Introduction
Acute renal injury (AKI), also known as acute renal
failure, refers to the clinical syndrome of a sudden decline in
renal function during the first 3 months of a disease course
(1). AKI can be caused by a variety
of factors, with clinical manifestations including fluid and
electrolyte balance and acid and alkaline balance disorders as well
as azotemia (2). AKI incidence in
critically ill patients is high (up to 30–50%), and AKI severity is
positively correlated with patient mortality, with AKI is one of
the leading causes of death in critically ill patients (3). AKI can increase the burden of disease
and the treatment costs of critically ill patients. At present, the
pathophysiological mechanism of AKI is not yet fully understood, so
improving treatment methods is a challenge. Therefore, AKI has
become one of the most difficult medical problems present
throughout the world (4,5). SCr is often used as a diagnostic index
for AKI, but SCr levels are affected by many factors (blood volume,
muscle mass and protein intake), leading to its uncertain
association with acute renal cell injury. As such, SCr cannot be
used to accurately and timely reflect the occurrence of AKI
(6). Early detection and timely
treatment is the key for the treatment of AKI, so the
identification of novel biomarkers of AKI for early diagnosis is
particularly important. As a member of lipocalin superfamily, NGAL
was considered to be one of the ideal and important biomarkers in
the diagnosis of AKI (7). CysC is a
member of the cysteine protease inhibitor superfamily and is
frequently used as a marker for the diagnosis of AKI. In this
study, we examined and analyzed NGAL levels in critically ill
patients after surgery. The present study provided a theoretical
basis for the early diagnosis of AKI.
Materials and methods
General information
Thirty-eight critically ill patients with acute
renal injury treated at Zhengzhou No. 7 People's Hospital between
December 2015 and November 2016 were selected to serve as AKI group
(observation group). At the same time, 38 critically ill patients
without acute renal injury were selected as the non-AKI group
(control group). Inclusion criteria were as follows: i) critically
ill patients with surgical treatment; ii) ICU stay ≥24 h; iii)
patients provided informed consent. Exclusion criteria were as
follows: i) patients had received nephrotoxic drugs within the week
prior to selection; ii) patients had received conventional dialysis
before admission; iii) patients with heart failure and malignant
tumors. There were no significant differences in general
information parameters between the two groups (P>0.05; Table I). The study was approved by the
Ethics Committee of Zhengzhou No. 7 People's Hospital.
 | Table I.General patient information. |
Table I.
General patient information.
| Items | Observation group
(n=38) | Control group
(n=38) | t/χ2 | P-value |
|---|
| Sex
(male/female) | 21/17 | 20/18 | 0.046 | 0.829 |
| Age range
(years) | 40–75 | 35–75 |
|
|
| Average age
(years) | 48.76±7.48 | 49.07±7.86 | 0.176 | 0.861 |
| MAP (mmHg) | 96.87±12.37 | 97.35±11.58 | 0.175 | 0.862 |
| WBC
(109/l) | 16.06±5.93 | 15.84±5.74 | 0.164 | 0.869 |
| Serum BUN
(mmol/n) | 29.03±5.83 | 28.14±5.35 | 0.693 | 0.490 |
| Type of damage (n,
%) |
| Acute
tubular necrosis | 15 (39.47) | 16 (42.11) | 0.047 | 0.827 |
| Acute
glomerular injury | 14 (36.84) | 15 (39.47) | 0.053 | 0.818 |
| Acute
interstitial nephritis | 9 (23.68) | 7 (18.42) | 0.076 | 0.781 |
Experimental methods
Experimental equipment and reagents
Main equipment consisted of a microplate reader
(Jiangsu Potebio Biotechnology Co., Ltd., Jiangsu, China),
automatic biochemical instrument (Precise, Beijing, China),
centrifuge (Beijing Guangan Medical Equipment Factory), pipettes
(Dragon Laboratory Instruments Ltd., Beijing, China), EP tubes and
centrifuge tubes (Haimen Innovative Experimental Equipment Factory,
Jiangsu, China). Experimental reagents consisted of NGAL ELISA kits
(R&D Systems, Inc., Minneapolis, MN, USA), CysC kits (Beijing
Strong Biotechnologies, Inc., Beijing, China) and SCr kits
(BioSino, Beijing, China).
