Introduction
Coronary artery bypass graft (CABG) surgery is a
procedure that can improve the supply of blood to the myocardium,
and is conducted in order to relieve angina and decrease the risk
of mortality from coronary artery disease (1,2). The
most commonly used conduits in CABG surgery are the saphenous vein
(SV), internal thoracic artery (ITA) and radial artery (RA)
(3). The choice and quality of the
conduits used for revascularization have a major role in the
success of CABG, with the long-term patency of these conduits being
particularly important. The SV was the first used conduit in CABG
surgery, and remains the most common, because of its relatively
large diameter and technical ease of use. However, the ITA is
currently the first choice of bypass conduits due to its excellent
results, with a patency rate of 90% at 10 years after CABG. The RA
is often considered as the second graft of choice after the ITA,
having a high patency rates close to 90% up to 10 years after CABG
(4).
The CABG technique consists in taking arteries or
veins from elsewhere in the patient's body and grafting them in
order to bypass atherosclerotic narrowings (5). Usually a patient might receive between
two and five bypass grafts, including arteries such as the ITA and
RA, and veins, such as the SV (6,7). The
lack of a convenient method to objectively assess pre-operatively
the intimal quality may lead to early graft failures (8,9).
The aim of the present morphological and
morphometric study was to conduct an analysis of grafts from the
ITA, RA and SV, prior to their use in aortocoronary bypass surgery,
in order to identify pre-operative histological changes and to draw
conclusions concerning the viability of the grafts. Another aim was
the assessment of clinical and laboratory risk factors (10) considered to be significant predictors
of lesion severity in intimal hyperplasia, atherosclerosis and
other pathologies treated by CABGs.
Materials and methods
Patient enrolment
A total of 26 patients who were undergoing surgical
coronary revascularization at the ‘Prof. Dr. George I.M. Georgescu’
Institute of Cardiovascular Diseases (Iasi, Romania) were enrolled
in the present study between January 2013 and December 2013. Their
ages ranged from 42–78 years (mean age, 60 years). The patients
comprised 20 men (76.92%) and 6 women (23.08%). Ethical approval
for the experiments conducted in the present study was obtained
from the Institutional Board of ‘Prof. Dr. George I.M. Georgescu’
Institute of Cardiovascular Diseases. Written informed consent was
obtained from all patients.
Morphological and morphometric
analysis of the grafts
A total of 54 distal segments of the ITA, RA and SV
were evaluated. For histological examination, all sections were
stained with hematoxylin and eosin (H&E), as well as with
elastic Van Gieson (EVG) and Sirius red (SR) stains. Histological
assessment was made with an optical microscope (Olympus CX41;
Olympus Corporation, Tokyo, Japan). The measurements were conducted
using a color image analysis system (QuickPHOTO MICRO 3.0;
Promicra, Prague, Czech Republic). Intima and media thickness and
surface area were measured, in order to assess the intimal
thickness index (ITI) and luminal narrowing.
Evaluation of the ITI and intimal
narrowing
The degree of intimal thickening (by intimal
hyperplasia and atherosclerosis) and luminal narrowing of the
vascular conduits was evaluated by the determination of the ITI,
which was calculated from the ratio of intimal and medial areas.
The intima was defined as the distance from the lumen to the
internal elastic lamella (IEL), in the area with the greatest
intimal thickness. The media was considered as the distance from
the internal elastic lamella to the adventitia, at the level of the
greatest medial thickness. Two severity indices were calculated
from the most severely diseased sections of the specimens using the
following formulae: i) ITI = intimal area/medial area; and ii)
luminal narrowing (%) = intimal area/IEL area × 100. The ratio of
the thickness of the intima to that of the media (R) was used as
the index for arteriosclerosis, in accordance with the method of
Kobayashi et al (11).
Atherosclerosis was graded on the basis of R as follows: Grade I,
insignificant (R<0.1); grade II, mild (0.1≤R<1.0); grade III,
moderate (1.0≤R<3.0); and grade IV, severe (R≥3.0).
