Introduction
Since the technological development of the
laparoscope, laparoscopic common bile duct exploration (LCBDE) has
been adopted at an increasing number of hospitals, in particular
due to its advantages, including small scarring, painlessness, a
quick-recovery time, short hospital stays and few complications
(1). The primary aim of LCBDE is the
removal of incarcerated calculi from the lower part of the common
bile duct.
The present study aimed to investigate the
practicability and clinical value of applying laparotomy biliary
lithotomy forceps to the LCBDE protocol.
Patients and methods
Clinical data
Between August 2013 and December 2014, 63 patients,
including 29 males and 34 females (male: female=1:1.2), with
choledocholithiasis were admitted to the Department of
Hepatopancreatobiliary Surgery at the Affiliated Hospital of
Yanbian University (Yanji, China). The patients were aged between
31 and 87 years, with an average age of 59 years. All 63 cases had
been diagnosed with both cholecystolithiasis and
choledocholithiasis, of which 16 cases had incarcerated calculi at
the lower end of the common bile duct.
Surgical methods
General anesthesia was administered by tracheal
intubation and the patient was placed in the left lateral tilt
position with the head elevated. The pore for the laparoscope was
established within the lower side of the navel, whereas the mail
operational pore was created 2 cm below the xiphoid process and two
auxiliary operational pores were established to the right of the
midclavicular line and 2 cm below the costal margin of the anterior
axillary line on the right side. Following localization of the
common bile duct under a laparoscope, a 1–1.5 cm longitudinal
incision was made close to the upper side of the duodenum.
