Introduction
Acute appendicitis is a common acute abdominal
condition and the conventional treatment is excision (1). There are three types of excision
surgery for the treatment of acute appendicitis: Single-incision
laparoscopic surgery (SILS), conventional laparoscopic appendectomy
(CLA) and open appendectomy (OA) (1–4). OA is
widely used clinically, even though CLA was first introduced in
1983 (5).
Compared with OA, CLA has the merits of precise
diagnosis, minimal trauma, less pain, quick recovery, less
bleeding, fewer complications and a reduced duration of
hospitalization (6). However, a
previous study has reported that CLA has a greater surgical
duration than OA, a high cost and provides no significant advantage
for the recovery of patients (7).
With the advancement of laparoscopic surgical
instruments and technology, SILS was developed and applied for the
treatment of acute appendicitis (8).
Previous studies have typically compared two methods of
appendectomy (9,10), and few have concurrently evaluated
the effect of the three surgical methods for acute appendicitis
treatment. Therefore, a network meta-analysis was conducted in the
present study to systematically assess the therapeutic effect of
SILS, CLA and OA in the treatment of acute appendicitis. The aim
was to determine the optimal surgical procedure for the treatment
of acute appendicitis, and to serve as a reference for surgeons
when selecting the appropriate treatment.
Materials and methods
Source of data
PubMed (http://www.ncbi.nlm.nih.gov/pubmed) and Embase
(http://www.embase.com) databases up to April 2016
were systematically searched using the predesigned search terms:
‘single-incision laparoscopic appendectomy’, ‘SILA’, ‘single
incision laparoscopic surgery’, ‘SILS appendectomy’ and/or
‘laparoscope or laparoscopic appendectomy’ and/or ‘open surgery or
laparotomy or open appendectomy’ and ‘appendicite aigue or acute
appendicitis’.
Inclusion and exclusion criteria
The included studies for analysis had to satisfy the
following criteria: i) Studies were randomized controlled trials;
ii) at least two of the methods for treatment of acute appendicitis
(SILS, CLA and OA) were compared; and iii) the outcome measures
included surgical procedure duration, duration of hospital stay,
wound infection and incidence of abscesses. All reviews, comments,
reports and letters were excluded.
Data extraction and quality
assessment
The following details of the included studies were
extracted independently by two reviewers: The first author,
publication year, study region, study time, methods of treatment,
the corresponding number of the patients and the demographic
characteristics of the participants, including age, gender and body
mass index (BMI).
Quality of the included studies was assessed
independently by two reviewers in terms of the risk of bias
assessment according to Cochrane Collaboration recommendations