Risk factor analysis
The prevalence of potential risk factors for
atherosclerosis were assessed as follows: Age, diabetes mellitus
(DM), arterial hypertension (AHT), history of cigarette smoking,
hyperlipidemia and obesity. The associations between lesion
severity and the number of atherosclerotic risk factors were
investigated. Results are expressed as mean values or
frequencies.
Results
Patient characteristics
All analyzed patients presented signs of unstable
angina pectoris at hospital admission. Table I shows the vessels used for
myocardial revascularization according to patient gender.
 | Table I.Vascular conduits according to
gender. |
Table I.
Vascular conduits according to
gender.
| Gender | ITA | RA | SV | Total |
|---|
| Male | 20 | 10 | 18 | 48 |
| Female | 4 | 2 | 0 | 6 |
| Total | 24 | 12 | 18 | 54 |
Morphological analysis
The results of the histological investigation
(Table II) indicated that
morphological changes were present with high incidence in the walls
of the fresh ‘normal’ vessels (ITAs, RAs and SVs) prior to their
use as aortocoronary conduits. The identification of the presence
of preoperatory vessel lesions is very important in the viability
assessment of the graft conduits and for long-term assessment.
According to their descending order of frequency, the graft lesions
were represented by intimal thickening or hyperplasia (20 cases),
medial fibrosis (17 cases) and fatty streaks (2 cases).
| Table II.Lesion types in the different types of
vessel conduit. |
Table II.
Lesion types in the different types of
vessel conduit.
|
|
| Lesion |
|
|---|
|
|
|
|
|
|---|
| Vessel type | Normal | Intimal
hyperplasia | Atherosclerosis | Medial fibrosis | Total |
|---|
| ITA | 7 | 10 | 2 | 5 | 24 |
| RA | 3 | 4 | 0 | 5 | 12 |
| SV | 5 | 6 | 0 | 7 | 18 |
| Total | 15 | 20 | 2 | 17 | 54 |
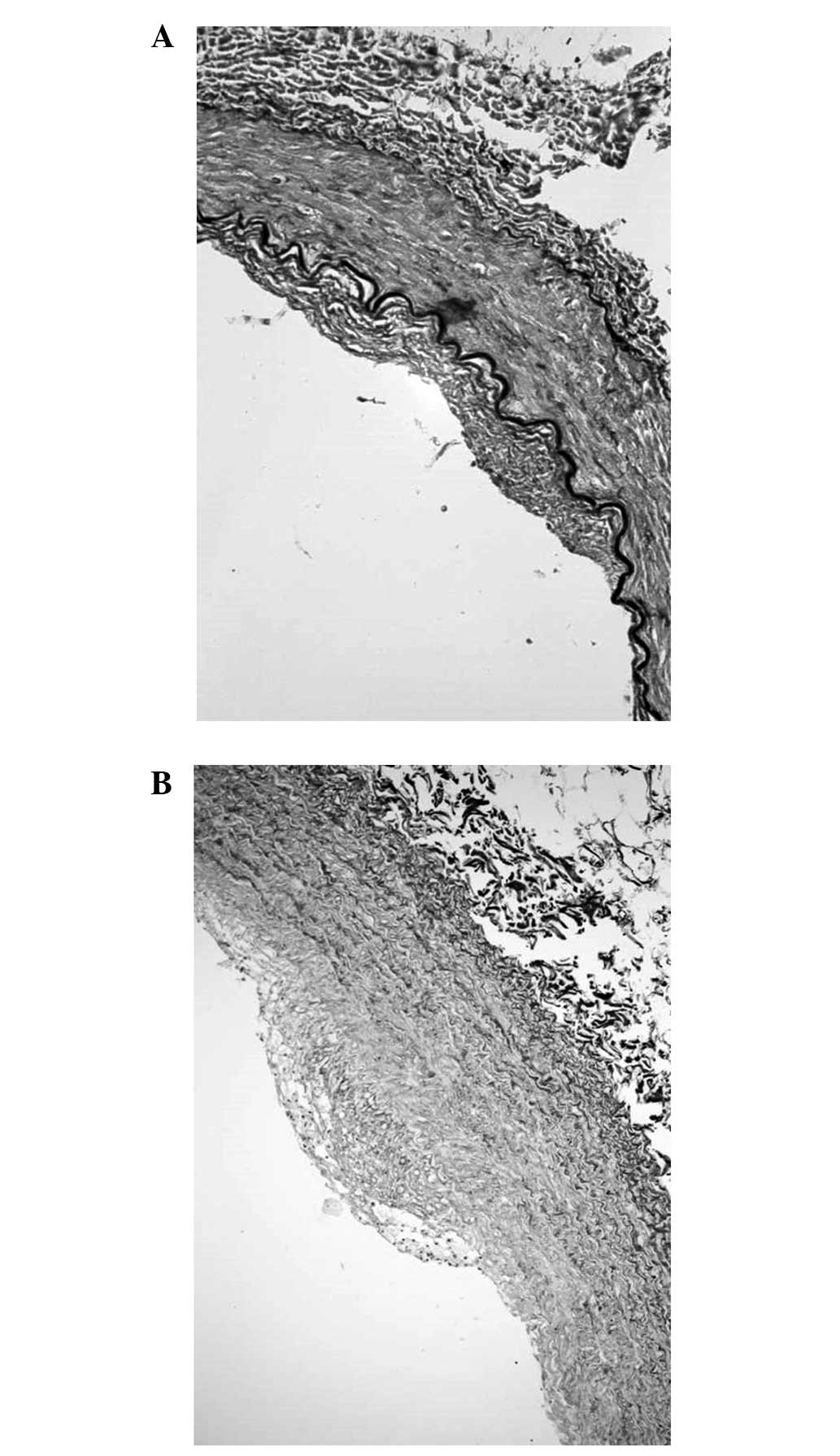
