B) Quantitative analysis of the
mRNA levels of TNF-α, IL-1β, IL-6, and IL-10 and β-actin in lung
tissues. Data are presented as the mean ± standard error (n=6). (C)
BMSC infusion significantly reduced IRI-induced secretion of
pro-inflammatory cytokines. The levels of CINC-1, IL-1β, and TNF-α
in BAL fluid were measured using ELISA. Data are presented as the
mean ± standard error (n=10). *P<0.05, vs. sham group;
#P<0.05, vs. IRI + PBS group. BMSCs, bone
marrow-derived mesenchymal stem cells; IRI, ischemia-reperfusion
injury; PBS, phosphate-buffered saline; TNF-α, tumor necrosis
factor-α, IL, interleukin; BAL, bronchoalveolar lavage; CINC-1,
cytokine-induced neutrophil chemoattractant-1. |
Discussion
In the present study, the intravenous injection of
BMSCs was found to preserve the pulmonary function and
significantly reduce IRI-induced pulmonary tissue damage in rats,
possibly by attenuating the IRI-mediated pulmonary inflammation. To
the best of our knowledge, the present study is the first to show
that BMSC infusion markedly stimulates the expression of
anti-inflammatory cytokine IL-10 in the lung tissue of rats with
pulmonary IRI. The beneficial effects of MSC transplantation have
been observed in animal models of IRI in the heart, brain, kidney,
liver and intestine (8–13). The application of MSC cell therapy
has also been investigated in animal models of pulmonary IRI. Chen
et al (14) found that
ischemic postconditioning treatment may improve the survival rate
of MSC engraftment and subsequently enhance the protective effects
of MSC engraftment on the lung in a rat model of IRI. It has also
been reported that autologous transplantation of adipose-derived
MSCs can markedly alleviate IRI in a rat model by suppressing
oxidative stress and inflammatory reactions (15). The present findings are consistent
with the results of the aforementioned studies.
The precise molecular mechanism underlying the
protective effects of MSC transplantation against pulmonary IRI
remains unclear; however, the immunomodulatory properties of MSCs
have been suggested to contribute to these protective effects. The
current study demonstrated that BMSC infusion markedly increased
the expression of the anti-inflammatory cytokine IL-10 and
simultaneously reduced the IRI-mediated upregulation of the
pro-inflammatory cytokines TNF-α, IL-1β and IL-6. In addition, the
IRI-induced release of the pro-inflammatory cytokines CINC-1, TNF-α
and IL-1β was significantly reduced by BMSC infusion. The essential
role of IL-10 in mediating the beneficial effects of MSC
transplantation has been previously demonstrated. For instance,
Németh et al (16) found that
BMSCs, which can be activated by TNF-α, may reprogram macrophage or
monocytes to increase IL-10 production in the septic lung in a
mouse model of sepsis, leading to the reduction of mortality and
improvement of organ function. Furthermore, it was observed that
the beneficial effects of BMSCs may be inhibited by macrophage
depletion or pretreatment with functional blocking antibodies for
IL-10 or IL-10 receptor (16),
indicating the key role of IL-10 in mediating the beneficial
effects of MSC transplantation.
IL-10 may mediate the beneficial effects of BMSC
infusion in rats with pulmonary IRI by inhibiting the function of
neutrophils. Yang et al (2)
and Sharma et al (3) found
that the accumulation of CD4+ T lymphocytes and
neutrophils during reperfusion contributes to pulmonary IRI.
Neutrophils are considered to play a critical role in the
development of pulmonary microvascular leakage during pulmonary IRI
(21). Ajuebor et al
(22) reported that IL-10 can block
transepithelial migration of neutrophils. In addition, Mei et
al (23) demonstrated that
decreased levels of TNF-α and elevated levels of IL-10 in the BAL
fluid and plasma are associated with the MSCs-mediated improvement
of survival and attenuation of pulmonary injury in a mouse model of
intrabronchial E. coli endotoxin-induced acute pulmonary
injury. Similar to the results of the aforementioned studies, the
present results further support the role of IL-10 in mediating the
protective effects of BMSCs.