(11). The discrepancies during the
process were discussed with a third reviewer and resolved by
consensus.
Statistical analysis
All data analyses were performed using ADDIS 1.16.5
software (Drug Information Systems, Groningen, The Netherlands)
(12,13). A direct comparison meta-analysis was
first performed. Dichotomous data for effectiveness were analyzed
using the odds ratio (OR) and 95% confidence interval (CI).
Quantitative data for effectiveness were estimated using the
standardized mean difference (SMD) and 95% CI. Heterogeneity was
evaluated using the I2 statistical method (14). A value >50% was regarded as
substantial heterogeneity. A random effects model was applied when
significant heterogeneity was identified (I2 >50%);
otherwise, a fixed-effect model was performed (15). In the network meta-analysis, when the
three treatments were connected as a loop, the inconsistency was
assessed using node-splitting analysis and inconsistency standard
deviation (ISD) (16). If
node-splitting analysis determined P>0.05 and the 95% CI of ISD
encompassed 1, the consistency model was used for pooled analysis.
Otherwise, the inconsistency model was used as described previously
(17). Convergence was assessed
using potential scale reduction factor (PSRF) and the
Brooks-Gelman-Rubin (BGR) method (18), and a value of ~1 indicated a good
convergence (18). P<0.05 was
considered to indicate a statistically significant result.
Results
Study selection
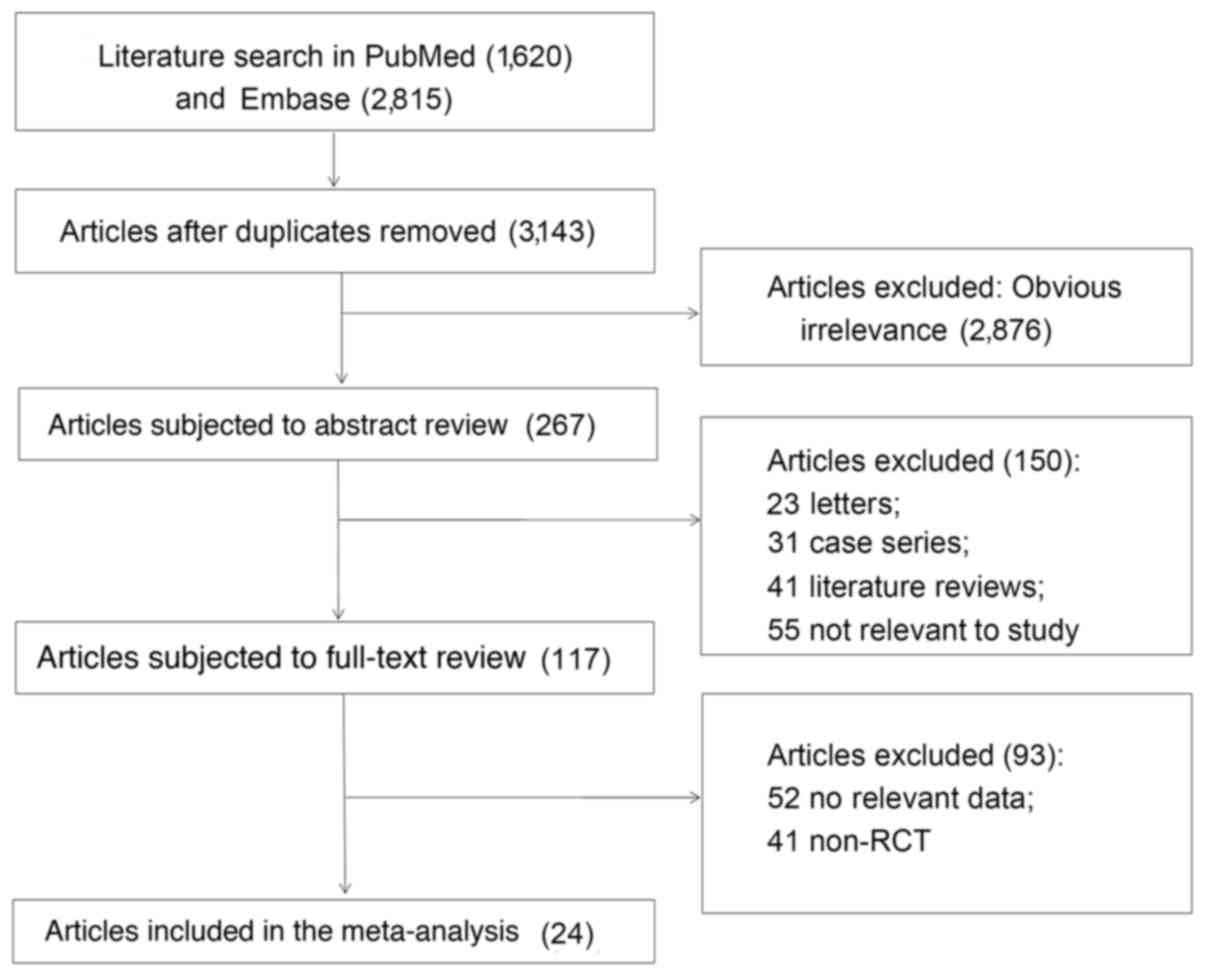
As shown in Fig. 1, a
total of 4,435 records were identified from PubMed (1,620) and
Embase (2,815) databases by initial retrieval. Initially, 1,292
duplicate records were removed and another 3,026 studies that
deviated from inclusion criteria were excluded by reviewing the
titles and abstracts. From the remaining 117 studies, the
full-texts were reviewed and 93 studies were removed due to
unavailable data or due to the non-randomized control trial design.
A total of 24 eligible studies were included in the present
meta-analysis (9,10,19–40).
Characteristics of included
studies
The characteristics of the included studies are
displayed in Table I (9–32). These
include studies published between 1996 and 2015. The participants
were distributed in USA, Chile, Turkey, Spain, Sweden, Denmark,
Greece, Australia, Korea, India and China. The treatment strategies
for acute appendicitis included SILS, CLA and OA. There were no
significant differences in demographic characteristics, including
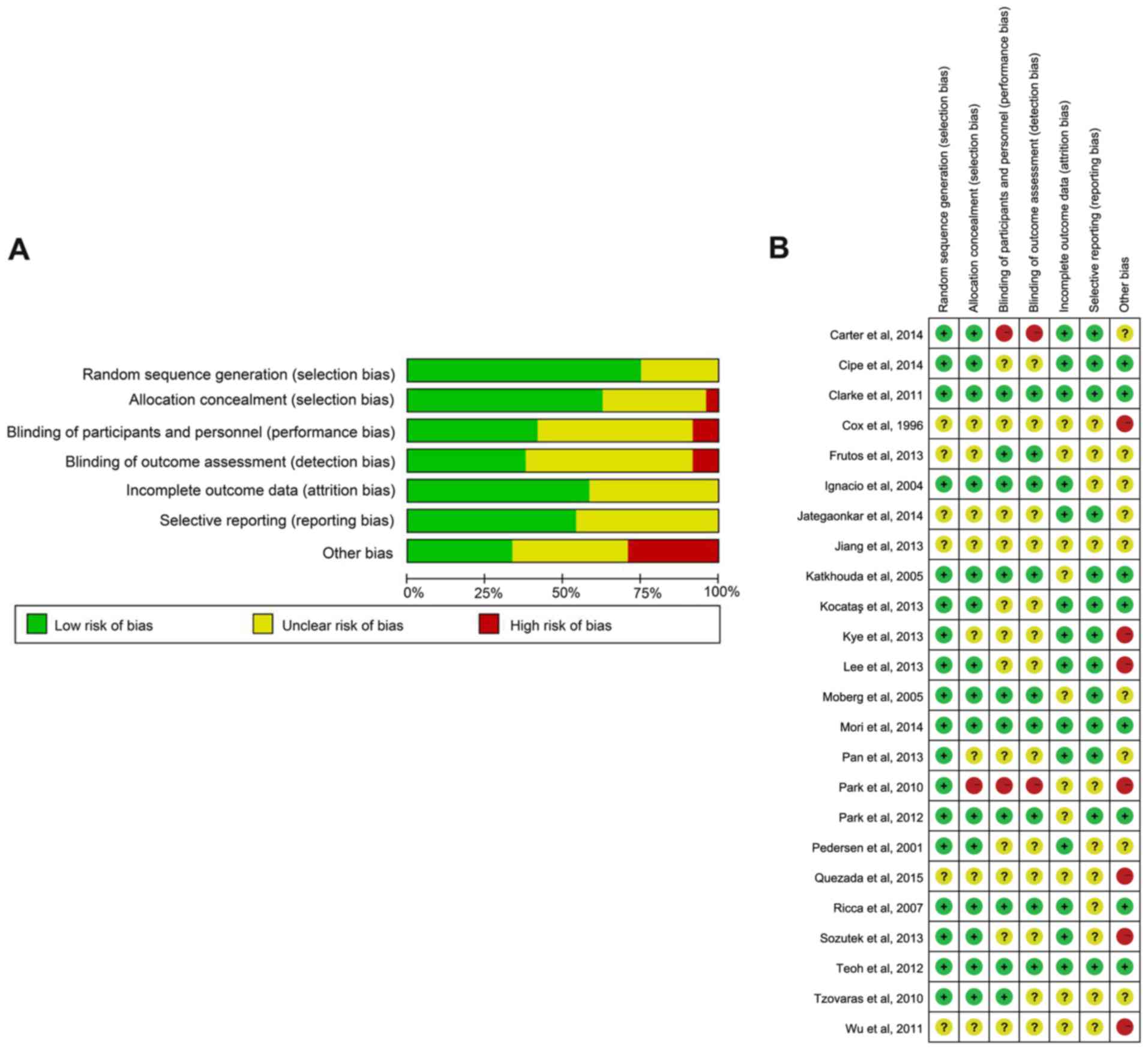
age, sex and BMI between the groups in each comparison. Quality
assessment showed that there was a relatively low risk of bias in
the included studies. However, blinding of participants and
personnel (performance bias) and blinding of outcome assessment
(detection bias) of the included studies revealed a notably high
risk of bias (Fig. 2).