Morphological examination indicated that the ITA
lesions consisted mainly of intimal hyperplasia associated with
intimal thickening (Fig. 1A), medial
fibrosis (including 1 case with medial dissection) and fatty
streaks (Fig. 1B). The RA lesions
consisted of intimal thickening (Fig.
2A) and medial fibrosis, in equal proportions. SV lesions
consisted mainly of intimal hyperplasia, which was rarely severe
enough to narrow the lumen significantly, and medial fibrosis
(Fig. 2B).
Morphometrical analysis
In the morphometric analysis, the ITI of the vessel
conduit was calculated as a measure of the degree of preoperative
luminal narrowing dependent on intimal thickness (Table III). The mean ITI values for the
vessel conduits were 0.37 for the SVs, 0.95 for the RAs, and 1.66
for the ITAs. No patient had >50% conduit stenosis.
| Table III.ITI assessment and vessel conduit
measurements. |
Table III.
ITI assessment and vessel conduit
measurements.
|
|
|
| ITI (mean) |
|
|---|
|
|
|
|
|
|
|---|
| Atherosclerosis grade
(R) | Degree of intimal
thickening | Luminal
narrowing | RA | SV | ITA | Total cases |
|---|
| Grade 0 | Normal | | 0.00 | 0.00 | 0.00 | 0.00 |
| Grade I
(<0.1) | Insignificant | Minimal | 0.00 | 0.00 | 0.00 | 0.00 |
| Grade II
(0.1–1.0) | Mild | <25% | 0.95 | 0.37 | 0.00 | 16.00 |
| Grade III
(1.0–3.0) | Moderate | 25–50% | 0.00 | 0.00 | 1.66 | 10.00 |
| Grade IV
(>3.0) | Severe | >50% | 0.00 | 0.00 | 0.00 | 0.00 |
Risk factor analysis
Table IV shows the
incidence rates of selected cardiovascular risk factors associated
with vessel conduits. All patients showed risk factors for
atherosclerosis, such as age >60 years, arterial hypertension,
smoking, DM, obesity and hyperlipidemia. Arterial hypertension was
found in 65.38% of all cases, having an impact on the development
of atherosclerotic plaques and fibrointimal hyperplasia.