Specimen collection
Blood samples were extracted from the radial artery
of all patients at 2, 8, 12 and 24 h post-operation. The blood
samples were centrifuged for 5 min, and the supernatant was
transferred into EP tubes and kept at −80°C for storage.
Indicator detection
NGAL and Scr levels were detected using ELISA
according to the manufacturers instructions. In brief: i) blood
stored at −80°C was thawed at room temperature (20°C); ii) samples
and standards were diluted (dilution ratio 1:5) and transferred to
the plate; iii) samples were incubated in the plate for 30 min at
37°C and then washed with phosphate-buffered saline (PBS) 5 times
for 15 sec for each time; iv) enzyme-conjugated reagent (50 µl) was
added and incubated at 37°C for 30 min, followed by four 15-sec
washes; v) color developer A and B were added and the samples were
incubated at room temperature in the dark for 15 min. The
termination solution was then added, and the OD value at 450 nm was
measured using a microplate reader within 15 min. These readings
were used to calculate NGAL and Scr levels.
CysC levels were detected using PETIA, under the
principle that serum CysC can bind to latex particles coated with
goat anti-human CysC polyclonal antibodies (dilution 1:500; cat.
no. PD-RM-0006-M0001; Biomart, Wuhan, China), resulting in
increased turbidity at 600 nm proportional to CysC levels. The main
parameters of the assay were as follows: main wavelength, 600 nm;
reaction methods, point end assay; reaction direction, positive;
temperature, 37°C. The difference in OD value of the calibration
solution (OD value at 5 min later - OD value at 1 min later) was
calculated, and an absorbance-concentration curve for the
calibration solution was established. The difference in sample OD
value was then calculated and CysC level was calculated according
to the absorbance-concentration curve.
Evaluation criteria
Serum NGAL and Scr levels were measured by ELISA at
2, 8, 12 and 24 h post-operation and serum CysC levels were
measured by PETIA at the same time-points.
Statistical analysis
Data were processed using the SPSS 19.0 (SPSS, Inc.,
Chicago, IL, USA) software. Measurement data were expressed as mean
± standard deviation (false) and comparisons between groups were
performed using the t-test. Measurement data were expressed by
ratio and comparison between the groups were performed using
χ2 test. Pearson correlation coefficient analysis was
carried out for correlation analysis. Diagnostic value was analyzed
by ROC curve. P<0.05 was considered to be statistically
significant.
Results
Serum NGAL levels
The serum NGAL level in the observation group was
significantly higher than in the control group at 2, 8, 12 and 24 h
after operation (P<0.05; Table
II).
| Table II.NGAL level comparison (ng/ml). |
Table II.
NGAL level comparison (ng/ml).
| Group | Cases | 2 h | 8 h | 12 h | 24 h |
|---|
| Observation | 38 | 81.78±3.48 | 83.93±3.23 | 85.29±3.48 | 89.29±3.48 |
| Control | 38 | 23.04±3.98 | 21.05±3.32 | 18.06±3.59 | 17.64±3.59 |
| t-value |
| 68.941 | 83.683 | 82.889 | 88.339 |
| P-value |
| <0.001 | <0.001 | <0.001 | <0.001 |
Serum SCr levels
No significant difference in SCr level was found
between observation and control groups at 2, 8, 12 and 24 h after
operation (P<0.05; Table
III).
| Table III.SCr level comparison (µmol/l). |
Table III.
SCr level comparison (µmol/l).
| Group | Cases | 2 h | 8 h | 12 h | 24 h |
|---|
| Observation | 38 | 72.18±3.54 | 70.84±3.28 | 73.87±3.25 | 78.78±3.74 |
| Control | 38 | 72.05±3.72 | 71.03±3.62 | 74.25±3.17 | 79.04±3.69 |
| t-value |
| 0.156 | 0.240 | 0.516 | 0.305 |
| P-value |
| 0.876 | 0.811 | 0.607 | 0.761 |
Serum CysC levels
The serum CysC level in the observation group was
significantly higher than in the control group at 2, 8, 12 and 24 h
after operation (P<0.05; Table
IV).
| Table IV.CysC level comparison (mg/l). |
Table IV.