 | Table I.Characteristics of included
studies. |
Table I.
Characteristics of included
studies.
| Author, year | Study location | Study year | Item | Number of
patients | Age (years) | Sex (M/F) | Body mass index | (Refs.) |
|---|
| Park et al,
2010 | Korea | 2009 | SILS | 20 | NA | 9/11 | NA | (32) |
|
|
|
| CLA | 20 | NA | 8/12 | NA |
|
| Park et al,
2012 | Korea | 2008–2009 | SILS | 42 | 23.90±11.90 | 14/28 | 21.00±2.80 | (31) |
|
|
|
| CLA | 62 | 29.90±12.20 | 41/21 | 23.00±3.10 |
|
| Teoh et al,
2012 | China | 2009–2011 | SILS | 98 | 39.19±15.55 | 58/40 | NA | (37) |
|
|
|
| CLA | 97 | 40.65±15.68 | 59/38 | NA |
|
| Lee et al,
2013 | Korea | 2010–2011 | SILS | 116 | 28.40±15.40 | 64/52 | 21.40±3.20 | (10) |
|
|
|
| CLA | 113 | 28.50±17.20 | 68/45 | 22.70±4.40 |
|
| Frutos et
al, 2013 | Spain | 2009–2010 | SILS | 91 | 28.04±11.03 | 42/49 | 23.84±3.98 | (9) |
|
|
|
| CLA | 93 | 31.02±12.41 | 47/46 | 24.02±3.84 |
|
| Kye et al,
2013 | Korea | 2009–2010 | SILS | 51 | 27.55±12.40 | NA | 22.03±4.07 | (27) |
|
|
|
| CLA | 51 | 29.20±13.98 | NA | 21.97±3.49 |
|
| Pan et al,
2013 | China | 2009–2011 | SILS | 42 | 34.10±14.50 | 24/18 | 23.40±3.50 | (30) |
|
|
|
| CLA | 42 | 34.90±14.90 | 20/22 | 23.50±4.40 |
|
| Mori et al,
2014 | Spain | 2011–2012 | SILS | 60 | 28.10±9.30 | 42/18 | 24.60±3.00 | (29) |
|
|
|
| CLA | 60 | 30.00±9.20 | 34/26 | 24.40±2.10 |
|
| Carter et
al, 2014 | USA | 2010–2012 | SILS | 37 | 34.00±11.00 | 19/18 | 25.00±4.00 | (17) |
|
|
|
| CLA | 38 | 35.00±12.00 | 24/14 | 25.00±4.00 |
|
| Clarke et
al, 2011 | USA | 1997–2001 | CLA | 23 | 31 (19–60) | 15/8 | NA | (21) |
|
|
|
| OA | 14 | 33 (18–50) | 9/5 | NA |
|
| Cox et al,
1996 | Australia | NA | CLA | 33 | 25 (18–75) | 33/0 | NA | (40) |
|
|
|
| OA | 31 | 25 (18–84) | 31/0 | NA |
|
| Ignacio et
al, 2004 | USA | 2001 | CLA | 26 | 28.4±6.6 | NA | NA | (22) |
|
|
|
| OA | 26 | 27.4±9.3 | NA | NA |
|
| Katkhouda et
al, 2005 | USA | NA | CLA | 113 | 29 (18–71) | 78/35 | NA | (25) |
|
|
|
| OA | 134 | 28 (17–63) | 104/30 | NA |
|
| Moberg et
al, 2005 | Sweden | 2001–2003 | CLA | 81 | 31 (15–71) | 46/35 | 24 (17–34) | (28) |
|
|
|
| OA | 82 | 31 (15–83) | 58/24 | 25 (17–43) |
|
| Pedersen et
al, 2001 | Denmark | NA | CLA | 282 | 26 (18–40) | 131/151 | NA | (33) |
|
|
|
| OA | 301 | 27 (18–40) | 143/158 | NA |
|
| Ricca et al,
2007 | USA | NA | CLA | 26 | NA | NA | ≥25 | (35) |
|
|
|
| OA | 26 | NA | NA | ≥25 |
|
| Tzovaras et
al, 2010 | Greece | 2002–2008 | CLA | 72 | 26 (15–68) | NA | 26 (18–35) | (38) |
|
|
|
| OA | 75 | 22 (14–65) | NA | 24 (18–36) |
|
| Quezada et
al, 2015 | Chile | 2003 | CLA | 97 | 39±17.1 | 49/48 | NA | (34) |
|
|
|
| OA | 130 | 38±17.5 | 49/81 | NA |
| Cipe et al,
2014 | Turkey | 2012 | CLA | 121 | 26.4±9.7 | 65/56 | 23.7±2.5 | (20) |
|
|
|
| OA | 120 | 29.7±12.8 | 71/49 | 24.4±2.9 |
|
| Jiang et al,
2013 | China | 2011–2012 | SILS | 10 | 32.5± 8.0 | 10/0 | NA | (24) |
|
|
|
| CLA | 20 | 34.0± 7.3 | 13/7 | NA |
|
|
|
|
| OA | 20 | 39.7±13.8 | 10/10 | NA |
|
| Wu et al,
2011 | China | 2005–2009 | CLA | 62 | 75.3±7.1 | 33/29 | NA | (39) |
|
|
|
| OA | 88 | 75.5±8.1 | 46/42 | NA |
|
| Kocataş et
al, 2013 | Turkey | NA | CLA | 50 | 27.4±18.5 | NA | NA | (26) |
|
|
|
| OA | 46 | 27.4±18.5 | NA | NA |
|
| Sozutek et
al, 2013 | Turkey | 2010–2011 | SILS | 25 | 30.6±12.4 | 12/13 | 23.2±3.79 | (36) |
|
|
|
| CLA | 25 | 30±11 | 7/18 | 23.1±2.58 |
|
|
|
|
| OA | 25 | 32.2±9.4 | 14/11 | 23±3.07 |
|
| Jategaonkar and
Yadav, 2014 | India | 2009–2011 | SILS | 212 | 33.79±12.61 | 148/64 | 24.13±2.02 | (23) |
|
|
|
| CLA | 218 | 35.30±13.37 | 165/53 | 23.61±2.40 |
|
Results of direct comparison by
meta-analysis
Heterogeneity tests were performed. The appropriate
effect model was chosen according to the results of I2.