Hyperlipidemia was also present in 65.38% of all cases. DM was
present in 38.46% of cases; DM is associated with the progression
of atherosclerosis in the native vessels and the functional
impairment of veins where the level of prostacyclin production is
reduced (12). Smoking was a factor
present in 34.62% of all cases; it is an important risk factor for
the early and late thrombosis of venous grafts (13). Obesity was less frequently involved,
and was present in only 15.38% of all cases in the study group.
| Table IV.Incidence rates of selected risk
factors associated with vessel conduits. |
Table IV.
Incidence rates of selected risk
factors associated with vessel conduits.
| Risk factor | Patients, n (%) |
|---|
| Age >60 years | 16 (61.54) |
| Smoking | 9
(34.62) |
| Arterial
hypertension | 17 (65.38) |
| Hyperlipidemia | 17 (65.38) |
| Diabetes
mellitus | 10 (38.46) |
| Obesity | 4
(15.38) |
The association between the cumulative number of
risk factors and degree of conduit stenosis is shown in Table V. Vascular conduit stenosis of
<25% (ITI range, 0.18–0.95) was found in 16 patients and 88% of
them (14/16) had three or fewer cumulative risk factors. The degree
of narrowing was 25–50% of the vascular conduit (ITI range,
1.02–1.67) in 10 patients and 70% of them (7/10) had more than
three cumulative risk factors.
| Table V.Association of the degree of conduct
stenosis with the number of cardiovascular risk factors. |
Table V.
Association of the degree of conduct
stenosis with the number of cardiovascular risk factors.
|
|
| Number of risk
factors |
|
|---|
|
|
|
|
|
|---|
| ITI | Degree of
narrowing | 7 | 6 | 5 | 4 | 3 | 2 | 1 | Total |
|---|
| Grade IV | >50% | – | – | – | – | – | – | – | – |
| Grade III | 25–50% | 1 | 2 | 2 | 2 | 2 | 1 | – | 10 |
| Grade II | <25% | – | – | 1 | 1 | 6 | 5 | 3 | 16 |
| Grade I | Insignificant | – | – | – | – | – | – | – | – |
| Total |
| 1 | 2 | 3 | 3 | 8 | 6 | 3 | 26 |
Discussion
Three types of vascular lesions were identified in
the grafts, namely intimal hyperplasia, atherosclerosis and medial
fibrosis. Mild intimal hyperplasia was observed in the majority of
the graft segments taken from the patients undergoing CABG. Intimal
hyperplasia occurred more frequently in ITA grafts (10/24 cases,
41.67%) than in SV grafts (6/18 cases, 33.33%) and RA grafts (4/12
cases, 33.33%). Intimal hyperplasia, which was identified in 37.04%
of all vessels, was observed in the majority of the graft samples
removed from diabetic patients, who comprised 38.46% of the study
population undergoing CABG. Intimal hyperplasia occurs as a
response to physiological stimuli, as the tissue attempts to
maintain normal conditions of flow and/or wall tension (14).
Excessive lipoprotein in the plasma may cause
atherosclerosis, due to its tendency to accumulate in the
hyperplastic intima (15). In the
present study, the incidence of hyperlipidemia was 65.38% (17
cases), and the incidence of atherosclerosis in the ITA was 8.33%
(2/24 cases), whereas no atherosclerosis was identified in the RAs.
The prevalence of atherosclerosis in the two arteries may have been
underestimated in this study because only the distal ends of
arteries were examined, and atherosclerosis is a segmental
disease.
When investigated using microscopy, 27.78% of the
specimens were found to be normal, and 31.48% were mildly to
moderately fibrotic. On histopathological evaluation, vascular
medial fibrosis of the tunica media was found to be present in all
types of vessel grafts, suggesting that fibrosis is a global
process that occurs regardless of the involved vessel. Among all
cases of medial fibrosis, the SVs accounted for 41.17% (7 cases),
compared with 29.41% (5 cases each) by the RA and ITA,
respectively.