In the present study, BMSC infusion initiated at the
onset of reperfusion and had the same duration as reperfusion;
therefore, BMSCs were administered during the course of pulmonary
injury development, indicating that this administrating route may
be therapeutic. However, the long-term effects of BMSC infusion on
pulmonary IRI require further investigation.
In conclusion, the present study demonstrated that
the intravenous infusion of BMSCs significantly preserved the
pulmonary function in rats with pulmonary IRI, as well as
substantially reduced IRI-induced pulmonary tissue damage. The
mechanism underlying the beneficial effects of BMSC infusion may be
associated with a reduction in pro-inflammatory cytokines and a
stimulation of anti-inflammatory cytokines. The present results
indicate that BMSC transplantation may be a promising cell therapy
for patients with pulmonary IRI.
Acknowledgements
This study was supported by grants from the National
Natural Science Fund of China (no. 81100225) and the Science and
Technology Project of Xiamen (no. 3502Z20134013).
References
|
1
|
Trulock EP, Edwards LB, Taylor DO, Boucek
MM, Keck BM and Hertz MI: International Society for Heart and Lung
Transplantation: Registry of the international society for heart
and lung transplantation: Twenty-third official adult lung and
heart-lung transplantation report-2006. J Heart Lung Transplant.
25:880–892. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Yang Z, Sharma AK, Linden J, Kron IL and
Laubach VE: CD4+ T lymphocytes mediate acute pulmonary
ischemia-reperfusion injury. J Thorac Cardiovasc Surg. 137:695–702.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Sharma AK, Laubach VE, Ramos SI, Zhao Y,
Stukenborg G, Linden J, Kron IL and Yang Z: Adenosine A2A receptor
activation on CD4+ T lymphocytes and neutrophils attenuates lung
ischemia-reperfusion injury. J Thorac Cardiovasc Surg. 139:474–482.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Anvari F, Sharma AK, Fernandez LG, Hranjec
T, Ravid K, Kron IL and Laubach VE: Tissue-derived proinflammatory
effect of adenosine A2B receptor in lung ischemia-reperfusion
injury. J Thorac Cardiovasc Surg. 140:871–877. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Naidu BV, Woolley SM, Farivar AS, Thomas
R, Fraga CH, Goss CH and Mulligan MS: Early tumor necrosis
factor-alpha release from the pulmonary macrophage in lung ischemia
reperfusion injury. J Thorac Cardiovasc Surg. 127:1502–1508. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Maxey TS, Enelow RI, Gaston B, Kron IL,
Laubach VE and Doctor A: Tumor necrosis factor-alpha from resident
lung cells is a key initiating factor in pulmonary
ischemia-reperfusion injury. J Thorac Cardiovasc Surg. 127:541–547.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ding JY, Tang L, Xu ST and Wang Q:
Influence of pyrrolidine dithiocarbamate pretreatment on function
of the transplanted rat lung. Zhong Guo Lin Chuang Yi Xue.
17:795–798. 2010.(In Chinese).
|
|
8
|
Kanazawa H, Fujimoto Y, Teratani T,
Iwasaki J, Kasahara N, Negishi K, Tsuruyama T, Uemoto S and
Kobayashi E: Bone marrow-derived mesenchymal stem cells ameliorate
hepatic ischemia reperfusion injury in a rat model. PLoS One.
6:e191952011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Liu H, Liu S, Li Y, Wang X, Xue W, Ge G
and Luo X: The Role of SDF-1-CXCR4/CXCR7 Axis in the therapeutic
effects of hypoxia-preconditioned mesenchymal stem cells for renal
ischemia/reperfusion injury. PLoS ONE. 7:e346082012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Jiang H, Qu L, Li Y, Gu L, Shi Y, Zhang J,
Zhu W and Li J: Bone marrow mesenchymal stem cells reduce
intestinal ischemia/reperfusion injuries in rats. J Surg Res.