As shown in Table II, the random
effects model was performed for the three comparisons of surgical
procedure duration (CLA vs. OA, CLA vs. SILA and OA vs. SILA) and
for the comparison between CLA and OA in duration of hospital stay
(all I2>50%), which indicated heterogeneity among
studies. Furthermore, duration of hospital stay (CLA vs. SILA and
OA vs. SILA), assessment of wound infection and incidence of
abscesses were investigated using the fixed-effect model.
| Table II.Results of direct comparison
meta-analysis. |
Table II.
Results of direct comparison
meta-analysis.
| Item | Comparison | K | I2 | Model | SMD/OR (95%CI) | Z | P-value |
|---|
| Duration of
surgical | CLA vs. OA | 7 | 76.1 | Random effects
model | −0.24 (−0.58 to
0.11) | 1.36 | 0.17 |
| procedure | CLA vs. SILA | 12 | 83.5 | Random effects
model | 0.46 (0.20 to
0.72) | 2.61 | 0.01 |
|
| OA vs. SILA | 2 | 96.3 | Random effects
model | 2.44 (−1.33 to
6.72) | 1.19 | 0.23 |
| Duration of | CLA vs. OA | 11 | 50.3 | Random effects
model | 0.43 (0.24 to
0.61) | 4.56 | <0.01 |
| hospital stay | CLA vs. SILA | 10 | 10.2 | Fixed-effect
model | −0.10 (−0.21 to
0.00) | 1.87 | 0.06 |
|
| OA vs. SILA | 2 | 0 | Fixed-effect
model | −1.30 (−1.78 to
−0.82) | 5.31 | <0.01 |
| Wound
infection | CLA vs. OA | 13 | 0 | Fixed-effect
model | 1.90 (1.18 to
3.07) | 2.63 | 0.01 |
|
| CLA vs. SILA | 10 | 0 | Fixed-effect
model | 1.00 (0.55 to
1.81) | <0.01 | 1 |
|
| OA vs. SILA | 1 | – | – | 0.33 (0.04 to
2.99) | 1.01 | 0.31 |
| Incidence of | CLA vs. OA | 9 | 0 | Fixed-effect
model | 0.60 (0.34 to
1.05) | 1.78 | 0.08 |
| abscesses | CLA vs. SILA | 6 | 0 | Fixed-effect
model | 1.79 (0.64 to
5.02) | 1.11 | 0.27 |
Network analysis
Parameter setting of ADDIS was follows: Number of
chains, 4; tuning iterations, 20,000; simulation iterations,
50,000; thinning interval, 10; inference samples, 10,000; variance
scaling factor, 2.5. According to the consistency test, the
consistency model was used to pool data regarding to the outcomes
of surgical procedure duration (P=0.18; ISD, 19.66; 95% CI, 0.70 to
52.27), duration of hospital stay (P=0.96; ISD, 1.02; 95% CI, 0.02
to 7.16), wound infection (P=0.77; ISD, 0.92; 95% CI, 0.04 to 2.04)
and incidence of abscesses (P=0.93; ISD, 0.92; 95% CI, 0.04 to
2.04). The PSRFs in each item were 1.02, 1.03, 1.03 and 1.02, which
