Introduction
Proliferative myositis is a rare pseudosarcomatous
(mimicking sarcoma) condition. It usually occurs in adults aged
>40-years-old, and occasionally in children (1). Although proliferative myositis grows
rapidly, it is actually a benign lesion and can regress or
completely resolve spontaneously. The incidence of proliferative
myositis remains unknown, however recurrence is extremely rare
(2). Although the cause of
proliferative myositis remains unclear, a history of recent local
trauma may be a risk factor, as noted in some reports (1,3,4). Diagnosis of proliferative myositis is
largely dependent on the patient's age, history of recent trauma,
and a rapidly growing, painful solitary soft-tissue mass located in
the muscle, together with radiological evidence, such as magnetic
resonance imaging (MRI). Pathological examination of a biopsy is
the final and most accurate method for the diagnosis of
proliferative myositis. There is no specific treatment recommended
following establishment of a diagnosis of proliferative myositis,
since of proliferative myositis may disappear spontaneously
(2,5). Excision may be preferred for the
confirmation of a diagnosis and for cosmetic reasons (2). The most commonly involved sites are the
head, neck, and extremities. Herein, we report a case of
proliferative myositis in the right brachioradialis. To the best of
our knowledge, this is the first case reported at this site and
will further improve our understanding of the sites affected by
this disease.
Case report
A 64-year-old man was admitted to The First Hospital
of Jilin University (Changchun, China) in September 2014 after
presenting with a mass in his right forearm. The mass was
incidentally found by the patient 2 weeks previously, and upon
hospitalization had grown larger. On examination, a mass 3.0×2.5 cm
was palpated in the right brachioradialis, on the lateral side of
the proximal end of the right forearm. During movement and rest of
his right arm, the patient experienced no discomfort. The skin
surface above the mass was elevated, and exhibited normal
pigmentation and temperature. The mass was mildly tender with a
hard texture and smooth surface, although the border with the
surrounding tissue was not pronounced.
Neurological examination of the right arm was
unremarkable. MRI showed a hyperintense lesion in T1- and
T2-weighted images (Fig. 1).
Fine-needle biopsy of the lesion revealed spindle cells and
ganglion cells, suggesting proliferative myositis. Pathological
examination was subsequently performed. The specimen was fixed in
10% formalin-saline solution, followed by embedding in paraffin for
24 h, sectioning at 4-µm thickness, and staining with hematoxylin
and eosin. Subsequently, the sections were examined under a light
microscope (DP20; Olympus Corp., Tokyo, Japan) at a magnification
of ×40. Since pathological examination demonstrated that the lesion
was benign and the function of the arm was not affected, a
watch-and-wait strategy was recommended. However, the patient
insisted on surgical resection of the mass.
Intraoperatively, the mass was discovered to be
incorporated with surrounding muscular tissues. Complete resection
of the mass was performed with dissection of the surrounding normal
tissues.