Subsequently, as a choledochoscope was used to confirm the size and
position of the incarcerated calculi, another incision was made on
the abdominal wall directly above the longitudinal incision of the
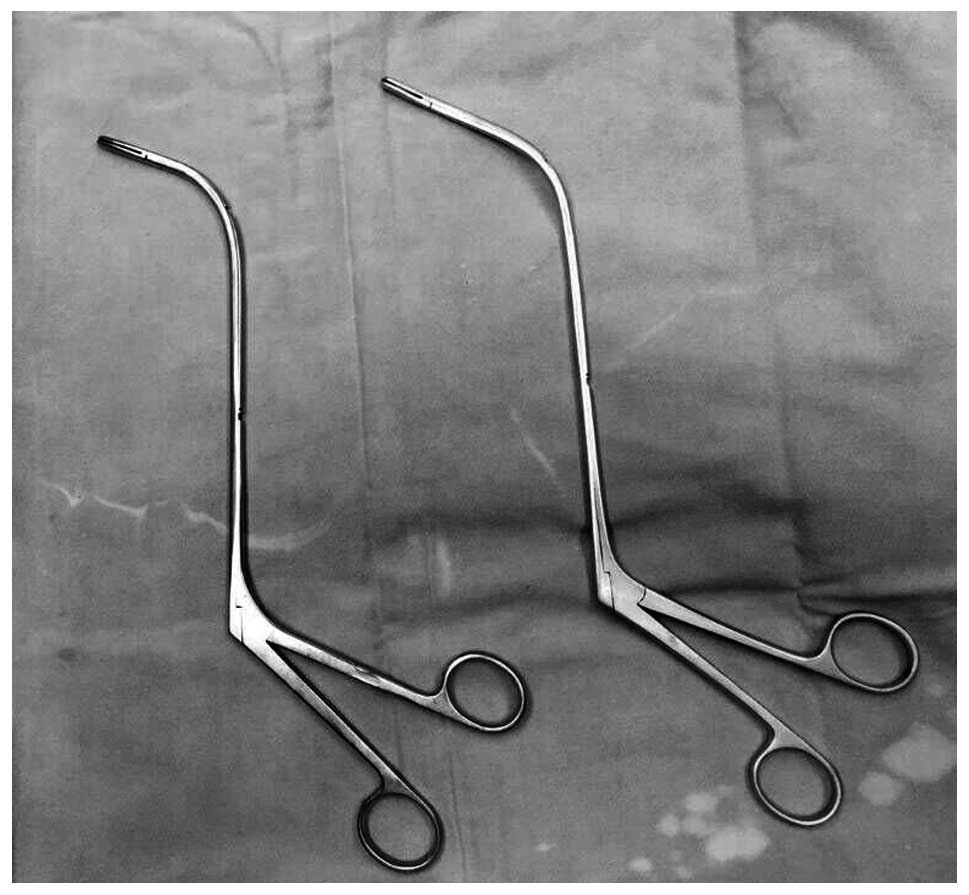
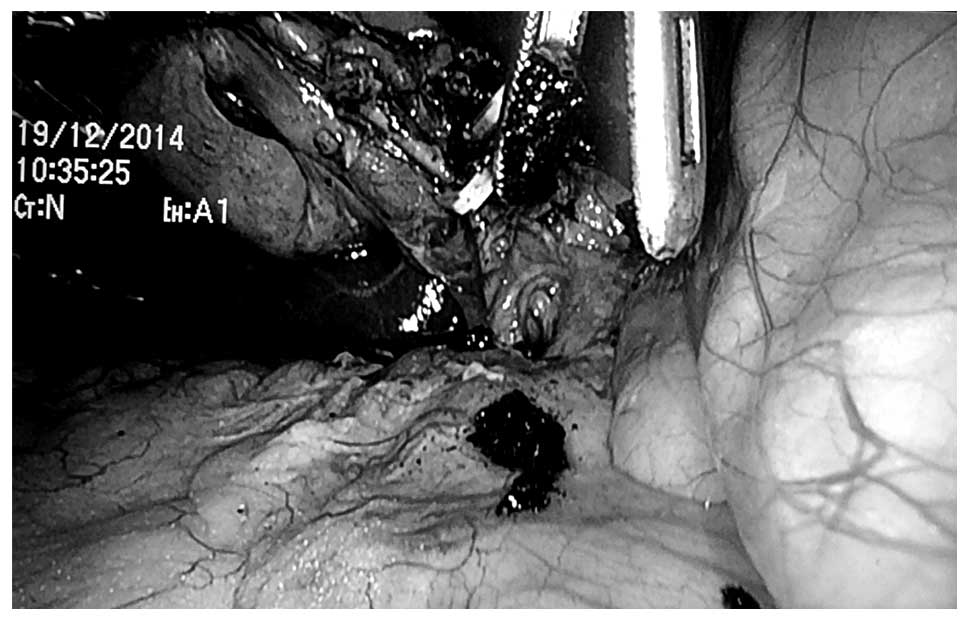
common bile duct. Through this small incision, laparotomy biliary
lithotomy forceps (Fig. 1) of the
correct size and radian were inserted (Fig. 2), during which the intra-abdominal
pressure was lowered to 9 mmHg in order to reduce the distance
between the abdominal wall and incision on the common bile duct.
According to the anatomical structure of the common bile duct, the
calculi were gently removed (Fig.
3). A choledochoscopic examination was performed to confirm
that there were no residual calculi within the common bile duct. A
lithotomy forcep was inserted into the incision on the abdominal
wall and remained in the wall until the calculi were removed to
prevent leakage. In the event of any contamination of the
facilities, the forceps were washed and then removed outside of the
abdominal cavity.
Results
Outcomes
The laparotomy biliary lithotomy forceps were used
in 16 cases, of which only one failed. During the surgery, a
T-shaped tube was inserted during the initial surgery, and after 6
weeks, the calculi were removed under a choledochoscope. The
insertion of a T-shaped tube or primary suturing of the common bile
duct was performed in the 15 successful cases, according to the
extent of dilatation of the common bile duct and the extent of
obstruction of the distal bile duct. The mean surgical duration of
the 15 cases who were treated successfully was 1.5 h, and the mean
hospitalization duration post-surgery was 6 days.