168:127–134. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Wang M, Tsai BM, Crisostomo PR and Meldrum
DR: Pretreatment with adult progenitor cells improves recovery and
decreases native myocardial proinflammatory signaling after
ischemia. Shock. 25:454–459. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Dharmasaroja P: Bone marrow-derived
mesenchymal stem cells for the treatment of ischemic stroke. J Clin
Neurosci. 16:12–20. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Tögel F, Hu Z, Weiss K, Isaac J, Lange C
and Westenfelder C: Administered mesenchymal stem cells protect
against ischemic acute renal failure through
differentiation-independent mechanisms. Am J Physiol Renal Physiol.
289:F31–F42. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Chen S, Chen L, Wu X, Lin J, Fang J, Chen
X, Wei S, Xu J, Gao Q and Kang M: Ischemia postconditioning and
mesenchymal stem cells engraftment synergistically attenuate
ischemia reperfusion-induced lung injury in rats. J Surg Res.
178:81–91. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Sun CK, Yen CH, Lin YC, Tsai TH, Chang LT,
Kao YH, Chua S, Fu M, Ko SF, Leu S and Yip HK: Autologous
transplantation of adipose-derived mesenchymal stem cells markedly
reduced acute ischemia-reperfusion lung injury in a rodent model. J
Transl Med. 9:1182011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Németh K, Leelahavanichkul A, Yuen PS,
Mayer B, Parmelee A, Doi K, Robey PG, Leelahavanichkul K, Koller
BH, Brown JM, et al: Bone marrow stromal cells attenuate sepsis via
prostaglandin E(2)-dependent reprogramming of host macrophages to
increase their interleukin-10 production. Nat Med. 15:42–49. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Nauta AJ and Fibbe WE: Immunomodulatory
properties of mesenchymal stromal cells. Blood. 110:3499–3506.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Rasmusson I: Immune modulation by
mesenchymal stem cells. Exp Cell Res. 312:2169–2179. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Ishikane S, Ohnishi S, Yamahara K, Sada M,
Harada K, Mishima K, Iwasaki K, Fujiwara M, Kitamura S, Nagaya N
and Ikeda T: Allogeneic injection of fetal membrane-derived
mesenchymal stem cells induces therapeutic angiogenesis in a rat
model of hind limb ischemia. Stem Cells. 26:2625–2633. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Dominici M, Le Blanc K, Mueller I,
Slaper-Cortenbach I, Marini F, Krause D, Deans R, Keating A,
Prockop DJ and Horwitz E: Minimal criteria for defining multipotent
mesenchymal stromal cells. The international society for cellular
therapy position statement. Cytotherapy. 8:315–317. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Kabay B, Aytekin FO, Aydin C, Ozer A,
Kabay N, Tekin K, Sungurtekin U, Erdem E and Ozden A:
Interleukin-10 gene therapy attenuates pulmonary tissue injury
caused by mesenteric ischemia-reperfusion in a mouse model. Tohoku
J Exp Med. 207:133–142. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ajuebor MN, Das AM, Virág L, Flower RJ,
Szabó C and Perretti M: Role of resident peritoneal macrophages and
mast cells in chemokine production and neutrophil migration in
acute inflammation: Evidence for an inhibitory loop involving
endogenous IL-10. J Immunol. 162:1685–1691. 1999.PubMed/NCBI
|
|
23
|
Mei SH, Haitsma JJ, Dos Santos CC, Deng Y,
Lai PF, Slutsky AS, Liles WC and Stewart DJ: Mesenchymal stem cells
reduce inflammation while enhancing bacterial clearance and
improving survival in sepsis. Am J Respir Crit Care Med.
182:1047–1057. 2010. View Article : Google Scholar : PubMed/NCBI
|