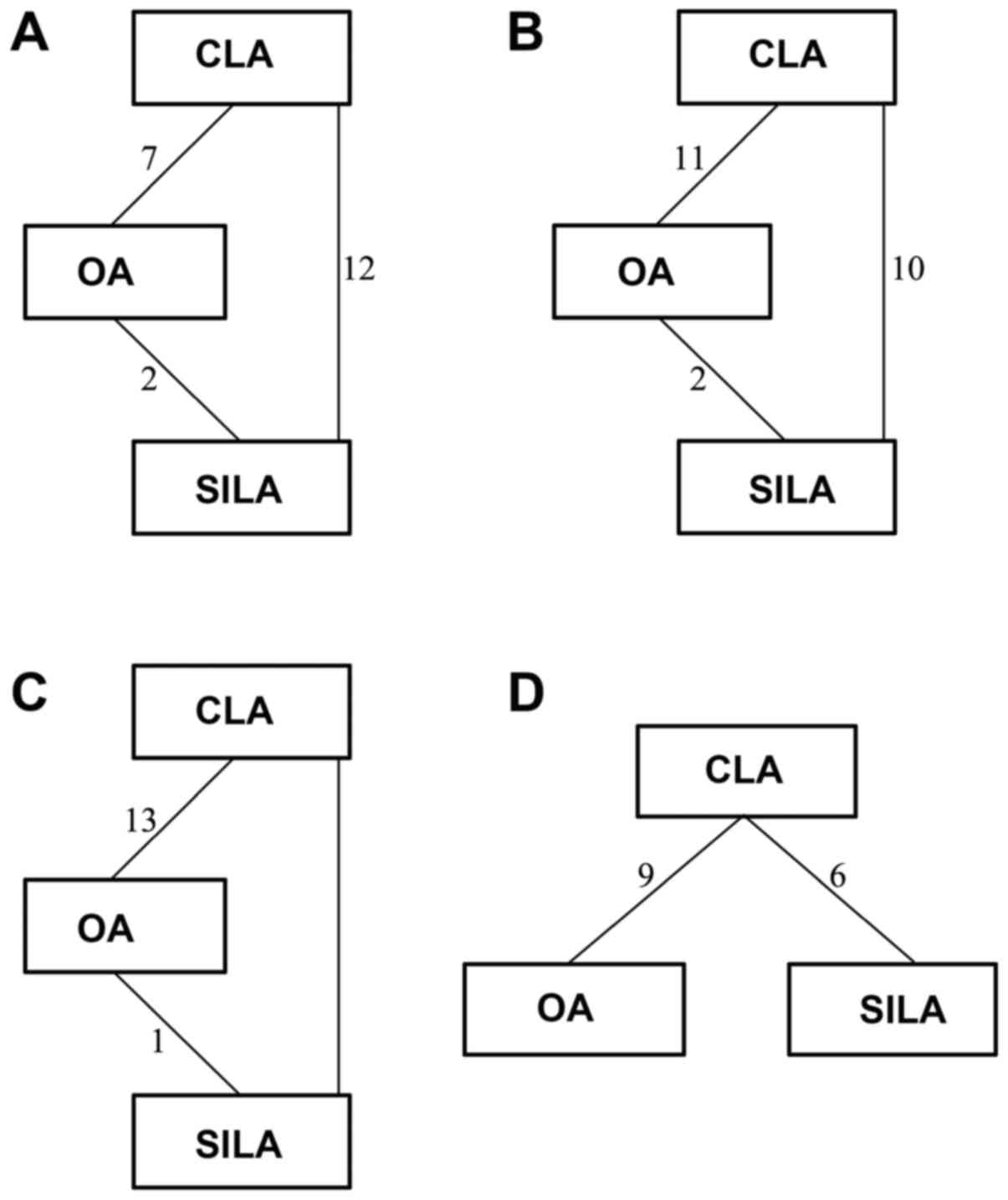
indicated complete convergence. Fig.
3A-D demonstrates the network of surgical procedure duration,
duration of hospital stay, wound infection and incidence of
abscesses of the three surgical procedures, respectively. As shown
in Table III, the pooled results
revealed that the surgical procedure duration of OA was the
shortest and a significant difference was identified between OA and
SILS (P=0.01). However, there was no significant difference in
surgical duration between SILS and CLA. In comparison with OA, SILS
and CLA exhibited a significantly shorter duration of hospital stay
(all P<0.01) and lower risk of wound infection (SILS vs. OA,
P=0.02 and CLA vs. OA, P<0.01, respectively); however, no
significant differences were indicated between SILS and CLA.
Furthermore, SILS exhibited a significantly lower incidence of
abscesses compared with OA (P=0.04), while no significant
difference was observed between OA and CLA.
| Table III.Comparison of the different methods
for treatment of acute appendicitis. |
Table III.
Comparison of the different methods
for treatment of acute appendicitis.
| Factor | Value | Z-value | P-value |
|---|
| Duration of
surgical procedure (SMD) |
|
|
|
| CLA vs.
OA | 9.53
(−1.8,21.21) | 1.62 | 0.10 |
| CLA vs.
SILS | −9.25 (−17.90,
−0.68) | 2.11 | 0.04 |
| OA vs.
CLA | −9.53
(−21.21,1.80) | 1.62 | 0.10 |
| OA vs.
SILS | −18.72 (−32.29,
−5.49) | 2.74 | 0.01 |
| SILS
vs. CLA | 9.25 (0.68,
17.90) | 2.11 | 0.04 |
| SILS
vs. OA | 18.72 (5.49,
32.29) | 2.74 | 0.01 |
| Duration of
hospital stay (SMD) |
|
|
|
| CLA vs.
OA | −0.65 (−1.13,
−0.39 | 3.44 | 0.01 |
| CLA vs.
SILS | 0.19 (−0.06,
0.49) | 1.34 | 0.18 |
| OA vs.
CLA | 0.65 (0.39,
1.13) | 3.44 | 0.01 |
| OA vs.
SILS | 0.84 (0.53,
1.43) | 3.66 | 0.01 |
| SILS
vs. CLA | −0.19 (−0.49,
0.06) | 1.35 | 0.18 |
| SILS
vs. OA | −0.84 (−1.43,
−0.53) | 3.66 | 0.01 |
| Wound infection
(OR) |
|
|
|
| CLA vs.
OA | 0.43 (0.24,
0.75) | 2.90 | 0.01 |
| CLA vs.
SILS | 1.23 (0.63,
2.39) | 0.61 | 0.54 |
| OA vs.
CLA | 2.31 (1.33,
4.10) | 2.90 | 0.01 |
| OA vs.
SILS | 2.83 (1.20,
6.76) | 2.36 | 0.02 |
| SILS
vs. CLA | 0.81 (0.42,
1.58) | 0.61 | 0.54 |
| SILS
vs. OA | 0.35 (0.15,
0.83) | 2.36 | 0.02 |
| Incidence of
abscesses (OR) |
|
|
|
| CLA vs.