Medial vascular fibrosis increases the risk of
cardiovascular events by contributing to the stiffening of vessels
and reduced vascular compliance (16). In the patients of the present study,
the known cardiovascular risk factors hypertension (65.38%), DM
(38.46%) and age (61.54%) were present, which may be associated
with increased vascular fibrosis. Selvin et al (17) reported that vascular fibrosis is a
global process associated with diseases of elevated pulse pressure
and aging.
Two indices, ITI and percentage of luminal
narrowing, were used for morphometric analysis in the present
study. ITI analyses showed that the ITAs had thicker intima than
the RAs and SVs. The severity indices reflect the degree of luminal
narrowing, and the ITI was significantly greater in the ITAs (1.66)
than in the RAs (0.95) and SVs (0.37). These measurements
correspond to different degrees of luminal narrowing in the conduit
vessels that were used, which were grade III in the ITAs and grade
II in the RA and VSs. These results indicate that SVs have the
least severe pre-existing lesions prior to CABG surgery.
The percentage of luminal narrowing indicates the
degree of intimal thickening, including atherosclerosis. The area
of the intima, rather than the thickness, was measured to allow
eccentric or irregular lesions to be evaluated more accurately. The
percentage of luminal narrowing is considered to be the parameter
most useful for comparing intimal thickening in vascular beds of
different types (18).
The authors of the present study hypothesized that
ITI and IMR may be used to compare the intimal layer thickness in
various vascular diseases, which is consistent with a previous
study (19). In our previous study
we demonstrated that the ITI method was more accurate, since it
uses areas, rather than dimensions such as width (20).
There were several limitations to the present study.
First, only the changes of ITA, RA and SV histology immediately
prior to CABG were evaluated, and secondly, the patients were not
clinically followed up, and so it was not possible to correlate
CABG outcome with the histopathological findings.
In conclusion, the present study revealed the
presence of preoperative vascular lesions, such as intimal
hyperplasia and medial fibrosis, in many of the vessels, which is
significant since preoperative lesions are likely to have an effect
on the long-term viability of the conduit. Calculation of the ITI
provided an indication of the degree of lumen narrowing in the
preoperative vascular conduits. The ITI and measurements of intimal
and medial areas may serve as reference points in the follow-up
assessment of arterial and venous conduit patency. Factors
identified in the patients that are likely to be significant
predictors of lesion severity (associated with, for example intimal
hyperplasia and atherosclerosis) in the CABGs were hyperlipidemia,
arterial hypertension, smoking, age and DM.
References
|
1
|
Velazquez EJ, Lee KL, Deja MA, Jain A,
Sopko G, Marchenko A, Ali IS, Pohost G, Gradinac S, Abraham WT, et
al: Coronary-artery bypass surgery in patients with left
ventricular dysfunction. N Engl J Med. 364:1607–1616. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Vassiliades T Jr: Enabling technology for
minimally invasive coronary artery bypass grafting. Semin Thorac
Cardiovasc Surg. 21:237–244. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Sabik JF III, Lytle BW, Blackstone EH,
Houghtaling PL and Cosgrove DM: Comparison of saphenous vein and
internal thoracic artery graft patency by coronary system. Ann
Thorac Surg. 79:544–551. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Tatoulis J, Buxton BF, Fuller JA, Meswani
M, Theodore S, Powar N and Wynne R: Long-term patency of 1108
radial arterial-coronary angiograms over 10 years. Ann Thorac Surg.
88:23–30. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Wijns W, Kolh P, Danchin N, Di Mario C,
Falk V, Folliguet T, Garg S, Huber K, James S, Knuuti J, et al: The
Task Force on Myocardial Revascularization of the European Society
of Cardiology (ESC) and the European Association for
Cardio-Thoracic Surgery (EACTS); European Association for
Percutaneous Cardiovascular Interventions (EAPCI): Guidelines on
myocardial revascularization. Eur Heart J. 31:2501–2555.