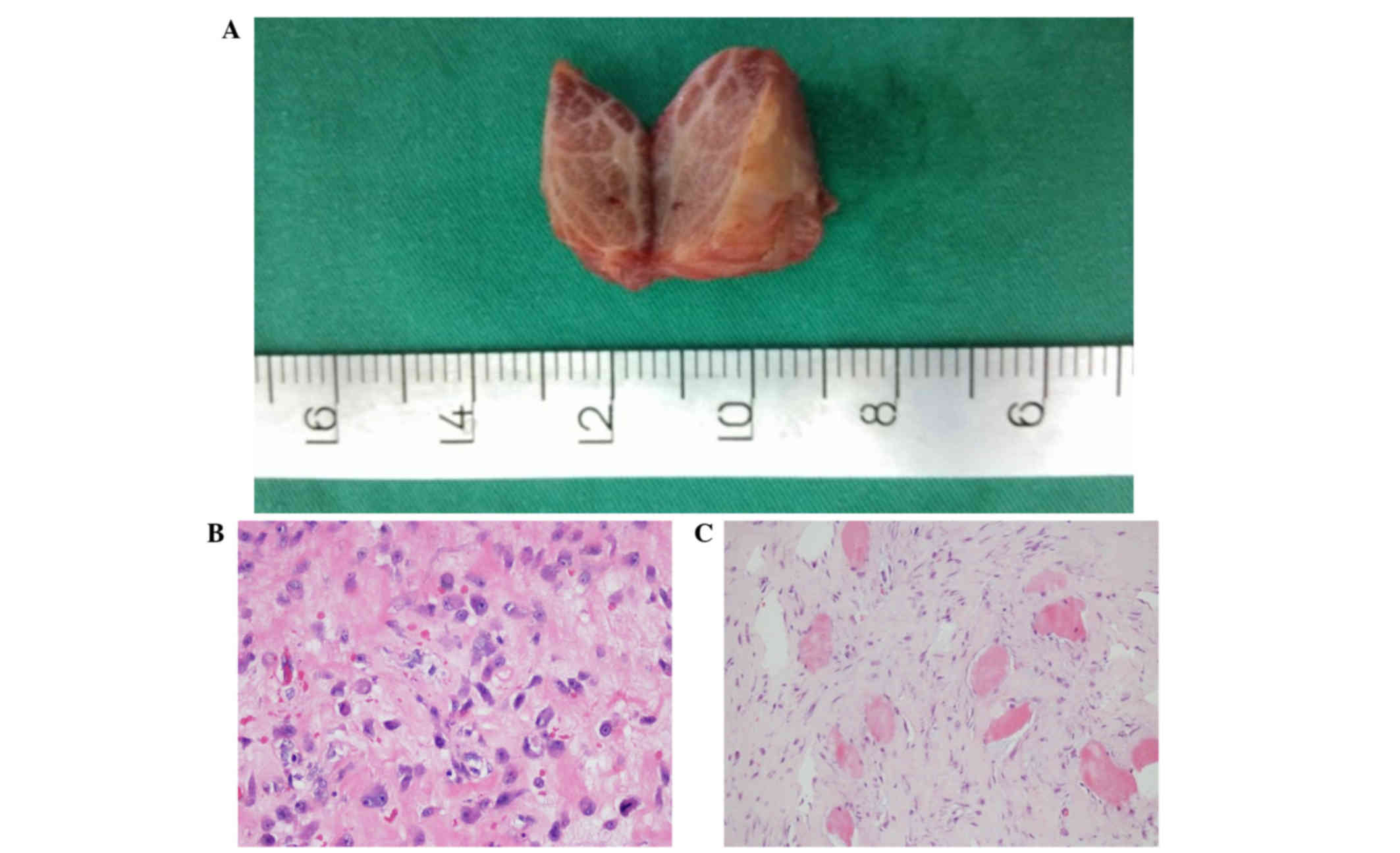
Gross pathological examination showed that the
resected mass was pink-gray on the transverse section surface
(Fig. 2A). Microscopic examination
revealed ganglion-like giant basophilic cells and spindle cells
(Fig. 2B and C). A diagnosis of
proliferative myositis was confirmed pathologically. Upon follow-up
13 months after surgery, the patient exhibited a well-healed
surgical incision and good elbow joint function, without any
swelling or tenderness. No recurrence of the mass was detected. The
patient refused a follow-up MRI examination.
Ethical approval for the present study was obtained
from The First Hospital of Jilin University and written informed
consent was obtained from the patient.
Discussion
Proliferative myositis was first reported by Kern in
1960 (2). Several theories regarding
its etiology have been proposed, such as mechanical injury and
ischemia, which remain inconclusive (6–9). The
mass usually grows rapidly and is able to cause local compression
symptoms.
Proliferative myositis shows no specific features
upon laboratory and imaging examinations; therefore, pathological
examination is required for a definitive diagnosis. The resected
mass is lobular and infiltrative. Its section surface is gray in
color, with a solid texture. Pathologically, the proliferative mass
is characterized by a checkerboard of myofibroblasts infiltrating
muscle fibers on the transverse section, and ganglion-like cells
(10).