OA | 1.73 (0.79,
3.88) | 1.35 | 0.18 |
| CLA vs.
SILS | 0.38 (0.10,
1.19) | 1.53 | 0.13 |
| OA vs.
CLA | 0.58 (0.26,
1.26) | 1.35 | 0.18 |
| OA vs.
SILS | 0.22 (0.04,
0.89) | 2.01 | 0.04 |
| SILS
vs. CLA | 2.63 (0.84,
10.34) | 1.53 | 0.13 |
| SILS
vs. OA | 4.54 (1.12,
23.51) | 2.01 | 0.04 |
Ranking of the three methods for treatment of acute
appendicitis is displayed in Fig. 4.
Regarding surgical procedure duration, OA was ranked the optimal
method whereas SILS was ranked as the worst. However, regarding
duration of hospital stay, wound infection and incidence of
abscesses, SILS was ranked as the optimal method whereas OA was
ranked as the worst.
Discussion
In the present study, the outcomes of three
appendectomy methods were systematically compared using network
meta-analysis. The results indicated that SILS resulted in a
shorter duration of hospital stay, lower incidence of wound
infection and lower incidence of abscesses, but demonstrated a
longer surgical procedure duration compared with OA. However, no
significant differences were identified between CLA and SILS in any
outcome.
The present results were in accordance with previous
meta-analyses (6,41), which showed that laparoscopic
appendectomy acquired faster postoperative rehabilitation, shorter
hospital stay and fewer postoperative complications compared with
OA. However, laparoscopic appendectomy exhibited a longer surgical
procedure duration compared with OA. It may be suggested that the
application of laparoscopic equipment increases the complexity of
the surgery and requires improved surgical skill; thus, the
surgical procedure duration was prolonged. However, improvements in
surgical skill may reduce the surgical time. Furthermore, the small
wounds created during CLA and SILS restrict the range of movement
during surgery, which may prolong the duration of the surgical
procedure.
Although SILS and CLA do not reduce surgical
procedure duration in comparison with other procedures, CLA and
SILS are used widely in the clinic due to their associated
benefits. For example, laparoscopic surgery may be used to
comprehensively and precisely check lesions in enterocoelia
(42). Furthermore, in some cases,
such as with obese patients, a larger wound is required to excise
the appendix when OA is performed (43). Additionally, single-incision
laparoscopic appendectomy (SILA) and CLA are postulated to reduce
postoperative pain and enhance cosmesis effectively (44). It is likely that CLA and SILS result
in reduced pain due the smaller wound that is cut.
SILS is an improved method of laparoscopic
appendectomy developed from CLA (9)
and is valuable for use in clinical settings due to the smaller
scar it leaves compared with CLA. Saber et al (45) simplified SILS in clinical settings
and improved the surgical procedure. Furthermore, Hua et al
(46) demonstrated that SILA is a
feasible and safe alternative procedure to CLA. Additionally, OA,
CLA and SILA are all effective for appendicitis; however, SILA is
considered a minimally invasive surgery (47), and has developed during the evolution
of the appendectomy procedure from OA to CLA to SILA. It may be
possible for surgeons improve their skills to reduce the duration
of surgery and gain improved surgical success. The future prospects
of SILS are better than those of OA and CLA due to patients'
requests to undergo a minimally scarring and painless procedure
with a good prognosis. Therefore, SILS procedures should be
developed and simplified according to clinical experience in order
to reduce the duration of the surgical procedure and abscess
risk.
Heterogeneity was observed in the present study. The
potential causes and sources of heterogeneity are diverse. In the
present study, articles from different regions, including USA,
Turkey, Australia, South Korea, Spain, India and China were
included. The patient characteristics, surgical skills, surgical
practice and severity of appendicitis may contribute to the
heterogeneity, in addition to the sample size of each study.
Furthermore, a few shortcomings should be taken into account in
this network meta-analysis. Firstly, the effectiveness among all of
the treatments for acute appendicitis was not compared due to the
incompleteness of data. A study by Wilms et al (48) compared the outcomes between
conservative antibiotics and appendectomies, but did not classify
the exact surgical approaches (CLA or OA). Therefore, the outcomes
of antibiotics were not included. For further studies, this point
should be considered and a strict experimental design followed.
Additionally, in the network meta-analysis of the incidence of
abscesses, the loop was not closed as OA and SILA were not compared
in any of the included studies; therefore, it was not possible to
use node-splitting analysis for consistency testing. Furthermore,
ADDIS software is not freely programmable, and thus the results
that can be reported were limited. Another potential limitation was
that only four outcomes were considered in the present network
meta-analysis and alternative outcomes such as pain score, amount
of bleeding and other postoperative complications were not included
due to a lack of original data. Furthermore, only two studies that
compared OA and SILS were included in the present study, which may
limit the credibility of the present results. Further studies and
stricter experimental design are required to further support the
present results. Despite these limitations, there are several
strengths in the present meta-analysis. The three methods of
managing acute appendicitis were systemically and comprehensively
compared for the first time. The results of the present study may
provide guidance for the treatment of acute appendicitis in the
clinic.
In conclusion, the present comprehensive network
meta-analysis indicates that laparoscopic appendectomy,
particularly SILS and CLA has greater advantages for treating acute
appendicitis compared with OA. Considering patients' requests for
minimal scarring and for the procedure to be painless with a good
prognosis, SILS appears to be an optimal procedure choice. However,
SILS requires improvement and simplification to reduce the duration
of the surgical procedure.
References
|
1
|
Ruffolo C, Fiorot A, Pagura G, Antoniutti
M, Massani M, Caratozzolo E, Bonariol L, di Pinto Calia F and Bassi
N: Acute appendicitis: What is the gold standard of treatment?