CysC level comparison (mg/l).
| Group | Cases | 2 h | 8 h | 12 h | 24 h |
|---|
| Observation | 38 | 4.08±0.43 | 4.23±0.28 | 4.39±0.38 | 4.59±0.47 |
| Control | 38 | 2.83±0.78 | 2.57±0.37 | 1.73±0.49 | 1.03±0.52 |
| t-value |
| 8.651 | 22.054 | 26.444 | 31.309 |
| P-value |
| <0.001 | <0.001 | <0.001 | <0.001 |
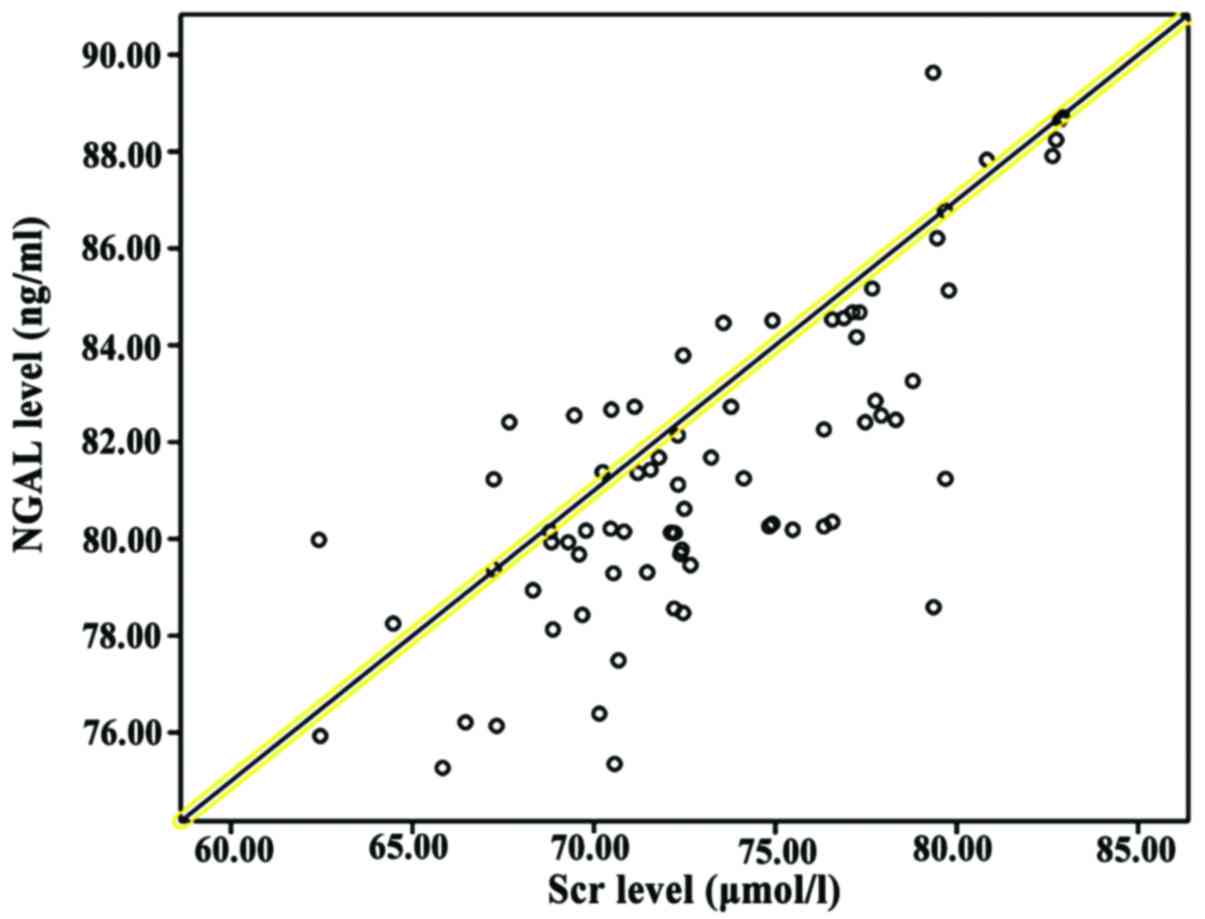
Correlation analysis between NGAL,
CysC and Scr
Pearson correlation coefficient analysis showed that
NGAL and CysC levels were positively correlated with SCr levels
(P<0.05; Table V and Figs. 1 and 2).