Proliferative myositis is distinct from
rhabdomyosarcoma, myositis ossificans, nodular fasciitis, and
proliferative fasciitis (2,11,12).
Differentiating between proliferative myositis and rhabdomyosarcoma
can be difficult. Soft tissue sarcoma is often round in shape or
nodular, lacking the normal structure of muscle fibers. In large
soft tissue sarcomas, necrosis, hemorrhage, and cysts may be found
(12). In addition, proliferative
myositis is negative for myosin staining, but positive in
rhabdomyosarcoma. Myositis ossificans exhibit characteristic
ossification in the lesion, as observed on MRI or computed
tomography (10). MR images of
proliferative myositis have been reported in several cases, with
hypo- or iso-intense T1 signals, compared with those of muscle and
homogeneous enhancement. T2-weighted MR images typically
demonstrate a hyperintense soft-tissue mass (1,2,5).
A watch-and-wait strategy is preferred for
proliferative myositis, due to its benign nature and the potential
for spontaneous resolution. Although the mass grows rapidly in its
initial phase, it typically stabilizes after a few weeks. No
malignancy or metastasis of proliferative myositis has ever been
reported (9). If the mass is causing
compression symptoms or affecting the patient's daily life,
surgical resection can be performed.
In conclusion, proliferative myositis is a rare,
self-limiting, benign disease that has not been described in the
right brachioradialis until now. Its diagnosis can be difficult
and, in many cases, diagnosis is not confirmed until after surgical
resection. Fine-needle biopsy is helpful in the diagnosis of
proliferative myositis, thus avoiding unnecessary surgical trauma
and costs.
References
|
1
|
Mulier S, Stas M, Delabie J, Lateur L,
Gysen M, Dal Cin P, Robberecht C and De Wever I: Proliferative
myositis in a child. Skeletal Radiol. 28:703–709. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Wlachovska B, Abraham B, Deux JF, Sibony
M, Marsault C and Le Breton C: Proliferative myositis in a patient
with AIDS. Skeletal Radiol. 33:237–240. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kern WH: Proliferative myositis; a
pseudosarcomatous reaction to injury: A report of seven cases. Arch
Pathol. 69:209–216. 1960.PubMed/NCBI
|
|
4
|
Enzinger FM and Dulcey F: Proliferative
myositis: Report of thirty-three cases. Cancer. 20:2213–2223. 1967.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kent MS, Flieder DB, Port JL and Altorki
NK: Proliferative myositis: a rare pseudosarcoma of the chest wall.
Ann Thorac Surg. 2002.73:1296–1298. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Wong NL: Fine needle aspiration cytology
of pseudosarcomatous reactive proliferative lesions of soft tissue.
Acta Cytol. 46:1049–1055. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Wong NL and Di F: Pseudosarcomatous
fasciitis and myositis diagnosisby fine-needle aspiration cytology.
Am J Clin Pathol. 132:857–865. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Brooks JK, Scheper MA, Kramer RE,
Papadimitriou JC, Sauk JJ and Nikitakis NG: Intraoral proliferative
myositis: Case report and literature review. Head Neck. 29:416–420.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Fauser C, Hrig J, Niedermeyer HP and
Arnold W: Proliferative myositisa rare pseudomalignant tumor of the
head and neck. Arch Otolaryngol Head Neck Surg. 134:437–440. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Klapsinou E, Despoina P and Dimitra D:
Cytologic findings and potential pitfalls in proliferative myositis
and myositis ossificans diagnosed by fine needle aspiration
cytology: Report of four cases and review of the literature. Diagn
Cytopathol. 40:239–244. 2012. View
Article : Google Scholar : PubMed/NCBI
|
|
11
|
Subramanian S and Sharma R: Can MR imaging
be used to reliably differentiate proliferative myositis from
myositis ossificans? Radiology. 246:9872008. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Demir MK, Beser M and Akinci O: Case 118:
Proliferative myositis. Radiology. 244:613–616. 2007. View Article : Google Scholar : PubMed/NCBI
|