World J Gastroenterol. 19:8799–8807. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Cai YL, Xiong XZ, Wu SJ, Cheng Y, Lu J,
Zhang J, Lin YX and Cheng NS: Single-incision laparoscopic
appendectomy vs conventional laparoscopic appendectomy: Systematic
review and meta-analysis. World J Gastroenterol. 19:5165–5173.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Sateesh S, Subraj H, Mahesh G and Rao PS:
Comparative analysis between single incision and conventional
laparoscopic appendectomy for acute appendicitis. Int J Res Med
Sci. 2:1626–1631. 2014. View Article : Google Scholar
|
|
4
|
Minutolo V, Licciardello A, Di Stefano B,
Arena M, Arena G and Antonacci V: Outcomes and cost analysis of
laparoscopic versus open appendectomy for treatment of acute
appendicitis: 4-years experience in a district hospital. BMC Surg.
14:142014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Semm K: Endoscopic appendectomy.
Endoscopy. 15:59–64. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Wei B, Qi CL, Chen TF, Zheng ZH, Huang JL,
Hu BG and Wei HB: Laparoscopic versus open appendectomy for acute
appendicitis: A metaanalysis. Surg Endosc. 25:1199–1208. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ingraham AM, Cohen ME, Bilimoria KY,
Pritts TA, Ko CY and Esposito TJ: Comparison of outcomes after
laparoscopic versus open appendectomy for acute appendicitis at 222
ACS NSQIP hospitals. Surgery. 148:625–637. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Cugura JF, Janković J, Kulis T, Kirac I
and Beslin MB: Single incision laparoscopic surgery (SILS)
cholecystectomy: Where are we? Acta Clin Croat. 47:245–248.
2008.PubMed/NCBI
|
|
9
|
Frutos MD, Abrisqueta J, Lujan J, Abellan
I and Parrilla P: Randomized prospective study to compare
laparoscopic appendectomy versus umbilical single-incision
appendectomy. Ann Surg. 257:413–418. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Lee WS, Choi ST, Lee JN, Kim KK, Park YH,
Lee WK, Baek JH and Lee TH: Single-port laparoscopic appendectomy
versus conventional laparoscopic appendectomy: A prospective
randomized controlled study. Ann Surg. 257:214–218. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Higgins JP and Green S: Cochrane Handbook
For Systematic Reviews Of Interventions. Wiley Online Library;
2008, View Article : Google Scholar
|
|
12
|
Hillege H, de Brock B, van Valkenhoef G
and Zhao J: ADDIS: An automated way to do network meta-analysis.
University of Groningen, Research Institute SOM (Systems,
Organisations and Management). 2012.
|
|
13
|
Valkenhoef G, Tervonen T, Zwinkels T,
Brock B and Hillege H: ADDIS: A decision support system for
evidence-based medicine. Decis Support Syst. 55:459–475. 2013.
View Article : Google Scholar
|
|
14
|
Lau J, Ioannidis JP and Schmid CH:
Quantitative synthesis in systematic reviews. Ann Intern Med.
127:820–826. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Feng RN, Zhao C, Sun CH and Li Y:
Meta-analysis of TNF 308 G/A polymorphism and type 2 diabetes
mellitus. PLoS One. 6:e184802011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Lu G and Ades A: Assessing evidence
inconsistency in mixed treatment comparisons. J Am Stat Assoc.
101:447–459. 2006. View Article : Google Scholar
|
|
17
|
Dias S, Welton NJ, Caldwell DM and Ades
AE: Checking consistency in mixed treatment comparison
meta-analysis. Stat Med. 29:932–944. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Brooks SP and Gelman A: General methods
for monitoring convergence of iterative simulations. J Comput
Graphical Stat. 7:434–455. 1998. View
Article : Google Scholar
|
|
19
|
Carter JT, Kaplan JA, Nguyen JN, Lin MY,
Rogers SJ and Harris HW: A prospective, randomized controlled trial
of single-incision laparoscopic vs conventional 3-port laparoscopic
appendectomy for treatment of acute appendicitis. J Am Coll Surg.
218:950–959. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Cipe G, Idiz O, Hasbahceci M, Bozkurt S,
Kadioglu H, Coskun H, Karatepe O and Muslumanoglu M: Laparoscopic
versus open appendectomy: Where are we now? Chirurgia (Bucur).
109:518–522. 2014.PubMed/NCBI
|
|
21
|
Clarke T, Katkhouda N, Mason RJ, Cheng BC,
Olasky J, Sohn HJ, Moazzez A, Algra J, Chaghouri E and Berne TV:
Laparoscopic versus open appendectomy for the obese patient: A
subset analysis from a prospective, randomized, double-blind study.
Surg Endosc. 25:1276–1280. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ignacio RC, Burke R, Spencer D, Bissell C,
Dorsainvil C and Lucha PA: Laparoscopic versus open appendectomy:
What is the real difference? Results of a prospective randomized
double-blinded trial. Surg Endosc. 18:334–337. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Jategaonkar PA and Yadav SP: Single site
multiport umbilical laparoscopic appendicectomy versus conventional
multiport laparoscopic appendicectomy in acute settings. Ann R Coll
Surg Engl. 96:452–457. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Jiang X, Meng HB, Zhou DL, Ding WX and Lu
LS: Comparison of clinical outcomes of open, laparoscopic and
single port appendicectomies. Ann R Coll Surg Engl. 95:468–472.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Katkhouda N, Mason RJ and Towfigh S:
Laparoscopic versus open appendectomy: A prospective, randomized,
double-blind study. Adv Surg. 40:1–19. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kocataş A, Gönenç M, Bozkurt MA, Karabulut
M, Gemici M and Alış H: Comparison of open and laparoscopic
appendectomy in uncomplicated appendicitis: A prospective
randomized clinical trial. Ulus Travma Acil Cerrahi Derg.