| Table V.Correlation between NGAL and CysC
levels and SCr level. |
Table V.
Correlation between NGAL and CysC
levels and SCr level.
| Indication | r | P-value |
|---|
| NGAL | 0.518 | 0.013 |
| CysC | 0.501 | 0.027 |
Comparison of NGAL, CysC and SCr for
the early diagnosis of AKI
The potential of NGAL, CysC and SCr for use as an
early diagnostic marker of AKI was evaluated. For NGAL, the area
under the AKI curve was 0.904, the sensitivity was 90.2% and the
specificity was 89.5%; for CysC, the area under the AKI curve was
0.806, the sensitivity was 79.2% and the specificity was 78.5%; for
Scr, the area under the AKI curve was 0.634, the sensitivity was
64.2% and the specificity was 62.5% (Fig. 3).
Discussion
AKI is a new concept proposed by the International
Renal Disease and Emergency Medicine community to replace the term
‘acute renal failure’. Infectious diseases are the main causes of
AKI, and other causes may include cardiogenic shock, hypovolemia,
septic shock and major surgery. AKI is common for critically ill
patients in the ICU. The mortality rate of AKI is high and AKI is
also an independent risk factor for death in critically ill
patients (8). The renal function of
AKI patients can be significantly reduced within a short time, and
the resultant inability to excrete metabolites reduces the
stability of the internal environment. The diagnostic criteria used
to identify AKI are: sudden changes in renal structure or function
within 48 h identified by imaging, or hematuria during routine
examination found within 3 months, with an increase in SCr content
greater than 26.4 µmol/l or 50% of the base value; urine output
below 0.5 ml/(kg·h) for more than 6 h, but not including patients
with dehydration and obstructive nephropathy (9). Compared with the term ‘acute renal
failure’, the term AKI covers a wider range, including renal damage
from slight changes in renal function to final renal function loss.
AKI can accurately reflect the developmental nature of nephropathy
(10). Although the incidence of AKI
is high, the awareness rate is generally low. Early symptoms of AKI
are not typical, and this, coupled with the fact that diagnoses are
affected by a variety of factors, results in low diagnostic
sensitivity. This in turn delays diagnosis and increases mortality
in critically ill patients (11).
Most AKI cases are reversible, and early diagnosis and treatment
can prevent the development of renal failure. Therefore, diagnosis
and treatment are keys in reducing the mortality rate in critically
ill patients with AKI (12).
Urine output and changes in SCr levels are usually
used to reflect changes in glomerular filtration rate and renal
function decline in order to provide a basis for the diagnosis of
AKI. Renal tubular damage can destroy the renal hypertonic
environment and reduce the ability to concentrate urine, resulting
in non-oliguric nephropathy (13).
In addition, urine output, which is affected by diuretics and
bladder capacity, cannot reflect renal function in real-time.
Therefore, for the diagnosis of AKI, urine output and SCr levels
cannot properly reflect renal injury. This misses the optimal
time-point for treatment and increases patient pain and systemic
economic burden (14). The results
of this study showed that there was no significant difference in
serum SCr level between the two groups at 2, 8, 12 and 24 h after
operation (P>0.05). This was because serum SCr level is affected
by nutritional status, muscle metabolism, and preoperative
medication. Renal compensatory and reserve capacity is strong under
normal conditions. SCr levels can only be increased slightly when
the glomerular filtration rate is reduced by 50% or more. In
addition, SCr accumulation takes time, and SCr levels cannot reach
a stable state within a short period (6). Therefore, SCr cannot be used as a
marker to accurately reflect short-term changes in renal
function.