Discussion
The common bile duct is divided into four segments
from the top to the bottom, as follows: Duodenal upper segment,
duodenal posterior segment, pancreas segment and medial wall of the
duodenum. The first two segments have smooth, thin muscular walls,
a wide lumen and are easily extended. The latter two sections, in
particular the fourth segment, are surrounded by numerous organs
and contain the sphincter of the common bile duct. Their lumens are
narrow, their walls are thick and they are located in a deep and
inaccessible position for dissection, therefore they are not easily
extended. As compared with the third segment, the fourth segment
rapidly narrows and crosses the wall of the duodenum, thus forming
an obtuse angle pointing outward and down (2). This leads to the center of the lumen
becoming eccentric and a diverticulum formation in the third
section allows the calculi to become embedded. The wrong treatment
or a surgical error during the removal of a common bile duct stone
may lead to complications, including iatrogenic damage of the
choledocho-pancreatico-duodenal junction and bleeding in the
biliary tract and duodenum. The general treatment principles for
embedded common bile duct stones are as follows: To remove the
lesions, to remove all calculi, to correct the narrowness, to
maintain unobstructed drainage, to prevent relapse, to reduce
injury and complications, and to lower risks. Therefore, it is
important to select an effective method for the treatment of
patients with incarcerated calculi of the common bile duct.
It is often challenging to remove calculi from
patients due to them being embedded, hard or large. The distal part
of lithotomy forceps is L-shaped with two 2-cm flat indented forcep
bites at the terminus. The maximum open angle of the lithotomy
forceps is 70°, which permits contact with the nearest surface of
the calculi only. However, basket extraction is also challenging,
as it may be unable to pass through the lumen and subsequently
unfold insufficiently to cover the calculi or it may be unable to
remove a large or embedded calculi. Furthermore, the force applied
during basket extraction may lead to bleeding, and basket
extraction is also time-consuming. If the calculi have been
incarcerated for a long time, thus becoming hard and completely
obstructive, mucosal tissue on the bile duct wall may undergo
hyperplasia and thickening, and this cannot be removed by lithotomy
forceps. In this case, laser or machinery methods could be adopted
to shatter the stone, after which the pieces may be removed
(3). Basket impaction or rupture of
the basket traction wire are complications unique to mechanical
lithotripsy (4,5), some patients cannot tolerate the
prolonged lithotripsy operating time, thus, the procedure has to be
conducted in several sessions (6,7).
Endoscopic electrohydraulic lithotripsy requires costly and fragile
endoscopes (8) as well as the
excellent coordination of two very experienced endoscopists.
Endoscopic laser lithotripsy is the most recent method, but its use
is still limited, also owing to the need for costly equipment
(9). Recent laser lithotriptors
combine the advantages of dye and solid-state lasers at a
reasonably low price (10), thus
potentially allowing for a future progressive diffusion of laser
lithotripsy worldwide (10,11). The critical determining factors for
the success of extracorporeal shock-wave lithotripsy (ESWL) are
stone size/structure (12) and CBD
diameter (13). ESWL is at present
not considered as being the first line treatment for difficult bile
duct stones (9).
The length and radian of the laparotomy biliary
lithotomy forceps are more suitable for the structure of the common
bile duct than that of the laparoscopic biliary lithotomy forceps.
Experienced surgeons are able to perform the surgery as gently and
carefully as a general laparotomy, such that iatrogenic biliary
tract damage may be rare. The essential protocols performed during
these type of surgery are summarized, as follows: i) The incision
should be made directly above the bile duct incision on the
abdominal wall to reduce the distance to the distal part of the
biliary tract and to prevent damage to the biliary tract; ii)
pneumoperitoneum pressure should be reduced to 9 mmHg in order to
shorten the distance between the abdominal wall and bile duct
incision; and iii) lithotomy forceps should be inserted through the
incision in the abdominal wall, left in the wall after the calculi
are removed to prevent leakage and removed when the surgery is
completed. If there is contamination of the facilities, they should
be washed and then be removed outside of the abdominal cavity.
Furthermore, the process should be performed under the supervision
of a laparoscope, and lithotomy should be guided according to
pre-operative images and choledochoscope examinations performed
intraoperatively, thus ensuring that the surgical process runs
smoothly. In addition, when the incarcerated calculi are dense,
forceps should be used initially to smash the calculi, followed by
removal. The surgeons that perform the operation should be
experienced in laparotomy since they should not make contact with
any organs during the LCBDE.