19:200–204. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Kye BH, Lee J, Kim W, Kim D and Lee D:
Comparative study between single-incision and three-port
laparoscopic appendectomy: A prospective randomized trial. J
Laparoendosc Adv Surg Tech A. 23:431–436. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Moberg AC, Berndsen F, Palmquist I,
Petersson U, Resch T and Montgomery A: Randomized clinical trial of
laparoscopic versus open appendicectomy for confirmed appendicitis.
Br J Surg. 92:298–304. 2005. View
Article : Google Scholar : PubMed/NCBI
|
|
29
|
Mori Villalobos R, Rufino Escoll J,
Herrerías González F, Mias Carballal MC, Escartin Arias A and
Olsina Kissler JJ: Prospective, randomized comparative study
between single-port laparoscopic appendectomy and conventional
laparoscopic appendectomy. Cir Esp. 92:472–477. 2014.(In English,
Spanish). PubMed/NCBI
|
|
30
|
Pan Z, Jiang XH, Zhou JH and Ji ZL:
Transumbilical single-incision laparoscopic appendectomy using
conventional instruments: The single working channel technique.
Surg Laparosc Endosc Percutan Tech. 23:208–211. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Park J, Kwak H, Kim SG and Lee S:
Single-port laparoscopic appendectomy: Comparison with conventional
laparoscopic appendectomy. J Laparoendosc Adv Surg Tech A.
22:142–145. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Park JH, Hyun KH, Park CH, Choi SY, Choi
WH, Kim DJ, Lee S and Kim JS: Laparoscopic vs transumbilical
single-port laparoscopic appendectomy; results of prospective
randomized trial. J Korean Surg Soc. 78:213–218. 2010. View Article : Google Scholar
|
|
33
|
Pedersen AG, Petersen O, Wara P, Rønning
H, Qvist N and Laurberg S: Randomized clinical trial of
laparoscopic versus open appendicectomy. Br J Surg. 88:200–205.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Quezada F, Quezada N, Mejia R, Brañes A,
Padilla O, Jarufe N and Pimentel F: Laparoscopic versus open
approach in the management of appendicitis complicated exclusively
with peritonitis: A single center experience. Int J Surg. 13:80–83.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Ricca R, Schneider JJ, Brar H and Lucha
PA: Laparoscopic appendectomy in patients with a body mass index of
25 or greater: Results of a double blind, prospective, randomized
trial. JSLS. 11:54–58. 2007.PubMed/NCBI
|
|
36
|
Sozutek A, Colak T, Dirlik M, Ocal K,
Turkmenoglu O and Dag A: A prospective randomized comparison of
single-port laparoscopic procedure with open and standard 3-port
laparoscopic procedures in the treatment of acute appendicitis.
Surg Laparosc Endosc Percutan Tech. 23:74–78. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Teoh AY, Chiu PW, Wong TC, Poon MC, Wong
SK, Leong HT, Lai PB and Ng EK: A double-blinded randomized
controlled trial of laparoendoscopic single-site access versus
conventional 3-port appendectomy. Ann Surg. 256:909–914. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Tzovaras G, Baloyiannis I, Kouritas V,
Symeonidis D, Spyridakis M, Poultsidi A, Tepetes K and Zacharoulis
D: Laparoscopic versus open appendectomy in men: A prospective
randomized trial. Surg Endosc. 24:2987–2992. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Wu SC, Wang YC, Fu CY, Chen RJ, Huang HC,
Huang JC, Lu CW, Hsieh CH and Lin CY: Laparoscopic appendectomy
provides better outcomes than open appendectomy in elderly
patients. Am Surg. 77:466–470. 2011.PubMed/NCBI
|
|
40
|
Cox MR, McCall JL, Toouli J, Padbury RT,
Wilson TG, Wattchow DA and Langcake M: Prospective randomized
comparison of open versus laparoscopic appendectomy in men. World J
Surg. 20:263–266. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Ohtani H, Tamamori Y, Arimoto Y,
Nishiguchi Y, Maeda K and Hirakawa K: Meta-analysis of the results
of randomized controlled trials that compared laparoscopic and open
surgery for acute appendicitis. J Gastrointest Surg. 16:1929–1939.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Huang YJ, Chen QJ and Xu LC: Laparoscopic
treatment of appendix root perforation complicated with acute
suppurative peritonitis. J Huaihai Med. 3:0062013.
|
|
43
|
Corneille MG, Steigelman MB, Myers JG,
Jundt J, Dent DL, Lopez PP, Cohn SM and Stewart RM: Laparoscopic
appendectomy is superior to open appendectomy in obese patients. Am
J Surg. 194:877–881. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Gill RS, Shi X, Al-Adra DP, Birch DW and
Karmali S: Single-incision appendectomy is comparable to
conventional laparoscopic appendectomy: A systematic review and
pooled analysis. Surg Laparosc Endosc Percutan Tech. 22:319–327.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Saber AA, Elgamal MH, El-Ghazaly TH,
Dewoolkar AV and Akl A: Simple technique for single incision
transumbilical laparoscopic appendectomy. Int J Surg. 8:128–130.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Hua J, Gong J, Xu B, Yang T and Song Z:
Single-incision versus conventional laparoscopic appendectomy: A
meta-analysis of randomized controlled trials. J Gastrointest Surg.
18:426–436. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Switzer NJ, Gill RS and Karmali S: The
evolution of the appendectomy: From open to laparoscopic to single
incision. Scientifica (Cairo). 2012:8954692012.PubMed/NCBI
|
|
48
|
Wilms IM, de Hoog DE, de Visser DC and
Janzing HM: Appendectomy versus antibiotic treatment for acute
appendicitis. Cochrane Database Syst Rev: CD008359. 2011.
View Article : Google Scholar
|