NGAL is a member of lipocalin superfamily with a
small molecular weight of only 25 kDa (15). NGAL was first found in human
neutrophils. NGAL is very stable, so it can be easily detected in
serum. Under normal conditions, low NGAL expression levels can be
detected in a variety of tissues (lung, kidney, large intestine and
stomach). High expression levels of NGAL can be induced by cell
apoptosis after epithelial cell damage (16). The results of this study showed that
serum NGAL levels in the observation group were significantly
higher than in the control group at 2, 8, 12 and 24 h after
operation (P<0.05). A possible mechanism for this phenomenon may
be that various factors stimulated renal tubular epithelial cells,
leading to increased NGAL expression. NGAL can be absorbed by renal
epithelial cells to regulate the expression of apoptosis-related
proteins, which in turn promotes cell maturation and induces
granulocyte apoptosis (16).
CysC, a member of the cysteine protease inhibitor
superfamily, is a type of non-glycosylated alkaline protein
secreted by karyocytes. CysC can be synthesized at a very stable
rate and released into the circulation. After complete glomerular
filtration, CysC will be uptaken and degraded by nearby tubule
epithelial cells. Therefore, serum CysC levels can precisely
reflect the glomerular filtration rate. As such, CysC can be an
ideal marker for the diagnosis of AKI (17–19).
Under normal conditions, CysC levels are low. However, CysC levels
can significantly increase after renal tubular injury (20). The results of this study showed that
the serum CysC levels in the observation group were significantly
higher than in the control group at 2, 8, 12,0 and 24 h after
operation (P<0.05), indicating that internal environment of the
patients was altered after AKI.
Relevant studies have confirmed that increased NGAL
and CysC levels appeared 24 to 48 h prior to SCr level increases in
the diagnosis of AKI (21). In the
present study, we found that for NGAL in early diagnosis, the area
under the AKI curve was 0.904, the sensitivity was 90.2% and the
specificity was 89.5%; for CysC in early diagnosis, the area under
the AKI curve was 0.806, the sensitivity was 79.2% and the
specificity was 78.5%; for SCr in early diagnosis, the area under
the AKI curve was 0.634, the sensitivity was 64.2% and the
specificity was 62.5%. Our findings were consistent with previous
studies. In addition, the sensitivity and specificity of NGAL were
higher than those of CysC and SCr for the detection of AKI. The
results also showed that the levels of NGAL and CysC were
positively correlated with SCr levels, indicating that the
increased expression of NGAL and CysC were consistent with the
upregulation of SCr expression.
In summary, evaluating NGAL levels in critically ill
patients may improve the early detection of AKI and facilitate
early treatment and improve prognosis.
References
|
1
|
Teles F, de Mendonça Uchôa JV, Mendonça
Mirelli Barreto D and Costa Falcão Pedrosa A: Acute kidney injury
in leptospirosis: The Kidney Disease Improving Global Outcomes
(KDIGO) criteria and mortality. Clin Nephrol. 86:303–309. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Brown JR, Robb JF and Malenka DJ: Abstract
1056: Does ‘safe’ dosing of iodinated contrast prevent
contrast-induced acute kidney injury. Cardiology. 131:2492015.
|
|
3
|
Hoste EA, Bagshaw SM, Bellomo R, Cely CM,
Colman R, Cruz DN, Edipidis K, Forni LG, Gomersall CD, Govil D, et
al: Epidemiology of acute kidney injury in critically ill patients:
The multinational AKI-EPI study. Intensive Care Med. 41:1411–1423.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Wang N, Jiang L, Zhu B, Wen Y and Xi XM:
Beijing Acute Kidney Injury Trial (BAKIT) Workgroup: Fluid balance
and mortality in critically ill patients with acute kidney injury:
A multicenter prospective epidemiological study. Crit Care.