2010.PubMed/NCBI
|
|
6
|
Fattouch K, Sampognaro R, Speziale G,
Salardino M, Novo G, Caruso M, Novo S and Ruvolo G: Impact of
moderate ischemic mitral regurgitation after isolated coronary
artery bypass grafting. Ann Thorac Surg. 90:1187–1194. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Beller GA and Ragosta M: Decision making
in multivessel coronary disease: The need for physiological lesion
assessment. JACC Cardiovasc Interv. 3:315–317. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Leacche M, Balaguer JM and Byrne JG:
Intraoperative grafts assessment. Semin Thorac Cardiovasc Surg.
21:207–212. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Turer AT and Hill JA: Pathogenesis of
myocardial ischemia-reperfusion injury and rationale for therapy.
Am J Cardiol. 106:360–368. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Tarakji KG, Sabik JF III, Bhudia SK,
Batizy LH and Blackstone EH: Temporal onset, risk factors and
outcomes associated with stroke after coronary artery bypass
grafting. JAMA. 305:381–390. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kobayashi H, Kitamura S, Kawachi K, Morita
R, Konishi Y and Tsutsumi M: A pathohistological and biochemical
study of arteriosclerosis in the internal thoracic artery, a vessel
commonly used as a graft in coronary artery bypass surgery. Surg
Today. 23:697–703. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Otsuka F, Yahagi K, Sakakura K and Virmani
R: Why is the mammary artery so special and what protects it from
atherosclerosis? Ann Cardiothorac Surg. 2:519–526. 2013.PubMed/NCBI
|
|
13
|
Domanski MJ, Borkowf CB, Campeau L,
Knatterud GL, White C, Hoogwerf B, Rosenberg Y and Geller NL:
Prognostic factors for atherosclerosis progression in saphenous
vein grafts: The postcoronary artery bypass graft (Post-CABG)
trial. Post-CABG Trial Investigators. J Am Coll Cardiol.
36:1877–1883. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Jones WB, Riley CP, Reeves TJ and
Sheffield LT: Natural history of coronary artery disease. Bull N Y
Acad Med. 48:1109–1125. 1972.PubMed/NCBI
|
|
15
|
Allon M, Litovsky S, Young CJ, Deierhoi
MH, Goodman J, Hanaway M, Lockhart ME and Robbin ML: Correlation of
pre-existing vascular pathology with arteriovenous graft outcomes
in hemodialysis patients. Am J Kidney Dis. 62:1122–1129. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Sulikowski T, Tejchman K, Ziętek Z,
Urasińska E, Domański L, Sieńko J, Romanowski M, Safranow K,
Zukowski M, Ciechanowicz A, et al: Histopathologic evaluation of
pretransplantation biopsy as a factor influencing graft function
after kidney transplantation in 3-year observation. Transplant
Proc. 42:3375–3381. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Selvin E, Najjar SS, Cornish TC and
Halushka MK: A comprehensive histopathological evaluation of
vascular medial fibrosis: Insights into the pathophysiology of
arterial stiffening. Atherosclerosis. 208:69–74. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Thiene G, Miazzi P, Valsecchi M, Valente
M, Bortolotti U, Casarotto D and Gallucci V: Histological survey of
the saphenous vein before its use as autologous aortocoronary
bypass graft. Thorax. 35:519–522. 1980. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Ruengsakulrach P, Sinclair R, Komeda M,
Raman J, Gordon I and Buxton B: Comparative histopathology of
radial artery versus internal thoracic artery and risk factors for
development of intimal hyperplasia and atherosclerosis.
Circulation. 100(19 Suppl): II139–II144. 1999.PubMed/NCBI
|
|
20
|
Tinică G, Luca C, Dumitraş EA and Butcovan
D: Pre-operative graft assessment before their use in aortocoronary
by-pass surgery. The 10th Congress of the Romanian
Society of Cardiovascular Surgery. International Hotel. (Iasi).
172014.
|