In conclusion, the present study demonstrated that
laparotomy biliary lithotomy forceps may be effectively used in
LCBDE for the surgical treatment of incarcerated calculi, in
particular in basic-level hospitals. The numerous advantages of
this include surgical ease, short operation and hospitalization
time, and low costs.
References
|
1
|
Noble H, Tranter S, Chesworth T, Norton S
and Thompson M: A randomized, clinical trial to compare endoscopic
sphincterotomy and subsequent laparoscopic cholecystectomy with
primary laparoscopic bile duct exploration during cholecystectomy
in higher risk patients with choledocholithiasis. J Laparoendosc
Tech A. 19:713–720. 2009. View Article : Google Scholar
|
|
2
|
Kune GA: Surgical anatomy of common bile
duct. Arch Surg. 89:995–1004. 1964. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kuroki T, Tajima Y, Tsuneoka N, Kitasato
A, Adachi T, Kosaka T, Okamoto T, Ohno S and Kanematsu T: Placement
of a plasticbiliary biliary stent tube with primary closure of the
common bile duct after laparoscopic common bile duct exploration.
Hepatogastroenterology. 57:1034–1036. 2010.PubMed/NCBI
|
|
4
|
Lux G, Ell C, Hochberger J, Müller D and
Demling L: The first successful endoscopic retrograde laser
lithotripsy of common bile duct stones in man using a pulsed
neodymium-YAG laser. Endoscopy. 18:144–145. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Moon JH, Cha SW, Ryu CB, Kim YS, Hong SJ,
Cheon YK, Cho YD, Kim YS, Lee JS, Lee MS, et al: Endoscopic
treatment of retained bile-duct stones by using a balloon catheter
for electrohydraulic lithotripsy without cholangioscopy.
Gastrointest Endosc. 60:562–566. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Cipolletta L, Costamagna G, Bianco MA,
Rotondano G, Piscopo R, Mutignani M and Marmo R: Endoscopic
mechanical lithotripsy of difficult common bile duct stones. Br J
Surg. 84:1407–1409. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Garg PK, Tandon RK, Ahuja V, Makharia GK
and Batra Y: Predictors of unsuccessful mechanical lithotripsy and
endoscopic clearance of large bile duct stones. Gastrointest
Endosc. 59:601–605. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Chang WH, Chu CH, Wang TE, Chen MJ and Lin
CC: Outcome of simple use of mechanical lithotripsy of difficult
common bile duct stones. World J Gastroenterol. 11:593–596. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Shim CS: How Should Biliary Stones be
Managed? Gut Liver. 4:161–172. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Hochberger J, Tex S, Maiss J and Hahn EG:
Management of difficult common bile duct stones. Gastrointest
Endosc Clin N Am. 13:623–634. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Patel SN, Rosenkranz L, Hooks B, Tarnasky
PR, Raijman I, Fishman DS, Sauer BG and Kahaleh M: Holmium-yttrium
aluminum garnet laser lithotripsy in the treatment of biliary
calculi using single-operator cholangioscopy: A multicenter
experience (with video). Gastrointest Endosc. 79:344–348. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Tandan M, Reddy DN, Santosh D, Reddy V,
Koppuju V, Lakhtakia S, Gupta R, Ramchandani M and Rao GV:
Extracorporeal shock wave lithotripsy of large difficult common
bile duct stones: Efficacy and analysis of factors that favor stone
fragmentation. J Gastroenterol Hepatol. 24:1370–1374. 2014.
View Article : Google Scholar
|
|
13
|
Amplatz S, Piazzi L, Felder M, Comberlato
M, Benvenuti S, Zancanella L, Di Fede F, de'Guelmi A, Bertozzo A,
Farris P, et al: Extracorporeal shock wave lithotripsy for
clearance of refractory bile duct stones. Dig Liver Dis.
39:267–272. 2007. View Article : Google Scholar : PubMed/NCBI
|