19:3712015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Cuartero M, Betbesé A, Sabater J, Ballús J
and Ordóñez J: Urinary TIMP2 and IGFBP7 as early biomarkers of
acute kidney injury in septic and nonseptic critically ill
patients. Crit Care. 19 Suppl 1:191–201. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Lagos-Arevalo P, Palijan A, Vertullo L,
Devarajan P, Bennett MR, Sabbisetti V, Bonventre JV, Ma Q,
Gottesman RD and Zappitelli M: Cystatin C in acute kidney injury
diagnosis: Early biomarker or alternative to serum creatinine?
Pediatr Nephrol. 30:665–676. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Veighey K and MacAllister R: Clinical
applications of remote ischaemic preconditioning in native and
transplant acute kidney injury. Pediatr Nephrol. 30:1749–1759.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ostermann M, Dickie H and Barrett NA:
Renal replacement therapy in critically ill patients with acute
kidney injury - when to start. Nephrol Dial Transplant.
27:2242–2248. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Bagshaw SM, Zappitelli M and Chawla LS:
Novel biomarkers of AKI: The challenges of progress ‘Amid the noise
and the haste’. Nephrol Dial Transplant. 28:235–238. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Young P, Bailey M, Beasley R, Henderson S,
Mackle D, McArthur C, McGuinness S, Mehrtens J, Myburgh J, Psirides
A, et al: SPLIT Investigators; ANZICS CTG: Effect of a buffered
crystalloid solution vs saline on acute kidney injury among
patients in the intensive care unit: The SPLIT Randomized Clinical
Trial. JAMA. 314:1701–1710. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Siew ED and Davenport A: The growth of
acute kidney injury: A rising tide or just closer attention to
detail? Kidney Int. 87:46–61. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Karvellas CJ, Durand F and Nadim MK: Acute
kidney injury in Cirrhosis. Crit Care Clin. 31:737–750. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Siew ED and Matheny ME: Choice of
reference Serum creatinine in defining acute kidney injury.
Nephron. 131:107–112. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Grynberg K, Polkinghorne KR, Ford S,
Stenning F, Lew TE, Barrett JA and Summers SA: Early serum
creatinine accurately predicts acute kidney injury post cardiac
surgery. BMC Nephrol. 18:932017. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
de Geus HR, Betjes MG, Schaick R and
Groeneveld JA: Plasma NGAL similarly predicts acute kidney injury
in sepsis and nonsepsis. Biomarkers Med. 7:415–421. 2013.
View Article : Google Scholar
|
|
16
|
Devarajan P: NGAL for the detection of
acute kidney injury in the emergency room. Biomarkers Med.
8:217–219. 2014. View Article : Google Scholar
|
|
17
|
Yim H, Kym D, Seo DK, Yoon J, Yang HT, Lee
J, Cho YS, Hur J, Chun W and Han SW: Serum cystatin C and
microalbuminuria in burn patients with acute kidney injury. Eur J
Clin Invest. 45:594–600. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Bongiovanni C, Magrini L, Salerno G, Gori
CS, Cardelli P, Hur M, Buggi M and Di Somma S: Serum cystatin C for
the diagnosis of acute kidney injury in patients admitted in the
emergency department. Dis Markers. 2015:4160592015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Volpon LC, Sugo EK and Carlotti AP:
Diagnostic and prognostic value of serum cystatin C in critically
ill children with acute kidney injury. Pediatr Crit Care Med.
16:e125–e131. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Gaygısız Ü, Aydoğdu M, Badoğlu M, Boyacı
N, Güllü Z and Gürsel G: Can admission serum cystatin C level be an
early marker subclinical acute kidney injury in critical care
patients? Scand J Clin Lab Invest. 76:143–150. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ghonemy TA and Amro GM: Plasma neutrophil
gelatinase-associated lipocalin (NGAL) and plasma cystatin C (CysC)
as biomarker of acute kidney injury after cardiac surgery. Saudi J
Kidney Dis Transpl. 25:582–588. 2014. View Article : Google Scholar : PubMed/NCBI
|